O'Connell AC, Marini JC. Evaluation of oral problems in an osteogenesis imperfecta population. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 87:189-196 https://doi.org/10.1016/s1079-2104(99)70272-6
Ruggiero SL, Dodson TB, Fantasia J American Association of Oral and Maxillofacial Surgeons position paper on medication-related osteonecrosis of the jaw. 2014 update. J Oral Maxillofac Surg. 2014; 72:1938-1956 https://doi.org/10.1016/j.joms.2014.04.031
Marini JC, Reich A, Smith SM. Osteogenesis imperfecta due to mutations in non-collagenous genes: lessons in the biology of bone formation. Curr Opin Pediatr. 2014; 26:500-507 https://doi.org/10.1097/MOP.0000000000000117
Sykes B, Ogilvie D, Wordsworth P Consistent linkage of dominantly inherited osteogenesis imperfecta to the type I collagen loci: COL1A1 and COL1A2. Am J Hum Genet. 1990; 46:293-307
van Dijk FS, Cobben JM, Kariminejad A Osteogenesis imperfecta: a review with clinical examples. Mol Syndromol. 2011; 2:1-20 https://doi.org/10.1159/000332228
Hald JD, Folkestad L, Swan CZ Osteogenesis imperfecta and the teeth, eyes, and ears – a study of non-skeletal phenotypes in adults. Osteoporos Int. 2018; 29:2781-2789 https://doi.org/10.1007/s00198-018-4663-x
Mäyränpää MK, Tamminen IS, Kröger H, Mäkitie O. Bone biopsy findings and correlation with clinical, radiological, and biochemical parameters in children with fractures. J Bone Miner Res. 2011; 26:1748-1758 https://doi.org/10.1002/jbmr.373
Bhatt RN, Hibbert SA, Munns CF. The use of bisphosphonates in children: review of the literature and guidelines for dental management. Aust Dent J. 2014; 59:9-19 https://doi.org/10.1111/adj.12140
Brown JJ, Ramalingam L, Zacharin MR. Bisphosphonate-associated osteonecrosis of the jaw: does it occur in children?. Clin Endocrinol (Oxf). 2008; 68:863-867 https://doi.org/10.1111/j.1365-2265.2008.03189.x
Chahine C, Cheung MS, Head TW Tooth extraction socket healing in pediatric patients treated with intravenous pamidronate. J Pediatr. 2008; 153:719-720 https://doi.org/10.1016/j.jpeds.2008.05.003
Schwartz S, Joseph C, Iera D, Vu DD. Bisphosphonates, osteonecrosis, osteogenesis imperfecta and dental extractions: a case series. J Can Dent Assoc. 2008; 74:537-542
Malmgren B, Aström E, Söderhäll S. No osteonecrosis in jaws of young patients with osteogenesis imperfecta treated with bisphosphonates. J Oral Pathol Med. 2008; 37:196-200 https://doi.org/10.1111/j.1600-0714.2007.00607.x
Hennedige AA, Jayasinghe J, Khajeh J, Macfarlane TV. Systematic review on the incidence of bisphosphonate related osteonecrosis of the jaw in children diagnosed with osteogenesis imperfecta. J Oral Maxillofac Res. 2014; 4 https://doi.org/10.5037/jomr.2013.4401
Kamoun-Goldrat A, Ginisty D, Le Merrer M. Effects of bisphosphonates on tooth eruption in children with osteogenesis imperfecta. Eur J Oral Sci. 2008; 116:195-18 https://doi.org/10.1111/j.1600-0722.2008.00529.x
Bhatt RN, Munns CM, Hibbert SA, Blinkhorn AS. Baseline survey on the oral health of children on intravenous bisphosphonates.Sydney: University of Sydney; 2010
Rody WJ, King GJ, Gu G. Osteoclast recruitment to sites of compression in orthodontic tooth movement. Am J Orthod Dentofacial Orthop. 2001; 120:477-489 https://doi.org/10.1067/mod.2001.118623
Iglesias-Linares A, Yáñez-Vico RM, Solano-Reina E Influence of bisphosphonates in orthodontic therapy: systematic review. J Dent. 2010; 38:603-611 https://doi.org/10.1016/j.jdent.2010.05.012
Venkataramana V, Chidambaram S, Reddy BV Impact of bisphosphonate on orthodontic tooth movement and osteoclastic count: an animal study. J Int Oral Health. 2014; 6:1-8
Osteogenesis imperfecta: minimizing complications in oral surgery/orthodontic treatment Kaye Jordan Emily Carter Ciarán P Devine Aliki Tsichlaki Judith Jones Dental Update 2025 48:9, 726-730.
Osteogenesis imperfecta (OI) is a rare genetic condition that affects connective tissue and is primarily characterized by bone fragility. Owing to the progressive nature of the disease, patients require life-long management of the adverse effects and the subsequent complications they can experience. Since the introduction of bisphosphonates as a treatment modality, complications and bone deformities associated with OI have been minimized. However, intravenous bisphosphonates in young patients could present a new era of difficulties for the dental profession. We report on a case of a patient with OI who presented with severe orthodontic crowding and describe the multidisciplinary treatment planning required to minimize potential complications.
CPD/Clinical Relevance: General dental practitioners should be aware of the characteristics of osteogenesis imperfecta and the potential complications associated with dental treatment.
Article
Osteogenesis imperfecta (OI) is a hereditary connective tissue disorder with variable phenotypic presentations.1 There is a reported incidence of 15,000–20,000 live births globally.2 OI is characterized by a decreased amount of normal type 1 collagen and this can be a result of decreased collagen secretion or abnormal collagen production.1 Traditionally OI has been subdivided into four subtypes (Table 1).3 In recent years however, at least three further subtypes have been discovered.1 It has now been suggested that all classifications represent a continuum of the same disease, ranging from mild to severe, with the majority of OI cases classified as type 1 of mild.1
Inheritance
Collagen disorder
Sclera
Fractures
Severity
Type 1
AD
Quantitative
Blue
Pre-pubertal
Mild
Type 2
AD
Qualitative/quantitative
Blue
Perinatal
Perinatal lethality
Type 3
AD
Qualitative
Normal
In utero
Progressive deformity
Type 4
AD
Qualitative
Normal
Pre-ambulatory
Moderately severe
AD: autosomal dominant.
Collagen forms a major portion of connective tissue, which is used to establish the framework for bone formation. With bone being poorly formed, a common descriptor for this condition has aptly been ‘brittle bone disease’. Apart from brittle bones however, other tissues and systems are affected including ocular, dental and cardiac.4,5
Treatment is largely aimed at preventing further development of the disease side effects and symptoms, with the primary treatment modality being the use of regular intravenous (IV) bisphosphonate medications. This treatment can potentially have a major impact on the provision of safe dental treatment such as the potential for medication-related osteonecrosis of the jaw (MRONJ).
MRONJ is defined as exposed bone, or bone that can be probed through an intra- or extra-oral fistula in the maxillofacial region that has persisted for more than 8 weeks in patients with a history of treatment with anti-resorptive or anti-angiogenic drugs, and where there has been no history of radiation therapy to the jaw or no obvious metastatic disease to the jaws.6 Signs and symptoms of MRONJ are summarized in Figure 2, although, on occasion, patients are asymptomatic. Here, we present a case of an adolescent patient with OI transitioning through orthodontic and oral surgery treatment in order to correct their malocclusion.
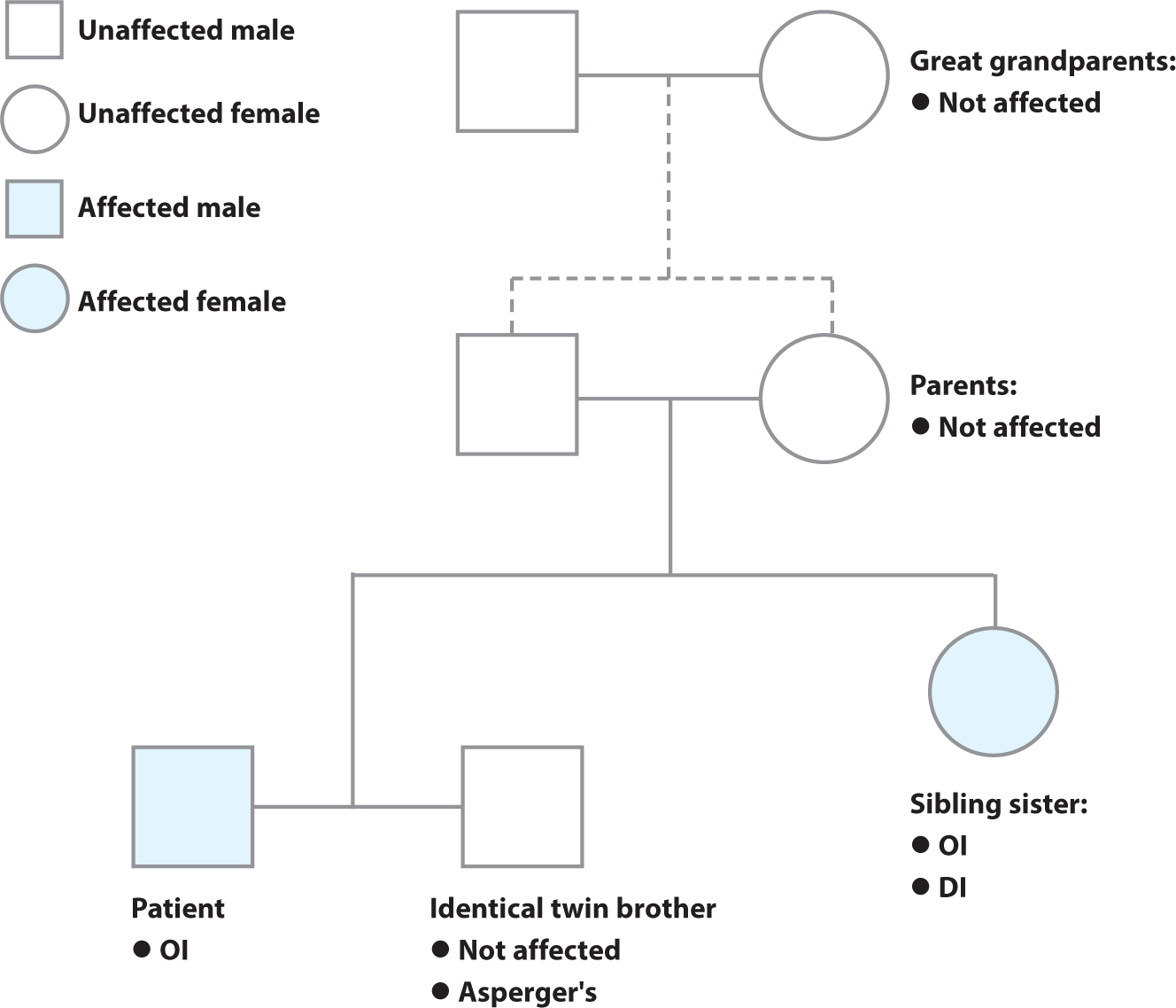
Figure 1. Family tree of the patient, showing consanguinity of his parents. AD: autosomal dominant; OI: osteogenesis imperfecta; DI = dentinogenesis imperfecta.Figure 2. Signs and symptoms of medication-related osteonecrosis of the jaw.13
Case report
A 12-year-old male patient presented to the Orthodontic Department of The Royal London Dental Hospital, following a referral from his general dental practitioner, with concerns regarding crowding and the aesthetics of his upper teeth. His medical history included type 1 OI, which was diagnosed at the age of 11 following a history of recurring bone fractures. No other comorbidities were recorded.
The patient received intravenous bisphosphonate infusions of pamidronic acid every 6 months following diagnosis, and this treatment was likely to continue for the foreseeable future. Additionally, the patient had regular bone density scans to review his response to treatment.
Relevant family history included that the patient's parents were consanguineous (Figure 1). The patient also had two siblings; the patient's younger sibling had a similar diagnosis, having been diagnosed at 4 years of age and was also undergoing a similar intravenous bisphosphonate infusion. The patient's twin did not have OI.
Clinical examination revealed a Class III incisor relationship on a Class III skeletal base. The patient had competent lips and an average Frankfort mandibular plane angle. There was a partially restored dentition with good oral hygiene. The patient had a Class II molar relationship bilaterally; half a unit on the right and a quarter unit on the left. Severe crowding was recorded in the upper labial segment and moderate crowding in the lower labial segment. The upper centre line was in line with the midfacial axis and there was a 2 mm displacement of the lower centre line to the right. Figures 3–6 show the occlusion at initial presentation. Radiographic examination revealed unerupted third molar teeth in each quadrant.
Figure 3. Intra-oral right side view.Figure 4. Intra-oral left side view.Figure 5. Intra-oral view of upper arch.Figure 6. Intra-oral frontal view.
The following treatment options were discussed with the patient and his parents:
Monitor and review;
Orthodontic treatment alone to align the upper anterior teeth and improve aesthetics, while accepting the palatally excluded UL2;
Orthodontic and oral surgery treatment with extractions of teeth to facilitate relief of crowding;
Orthodontic and orthognathic treatment to correct skeletal discrepancy and comprehensively address the malocclusion.
Owing to the patient's history of intravenous bisphosphonate medication, certain potential complications needed to be taken into consideration including the risk of MRONJ after extraction, and also the risk of compromised orthodontic tooth movement.
The patient's endocrinologist was also consulted with respect to the treatment options before making a final decision with the patient regarding definitive treatment. Even though the risk of MRONJ was considered low, its potential consequences were still taken into account because of the potential detrimental impact on the patients' quality of life.
The ideal treatment plan would have been to carry out extractions to create space in all four quadrants, followed by fixed orthodontic appliances with or without orthognathic surgery to correct the skeletal discrepancy. However, considering the risks for this patient, a more conservative treatment plan was proposed with the aim of addressing the patient's main aesthetic concern and minimizing any potential complications. The treatment plans were discussed with both the patient and the parents, and an informed decision was made to proceed with a more conservative treatment option.
Following a period of monitoring growth and development, a staged treatment plan was formulated, with the first stage involving bonding orthodontic brackets to the upper arch, excluding the lateral incisors. This was to assess whether the teeth were amenable to orthodontic tooth movement and was evaluated over a 4-month period, with no adverse effects noted.
Following this, the upper lateral incisors were extracted. The lateral incisors were chosen as the ideal tooth for removal in this case because of their initial displacement, the amount tooth movement required after extraction to close the space, and the location of space relative to the upper arch crowding. This meant they were the preferred option for optimizing treatment success and minimizing any effects of extended orthodontic movement, such as root resorption and residual spacing.
These extractions were completed under local anaesthetic at separate appointments. Periods of 4 weeks after each procedure allowed for assessment of the healing response. With the exception of pre-operative 0.2% chlorhexidine mouthwash, no additional preventative measures were prescribed and healing was uneventful.
Once the sockets had healed, the second stage of treatment commenced. It involved continuing with fixed orthodontic appliances in the maxillary arch only because this was the main area of concern for the patient. Alignment of the maxillary arch was successful, taking an average of 2 years to complete. No mandibular extractions were required because no lower arch treatment was proposed at this stage.
While this did not produce the ideal occlusion or alignment, the patient was very pleased with the post-operative results, experiencing no signs of MRONJ and the treatment was therefore deemed a success. Post-operative photographs (Figures 7,8,9,10) show the improved aesthetics following this limited treatment.
Figure 7. Intra-oral right side view.Figure 8. Intra-oral left side view.Figure 9. Intra-oral view of upper arch.Figure 10. Intra-oral frontal view.
Discussion
OI is a connective tissue collagenous disorder, primarily caused by an autosomal dominant gene. Of all OI cases, 90% present with mutations to the type 1 collagen genes: COL1A1 and COL1A2.7,8 Mutations to these genes result in abnormal collagen crosslinking. These genes may be inherited or may spontaneously mutate. Therefore, children with no family history of OI can develop the condition, as was the situation in this case. Approximately 10–15% of all cases are due to an autosomal recessive gene, and consanguinity increases the risk of OI.7
Clinical presentations vary depending upon subtype and the individual.9 Type 1 collagen is a major protein in bone production and therefore, the majority of clinical manifestations present in bone: bones are considered brittle and have a tendency to break. Although they can heal, they cannot remodel correctly and this predisposes them to bowing or other malformations.1,9 Other orthopaedic presentations include short stature, joint hypermobility and scoliosis.9 Non-orthopaedic presentations include: blue sclera; myopia; astigmatism; hearing loss; hypermetabolism (increasing the risk of malignant hyperthermia); mitral valve regurgitation; aortic prolapse; and increased bleeding tendencies.10
Various orofacial abnormalities are associated with OI and include dysmorphic triangular faces with broad foreheads, macrocephaly, class III malocclusion, anterior and posterior openbite, crossbite, dentinogenesis imperfecta, ectopic teeth and susceptibility to caries and tooth surface loss.5,9,10 Additionally, there may be difficulty with patient positioning during dental treatment because of orthopaedic abnormalities and dental anxiety.5,9 Teeth often show signs of obliterated pulp chambers, short and thin roots and discolouration of the crown.5
A fracture history and a low bone mineral density tested with dual-energy X-ray absorptiometry (DEXA) alone are often sufficient to diagnose OI in children. Clinicians should have a high suspicion in patients with a family history of OI. A bone biopsy and radiographs are additional diagnostic methods that are less commonly employed. Genetic testing can assist in diagnosis and identification of the inheritance pattern and the risk of subsequent siblings being affected.11 Genetic counselling may be offered to patients and parents of patients affected by OI who may be planning for a family.
Common treatments include physical therapy, surgical intervention and medications. The most common medical treatment for OI is IV bisphosphonate infusions.12 Since their introduction, bisphosphonates have greatly reduced the incidence of bone fractures. However, they also have an undesirable effect on oral health and dental treatment with an increased risk of MRONJ, delayed exfoliation of teeth and slower orthodontic tooth movement in these patients.13
MRONJ can occur spontaneously, but generally, there is an increased risk after dental procedures involving bone.13,14 The general incidence of MRONJ in patients treated with IV bisphosphonates ranges from 0.001% to 1%.14 Patients are often considered high or low risk depending on the method of administration, the treatment received and the duration of treatment.14 As in the case reported above, patients who have been on intravenous bisphosphonates for over 5 years at the time treatment options are considered are classified as being high risk for developing MRONJ post-surgery.
The manifestation of MRONJ in adults receiving IV bisphosphonates following dental extractions is well reported;14 however, there have been no reported cases to date of MRONJ in children under similar circumstances.15 Brown et al revealed that of 42 children who were having bisphosphonate therapy and undergoing dental extractions, no cases of MRONJ were reported post operatively.15 Additionally, Chahine et al found no cases of MRONJ after dental extractions in 278 children receiving bisphosphonates.16 Other studies have reported no evidence of MRONJ after dental extractions in children being treated for OI specifically with IV bisphosphonates.17,18,19
Although the evidence for MRONJ in children is sparse, there is still a potential risk. Current guidelines in the UK for patients undergoing an oral surgery procedure while receiving bisphosphonate therapy have limited information pertaining to children.14 Guidelines released by the Australian Dental Association cover a number of treatment considerations to minimize potential MRONJ risks in children while undergoing oral surgery procedures; these are summarized in Table 2.13 These guidelines can be used to assist management of patients with OI, although the evidence for this is not clear. In this case the multidisciplinary consensus was that the risk of having peri-operative antibiotics outweighed their potential benefits and therefore, the only prophylactic medication administered was a single pre-operative dose of chlorhexidine 0.2% mouthwash.
Timing
Techniques
Prior to therapy
Comprehensive dental assessment
Clinical
Radiographic
Patient and parent education
Oral hygiene advice
Dietary advice
Ideally invasive dental treatment completed
Bisphosphonates postponed for 3 weeks after this
During therapy
Regular dental reviews
Reinforce oral hygiene and dietary advice
Emergency dental treatment should not be delayed
Oral surgery treatment
Delay elective treatment if infusion for a short term
Timing of treatment for as long after last infusion
Allow 3 weeks for healing before next infusion is administered
Chlorhexidine 0.2% mouthwash prophylactically
Conservative surgical technique
Primary closure if possible
Periodic review of socket after extraction
Prophylactic antibiotics in patients with the highest risk of developing MRONJ
Bisphosphonate medications inhibit bone resorption and, therefore, it is understandable that effects on exfoliation and eruption may be observed. Patients receiving bisphosphonate medications have been shown to have delayed dental exfoliation and an increased dental chronological age by up to 1.5 years.20 In addition, infra-occlusion in the primary dentition has been shown to be increased by up to 27% in patients undergoing bisphosphonate therapy.21 Delayed dental eruption was also observed in 12.5% of patients.21
Bisphosphonate use can also affect orthodontic treatment by reducing the rate of orthodontic tooth movement.22 Bisphosphonates affect osteoclastic and osteoblastic activity (inhibition), therefore making tooth movement more difficult and resulting in longer treatment times.24 Despite the well-known orthodontic disadvantages, attempts have been made in recent years to improve anchorage by local deposition of bisphosphonates around teeth.25 Other theoretical potential benefits include reduced root resorption and reduced relapse potential.12 In the case presented above, tooth movement took twice as long as expected, which mirrors the findings in the literature regarding the effect of bisphosphonates on orthodontic tooth movement.
Methods employed to reduce the incidence of the negative effects of bisphosphonate therapy in this case included:
Limiting the number of tooth extractions and other oral surgery procedures;
Unavoidable oral surgery procedures were completed as atraumatically as possible;
Oral surgery procedures were closely followed up to assess for healing before proceeding with further procedures/infusions;
Avoidance of orthognathic surgical procedures;
Limiting the amount of orthodontic tooth movement required.
Owing to the potential risks from IV bisphosphonates, a compromised treatment plan was formulated with a reduced extraction pattern being favoured, and this only commenced when some orthodontic tooth movement had already been accomplished. In similar instances, it is important to communicate the likely outcomes, as well as the uncertainties, to the patient and document this clearly.
Overall, the patient received an aesthetically pleasing result and was very satisfied with the outcome, having had his upper labial segment crowding addressed. If the patient became concerned about the appearance of the canines in the lateral incisor position, restorative intervention in primary care using adhesive resin composite to lateralize the canine teeth could be considered, and this was discussed with him at the start.
Conclusion
This patient presented with a treatment planning dilemma due to the unknown risk of IV bisphosphonate therapy on orthodontic and oral surgery treatment in an adolescent, both of which were fundamentally elective in nature. An alternative treatment plan was subsequently formulated to address the patient's concerns, while also considering the potential risks and benefits to the patient and their expectation of treatment, and centred upon the limited information available in the literature. Although we did not achieve the ‘ideal’ occlusion or aesthetic result, no MRONJ was caused by the treatment, the patients concerns were satisfactorily addressed and he was pleased with the result. Ultimately, we must continually revisit our understanding of success and the aims of our treatments, and take into account the patient's perspective: are we aiming for academic definitions of success and ideal occlusions, or are we aiming for patient satisfaction?