Rodd HD, Graham A, Tajmehr N Molar incisor hypomineralisation: current knowledge and practice. Int Dent J. 2021; 71:285-291 https://doi.org/10.1111/idj.12624
Mathu-Muju K, Wright JT Diagnosis and treatment of molar incisor hypomineralization. Compend Contin Educ Dent. 2006; 27:604-610
Patel S, Ashley P, Noar J Radiographic prognostic factors determining spontaneous space closure after loss of the permanent first molar. Am J Orthod Dentofacial Orthop. 2017; 151:718-726 https://doi.org/10.1016/j.ajodo.2016.09.018
Saber AM, Altoukhi DH, Horaib MF Consequences of early extraction of compromised first permanent molar: a systematic review. BMC Oral Health. 2018; 18 https://doi.org/10.1186/s12903-018-0516-4
Kupietzky A Correction of ectopic eruption of permanent molars utilizing the brass wire technique. Pediatr Dent. 2000; 22:408-412
Borrie FRP, Bearn DR, Innes NPT, Iheozor-Ejiofor Z Interventions for the cessation of non-nutritive sucking habits in children. Cochrane Database Syst Rev. 2015; 2015 https://doi.org/10.1002/14651858.CD008694.pub2
Haryett RD, Hansen FC, Davidson PO, Sandilands ML Chronic thumb-sucking: the psychologic effects and the relative effectiveness of various methods of treatment. Am J Orthod. 1967; 53:569-585 https://doi.org/10.1016/0002-9416(67)90069-3
Phillips JM, McCann CT, Welbury R Endodontic management of traumatised permanent anterior teeth. Prim Dent J. 2020; 9:37-44
Sandler C, Al-Musfir T, Barry S Guidelines for the orthodontic management of the traumatised tooth. J Orthod. 2021; 48:74-81 https://doi.org/10.1177/1465312520977498
Patel K, Mack G, Djemal S Management of acute traumatic dental injuries in the orthodontic patient. Br Dent J. 2022; 232:695-700 https://doi.org/10.1038/s41415-022-4244-4
González OL, Vera J, Orozco MS Transient apical breakdown and its relationship with orthodontic forces: a case report. J Endod. 2014; 40:1265-1267 https://doi.org/10.1016/j.joen.2014.01.006
Bourguignon C, Cohenca N, Lauridsen E International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent Traumatol. 2020; 36:314-330 https://doi.org/10.1111/edt.12578
The orthodontic–paediatric interface ensures that children are assessed and managed by the right people, in the right place, at the right time. This two-part series offers general dental practitioners (GDPs) and specialists an update on common joint orthodontic–paediatric problems in the mixed dentition alongside practical considerations to resolve them. The first paper will focus on: management of compromised first permanent molars, extraction of primary teeth and subsequent space maintenance, management of habits and possible sequelae, and orthodontic management of dental trauma.
CPD/Clinical Relevance: This series will enable GDPs to recognize and manage common problems in primary care, while also increasing knowledge regarding the optimal time for referral to specialist care.
Article
The impact of dental decisions made during childhood and adolescence have the potential to last a lifetime.1 Therefore, input and management of issues in the mixed dentition by paediatric dentists and orthodontists, is crucial in ensuring the best outcome when treating a developing malocclusion.
Close collaboration between orthodontics and paediatric dentistry is commonplace in secondary care, both on a daily basis, but more exclusively during multidisciplinary clinics. Such clinics enable direct discussion between clinicians and families to address all aspects of any proposed management plan. This close-working relationship has been key to effectively and efficiently managing patients for decades, however, it also allows for liaison with referring general dental practitioners (GDPs), who will be regularly seeing the patient during a long-term course of treatment.
It is important that GDPs are able to manage common issues, as well as recognize abnormal development and refer patients when appropriate, hence this article provides an update on common joint orthodontic–paediatric problems in the mixed dentition and their possible solutions.
First permanent molars
First permanent molars (FPMs) are often the subject of concern during dental development. They are one of the first permanent teeth to erupt into the oral cavity and their early presence can increase their vulnerability for caries, hence it is no surprise that they are the most commonly filled tooth in the adult dentition.2 Additionally, their stage of development can make them more vulnerable to the effects of maternal and systemic illness, medications and environmental factors.3
Molar–incisor hypomineralization (MIH)
Molar–incisor hypomineralization (MIH) is a common condition and is estimated to affect up to 14.3% of the children worldwide, while in the UK around one in eight are affected, equating to around 1 million children.4,5 MIH can be defined as: ‘hypomineralization of systemic origin, presenting as demarcated, qualitative defects of enamel of one to four first permanent molars frequently associated with affected incisors.’6
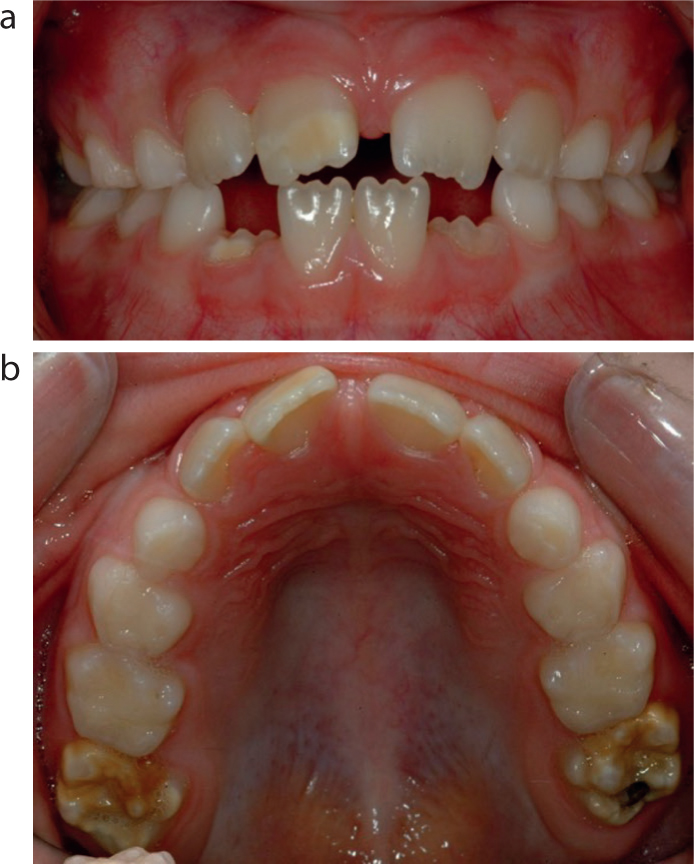
There is a continuum of severity in relation to MIH, with some teeth mildly affected, while others experience post-eruptive breakdown (PEB) of the molars and white and/or brown hypomineralized lesions on the incisor teeth (Figure 1).
Figure 1. (a) 7-year-old child in the early-mixed dentition with MIH, showing well-demarcated, creamy white-yellow opacities on the UR1 and partially erupted LR2. (b) The same 7-year-old child with visible post-eruptive breakdown of the upper first permanent molar teeth, typical of MIH. Caries is noted occlusally on the UR6.
The timely management of MIH can be useful to reduce the potential consequences of loss of the first permanent molars. Additionally, clinical guidelines exist for the management of poor-prognosis first permanent molars in relation to the malocclusion.7
When considering the management of affected first permanent molars, the extent and severity of the defects is important to take into account alongside other wider patient factors: a simple way to consider these factors is with the acronym ‘M-O-R-S-E C-O-D-E’ (Table 1). Teeth with affected load-bearing surfaces, or with areas of post-eruptive breakdown affecting multiple surfaces with or without cuspal involvement, would be considered to represent increased severity.8 Additionally, if the patient is experiencing symptoms with the tooth or rapid caries progression, treatment may be required earlier than the ideal time. Patient cooperation is important to consider because general anaesthetic may require a more comprehensive and invasive plan, to avoid the risk of repeat general anaesthetics. Future orthodontic needs require careful thought prior to extraction of poor prognosis molars. The severity of crowding or an increased overjet may require retention of the first permanent molar in some cases until the second permanent molar erupts, although in severe cases, extraction at an ideal time followed by a future premolar extraction may be required. In the former case, an appliance to aid in space maintenance, such as a removable appliance or transpalatal arch, could be fitted prior to extraction. At an early age, decisions with regards to the need for growth modification treatment, for example twin block or protraction facemask treatment, can be challenging. However, if the teeth are asymptomatic, these cases may require first permanent molars for retention of removable or fixed appliances and therefore extraction of these may be delayed to facilitate this.
Table 1. Considerations for the management of compromised first permanent molars.
Consideration
Questions
Malocclusion
Does the patient have an increased overjet and/or significant crowding?Does the patient have any developmentally absent teeth?Is there a severely ectopic tooth in the same quadrant?Is there a second poor prognosis tooth in the same quadrant?
Opposing contacts
Does the opposing tooth have an occlusal contact to prevent future overeruption?
Restorability
Is the tooth restorable?What is the likely long-term prognosis of the tooth?
Sevens (second permanent molars)
What is the stage of development of the second permanent molars on the orthopantomogram (OPT)?
Eights (third permanent molars)
Are there third permanent molars developing on the OPT?
Crown of the second premolar
Is the crown of the developing second premolar positioned within the roots of the deciduous second molar?
Orthodontic treatment plan
What is the likely orthodontic treatment modality?When is the optimal timing for orthodontic treatment?Do they require a functional appliance?
Dental symptoms
Does the tooth or teeth hurt?Is there reported sensitivity?Are there any visible abscesses or sinuses?
Experience of dental treatment
Has the patient had any previous dental treatment?If extractions are required, what is the likely treatment modality?Is the child dentally anxious?
The malocclusion also needs to be taken into account because compensating extractions, whereby the same tooth in the opposing arch (usually a maxillary first permanent molar) is extracted to increase the chance of spontaneous space closure, although this is no longer considered routine practice.7 In some cases, for example Class II malocclusions, there may be a sufficient occlusal stop to prevent overeruption of the tooth, which could otherwise prevent spontaneous space closure in the lower arch, therefore it should be assessed on a case-by-case basis.
Consideration to maintaining the first permanent molar may be needed if the patient presents with hypodontia or severely ectopic teeth within the same quadrant because this could result in reduced occlusal stability and increased need for restorative intervention owing to spacing. If this is the case, it would be imperative to seek a specialist paediatric or orthodontic opinion.
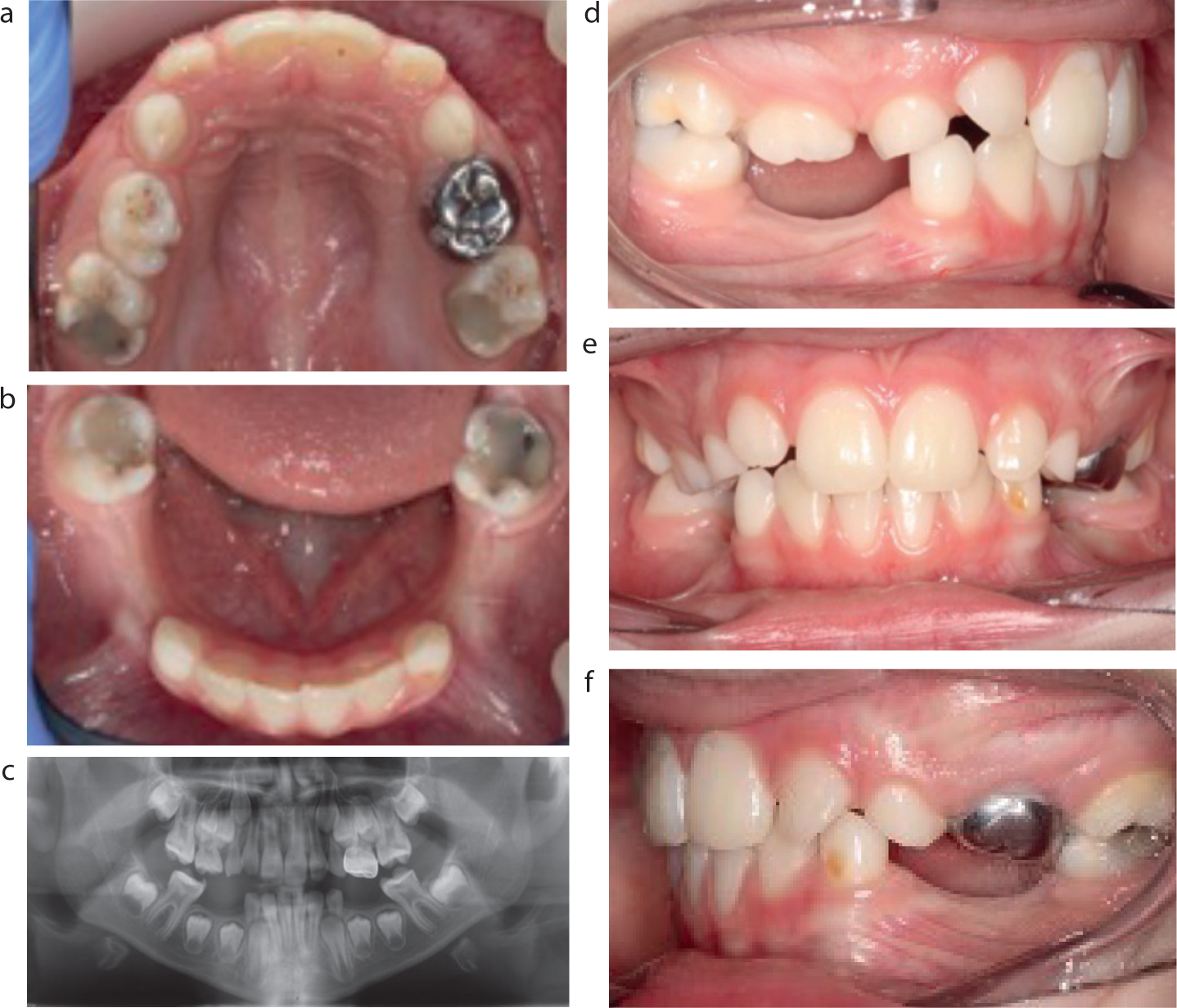
When aiming for spontaneous space closure following extraction of the first permanent molar, a number of factors have been shown to be positive prognostic factors in terms of timing of extraction. Recent evidence has shown the presence of the third molars and the angulation of the second molar are potentially more important in predicting spontaneous space closure.9 Saber and colleagues also described prognostic factors for spontaneous space closure and the importance of the position of the second premolar in the bifurcation of the second deciduous molar in addition to those described above.10 Unfortunately, delayed or early extraction can result in unfavourable tipping, rotation and incomplete space closure.7 The considerations to be made prior to extracting first permanent molar teeth are described in the recently updated guidelines by the Royal College of Surgeons of England.7Figure 2 provides an example of how the aforementioned factors can be considered to form a treatment plan for patients in this position.
Figure 2. (a–f) An 8-year-old child with poor prognosis FPMs and Class I occlusion. Using ‘MORSECODE,’ the key features of relevance are: Class I occlusion complicated by potentially severe upper arch crowding; large existing restorations on all four FPMs affect their long-term prognosis; lower 7s are immature and behind the ideal time for spontaneous space closure in lower arch; no clear-cut, obvious sign of 8s on OPT, but patient is only 8 years old and they could yet develop; will be likely to need later orthodontic treatment to address crowding (upper arch crowding that is likely to involve extractions); currently asymptomatic; had previous extractions and restorations. Possible options include the following:Maintain all four FPMs until upper 7s have erupted and then consider their removal to address upper arch crowding. This can be combined with reinforcing anchorage, e.g. placing a transpalatal arch using the upper 7s.Consider extractions of all four FPMs (will need to delay this slightly until lower 7s have reached bifurcation stage), aiming for spontaneous space closure in the mandibular arch. Patient will be likely to need a removal of two further units in the upper arch to address crowding later on.
Impacted first permanent molars
First permanent molars can become impacted against the second deciduous molars. Previous literature quotes a prevalence of 2–6%, with increased presentation in the maxillary arch compared to the mandibular arch.11 This can be a result of: unusually large deciduous molars; ill-fitting preformed metal crowns used to restore carious primary second primary molars; mesial eruption direction; lack of arch length; uncoordinated growth; and delayed first permanent molar development. Genetically, it can present with a familial tendency or in patients with cleft lip and/or palate.11
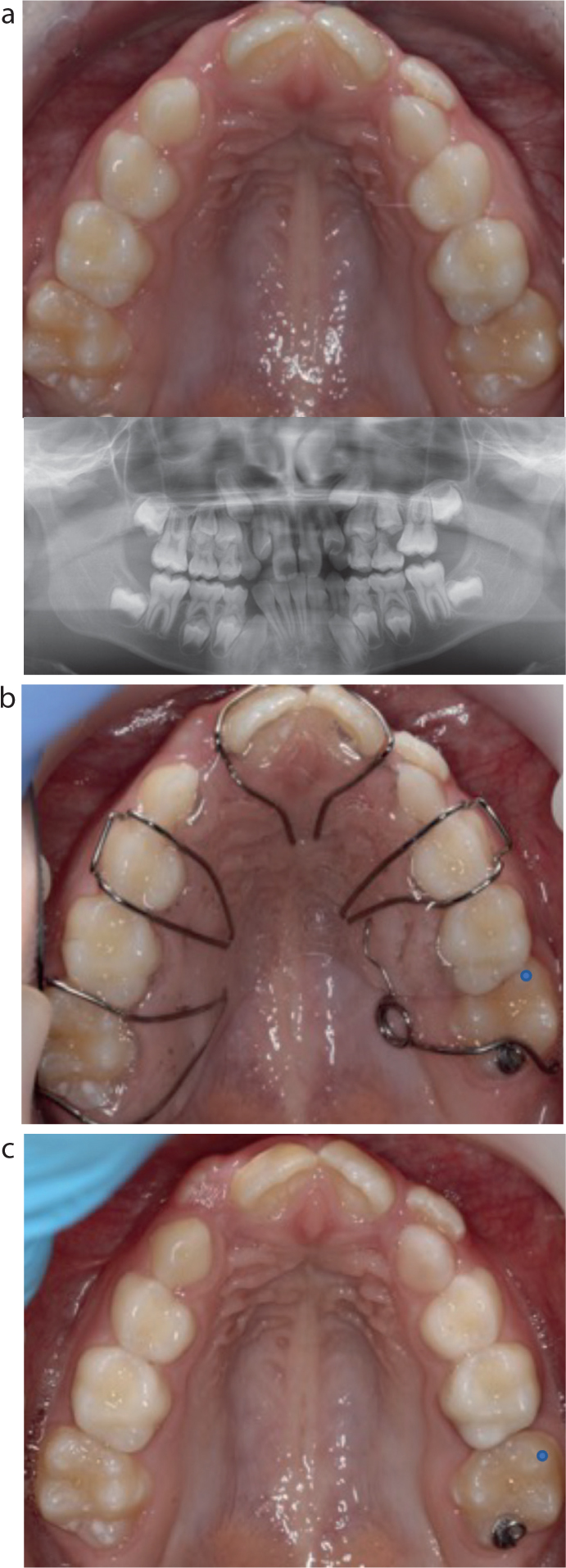
Impacted first permanent molars or patients with a history of FPM impaction are often noted coincidentally on radiographic assessment. They can be classified as reversible or irreversible depending on the spontaneous correction of the impaction. During a period of monitoring, spontaneous correction may have occurred in approximately 60% of cases.11 In irreversible forms, further intervention may be required. The use of brass wire or separators has been described in the literature.11 Additionally, uprighting of the first permanent molar can be carried out using an upper removable appliance (URA) with a palatal finger spring engaging a button bonded occlusally on the molar tooth (Figure 3), or a Humphrey's appliance. In cases where the prognosis of the second deciduous molar is poor owing to external resorption caused by the ectopic first permanent molar, extraction may be indicated, and subsequent space maintenance can be considered to prevent mid-arch crowding as a result of space loss. Space maintainers, such as transpalatal arches, band and loop and URAs have been used for this purpose.
Figure 3. (a) Upper occlusal photograph and OPT demonstrate severe potential crowding in the upper left quadrant, which also has an impacted UL6. The crowding is so severe that the patient will potentially require removal of >1 unit later on. (b) URA with palatal finger spring to disimpact UL6 (with button bonded to occlusal surface). The ULE should be monitored because there is a risk of this tooth having irreversible pulpitis and infection relating to the significant external resorption. (c) Excellent cooperation has successfully led to disimpaction of UL6 evidenced by the movement of the blue dot on the mesiobuccal cusp of the UL6.
Extraction of primary teeth and space maintenance
Extraction of primary teeth
Patients may require early extraction of primary teeth as a result of caries, periapical/interradicular pathology, trauma, infra-occlusion or interceptive management. Those who present with pain or acute infection often require more immediate management, while those with currently asymptomatic chronic conditions, may provide time for a comprehensive treatment plan, particularly if the patient is due to have a general anaesthetic to facilitate the treatment. Sometimes deciduous canine teeth are extracted to allow eruption of lateral incisor teeth where there is likely crowding to allow space for alignment of an unerupted central incisor or correction of a crossbite.
Sequelae
Early loss of deciduous teeth can result in space loss, which can present as crowding of the permanent dentition with associated impactions, centreline shifts and tipping of the adjacent teeth.12 The centreline is likely to be affected the more anteriorly a tooth is lost; however high-quality experimental evidence is lacking to support this clinical finding. A reduction in arch length may later necessitate the need for extractions of permanent teeth if the patient requires orthodontic treatment.
Space maintenance
A patient with caries is unlikely to be an appropriate candidate for a space maintainer, given the need for good oral hygiene and cooperation. Space maintenance can be considered in cases when an infra-occluded second deciduous molar, especially in a single quadrant, has to be extracted and there is a likelihood of crowding precipitating as a result of early extraction or pre-existing crowding. A removable appliance could be considered for space maintenance, however, it would require strict adherence to wearing it continuously. Alternatively, a band and loop design from an erupted first permanent molar is an effective means of maintaining the space, and is cemented into place, negating the need for patient cooperation with wearing it, although good oral hygiene needs to be maintained. In the upper arch, a transpalatal arch with a nance button could be considered as a space maintainer and in the lower arch, a lingual arch could be used. However, as with a band and loop, sufficient oral hygiene needs to be maintained throughout.
Habits
Types of habits
A habit is considered ‘an acquired behaviour pattern regularly followed until it has become almost involuntary.’13 Within dentistry, they often present as persistent sucking habits (dummy or digit), but can also present as chewing on objects, such as pens or oral piercings. Digit or pacifier sucking habits have been shown to persist past the age of 7 years in 12.1% of children, with this being more common among females than males.14
Sequelae
The effects of habits are very specific to the mechanism of the habit. Common effects with sucking habits can include constriction of the maxilla, contributing to a posterior crossbite, which is often unilateral, and can sometimes be associated with a displacement. Proclined upper incisors and retroclined lower incisors may also be a presenting feature resulting in an increased overjet. An anterior or lateral open bite is often seen, potentially being asymmetrical depending on the side the patient is more likely to place their digit or dummy (Figure 4). The presence of an anterior open bite has also been shown to be related to defective speech, for example a lisp.15 It is also useful to assess the patient's digits if there is a reported history of sucking. The used digits could present with a deformity, or have inflammation surrounding the nail bed.16 Other habits, such as chewing habits, may cause non-carious tooth tissue loss (NCTTL) and result in gingival recession defects and/or tooth mobility.
Figure 4. Differences between (a–c) asymmetrical and (d–f) symmetrical digit-sucking habits. NB Tendency towards crossbite development on affected side(s).
Management
Ideally, non-nutritive sucking habits should be stopped prior to the development of the permanent dentition to prevent unintended effects on the occlusion. A Cochrane review, carried out in 2015, suggested that both orthodontic appliances, as well as psychological interventions, such as positive and negative reinforcement, are effective at encouraging the cessation of a sucking habit, although the evidence was low quality.17 Assessing the mechanism of the habit and understanding the history can be helpful in guiding management. In addition, the need for patient and family compliance is key. Behavioural modification techniques, such as positive reinforcement, could be used. For example, praise and reward methods. Other commonly suggested methods include the use of a deterrent such as an unpleasant tasting varnish, a plaster on the used digit or a sock/glove over the hand. If the patient uses an object such as a pacifier, this should be removed.
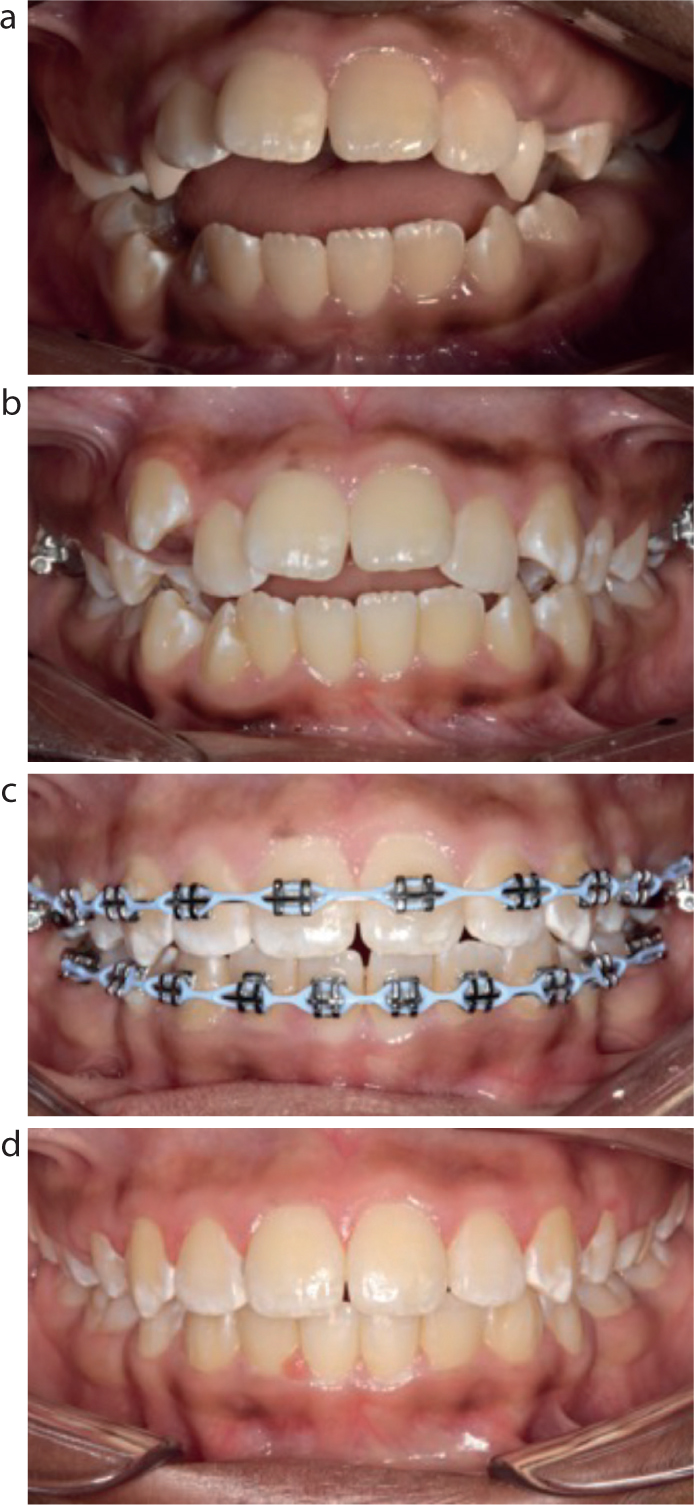
Orthodontic appliances can also be used. These are usually placed following less invasive attempts where there has been persistence of the habit. They may include a palatal crib such as a Hayrake appliance or palatal arch similar to that described by Haryett.18 Use of a removable appliance such as a twin block appliance can also prevent the patient getting satisfaction through the habit and can aid in cessation while also treating a developing malocclusion. Figure 5 provides an example of the treatment received by a patient who initially presented with a significant digit-sucking habit.
Figure 5. (a) Patient who presented with an extensive, symmetrical digit-sucking habit combined with high vertical proportions. (b) Following Hayrake appliance. (c) During fixed appliances and loss of four premolars. (d) Debond.
If interception of the habit is not successful, the traits that present in the malocclusion may require future treatment with maxillary expansion devices, growth modification, orthodontic camoflauge treatment with extractions and fixed appliances or a joint orthodontic–surgical approach.
Trauma
The management of traumatic dental injuries (TDI) for patients undergoing active orthodontic treatment is complex and often requires a multidisciplinary team approach. These patients typically present initially to GDPs in primary care or out-of-hours to emergency departments (ED) and have their initial assessments and management carried out by the oral and maxillofacial surgery (OMFS) team, hence knowledge of the management of TDI is crucial.
In addition, with the knowledge that approximately one-in-four individuals will sustain a traumatic dental injury to their permanent dentition before the age of 16 years and around 200,000 children and young people start orthodontic treatment each year in England and Wales, recent guidance has been published regarding the orthodontic management of previously traumatized teeth and management of acute dental injuries in the active orthodontic phase.19,20,21 It is important for GDPs who refer patients for orthodontic assessment to ensure that they notify the orthodontist of any documented traumatic dental injuries.
Following TDI in patients undergoing active orthodontics, consideration must be given to the phenomenon of ‘transient apical breakdown’ or ‘TAB’, defined as ‘a reversible resorptive process in which the apex of a tooth shows some radiographic evidence of resorption and the crown may display some discolouration.’22 When related to orthodontic treatment, TAB usually requires no intervention other than cessation of the orthodontic forces on the affected tooth and monitoring. However, in relation to TDI, TAB is most associated with luxation injuries (one of the most common TDIs experienced), making decision making more of a challenge, with a delicate risk–benefits analysis required.23 Conhenca and colleagues advise that multiple factors must be taken into consideration when deciding to monitor for TAB and spontaneous revascularization, or proceed with endodontic therapy: the trauma itself, the extent of the pulpal injury and known associated risk of pulpal necrosis (especially with regards to immature versus mature apices) and the ability of the patient to conform to a frequent recall schedule.23 If there has been a significant traumatic dental injury, it would be advisable to involve a paediatric dentistry specialist to consider the long-term prognosis of the injured tooth/teeth to ensure that this is considered in future treatment planning.
Orthodontic management of trauma
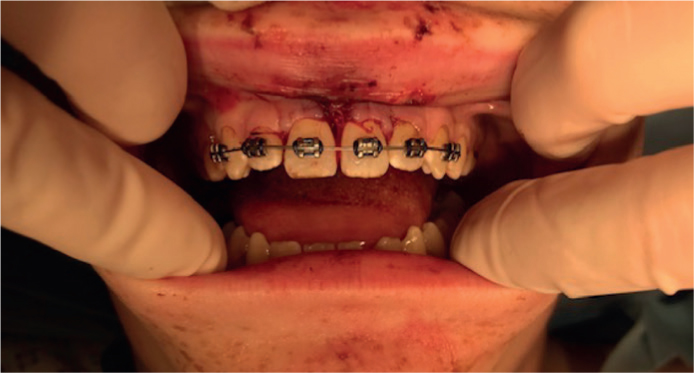
Orthodontics can be used to manage both acute trauma as well as the sequelae following trauma. Sandler and colleagues have produced guidelines for the orthodontic management of trauma.20 Orthodontic brackets and archwires (minimum 0.016” stainless steel) can be used to splint traumatized teeth to adjacent non-affected teeth for the time recommended in the International Association of Dental Traumatology (IADT) guidelines, dependent on the type of injury. Although in an acute situation, a titanium trauma splint secured with composite may be used instead of brackets – brackets have the benefit of allowing monitoring of individual teeth at reviews, for example assessment of mobility and tenderness to percussion (Figure 6). Orthodontics is sometimes advocated to be used in intrusion injuries to enable repositioning (Figure 7). In immature teeth, this is considered after 4 weeks of monitoring for spontaneous repositioning. In mature teeth, a tooth intruded 3–7 mm or less than 3 mm (that has failed to re-erupt in 8 weeks) is considered for orthodontic repositioning. This may be guided by the need for root canal treatment (depending on the clinical and radiographic findings at subsequent follow-up appointments) and surgical repositioning may be preferred to allow this to be initiated at an earlier stage, reducing the risk of external inflammatory root resorption.24 Extrusion mechanics can also be employed in cases of crown-root fractures to extrude root fragments sufficiently to provide access for a definitive restoration, although this does compromise the crown-root ratio.
Figure 6. Trauma splint using brackets and wire: child sustained avulsion UR1, UL1 and lateral luxation UR2, UL2.Figure 7. (a–f) Severe intrusion injury of UR1 (which has an immature apex) with minimal signs of spontaneous eruption over a 4-week period as per IADT Dental Traumatology guidelines. (g–k) An upper fixed appliance used to extrude UR1 to correct incisal level, followed by placement of a bonded retainer. Paediatric dental trauma follow-up appointments were scheduled to assess post-traumatic sequelae. A later course of orthodontic treatment was planned to address the increased overjet in the permanent dentition.
The sequalae of trauma can result in the need for prosthetic replacement of teeth or space closure (Figure 8). Orthodontic appliances can be used to redistribute and optimise spaces for restorations, such as resin-bonded bridges or implants. Fixed appliances can control root movement, encouraging divergence in the region where implants are required. In younger patients, the restorations may not be placed immediately. In particular, implants are not placed until growth has stopped and therefore, these spaces need good retention regimens to prevent space loss and tipping of roots into the proposed implant space. To reduce this risk, it is often the case that orthodontic treatment may be commenced when the patient is slightly older.
Figure 8. (a–e) Example of managing traumatic loss of upper central incisor via camouflage of adjacent lateral incisor. Patient treated using fixed appliances, extraction of UR4 and anchorage reinforcement to correct upper centre-line shift following mesial movement of UR1. (f–j) Following composite build-up to camouflage UL2 as UL1.
Interceptive treatment with orthodontics has been shown to reduce the risk of incisal trauma. Use of a functional twinblock appliance for example, can help a patient gain a lip seal and reduce the overjet, which are key factors increasing an individual's risk of dental trauma.25 This is discussed further in Part 2 of this series.
Conclusion
This article highlights how close collaboration between orthodontists and paediatric dentists can result in optimal outcomes across a wide variety of clinical cases. General dental practitioners play a key role in the timely referral and routine follow-up of joint orthodontic–paediatric cases, hence this article provides knowledge on how to recognize and manage common problems in primary care. An efficient tripartite relationship between orthodontist, paediatric dentist and GDP combines the skills of all members, and ensures patients are seen by the right people, in the right place, at the right time.