Kramer IRH, Pindborg JJ, Shear M., 2nd edn. Berlin, Heidelberg, New York: Springer; 1992
White SC. Cone-beam imaging in dentistry. Health Phys. 2008; 95:(5)628-637
Jones AV, Craig GT, Franklin CD. Range and demographics of odontogenic cysts diagnosed in a UK population over a 30-year period. J Oral Pathol Med. 2006; 35:(8)500-507
Meghji S, Qureshi W, Henderson B, Harris M. The role of endotoxin and cytokines in the pathogenesis of odontogenic cysts. Arch Oral Biol. 1996; 41:(6)523-531
Mortensen H, Winther JE, Birn H. Periapical granulomas and cysts. An investigation of 1,600 cases. Scand J Dent Res. 1970; 78:(3)241-250
Shear M. Cholesterol in dental cysts. Oral Surg Oral Med Oral Pathol. 1963; 16:1465-1473
Main DM. Epithelial jaw cysts: a clinicopathological reappraisal. Br J Oral Surg. 1970; 8:(2)114-125
Struthers P, Shear M. Root resorption by ameloblastomas and cysts of the jaws. Int J Oral Surg. 1976; 5:(3)128-132
Main DM. The enlargement of epithelial jaw cysts. Odontol Revy. 1970; 21:(1)29-49
Bodner L. Cystic lesions of the jaws in children. Int J Pediatr Otorhinolaryngol. 2002; 62:(1)25-29
Shear M. Clinical statistics of dental cysts. J Dent Assoc S Af. 1961; 16:360-364
Rasmusson LG, Magnusson BC, Borrman H. The lateral periodontal cyst. A histopathological and radiographic study of 32 cases. Br J Oral Maxillofac Surg. 1991; 29:(1)54-57
Cohen DA, Neville BW, Damm DD, White DK. The lateral periodontal cyst. A report of 37 cases. J Periodontol. 1984; 55:(4)230-234
Altini M, Shear M. The lateral periodontal cyst: an update. J Oral Pathol Med. 1992; 21:(6)245-250
Barnes L, Eveson JW, Reichart P, Sidransky D. Pathology and Genetics of Head and Neck Tumours.Lyon: IARC Press; 2005
Barreto DC, Gomez RS, Bale AE, Boson WL, De Marco L. PTCH gene mutations in odontogenic keratocysts. J Dent Res. 2000; 79:(6)1418-1422
Browne RM. The odontogenic keratocyst. Clinical aspects. Br Dent J. 1970; 128:(5)225-231
Morgan TA, Burton CC, Qian F. A retrospective review of treatment of the odontogenic keratocyst. J Oral Maxillofac Surg. 2005; 63:(5)635-639
Forssell K, Forssell H, Kahnberg KE. Recurrence of keratocysts. A long-term follow-up study. Int J Oral Maxillofac Surg. 1988; 17:(1)25-28
Brannon RB. The odontogenic keratocyst. A clinicopathologic study of 312 cases. Part I. Clinical features. Oral Surg Oral Med Oral Pathol. 1976; 42:(1)54-72
Dammer R Conservative or radical treatment of keratocysts: a retrospective review. Br J Oral Maxillofac Surg. 1997; 35:46-48
This article aims to discuss the clinical features, radiological assessment, histopathology and management of a variety of odontogenic cysts. It also highlights the reclassification of odontogenic keratocysts to keratocystic odontogenic tumours.
Clinical Relevance: Dentists should be aware of the multiple odontogenic cysts that can present in the oral cavity and be able to formulate appropriate management plans.
Article
An odontogenic cyst is a pathological, epithelial-lined cavity containing fluid or semi-fluid which arises from the epithelial remnants of tooth formation. The 1992 World Health Organization (WHO) classification of odontogenic cysts is widely recognized and categorizes them as developmental or inflammatory in nature.1
Odontogenic cysts are often asymptomatic and therefore may expand to a large size before any clinical signs are noted and, as such, their presence is often an incidental finding on radiographic examination. These cysts may become increasingly obvious clinically as they increase in size, initially creating a bony hard swelling. As this gradually and slowly enlarges, the bony covering becomes increasingly thin, which clinically may be demonstrated on palpation by the classic ‘egg shell cracking’ as the thin bone gives way. As the lesion expands beyond its bony confines, it then becomes a fluctuant swelling. The slow expansion of the cyst usually causes displacement of related structures, such as the inferior alveolar bundle in the mandible and thus altered sensation is not a common feature of mandibular cysts. When altered sensation occurs, it can be an indication of infection or more aggressive pathology.
The pathogenesis for the development and expansion of cysts is often debated and the authors aim to give a brief outline of this. However, specific details of pathogenesis and histopathology are outwith the scope of this article.
There is a myriad of cyst-like lesions which can manifest in the jaws. These include odontogenic tumours, such as ameloblastomas (Figure 1) and osteolytic lesions, such as metastatic cancer. Therefore, careful diagnosis and treatment planning of these lesions is essential.
Figure 1. Ameloblastoma affecting right mandible.
Further investigations are often required to establish a definitive diagnosis. For example, sensibility testing can be useful, particularly in the diagnosis of a radicular cyst. Radiographic imaging plays a significant role in determining features which can aid diagnosis. While plain radiographic films are useful, the advances in cone beam computed tomography (CBCT) have allowed for greater detailed imaging of, not only the lesion, but also the surrounding structures.2 Biopsies of the cyst lining allows for a definitive diagnosis prior to appropriate treatment planning in extensive lesions and this is essential where the diagnosis is unclear. Aspiration of cyst contents can be carried out and visual inspection can give an indication of what type of lesion is present. Electrophoresis is rarely carried out on cyst contents.
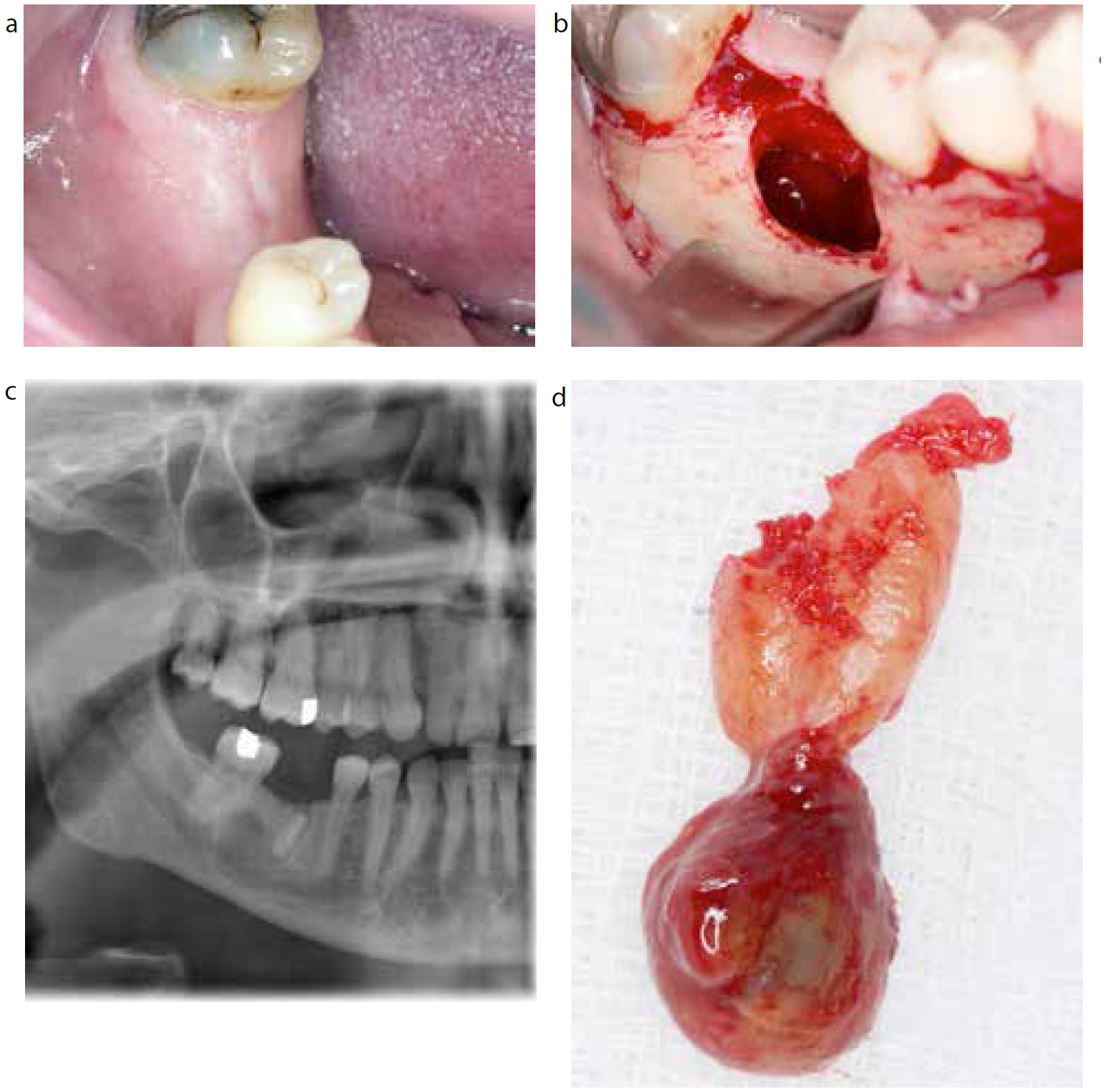
Most odontogenic cysts are treated by either enucleation or marsupialization. Enucleation involves the complete removal of the cyst and is the treatment of choice as it enables primary closure and also allows the whole lining to be examined pathologically (Figures 2a–d). However, incomplete removal of the lining may lead to recurrence. Incomplete removal often occurs when the cyst has perforated through the alveolar cortex and the cyst lining is adherent to the adjacent soft tissues. Alternatively, marsupialization can be undertaken. This technique involves the creation of a surgical window in the wall of the cyst, decompressing the cyst and allowing the removal of any cyst contents. Then the cyst lining is sutured to the surrounding mucosa, thus maintaining the opening into the cyst. The opening can also be maintained with packing material or a prosthetic bung. This obviously requires a compliant and dextrous patient who would be able to maintain hygiene. This decompression facilitates a reduction in the size of the cyst and so, at a later date, enucleation can be carried out. This would be indicated if enucleation would risk damaging surrounding structures, if there was a risk of pathological fracture of the jaw, or if the involved tooth is to be maintained. It may also be indicated if the patient was not medically fit enough for a general anaesthetic, which may be necessary for the management of large cystic lesions.
Figure 2. Enulceation of radicular cyst: (a) no clinical evidence of pathology; (b) cyst cavity following surgical removal of retained LR6 root and enucleation of associated lesion; (c) evidence of corticated radiolucency associated with retained root of LR6; (d) extracted root of LR6 with associated radicular cyst attached to apex.
It is important that dental practitioners are aware of these lesions, thus allowing inclusion as a differential diagnosis and construction of an appropriate management plan. This article aims to give a brief overview of a variety of odontogenic cysts.
Radicular cyst
Radicular cysts are inflammatory in nature and the most common cystic lesions of the jaws, accounting for approximately 60% of all odontogenic cysts.3 Although they can develop in all tooth-bearing regions, they are more often reported in the maxilla (60%) compared to the mandible (40%). The reason for this possible increased prevalence in the maxilla has been attributed to the increased risk of pulpal damage to anterior maxillary teeth due to trauma and palatal invaginations.
Often radicular cysts are asymptomatic and, on clinical examination, tissues appear normal, only becoming evident on radiographic examination. They are associated with the apex of a non-vital tooth. Patients may complain of pain related to the cystic lesion and, on occasion, a sinus may be present.
Development of these cysts is initiated by chronic inflammation following pulpal necrosis. The epithelial lining of radicular cysts develops from the rest cells of Malassez in the periodontal ligament. It is widely accepted that the rest cells of Malassez are stimulated by endotoxins and inflammatory cytokines.4 There are a number of theories of how these cysts form. The most widely accepted theory is that the epithelium surrounds a granuloma and, as the epithelial mass grows, the granuloma in the centre becomes necrotic and liquefies as it is further from nutritional sources. Another suggested theory is that the epithelium lines a cavity which is pre-existing. Once formed, the cyst enlarges with osmosis contributing to the increase in cyst size.
It has been suggested that there may be individuals who are prone to developing radicular cysts and this may explain why patients present with more than one.5
Classically, radicular cysts are round or ovoid radiolucencies with a radio-opaque margin extending from the lamina dura of the non-vital tooth. This margin, however, may not always be present in the case of infection or rapidly expanding cysts (Figure 3). Root resorption may be seen radiographically but the size of the lesion radiographically does not give an indication of whether the lesion is cystic in nature or an apical granuloma. Differentiating between apical granulomas and radicular cysts radiographically has proven challenging and inaccurate.6
Figure 3. Radicular cyst associated with non-vital UR2 with dens evaginatus.
Histopathologically, these cysts are lined by stratified squamous epithelium which may have mucous cells or ciliated cells, with deposits of cholesterol a common finding.7 The cyst contents include breakdown products of degenerating cells and a soluble protein content of 5–11 g/dl.
Treatment is by removal of the source of infection by completing root canal treatment or extraction of the associated non-vital tooth. Small cysts are shown to regress, however, larger cysts may require enucleation with peri-radicular surgery of the associated tooth or extraction.
Residual cysts
A residual cyst is the term given to a radicular cyst which remains following extraction of the associated tooth. These account for approximately 10% of all odontogenic cysts.8 Clinically, they present with similar features to a radicular cyst. Radiographically, they appear as a round or oval unilocular radiolucency but, in contrast to a radicular cyst, there is no obvious tooth involvement (Figure 4). Histopathological features are consistent with that of a radicular cyst, however, as the source of infection (the tooth) has been removed, they appear less inflammatory. Treatment for such cysts usually consists of marsupialization or enucleation.
Figure 4. Residual cyst in LR5 region.
Dentigerous cysts
Dentigerous cysts enclose the crown of an unerupted tooth by expansion of its follicle. These cysts are attached to the tooth at the amelo-cemental junction. They affect males more commonly than females and, although they can present in any age group, they are commonly seen in the third decade. The incidence of these varies between 18–24% of odontogenic cysts in different studies.3
Clinically, dentigerous cysts are associated with commonly impacted teeth, such as mandibular third molar teeth and maxillary canine teeth.3 They are usually detected incidentally on radiographs taken to investigate a missing tooth or a tooth that has failed to erupt.
These cysts are well circumscribed, unilocular radiolucencies with well-defined sclerotic margins associated with the crown of an unerupted tooth (Figure 5). Occasionally, trabeculations may be seen, suggesting erroneously that the lesion is multi-locular. Radiographically, there are three variations of dentigerous cysts:
Central – the crown is enveloped symmetrically;
Lateral – the follicle is dilated on one aspect and does not completely enclose the crown;
Circumferential – the cyst occurs in a band around the amelocemental junction and appears like a doughnut-shaped lesion. The entire tooth may appear to be enveloped by the cyst radiographically.
Figure 5. Dentigerous cyst associated with unerupted LR8.
Dentigerous cysts often cause resorption of the roots of adjacent teeth and adjacent structures may also be displaced.9
The exact mechanism for dentigerous cyst development is unknown but they are commonly thought to arise from fluid accumulation between enamel of the tooth and the reduced enamel epithelium.10 Cyst expansion is similar to that of a radicular cyst whereby it is dependent on bone resorption and hydrostatic pressure.
Histologically, the lining is a thin, regular layer 2–5 cells thick of non-keratinized stratified squamous or flattened/low cuboidal epithelium which resembles the reduced enamel epithelium. The cyst contains proteinaceous, yellowish fluid and cholesterol crystals with a soluble protein content of 5–7 g/dl.
Treatment may involve removal of the causative tooth and enucleation of the cyst lining. Marsupialization or enucleation of the cyst while leaving the tooth in place may allow the tooth to erupt if root formation of the involved tooth is incomplete.
Eruption cyst
This is a cyst associated with an unerupted tooth. However, unlike dentigerous cysts which develop around an unerupted tooth lying in bone, an eruption cyst is within the soft tissues overlying an unerupted tooth. These occur most frequently in children and only occasionally in adults. They account for approximately 22% of cystic lesions affecting paediatric patients but less than 1% among the adult population11,12 and affect deciduous and permanent teeth, most often anteriorly to the first permanent molar.
Clinically, a painless, soft, fluctuant swelling is seen on the gingivae overlying the erupting tooth. This may be the same colour as the gingivae or blue or purple in colour (Figure 6). Radiographs are not routinely required for investigation of an eruption cyst but, if taken, a radiolucent lesion at the alveolar margin may be seen. No bony involvement is noted.
Figure 6. Clinical image of an eruption cyst in an 18 month old child.
The pathogenesis is similar to a dentigerous cyst in that the epithelium is believed to be derived from the reduced enamel epithelium. However, eruption is impeded by soft tissue, rather than bone, particularly dense fibrous tissue.
Histology shows that the epithelial lining of the cyst consists of 2–3 layers of squamous epithelium resembling the reduced enamel epithelium. The lining is usually intensely inflamed. Most eruption cysts burst spontaneously, but if they persist, marsupialization can be undertaken. This involves excising the dome of the cyst, exposing the crown of the tooth and letting it erupt.
Lateral periodontal cysts
Lateral periodontal cysts account for less than 1% of cysts occurring in the jaws3 and, as the name suggests, these form in the lateral periodontal position. They are inflammatory in nature. These can develop at any age, however, are more prevalent in those aged 40–70 years of age with equal gender distribution.13,14 The most commonly affected sites are the mandibular premolar areas and anterior maxilla.
Similar to other cysts, these often go undetected for some time, but occasionally a blue fluctuant swelling is noted which is associated with the gingiva adjacent to a vital tooth (Figure 7). Pain is not a common complaint on presentation.
Figure 7. Lateral periodontal cyst.
Although it is widely accepted that these are odontogenic in origin, there is uncertainty over the origin of epithelial lining. Possible sources are the rest cells of Malassez, remnants of the dental lamina or the reduced enamel epithelium.
Lateral periodontal cysts can be seen radiographically between the cervical margin of the tooth and the apex. They are typically round or oval in shape, less than 1 cm in diameter with a sclerotic margin15 (Figure 8). Their appearance can be very similar to a keratocystic odontogenic tumour, only differentiated following histological evaluation.
Figure 8. Radiographic appearance of lateral periodontal cyst between LR2 and LR3.
Histologically, these unicystic or multicystic lesions are commonly lined by a thick, non-keratinized layer of squamous or cuboidal epithelium, usually ranging from 1–5 cell layers, similar to the appearance of reduced enamel epithelium, wide with small, pyknotic nuclei. Occasionally, glycogen-rich clear cells can be noted in the epithelial lining and, interestingly, many appear to have plaque formation or thickening of this epithelial lining.
Treatment of these cysts should involve enculeation of the lesion while maintaining the associated tooth. This is, however, not always possible and the tooth may have to be sacrificed.
Keratocystic odontogenic tumour
The authors feel that it is important to highlight the change of classification of odontogenic keratocyst to keratocystic odontogenic tumour by the WHO. This was because the new title better reflects its neoplastic nature.16
These have a peak incidence in the second and third decades and most commonly occur in males. Of keratocystic odontogenic tumours, 65–83% occur in the mandible and one-half originate at the angle of the mandible. Multiple keratocystic odontogenic tumours can be associated with naevoid basal cell carcinoma syndrome (Figure 9).
These lesions are developmental in nature but recent studies have demonstrated the role of the PTCH gene, a tumour suppressor, in the aetiology of these cysts.17 It is agreed that the cysts develop from odontogenic epithelium and two sources of epithelium have been suggested: the dental lamina and its remnants or extensions of basal cells from the overlying epithelium.
Clinically, these are locally destructive. As they can grow to a large size undetected and are commonly found in the angle of the mandible,18 the presenting symptom may be paraesthesia of the inferior alveolar nerve.
Recurrence rates of 50–60%19,20 have been reported and several possible reasons have been reported for this, including satellite cysts,21 and their thin and fragile lining makes them difficult to enucleate entirely.
Radiographically, they may appear as small, round or ovoid unilocular radiolucencies or they may be larger with scalloped margins. The lesions are well demarcated with distinct sclerotic margins, but may also be diffuse in parts. Multi-locular lesions can also occur. Adjacent teeth may be displaced but root resorption occurs rarely. Cortical perforation can be seen. Lesions can be multiple or solitary (Figure 10).
Figure 10. Unilocular keratocystic odontogenic tumour affecting the right angle of the mandible.
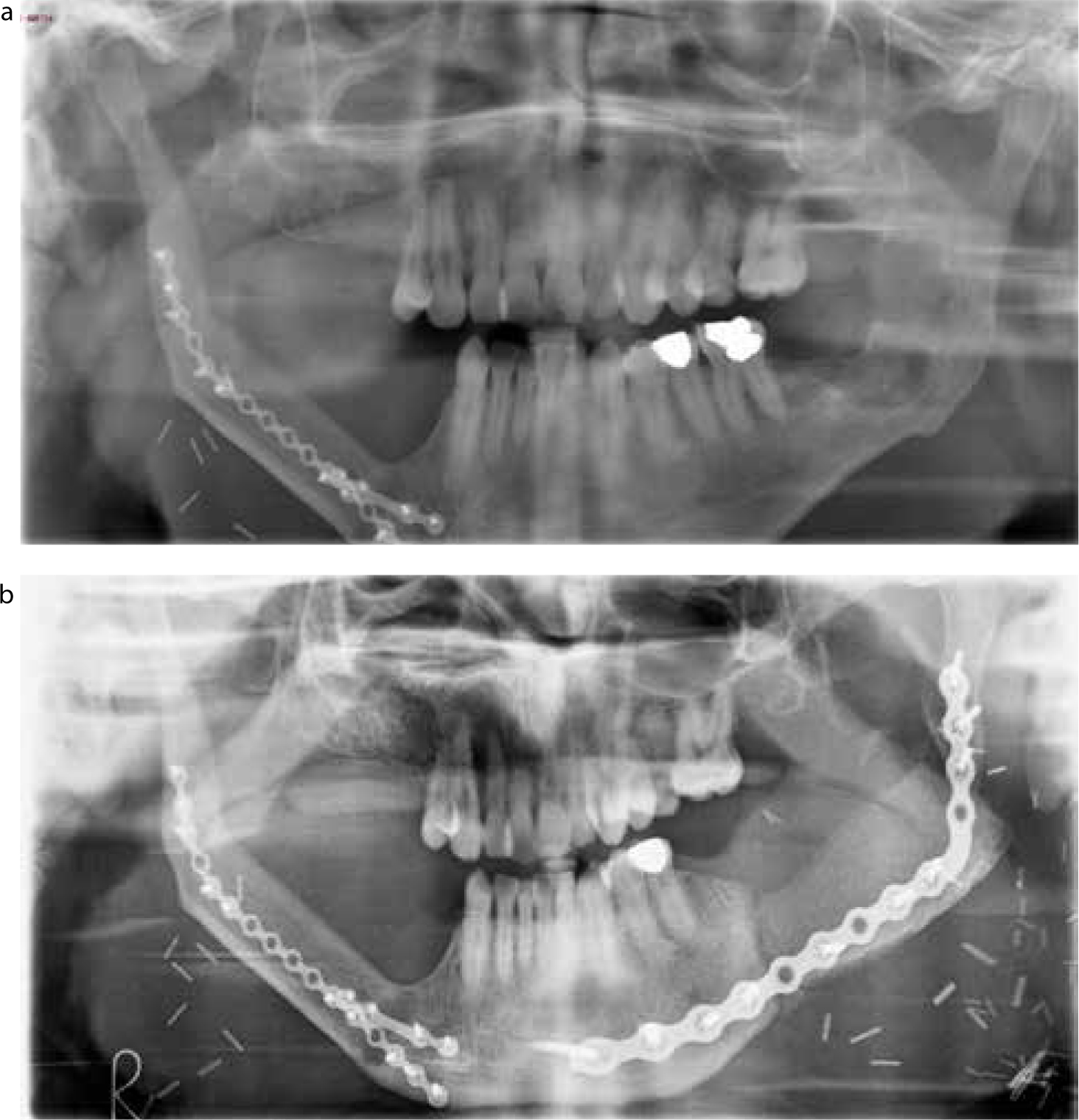
Histopathologically, the cyst is lined by regular keratinized stratified squamous epithelium of 5–8 cell layers thick. There are no rete ridges. The well-defined basal layer made up of columnar or cuboidal cells is intensely basophilic, which is an important distinguishing feature. Mitotic figures are often found in the suprabasal layers, and some linings show features of epithelial dysplasia. These can be unilocular, and associated with less aggressive behaviour, or multilocular. Management of these lesions is no longer enucleation with currettage but en-block resection, including the surrounding bone if the lesion is small enough to leave a rim of supporting bone. If the lesion is large, then bone resection and reconstruction with a composite free graft is required22 (Figure 11).
Figure 11. Bilateral keratocystic odontogenic tumours reconstruction. (a) Right-sided reconstruction with a fibula flap following resection of keratocystic odontogenic tumour and demonstrating a new left-sided lesion. (b) Left-sided reconstruction with a DCIA flap following resection of keratocystic odontogenic tumour.
Conclusion
There are a number of odontogenic cysts which can affect the jaws. This article provides a brief overview of these and highlights the importance of identifying and managing these lesions appropriately. A summary of these cysts can be found in Table 1.
Radicular
Residual
Dentigerous
Eruption
Lateral periodontal
Keratocystic odontogenic tumour
Aetiology
Cell rests of Malassez
Cell rests of Malassez
Reduced enamel epithelium
Reduced enamel epithelium
Inconclusive
Inconclusive
Clinical
Associated with non-vital teeth
Not associated with a tooth
Associated with crown of unerupted tooth
Painless, soft, fluctuant swelling seen on gingivae overlying erupting tooth that may be blue or purple.
May see blue fluctuant swelling associated with gingivae, adjacent to a vital tooth
May have associated inferior alveolar nerve paraesthesia
Peak age
3rd decade
>30 years
3rd decade
Most frequent in children
40–70 years
2nd and 3rd decades
Common sites
Maxilla
Maxilla
Mandibular third molars and maxillary canines
Deciduous and permanent teeth often anterior to first permanent molar
Mandibular premolar and anterior maxilla regions
Angle of mandible
Radiology
Round radiolucency with radio-opaque margin extending from lamina dura of non-vital tooth
Similar appearance to radicular cyst but not associated with tooth
Circumscribed, unilocular, well defined, sclerotic margins associated with crown of an unerupted tooth
Radiolucent lesion at alveolar margin and no bony involvement
Between cervical margin and apex of tooth, round or oval shape, less than 1cm diameter, sclerotic margin
May be unilocular or multi-locular. May have defined sclerotic margins but can also be diffuse. May have scalloped margins