Tanne K, Yoshida S, Kawata T An evaluation of the biomechanical response of the tooth and periodontium to orthodontic forces in adolescent and adult subjects. Br J Orthod. 1998; 25:109-115
Dudic A, Giannopoulou C, Kiliaridis S Factors related to the rate of orthodontically induced tooth movement. Am J Orthod Dentofacial Orthop. 2013; 143:616-621 https://doi.org/10.1016/j.ajodo.2012.12.009
Alruwaithi M, Jumah A, Alsadoon S Tooth ankylosis and its orthodontic implication. J Dent Med Sci. 2017; 16:108-112
Mirabella AD, Artun J Prevalence and severity of apical root resorption of maxillary anterior teeth in adult orthodontic patients. Eur J Orthod. 1995; 17:93-99 https://doi.org/10.1093/ejo/17.2.93
Huang J, Walsh RM, Witherspoon DE The prevalence, characteristics, and risk factors of external cervical resorption: a retrospective practice-based study. Clin Oral Investig. 2023; 27:5595-5604 https://doi.org/10.1007/s00784-023-05180-2
Danz JC, Greuter C, Sifakakis I Stability and relapse after orthodontic treatment of deep bite cases – a longterm follow-up study. Eur J Orthod. 2014; 36:522-530 https://doi.org/10.1093/ejo/cjs079
Moradi G, Mohamadi Bolbanabad A, Moinafshar A Evaluation of oral health status based on the decayed, missing and filled teeth (DMFT) Index. Iran J Public Health. 2019; 48:2050-2057
Zaleckiene V, Peciuliene V, Brukiene V, Drukteinis S Traumatic dental injuries: etiology, prevalence and possible outcomes. Stomatologija. 2014; 16:7-14
The Adult Orthodontic–Restorative Interface. Part 1: Concepts of Treatment and Presenting Challenges Graeme Bryce Robert Smith Christopher Stagles Dental Update 2025 51:9, 610-616.
This is the first article in a three-part series that discusses joint orthodontic–restorative care for the adult patient. Part 1 presents an overview of the clinical presentations, challenges and strategies that may be employed to treat this complex patient group.
CPD/Clinical Relevance: The reader should be able to describe a care pathway, with potential associated complications, for the provision of adult orthodontic–restorative treatment.
Article
The combination of the orthodontic and restorative disciplines can be essential to the dental rehabilitation for both child and adult patients. While it is recognized that orthodontics is crucial in optimising the restorative outcomes of adolescent patients with hypodontia or ectopic canines, in contrast, there is reduced available advice on orthodontics for adults suffering from either developmental or acquired disease.
This three-part series presents an overview of adult patients with developmental and acquired disease, who require joint orthodontic–restorative care. In Part 1, an overview ofthe clinical presentations and challenges associated with adult orthodontic care are provided and associated treatment strategies are discussed.
Rationale for orthodontic–restorative care within the adult patient
The demand for both adult orthodontic and restorative care has increased (Table 1),1 fuelled by a greater proportion of the population maintaining their dentitions into old age, and patients’ desire for improved aesthetics.2, 3 From a patient perspective, greater acceptance of orthodontic care in adulthood has been achieved via advances in clear aligner systems, ceramic brackets, and lingual fixed appliances that have offered an alternative to the visual impact associated with conventional fixed appliances.2, 4
Patient led
Clinician led
Increased awareness of smile aesthetics driven by societal pressures and social media
Management of malocclusion that was not treated as a child or was late presenting
Significant life events: new career, relationship breakdown and commencement of new relationships
Antero-posterior realignment:
Replacement of missing teeth
Developmental absence of teeth (e.g. hypodontia)
Traumatic or acquired absence of teeth
Inter-coronal space redistribution, or closure, to enable/assist with restorative care
Uprighting of teeth to facilitate fixed bridge or removable partial denture provision
Uprighting or mesial/distal movements of roots to facilitate implant placement
Relapse of previous orthodontic treatment
Vertical realignment:
Extrusion of teeth to increase supra-gingival coronal tooth structure
Intrusion of over-erupted teeth to increase the inter-occlusal space for placement of restorations
Overbite reduction with a combination of intrusion and extrusive movements
Failure to receive, or ineligibility for, orthodontic therapy as child
Correction of incisal/canine malalignment to improve functional excursive guidance
Increased awareness of orthodontics following their children's treatment
There is increased recognition of the functional and aesthetic benefits that can be realized by the integration of orthodontics into an overarching restorative plan. While the rationale for inclusion of orthodontic tooth movement may vary, common reasons include: redistribution of space associated with missing or diminutive teeth, ectopic teeth, parallelism of abutments,5 optimization of dental rehabilitation following severe tooth surface loss or trauma, and patients with tooth drifting secondary to periodontal attachment loss.6
Orthodontic challenges and risks within the adult patient
Tooth movement and treatment times
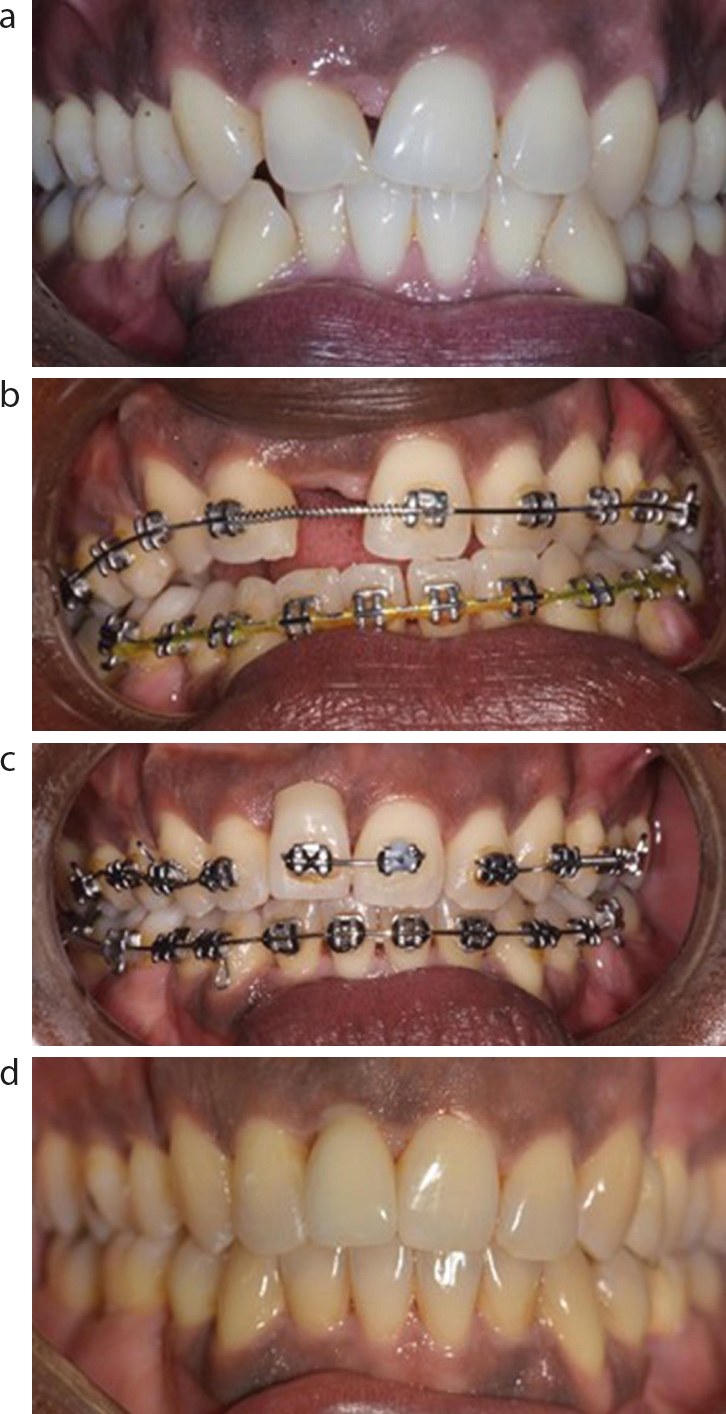
It is generally considered that teeth respond differently to the application of orthodontic forces in adult patients, with slower tooth movement and subsequent increased treatment duration to be anticipated.7, 8 At a biological level, factors that contribute to this problem include the cessation of craniofacial growth, a reduced cellular turnover rate, and delay to the response of the periodontal ligament (PDL) following the application of orthodontic forces. While total failure of a tooth/teeth to move on application of orthodontic forces is rare, this may occur, especially if ankylosis is present (Figure 1).9
Figure 1. (a–d) Patient with traumatically lost UR1 and unaesthetic space closure. Ankylosis of UL1 causing occlusal cant with fixed appliance. Treatment plan amended to accept position of UL1 (and camouflage angulation with enamel reduction) and dental implant restoration UR1.
Skeletal discrepancies in the growing patient may be treated with functional appliances, an approach not feasible when skeletal maturity has been attained in adulthood (normally in the late teens or early 20s). Growth cessation can add some certainty to treatment planning, although the magnitude of tooth movements achievable via orthodontic appliances is limited, and orthognathic surgery may be the only way to address severe antero-posterior skeletal discrepancies. The occlusal scheme with adult patients is also well established, which may include buccal segment relationships with deep cusp-embrasure contacts, and strong oral musculature that can impede significant ‘full-unit’ tooth movements.
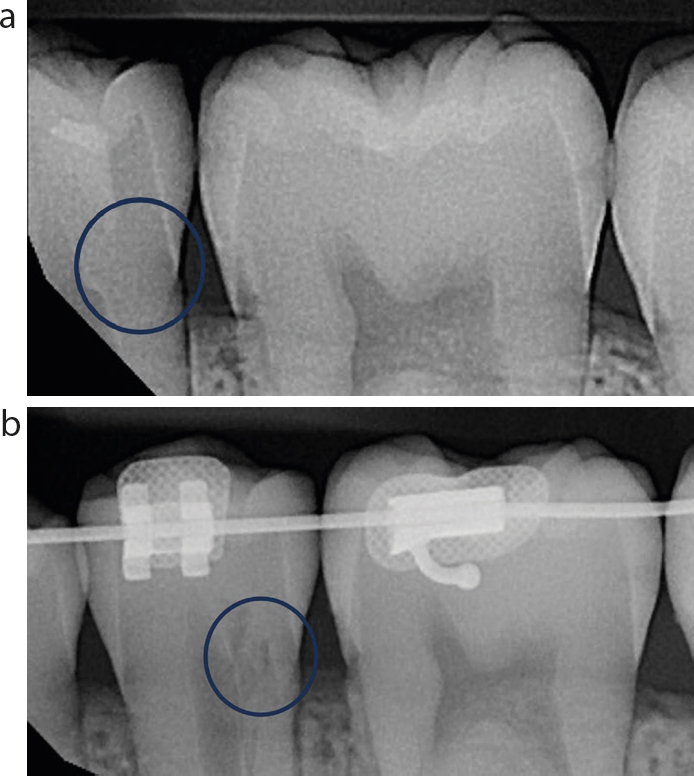
Some adult patients will have had previous orthodontic therapy, potentially presenting with relapse to the original malocclusion, or other unfavourable movements often related to the ageing process.10 While further orthodontic treatment is not necessarily contra-indicated, thorough radiographic assessment is a prerequisite before commencing treatment. Starting root lengths may be shorter, and subsequent episodes of orthodontic tooth movement are associated with an increased risk of orthodontically induced root resorption (OIRR),11 and external cervical root resorption (ECR) (Figure 2).12
Figure 2.
(a) Bitewing radiograph taken prior to initiation of orthodontic treatment, showing no evident ECR. (b) However, in a later radiograph, ECR is evident in the mandibular second premolar (confirmed clinically to be present on the buccal aspect) initiated following fixed appliance orthodontic therapy.
Overbite considerations
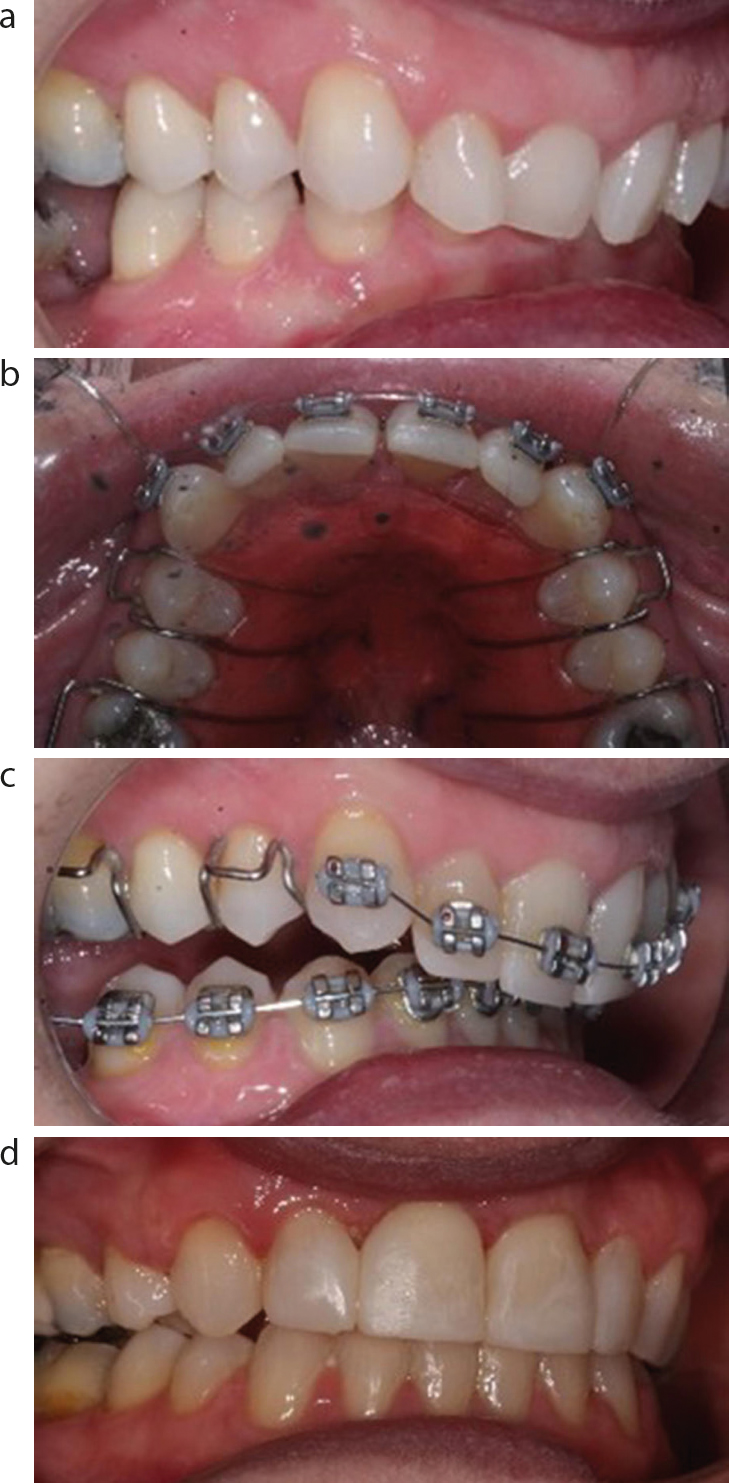
Treatment planning should detail the movements required to achieve the desired position and angulation of the maxillary incisor edge relative to the upper lip and subsequently aim to establish good inter-incisal contact, typically achieved by correcting the canines to a Class I relationship. Severe inter-incisor discrepancies can be difficult to camouflage in the adult patient, with subsequent impact on aesthetic and functional outcomes and the stability of the final tooth positions.13 In particular, the treatment of an increased overbite can be challenging in the older patient owing to the significantly reduced potential for vertical alveolar growth and/or elongation of the mandible at the condyle. A deep overbite may also often present insufficient space for labial fixed appliances, with an increased risk of bracket debond or wire fracture in the lower arch. Conventional mechanics, such as anterior bite platforms, can be used to increase inter-occlusal space to facilitate arch levelling and incisor intrusion, and are generally well tolerated in the adult patient when their requirement is explained in the consent stage (Figure 3). Alternative mechanics include temporarily increasing the vertical dimension using glass ionomer or composite stops on the posterior molars or the use of a lingual or aligner-type appliances which do not interfere with the anterior occlusion (Figure 4). Clear aligners are also useful at creating temporary interocclusal space, but are not generally accepted as being suited for complex mechanics where the roots of teeth need to be moved a significant distance.
Figure 3. (a–d) Deep overbite complicated by anterior tooth wear managed by a removable appliance with anterior bite plane (not shown) to create space for fixed appliances, upper premolar extractions and subsequent composite additions.Figure 4. Class II division 2 malocclusion with increased overbite and attritional tooth wear from parafunctional clenching. (a) The original restorative digital work-up for palatal veneers, which required an extensive palatal bite platform to provide occlusal contacts. (b) The patient subsequently opted for clear aligners, incorporating anterior bite planes and elastics, to reduce the overbite and overjet. (c) These corrections made the construction of thinner definitive palatal backings possible (diagnostic work-up in final image), which were easier to tolerate while still protecting the teeth surfaces from further attritional damage.
Skeletal discrepancies
Skeletal discrepancies in the growing patient may be treated with functional appliances, an approach not feasible in adulthood when skeletal maturity has been reached (normally in the late teens or early 20s). Growth cessation can add some certainty to treatment planning, particularly for a Class III skeletal relationship, but as the magnitude of tooth movements achievable via orthodontic appliances is limited, orthognathic surgery may be the only way to address severe antero-posterior skeletal discrepancies to establish a normal inter-incisal relationship.
The buccal occlusion within the adult patients is well established, often with deep cusp-embrasure contacts and strong oral musculature. Without temporary disclusion, this can often impede larger tooth movements that may be required to address an underlying skeletal discrepancy with orthodontic camouflage.
Compromised dentitions
In general, an increased restorative burden can be anticipated in older patients, particularly those from low socio-economic backgrounds.14 Damage to the dental hard tissues (via caries, trauma or tooth wear) or the presence of metal/ceramic restorations may compromise ideal orthodontic bracket positioning and bonding. For extensively restored teeth, additional consideration must be given to the increased potential for crack propagation or bulk fracture from forces applied during active orthodontic treatment, and upon bracket removal.
Achieving periodontal health prior to the provision of orthodontic therapy is a prerequisite. However, even once stabilized, reduced periodontal attachment levels may present problems with reduced anchorage support. It should also be considered that adults are more likely to have accumulations of dental traumatic injuries,15 with a subsequent increased incidence of ankylosis, pulpal disease, apical periodontitis and resorption. Such injuries may limit or exclude orthodontic therapy owing to their unpredictable reaction to orthodontic forces and potential for disease progression leading to tooth loss. When the orthodontic alignment requires extractions, there is often little option but to extract teeth with poorer prognosis, and this may subsequently negatively impact options for anchorage and thus compromise the final treatment result.
Dento-alveolar defects
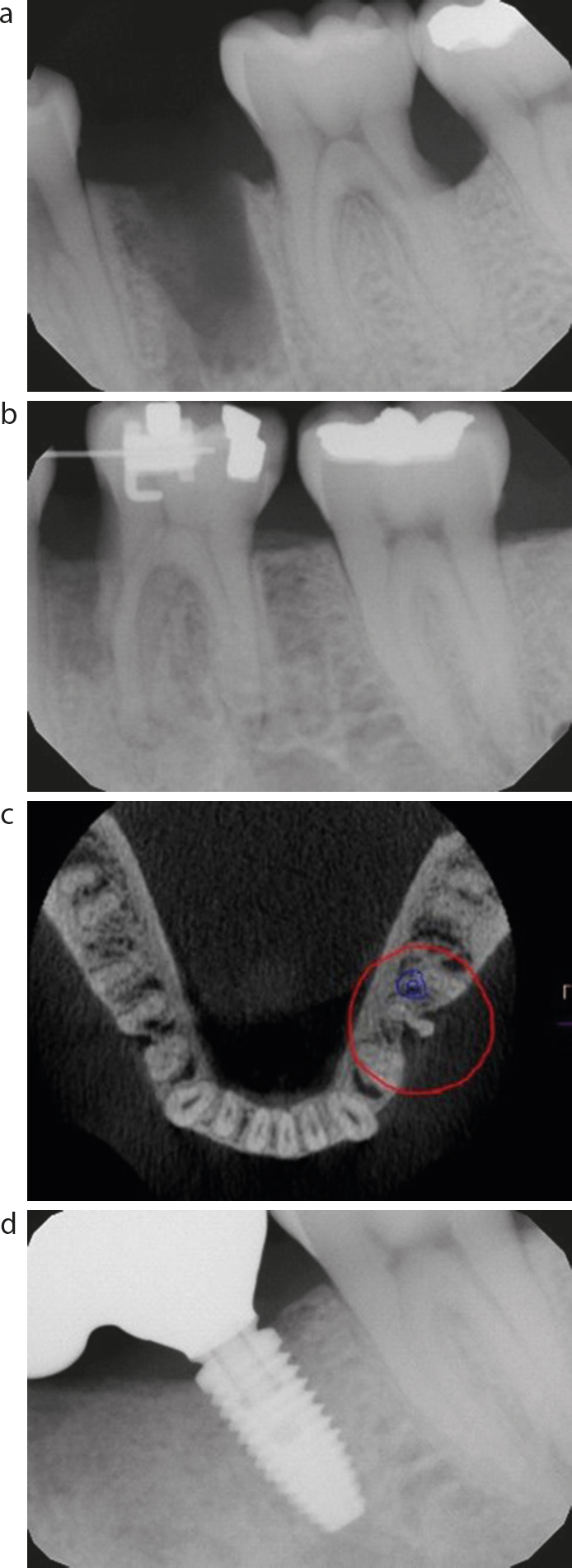
Adult patients often present with vertical and horizontal alveolar bone defects, in sites where teeth have been developmentally absent or lost through acquired disease.16 Clinical features associated with dento-alveolar bone defects include: reduced keratinized mucosa; spaced dentitions; tooth translocation, retained deciduous teeth; tipping/tilting/rotation; and vertical height discrepancies between teeth. Dento-alveolar defects present challenges to both orthodontic care (Figure 5), with an increased risk of moving teeth out of the dento-alveolar bone, and restorative replacement, owing to the increased difficulties associated with prosthetically disguising soft tissues and placing implants in reduced bone volumes.
Figure 5. (a–d) Radiograph series showing LL6 being moved anteriorly into a dento-alveolar defect from extracted LL5. The LL6 mesial root developed a perio-endo defect, and was subsequently extracted and replaced with an implant-supported restoration.
Principles of orthodontic–restorative treatment planning
Inter-disciplinary treatment planning should aim to achieve functional and aesthetic outcomes while preserving dental tissues. Oral health stability will underpin the success of any treatment plan, and ensuring patient commitment is particularly important within the adult patient with a high restorative burden, especially where poor compliance is likely to have contributed to many of the dental problems previously encountered.
A summary of key restorative considerations within the joint orthodontic–restorative patient are shown in Table 2.
Retainer(s) (fixed/removable)? If patient was provided with removable retainer, but no longer wears these, then when and why did they stop?
Implications: It is essential to ascertain the reasons for suboptimal outcomes of previous treatment, including poor compliance, root resorption and orthodontic relapse, when considering the possibility of further orthodontic treatment
History of trauma to the teeth/jaws
Screen for history of:
Trauma to the teeth and jaws?
If so, then:
Tooth/teeth/jaw(s) affected?
Single or multiple episodes?
Type of injury?
Date of injury
Management?
Implications: Dental trauma predisposes to a variety conditions, with implications for orthodontic–restorative management, including cracks/fractures (crown and root), resorption, pulpal complications, ankylosis. (See Part 3 of this series)
Clinical assessment
Enamel crazing, cracks and fractures
Dry teeth and assess for enamel crazing and cracks under magnification ± transillumination
Localized deep periodontal pocket(s) can be associated with vertical root fractures; screen for these using a UNC-15 probe
Implications: Cracks may propagate as a result of orthodontic forces. A tooth with a vertical root fracture may not be predictably restorable
Restorability assessment of fractured/broken-down teeth
Determine whether cavity margins can be isolated (for bonding procedures)
Where a crown is required, consider whether there is adequate tissue for ferrule effect. Ideally there should be a circumferential band of dentine at least 1 mm thick and ≥2 mm above the gingival margin. Where this is not possible, a partial ferrule may be possible. Where margins are sub-gingival these should not encroach into the supracrestal attachment (as chronic inflammation ± gingival recession will ensue)
Use a UNC-15 probe to assess the height and thickness of remaining tooth tissue
Options for increasing the clinical crown height include:
Gingivectomy
Surgical crown lengthening
Orthodontic extrusion
Endodontic status
Red/pink intrinsic discolouration of the crown with recent trauma may be associated with a pulpal haemorrhage (and could be transient)
Grey discolouration of tooth is often indicative of pulp necrosis
Yellow discolouration may be associated with calcific metamorphosis in a vital tooth
Tenderness to palpation may indicate a lesion of endodontic origin (LEO)
Development of a swelling or sinus may also indicate a LEO
Undertake both cold and electric type pulp tests - may get false negative pulp tests within the first 3 months following traumatic dental injury (TDI)
Implications: There are multiple potential causes of tooth discolouration, and tooth discolouration, in itself, is not an indication for root canal treatment. The risk of root resorption in teeth undergoing orthodontics is heightened in the presence of a LEO
Radiographic assessment
2D radiographic assessment (e.g. long cone peri-apical radiograph, or dental pantomogram)
Useful within the radiographic assessment of status of: anatomical crown, existing restorations, crestal bone levels, root form, thickness and length, presence/absence/thickening of periodontal ligament space (including peri-radicular lesions), resorption (all types – see Part 3 of the series), root/tooth proximity, unerupted teeth, status of adjacent teeth, and any other pathology
3D radiographic assessment (e.g. cone beam computed tomography (CBCT))
CBCT can be used to overcome some of the limitations of 2D assessment, particularly the problem of ‘anatomical noise’ via superposition of structures, localization of unerupted teeth, assessment of bone dimensions and proximity to key structuresImplications: While not often necessary within ‘routine’ orthodontic care, a CBCT taken principally for restorative assessment can provide useful information to inform the orthodontic plan; for instance the presence of resorptive or other anatomical defects and location of ectopic teeth
An overview of a conventional joint orthodontic–restorative care pathway (Figure 6)
Figure 6. Treatment of patient with traumatically lost UR1 and repeated resin-bonded bridge failures. Insufficient vertical space for implant crown. Upper removable appliance with bite plane, lower incisor extraction and lower arch fixed appliance used to improve incisor relationship. Implant was placed early without upper arch alignment for reduced overall treatment time. (a–c) Pre-treatment: deep, complete overbite with overeruption of lower incisors. (d–f) Stage 1: URA with bite plane. Composite build-up of tooth wear-affected lower incisors. (g–i) Early orthodontics: extraction required in lower arch for space creation. (j–l) Late orthodontics: implant placed. Essix retainer used to prevent pressure on implant fixture. (m–o) Finish: overbite reduced, incisors aligned.
Joint consultation with orthodontist and restorative dentist
Assessment of patient aspirations, history taking, examination, special tests and appropriate imaging is necessary to determine diagnoses and clinical challenges. A prerequisite of orthodontic–restorative care is that primary disease, including modifying aetiological factors, are stable prior to commencement. For patients with unstable periodontal disease, dental caries or tooth wear, further engagement with the general dental practitioner is required to provide appropriate treatment, prior to any orthodontic phase.
Treatment planning
The overall objectives of the restorative care plan should be specified. Further to this, the required tooth movements necessary to achieve the desired care plan should be determined, and then (from practical point of view) judgement applied to determine whether such movements are likely to be feasible from an orthodontic perspective. Normally this will require engagement with a dental laboratory to complete a diagnostic work-up (either in wax or digitally). The subsequent mockup can then be used to confirm or refute the plan, and aids communication of the intent with the patient. The mockup will also enable the identification of patients that cannot be managed solely by an orthodontic–restorative pathway and enable early discussion with other specialities, for instance oral and maxillofacial surgery (OMFS).
Consent
The patient should have sufficient capacity and time to process this information, so that they can fully understand the risks, benefits and challenges of the plan. Orthodontic–restorative pathways generally involve lengthy timescales and the anticipated duration should be discussed and documented within the consent process. The option for a compromised outcome with an increased retention requirement, or a limit to the scope of restorative modalities may be required.
Pre-orthodontic restorative care
Vulnerable teeth should be restored/stabilized to prevent disease progression and/or to facilitate bonding of orthodontic appliances and improved aesthetics through treatment. Early implant placement may be required for ‘absolute’ anchorage.
Commencement of the orthodontic phase of care
Review during orthodontic treatment
Predetermined joint orthodontic–restorative assessments to ascertain progress of care against plan.
Final review prior to debonding
The patient should have a joint orthodontic–restorative assessment prior to debonding to ensure that the orthodontic outcome has enabled the desired restorative interventions. If tooth replacement with a dental implant is planned, a long cone peri-apical radiograph should be taken prior to debond to check for root parallelism and inter-radicular space.
Debonding of appliances
The patient should be provided with retention that prevents relapse, but also enables restorative provision. This may include both fixed retainers and removable appliances, often supporting prosthetic teeth.
Definitive restorative care
This will require further assessment to ensure that the dentition is healthy and that the original plan is still viable. Further special tests, such as CBCTs to assess bone volumes for dental implants, and revised mock-ups are likely. The duration of the restorative phase of treatment will vary dependent on the treatment complexity and may range from months (for removable partial dentures, resin-bonded bridges or direct restorations only) to years (if bone grafting and implant-supported prostheses are employed).
Definitive retention
Including consideration of long-term wearing of fixed or removable retainers.
Review
Summary
Orthodontic–restorative care pathways are complex and of long duration. While this multi-disciplinary approach can offer solutions for the successful management of otherwise untreatable cases, it is essential that the patient undergoes precise assessment, diagnosis and treatment planning. In Part 2, orthodontic–restorative treatment strategies for adult patients with developmental anomalies of the dentition are discussed.