Song F, O'Meara S, Wilson P The effectiveness and cost-effectiveness of prophylactic removal of wisdom teeth. Health Technol Assess. 2000; 4:1-55
Huang GJ, Cunha-Cruz J, Rothen M A prospective study of clinical outcomes related to third molar removal or retention. Am J Public Health. 2014; 104:728-34 https://doi.org/10.2105/AJPH.2013.301649
McArdle LW, McDonald F, Jones J Distal cervical caries in the mandibular second molar: an indication for the prophylactic removal of third molar teeth?. Update. Br J Oral Maxillofac Surg. 2014; 52:185-189 https://doi.org/10.1016/j.bjoms.2013.11.007
Renton T, Al-Haboubi M, Pau A What has been the United Kingdom's experience with retention of third molars?. J Oral Maxillofac Surg. 2012; 70:(9 Suppl 1)S48-57 https://doi.org/10.1016/j.joms.2012.04.040
Renton T, Hankins M, Sproate C, McGurk M A randomised controlled clinical trial to compare the incidence of injury to the inferior alveolar nerve as a result of coronectomy and removal of mandibular third molars. Br J Oral Maxillofac Surg. 2005; 43:7-12 https://doi.org/10.1016/j.bjoms.2004.09.002
Matzen LH, Wenzel A Efficacy of CBCT for assessment of impacted mandibular third molars: a review – based on a hierarchical model of evidence. Dentomaxillofac Radiol. 2015; 44 https://doi.org/10.1259/dmfr.20140189
Araujo GTT, Peralta-Mamani M, Silva AFMD Influence of cone beam computed tomography versus panoramic radiography on the surgical technique of third molar removal: a systematic review. Int J Oral Maxillofac Surg. 2019; 48:1340-1347 https://doi.org/10.1016/j.ijom.2019.04.003
de Toledo Telles-Araújo G, Peralta-Mamani M, Caminha RDG CBCT does not reduce neurosensory disturbances after third molar removal compared to panoramic radiography: a systematic review and meta-analysis. Clin Oral Investig. 2020; 24:1137-1149 https://doi.org/10.1007/s00784-020-03231-6
Clé-Ovejero A, Sánchez-Torres A, Camps-Font O Does 3-dimensional imaging of the third molar reduce the risk of experiencing inferior alveolar nerve injury owing to extraction? A meta-analysis. J Am Dent Assoc. 2017; 148:575-583 https://doi.org/10.1016/j.adaj.2017.04.001
Petersen LB, Olsen KR, Christensen J, Wenzel A Image and surgeryrelated costs comparing cone beam CT and panoramic imaging before removal of impacted mandibular third molars. Dentomaxillofac Radiol. 2014; 43 https://doi.org/10.1259/dmfr.20140001
Lecomber AR, Downes SL, Mokhtari M, Faulkner K Optimisation of patient doses in programmable dental panoramic radiography. Dentomaxillofac Radiol. 2000; 29:107-112 https://doi.org/10.1038/sj/dmfr/4600513
The unilateral sagittal split osteotomy: A useful tool in the armamentarium for deeply impacted mandibular third molars Ross Leader Ashwin Kerai Laura Wade David Houghton Dental Update 2025 51:7, 490-494.
The unilateral sagittal split osteotomy may not be a particularly popularized method to access and remove impacted mandibular third molars (M3Ms). However, in unusual cases of deep impaction, it can provide a surgical option that minimizes bone removal and may reduce the risk of iatrogenic mandibular fracture and inferior alveolar nerve (IAN) injury, depending on the position of the third molar relative to the neurovascular bundle.
CPD/Clinical Relevance:
The unilateral sagittal split osteotomy may present an alternative method for removing impacted mandibular third molar teeth in certain situations.
Article
Mandibular third molar surgery is collectively one of the most common surgical procedures performed in secondary care.1 The unilateral sagittal split osteotomy is perhaps not a very well popularized method to access and remove impacted mandibular third molars (M3Ms). However, in unusual cases of deep impaction, it can provide a surgical option that minimizes bone removal and may reduce the risk of iatrogenic mandibular fracture and inferior alveolar nerve (IAN) injury, depending on the position of the third molar relative to the neurovascular bundle. With this in mind, we present a clinical case managed via this approach, and discuss the evidence base around imaging for impacted mandibular third molars (M3Ms) and the latest guidelines for their extraction.
Case history
A 62-year-old male of European origin was referred to the on-call oral and maxillofacial surgery core trainee via accident and emergency (A&E) with a 2-day history of discomfort and swelling to the right submandibular region. He was assessed initially with a provisional diagnosis of right submandibular gland sialadenitis and discharged with a 5-day course of amoxicillin and metronidazole. The patient was booked for follow up on the maxillofacial clinic 2 weeks later. At that review, signs and symptoms had settled and cone beam computed tomography (CBCT) was ordered to determine the position of the inferior alveolar nerve as the lower right third molar was felt to be the primary cause on review of the orthopantogram (OPG) (Figure 1).
Figure 1. Pre-operative orthopantomogram.
The patient attended a further review clinic for discussion of the CBCT findings. The patient recalled the symptoms at his initial visit as a dull ache to the right posterior mandible, radiating under the angle of his mandible and into his neck. He also reported a current paraesthesia of 50% in the distribution of the right IAN.
His past medical history included essential hypertension with a regular prescription of indapamide (2.5 mg once daily) and he also took cod liver oil, ginseng and garlic capsules over the counter. He reported no known drug allergies. He was an ex-smoker having quit 30 years previously with a 10-year pack history, and consumed 20 units of alcohol per week. On examination, there was no extra-oral swelling or lymphadenopathy, the oral soft tissues were unremarkable, the LR8 was not visible in the mouth and the LR7 and LR6 were grade 1 mobile.
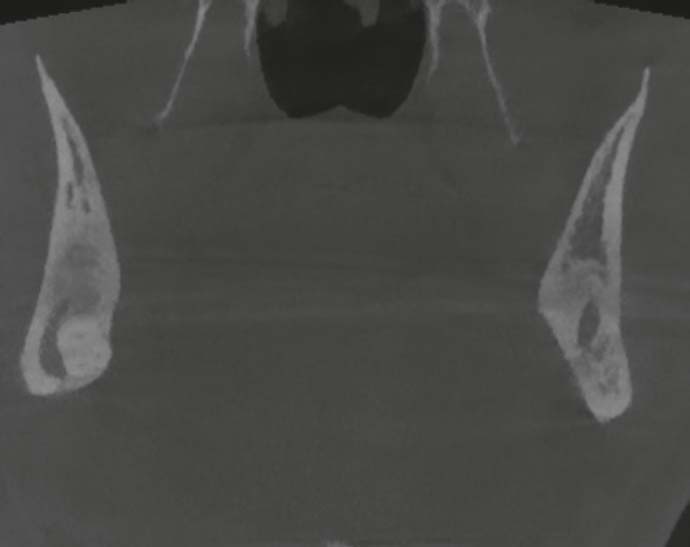
The OPG demonstrated a deeply impacted mesio-angular LR8 with evidence of internal resorption, and darkening of the root of the LR8 indicating close proximity to the ID canal (Figure 1). CBCT confirmed the above and buccal apposition of the inferior alveolar nerve with no intervening bone (Figure 2). Given this, the option of an extra-oral transcervical approach to remove the tooth would have carried with it a significant risk of permanent IAN injury as well as a scar, and the risk of temporary and permanent facial weakness due to the potential for injury to the marginal mandibular branch of VII.
Figure 2. Pre-operative CBCT (coronal slice) showing no bony apposition between the roots of LR8 and the IAN.
Subsequently an in-depth discussion with the patient regarding management options was undertaken. This included extraction of the tooth via a sagittal split versus an active surveillance approach. Despite the patient's initial resolution in symptoms with non-surgical management, it was stressed that recurrent infection would continue to be a significant possibility. The patient opted for active surveillance with periodic review as he was concerned at the risk of permanent anaesthesia should he have the tooth removed.
Five months later, the patient was admitted with a large right-sided submandibular swelling and trismus of 20 mm. He was initially managed with intravenous fluids, antibiotics (amoxicillin and metronidazole), and dexamethasone before undergoing acute surgical intervention, which involved incision, exploration and drainage of the right submandibular abscess and insertion of an extra-oral drain into the submandibular space. Following clinical improvement, the patient was discharged 2 days later.
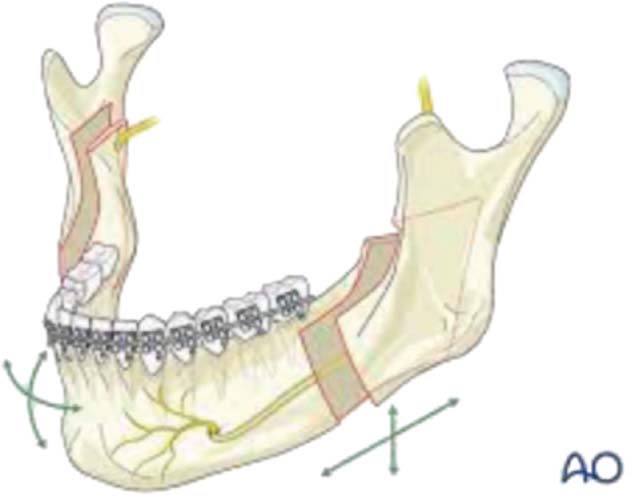
An elective admission was arranged 3 weeks later for removal of the tooth following further discussion regarding management options. A standard intra-oral trans-alveolar approach to remove the impacted LR8 would have resulted in a significant amount of bone removal, increasing the risk of mandibular fracture and placing the IAN at an unnecessarily high risk of injury. In light of this, a unilateral sagittal split osteotomy of the right mandible (Table 1 and Figure 3) under general anaesthesia was used to access the LR8. The impacted LR8 was elevated with the neurovascular bundle intact. The decision was taken to preplate the mandible prior to splitting the jaw to ensure that the bone could be re-fixed in its pre-operative position, so as not to alter the occlusion. This plate was removed prior to the split then subsequently re-applied and secured with 4 x 6 mm monocortical screws once the tooth had been removed.
Year
Development of the sagittal split osteotomy
1957
Obwegeser and Trauner: first description of the procedure
1961
Dal Pont modification: vertical buccal osteotomy between 6/7, allowing for greater surface area of contact between the cut bone
1968
Hunsuck modification: shorter medial cut, just distal to the lingula, minimizing soft tissue dissection
1977
Epker modification: proposed less stripping of the masseter to preserve blood supply to the mandible and reduce bone resorption at the gonial angle
Figure 3. Schematic of bilateral sagittal split osteotomy cuts. Courtesy of the AO Surgery Reference Catalogue.
He was subsequently discharged 2 days post-operatively with a degree of paraesthesia in the distribution for the right IAN (70%). Since discharge, he underwent three clinical reviews: post-operative swelling had resolved, there were no signs of residual infection, paraesthesia had much improved (now 10%) and his occlusion was unchanged. The post-operative OPG can be seen in Figure 4. The operating surgeons confirm that the entire tooth was removed and the radioopacity at the site of surgery on the post-operative OPG is consistent with localized osteosclerosis, from the recurrent acute-on-chronic infective episodes.
Figure 4. Post-operative orthopantomogram.
Guidelines on the removal of M3Ms
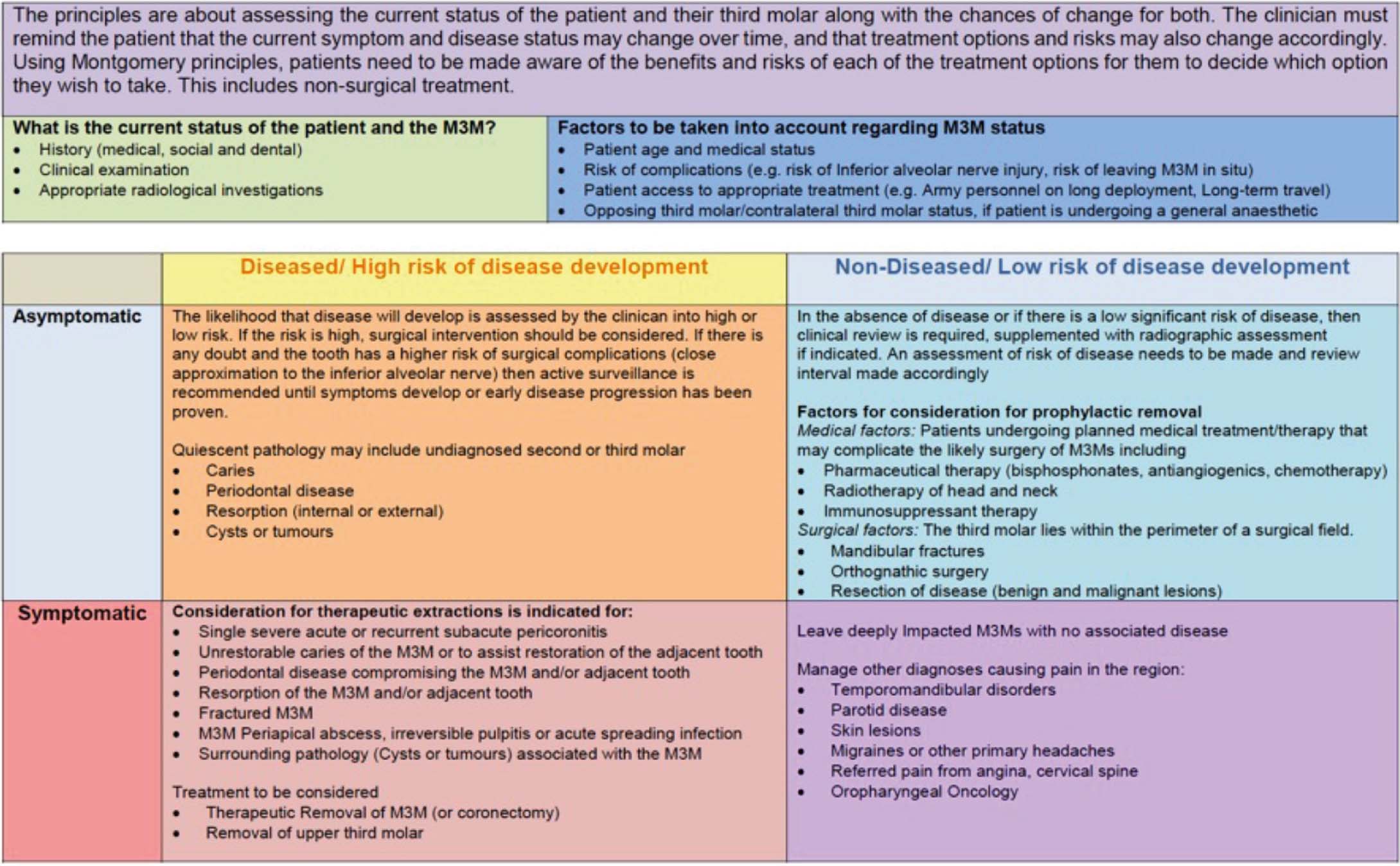
The National Institute for Health and Care Excellence (NICE) produced guidelines related to the removal of mandibular third molars (M3Ms) in 2000.2 This document discouraged the prophylactic removal of M3Ms.2,3 Since then, growing evidence has suggested that this may only delay their inevitable removal, and, as such, may not be the most sensible approach to the management of M3Ms in all cases.3,4,5,6,7 This prompted review of the evidence by the Faculty of Dental Surgery (FDS), the Royal College of Surgeons England, with the production of new guidance in 2020 (Figure 5).8 The emphasis of these guidelines is to provide a more holistic and patient-centred approach, and it is expected that these will, with time, supersede those produced by NICE.
Figure 5. Summary of the management of patients with M3Ms. Courtesy of RCSEng.8
CBCT: what's the evidence base for its use in the management of M3Ms?
Consistency in radiographic choices in the cross-specialty planning of surgical management of M3Ms is an important topic. Bearing in mind the stochastic effects of radiation, all prescriptions must be as low as reasonably practicable while providing the requisite information to facilitate decision making. A comparison of radiation dosages for the common modes of imaging can be seen in Table 2.
Imaging modality
Radiation dose (mSv)
OPG
0.002–0.003
Dento-alveolar CBCT
0.01–0.67
Craniofacial CBCT
0.03–1.1
Medical CT (mandible)
0.25–1.4
The Faculty of General Dental Practice provided selection criteria on the pre-operative imaging choices for M3Ms,9 which advocate pre-extraction radiographs for teeth that are impacted, buried or likely to have a close relation to important anatomical structures. For M3Ms, it is implied that this is achievable with an OPG.
A randomized controlled trial by Renton et al comparing the incidence of injury to the inferior alveolar nerve (IAN) as a result of coronectomy versus removal of M3Ms demonstrated that on OPG, diversion of the inferior alveolar canal, darkening of the root where crossed by the canal, and interruption of the white lines of the canal were associated with a significantly increased risk of inferior alveolar nerve injury (Table 3).10 Considering this, it can be theorized that the more detailed multi-dimensional CBCT imaging can allow for more meticulous surgical planning in terms of bone removal, sectioning, elevator placement, and direction of root delivery, and therefore, reduce the risk of neuropraxia and neurotmesis. Indeed, a review by Matzen et al showed that interruption of the white line of the inferior alveolar canal and darkening of the roots on OPG predicted contact between the root and canal on subsequent CBCTs in 23–56% of cases.11 However, these signs of proximity seen on CBCT do not appear to be any more predictive of inferior alveolar nerve injury than those seen on OPG alone.11 This has been corroborated by a further systematic review by Araujo et al, which concluded that OPG alone is enough to decide between surgical extraction or coronectomy.12 More recent systematic reviews have also concluded that pre-operative CBCT does not reduce the risk of IAN injury compared to OPG alone.13,14
Diversion of the inferior dental canal
Darkening of the root where it is crossed by the ID canal
Interruption of the white lines of the ID canal
The 2020 RCSEng guidelines8 took the above into consideration and gave a strong recommendation, based on evidence from meta-analyses, that the current evidence suggests that pre-operative CBCT has no effect on reducing inferior alveolar nerve (IAN) injury. They also state that the financial15 and radiation burden16 outweigh that of conventional OPG, and hence, CBCT should only be considered in carefully considered cases with the IAN in close apposition to the M3M, where findings are felt to alter management decisions.17 However, the three-dimensional CBCT could be argued to better facilitate discussions when considering Montgomery consent and when planning for a unilateral sagittal split osteotomy.
Conclusion
This case provides an example of where a unilateral sagittal split osteotomy can be an appropriate surgical method used to facilitate the removal of an impacted M3M. It is hoped that this article provides a guide as to when a unilateral sagittal split osteotomy is appropriate, a point of direction to the 2020 Royal College of Surgeons England guidelines on the management of M3Ms and choice of imaging.
Learning points
The unilateral sagittal split osteotomy is a safe option to access deeply impacted third molars requiring removal. It provides an option that preserves bone, reduces mandibular fracture and potentially the risk of IAN injury.
Pre-plating the mandible is one option that allows for correct anatomical repositioning of the bony cuts, and maintaining the pre-operative occlusion.
Always consider deeply impacted M3Ms as a cause for recurrent pain and swelling in the submandibular triangle, especially when associated with resorptive pathology of the tooth.
The latest RCSEng guidelines have given a strong recommendation, based on evidence from meta-analyses, that pre-operative CBCT has no effect on neurosensory disturbance, and should only be considered in carefully considered cases, where findings are felt to alter management decisions.
It is expected that the Royal College of Surgeons England guidelines in the management of mandibular third molars will supersede those produced by NICE.