Khalaf K, Miskelly J, Voge E, Macfarlane TV Prevalence of hypodontia and associated factors: a systematic review and metaanalysis. J Orthod. 2014; 41:299-316 https://doi.org/10.1179/1465313314Y.0000000116
Peck S, Peck L, Kataja M Site-specificity of tooth agenesis in subjects with maxillary canine malpositions. Angle Orthod. 1996; 66:473-476 https://doi.org/10.1043/0003-3219(1996)06
Silveira GS, de Almeida NV, Pereira DM, Mattos CT, Mucha JN Prosthetic replacement vs space closure for maxillary lateral incisor agenesis: a systematic review. Am J Orthod Dentofacial Orthop. 2016; 150:228-237 https://doi.org/10.1016/j.ajodo.2016.01.018
Westgate E, Waring D, Malik O, Darcey J Management of missing maxillary lateral incisors in general practice: space opening versus space closure. Br Dent J. 2019; 226:400-406 https://doi.org/10.1038/s41415-019-0082-4
Giachetti L, Bertini F, Landi D Morphological and functional rehabilitation of severely infra-occluded primary molars in the presence of aplasia of the permanent premolar: a clinical report. J Prosthet Dent. 2005; 93:121-124 https://doi.org/10.1016/j.prosdent.2004.11.003
Romeo E, Lops D, Amorfini L, Chiapasco M, Ghisolfi M, Vogel G Clinical and radiographic evaluation of smalldiameter (3.3-mm) implants followed for 1–7 years: a longitudinal study. Clin Oral Implants Res. 2006; 17:139-148 https://doi.org/10.1111/j.1600-0501.2005.01191.x
Lee JS, Kim HM, Kim CS, Choi SH, Chai JK, Jung UW Long-term retrospective study of narrow implants for fixed dental prostheses. Clin Oral Implants Res. 2013; 24:847-852
Chrcanovic BR, Kisch J, Albrektsson T, Wennerberg A Bruxism and dental implant treatment complications: a retrospective comparative study of 98 bruxer patients and a matched group. Clin Oral Implants Res. 2017; 28:e1-e9 https://doi.org/10.1111/clr.12844
Schoenbaum TR, Swift EJ Abutment emergence contours for single-unit implants. J Esthet Restor Dent. 2015; 27:1-3 https://doi.org/10.1111/jerd.12143.s
Soulami S, Slot DE, van der Weijden F Implant-abutment emergence angle and profile in relation to peri-implantitis: A systematic review. Clin Exp Dent Res. 2022; 8:795-806 https://doi.org/10.1002/cre2.594
Wisth PJ, Thunold K, Böe OE Frequency of hypodontia in relation to tooth size and dental arch width. Acta Odontol Scand. 1974; 32:201-206 https://doi.org/10.3109/00016357409002548.s
Bjerklin K, Bennett J The long-term survival of lower second primary molars in subjects with agenesis of the premolars. Eur J Orthod. 2000; 22:245-255 https://doi.org/10.1093/ejo/22.3.245
Sletten DW, Smith BM, Southard KA, Casko JS, Southard TE Retained deciduous mandibular molars in adults: a radiographic study of long-term changes. Am J Orthod Dentofacial Orthop. 2003; 124:625-630 https://doi.org/10.1016/j.ajodo.2003.07.002
Arhakis A, Boutiou E Etiology, Diagnosis, Consequences and Treatment of Infraoccluded Primary Molars. Open Dent J. 2016; 30:714-719 https://doi.org/10.2174/1874210601610010714
Peretz B, Absawi-Huri M, Bercovich R, Amir E Inter-relations between infraocclusion of primary mandibular molars, tipping of adjacent teeth, and alveolar bone height. Pediatr Dent. 2013; 35:325-328
Vermeulen AH, Keltjens HM, van't Hof MA, Kayser AF Ten-year evaluation of removable partial dentures: survival rates based on retreatment, not wearing and replacement. J Prosthet Dent. 1996; 76:267-72 https://doi.org/10.1016/s0022-3913(96)90170-5
Wagner B, Kern M Clinical evaluation of removable partial dentures 10 years after insertion: success rates, hygienic problems, and technical failures. Clin Oral Investig. 2000; 4:74-80 https://doi.org/10.1007/s007840050119
Pjetursson BE, Tan WC, Tan K, Brägger U, Zwahlen M, Lang NP A systematic review of the survival and complication rates of resin-bonded bridges after an observation period of at least 5 years. Clin Oral Implants Res. 2008; 19:131-141 https://doi.org/10.1111/j.1600-0501.2007.01527.x
Thoma DS, Sailer I, Ioannidis A, Zwahlen M, Makarov N, Pjetursson BE A systematic review of the survival and complication rates of resin-bonded fixed dental prostheses after a mean observation period of at least 5 years. Clin Oral Implants Res. 2017; 28:1421-1432 https://doi.org/10.1111/clr.13007
Pjetursson BE, Tan K, Lang NP, Brägger U, Egger M, Zwahlen M A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years. Clin Oral Implants Res. 2004; 15:625-642 https://doi.org/10.1111/j.1600-0501.2004.01117.x
Jung RE, Zembic A, Pjetursson BE, Zwahlen M, Thoma DS Systematic review of the survival rate and the incidence of biological, technical, and aesthetic complications of single crowns on implants reported in longitudinal studies with a mean follow-up of 5 years. Clin Oral Implants Res. 2012; 23:2-21 https://doi.org/10.1111/j.1600-0501.2012.02547.x
Husain J, Burden D, McSherry P, Morris D, Allen M National clinical guidelines for management of the palatally ectopic maxillary canine. Br Dent J. 2012; 213:171-176 https://doi.org/10.1038/sj.bdj.2012.726
Stewart JA, Heo G, Glover KE, Williamson PC, Lam EW, Major PW Factors that relate to treatment duration for patients with palatally impacted maxillary canines. Am J Orthod Dentofacial Orthop. 2001; 119:216-225 https://doi.org/10.1067/mod.2001.110989
Becker A, Chaushu S Success rate and duration of orthodontic treatment for adult patients with palatally impacted maxillary canines. Am J Orthod Dentofacial Orthop. 2003; 124:509-514 https://doi.org/10.1016/s0889-5406(03)00578-x
Fekonja A Prevalence of dental developmental anomalies of permanent teeth in children and their influence on esthetics. J Esthet Restor Dent. 2017; 29:276-283 https://doi.org/10.1111/jerd.12302
Jeong KH, Kim D, Song YM, Sung J, Kim YH Epidemiology and genetics of hypodontia and microdontia: a study of twin families. Angle Orthod. 2015; 85:980-985 https://doi.org/10.2319/052814-376.1
Agurto SP, Nicholson C, Del Sol M Proposal of anatomical terms for alterations in tooth size: ‘Microdontia and macrodontia’. Int J Morphol. 2019; 37:375-378
Alachioti XS, Dimopoulou E, Vlasakidou A, Athanasiou AE Amelogenesis imperfecta and anterior open bite: Etiological, classification, clinical and management interrelationships. J Orthod Sci. 2014; 3:1-6 https://doi.org/10.4103/2278-0203.127547
Kuroda S, Katayama A, Takano-Yamamoto T Severe anterior open-bite case treated using titanium screw anchorage. Angle Orthod. 2004; 74:558-67
Reichert I, Figel P, Winchester L Orthodontic treatment of anterior open bite: a review article—is surgery always necessary?. Oral Maxillofac Surg. 2014; 18:271-277 https://doi.org/10.1007/s10006-013-0430-5
The adult orthodontic–restorative interface. Part 2: treatment strategies for the management of developmental conditions Christopher Stagles Robert Smith Graeme Bryce Dental Update 2025 51:10, 677-682.
Authors
ChristopherStagles
BDS, MScD(Orth), MOrth, RCSEd, MFGDP, Specialist in Orthodontics; Defence Primary Healthcare (Dental), Defence Centre for Rehabilitative Dentistry, Aldershot
This is the second article in a three-part series that discusses joint orthodontic–restorative care for the adult patient. Part 2 considers the clinical presentations, challenges and strategies for developmental conditions presenting in adulthood, including the management of hypodontia, ectopic canine teeth and disorders of tooth structure.
CPD/Clinical Relevance:
The challenges and treatment strategies for providing orthodontic–restorative care for an adult patient presenting with developmental conditions and anomalies are outlined.
Article
The presence of developmental conditions and anomalies within the adult patient presents specific challenges to the clinical team providing orthodontic–restorative care pathways. This article outlines these challenges and suggests treatment strategies.
Hypodontia
Hypodontia is the developmental absence of one or more permanent teeth excluding third molars, with an overall prevalence of 6.4%.1 Many patients with hypodontia are identified in childhood, including those associated with broader syndromes, for instance: cleft lip and palate (CLP), ectodermal dysplasia and Down's syndrome. Late presentation in adulthood can be linked to failing primary teeth, changes in aesthetic expectations, poor access to dental services as a child, or a deliberate decision to delay treatment for options that are only possible once skeletal maturity is reached, such as dental implant placement or orthognathic treatment. Patients may also present with relapse or complications associated with previous treatments for their condition. In such presentations, close liaison with the previous care provider is essential to provide insight into why previous treatments were not successful and to help shape the future plan to avoid repeat failure.
Hypodontia is often associated with microdontia, interdental spacing, retention of primary teeth, rotations or tilting of teeth adjacent to the affected site, ectopic or unerupted teeth, and over eruption of unopposed teeth. Affected patients may also present with challenging interocclusal relationships, retroclination of the anterior teeth, deep overbites, and absence of canine guidance on excursive movements.2 These features are often exacerbated in the adult patient with untreated hypodontia due to the increased time for unfavourable tooth movement to occur.
Treatment options for developmentally missing teeth include:
The acceptance of missing teeth with management of retained primary teeth as appropriate;
Space closure;
Space redistribution/opening for a restorative intervention.
Sites in the anterior dentition (aesthetic zone)
The upper lateral incisor is the second most commonly absent tooth (24% of total), with bilateral absence being more frequent than unilateral.2 This can present specific challenges owing to the high impact of spacing in the aesthetic zone.
A common approach to orthodontic–restorative space closure is the alignment of maxillary canines within the site of developmentally missing lateral incisors. Orthodontic space closure is often preferrable because it reduces the requirement for prosthetic units, lowers the long-term maintenance burden and has been shown to achieve aesthetic results that are viewed more favourably by patients and lay people.3 However, in general, canines differ from lateral incisors by having a more convex labial form, a cuspal tip rather than incisal edge, narrower gingival emergence, and lower shade values. These factors should be considered when planning whether a canine can be successfully disguised as a lateral incisor. Orthodontically, the appearance of the canine can be amended by adding negative root torque to improve the labio-palatal angle, and limited extrusion to align the gingival margins with the central incisors, accepting that excessive movement can create an occlusal interference because the canine tooth is likely to be thicker and more convex. Restorative camouflage may include bleaching, enameloplasty to reduce the convexity or cuspal tip, and composite resin additions to create mesial/distal marginal ridges and an incisal edge.4
If canines are used to replace the lateral incisors, there usually follows a requirement to move and align the maxillary first premolars into the usual canine position, prior to camouflaging them as canine teeth. This is not always viable if the alveolar bone width is insufficient to accommodate the more mesial position of a two-rooted tooth without perforation of the cortical plate. The bicuspid anatomy of maxillary premolars may also ‘trap’ them within the occlusion, and achieving the required mesial movement may require the use of bite raising devices or composite resin occlusal stops at increased vertical dimension. Premolars are smaller than canines, with a higher and less convex emergence profile. This size discrepancy may be managed orthodontically via rotation of the tooth, to create increased mesio-distal width and intrusion (with or without crown lengthening) to appropriately align the zenith of the gingival margin level. Subsequently, a canine-like tooth can normally be created by the reduction of the premolar palatal cusp, along with the addition of composite resin to widen the tooth and create a more convex labial surface and cusp tip. In the highly aesthetically driven patient, with high lip line and gingival show, crown lengthening surgery may also be required to align emergence profiles with golden proportions.
If primary canines are present and stable, composite resin may be added to restore lost tooth structure, or to disguise as an adult successor.5 However, consideration must be given to whether composite additions will reduce the prognosis of the primary tooth, particularly if increased functional occlusal forces lead to increased rates of root resorption, and earlier tooth loss. Adult patients may often present with primary canines of poor prognosis, where retention is no longer viable.
Options to restore the spaces left by developmentally absent teeth are described in Table 1. When movement of teeth is required to redistribute space, the restorative objectives will normally be to provide a fixed prostheses that is aesthetic and conservative to the remaining dentition (Figure 1). Whether the patient is having a resin-bonded bridge (RBB) or implant, the orthodontist should aim to create a minimum 6.5–7 mm of inter-tooth/radicular space within lateral incisor sites. In this way, the patient could still choose to have an implant at a later date. In cases with crowding or increased overjet, it may also be necessary to create additional space within the arch, with extractions or molar distalization. While implants with narrower platform diameters (3 mm) may be employed when this inter-tooth space cannot be achieved,6,7 less is known about the longer-term survival of narrow implants exposed to high levels of occlusal force, for instance in patients with parafunctional habits.8 Narrower platform implants may also make it more difficult for the dental technician to achieve an aesthetic emergence profile, without over-contouring the restoration and compromising the cleansibility of the abutment/implant interface,9 which may result in an increased risk of peri-implantitis.10
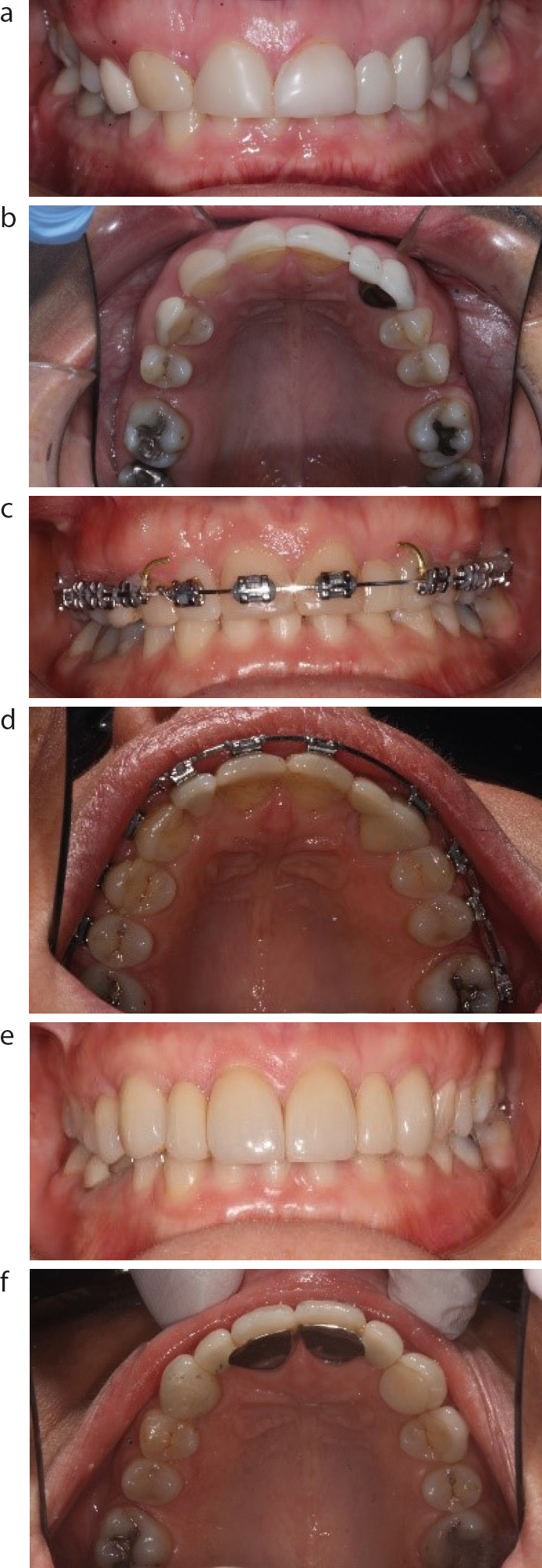
Figure 1.
(a–f) Adult hypodontia patient dissatisfied with previous restorative camouflage of missing UR2 and UL2. Orthodontics used to close posterior spaces, reduce overbite and retract canines to create symmetrical spaces for UR2 and UL2. Restorative treatment included crown lengthening surgery, resin-bonded bridges, and minimally preparative porcelain labial veneers for the UR1 and UL1.
Intervention
Indications
Benefits
Risks
Anticipated success
Removable partial denture (RPD)
Multiple missing teeth.
Unstable primary disease.
Interim prosthesis during definitive care pathway
Minimally invasive
May be poorly tolerated
Range: 50–60%16,17 at 10-years. However, 40% of RPD not worn unless replacing anterior teeth
Resin-bonded bridge (RBB)
Sufficient enamel with absence of developmental defects such as amelogenesis imperfecta
Sufficient coronal structure on abutment tooth (at least equivalent to dimensions of the pontic) Pontic clear of occlusion on excursive guidance movements and excessive occlusal forces (to reduce the risk of debond) Periodontal stability and adequate root length/support Site unsuitable for dental implant placement Parafunctional habits controlled
Good survival/success Minimally invasive
Debond Reduced survival in posterior sites Metal shine through/discolouration of the abutment tooth
88% at 5 years18 91.4% at 5 years to 82.9% at 10 years19
Fixed bridge
Heavily restored adjacent teeth or enamel disorders that render RBB approaches unpredictable Site not suitable for dental implant placement Parafunctional habits controlled
Good survival/success Aesthetics and occlusion may be easier to control
Endodontic complications Restorative spiral, leading to eventual loss of supporting abutment tooth/teeth
The success of RBBs can be dependent on the quality of the tooth surface that is available to bond to, which is often poorer in adult patients owing to previous damage (caries/trauma/tooth wear) and the presence of existing restorations. Full coverage retainer wings with opaque luting cements and pre-cementation media blasting is recommended to maximize bond strength. RBBs can be cemented high in occlusion so long as the excursive movements are controlled. Cantilever designs can be prone to rotational relapse if orthodontic retention is inadequate.
Sites in the posterior dentition
Excluding the third permanent molar, the lower second premolar is the most common developmentally missing tooth. This is an anomaly that is often unilateral11 and may result in centreline shift and localized crowding. Where the aesthetic requirements are reduced, the maintenance of primary teeth is a viable medium to long-term option12 because many teeth are still present in patients’ fourth decades and beyond.13 Retained primary molars commonly show some form of infra-occlusion, attributed to ankylosis,14 which increases the risk of over-eruption of the opposing tooth and mesial/distal tipping of the adjacent permanent teeth.15
Where loss of a primary molar is necessary, or desirable, orthodontic space closure may require the extraction of other, potentially healthy teeth to maintain centrelines, preserve the occlusion and reduce the mechanical interference from opposing cusps. Space closure in the upper arch is more suited to Class II occlusions when overjet reduction is required, and Class III relationships favour space closure in the lower jaw. It should also be considered that retained lower second primary molars are larger than their adult successors, therefore it can be difficult to fully close these large spaces in adult patients, especially if bone defects are present. The use of bone-supported mini-screws to provide anterior anchorage support can be used to minimize undesirable movements, and are often more predictable in adults owing to an increased bone density.
Ectopic canines
It is uncommon for the presence of ectopic canines not to be identified and managed in childhood. However, adults with ectopic canines may seek treatment when either concerns emerge regarding the risk of the ectopic tooth to the adjacent roots (e.g. pressureinduced root resorption), or if the primary tooth is no longer viable. Within the adult patient, interceptive treatment via extraction of the primary canine (and spontaneous space closure) is not possible, and treatment options are limited to accepting the ectopic canine in situ, orthodontic alignment (potentially requiring surgical exposure) or extraction.22
Ectopic canines that are most favourable for alignment will normally have mesial inclination and lie within 14 mm proximity of the canine site occlusal plane.23 Even if the tooth is favourably positioned, the success of alignment is reduced by the increased incidences of ankylosis and slower rates of tooth movement found in adult patients.24 In addition, ectopic canines can also be subject to malformations (Figure 2) or discolouration, which may pose unknown challenges to disguise within the smile line. Subsequently, patients over 30 years of age should be carefully consented before attempting to align an ectopic tooth, in all but the most favourable positions.
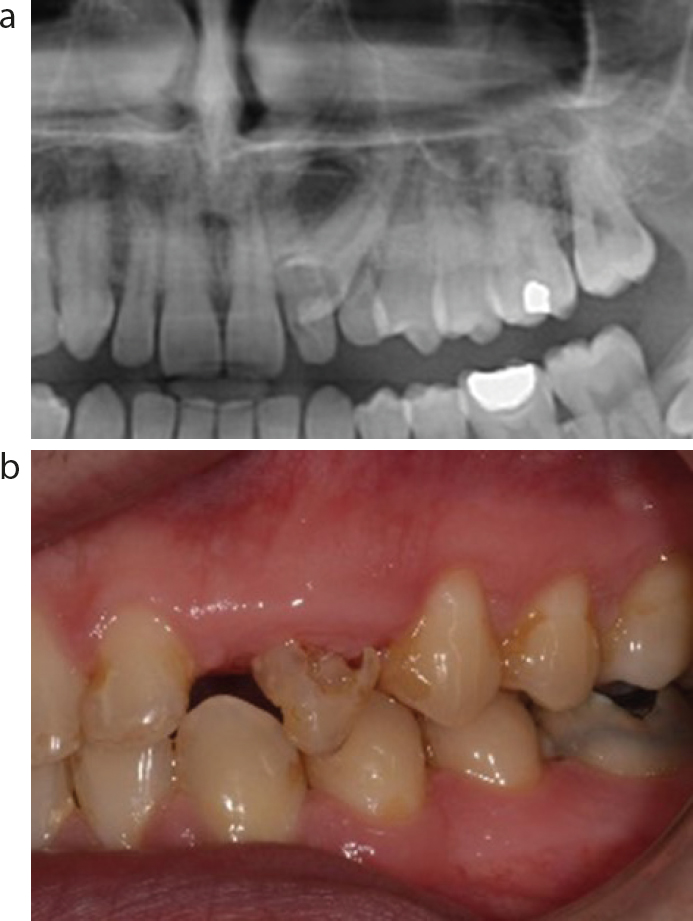
Figure 2.
(a,b) Palatal-positioned ectopic canine with abnormal appearance of crown on radiograph. Clinical presentation with severe hypomineralization and resorption, following exposure and alignment.
In cases with generalized crowding, extraction of the ectopic canine and orthodontic space closure can produce aesthetic results with a lower maintenance requirement. A small amount of residual space often remains following alignment owing to the mismatch in mesio-distal widths between the upper and lower arch, and restorative disguise of first premolar and/or the lateral incisors is often necessary (Figure 3). The extraction of other teeth within the arch should be considered for centreline correction and management of occlusal relationships. Correction of the vertical position of teeth in the opposing arch following over-eruption is often required. It should also be considered that surgical extraction of ectopic canines in adult patients may leave a significant bony defect, which complicates future dental implant placement, and less frequently presents issues with orthodontic space closure (Figure 4).
Figure 3.
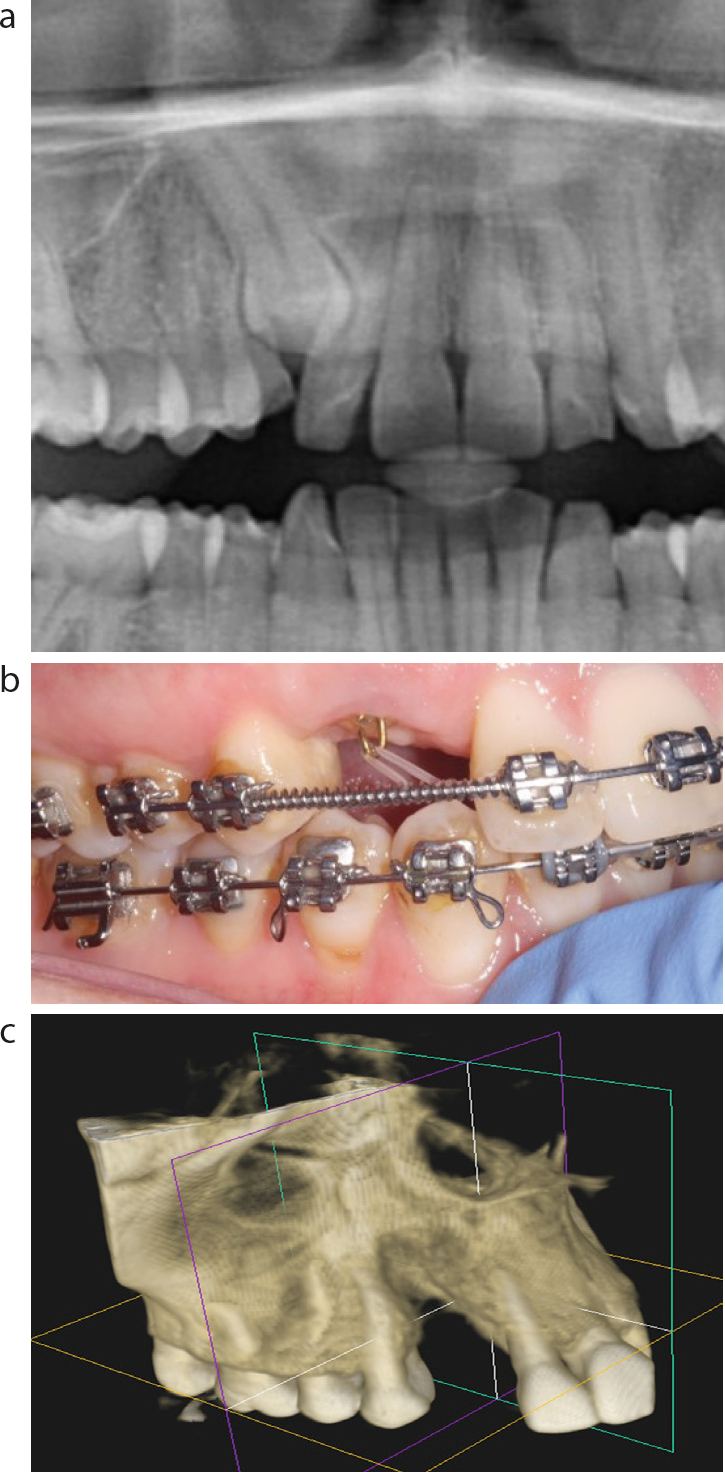
(a–f) Extraction of worn primary, and ectopic adult canine teeth with orthodontic space closure in a case with Class II buccal segment relationship. Residual space on LHS camouflaged with composite addition to premolar.Figure 4.
(a–c) Attempted alignment of ectopic canine in a 40 year old adult patient. Minimal movement was achieved following exposure and application of orthodontic forces. Surgical extraction resulted in a significant bone defect, contra-indicating implant placement.
If the ectopic tooth is to be left in situ, even though continued movement in adulthood is uncommon,22 it is still important to confirm the ectopic tooth's three-dimensional position, so that the risk of root resorption to adjacent roots can be assessed. The presence of an unerupted canine will also often preclude other orthodontic tooth movement in the affected arch, or dental implant placement.
Canines are also the teeth most affected by transposition (interchange in the position of two teeth within the same quadrant of the dental arch) with an incidence of 0.1–0.5%.25 Such transpositions can normally be disguised using the enamel-shaping and composite additions discussed above.
Developmental disorders of tooth structure
Developmental abnormalities may affect tooth dimensions, and the quality and form of enamel, dentine or cementum, with an array of genetic and environmental causes reported for these. The most commonly presenting conditions are microdontia, amelogenesis imperfecta (AI) and dentinogenesis imperfecta (DI). Anomalies are typically identified in childhood with treatment instigated for poor aesthetics, sensitivity, and an increased risk of caries or tooth fracture. Adults will often require maintenance and repair of previous restorative interventions, causing additional complications if orthodontic tooth movement is desired.
As previously discussed, microdontia is often associated with hypodontia and has a prevalence that varies with population ethnicity, but is approximately 3%.25,26 Microdontia may be localized, for instance limited to maxillary lateral incisors (peg laterals) or, more rarely, have a generalized distribution.28 In simple cases, most microdonts can be treated conservatively with direct composite additions to improve the crown contours and reduce interproximal or vertical spaces (Figure 5), either before or after orthodontic treatment provision.
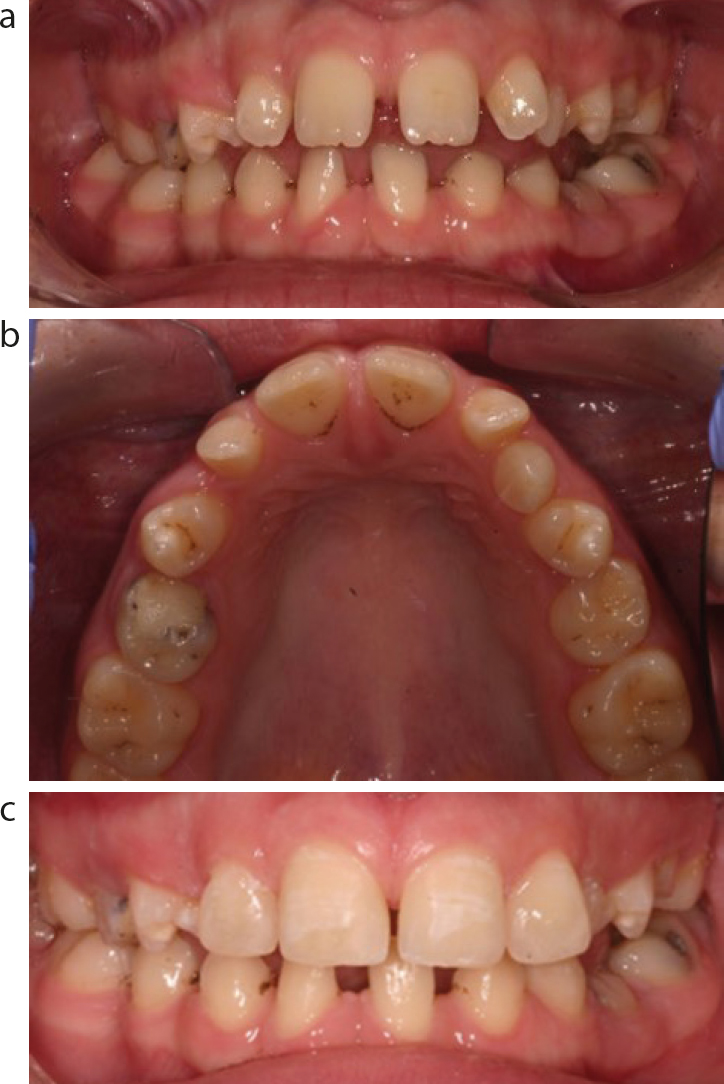
Figure 5.
(a–c) Young adult patient with conical shaped incisors, severe hypodontia including absence of UR3, UL3 and unilateral retained primary canine. Composite additions UR2–UL2 to aid bracket placement and visualization of anterior alignment, prior to bond-up.
The prevalence of AI varies within different populations but has been estimated as <0.5% globally.29 AI has multiple subtypes, and numerous classifications have been proposed which, at their simplest, can be classified as defective prismatic structure (hypomineralization, hypocalcification) or reduced enamel structure (hypoplasia). Adhesive bonding is less predictable within the hypomineralized variants, impacting the predictability of both conventional orthodontic bracket placement and restorative treatments. Assessing the relative predictability of adhesive bonding can be estimated via either the assessment of existing composites, or by evaluating the degree of ‘frosting’ achieved following trial etching of the enamel.
AI may also be associated with spacing, abnormal tooth position and eruption, and malocclusion including anterior open bite (AOB).30 The inability to be able to harness skeletal growth in adult patients limits management options, and can be beyond conventional orthodontic camouflage. The use of bone-anchored mini-screws to provide anchorage for posterior intrusion, has been reported as an alternative to orthognathic correction in less severe cases.31,32 Restorative-only approaches, using composite additions to the incisal edges, may also offer a solution for dentitions that have undergone additional tooth wear (Figure 6).33
DI may be classified as:
Type 1, as a component of osteogenesis imperfecta;
Type 2, the most frequently reported subtype with an incidence of 1:6000–1:8000; or,
Type 3, limited to the Brandywine population in Maryland.34
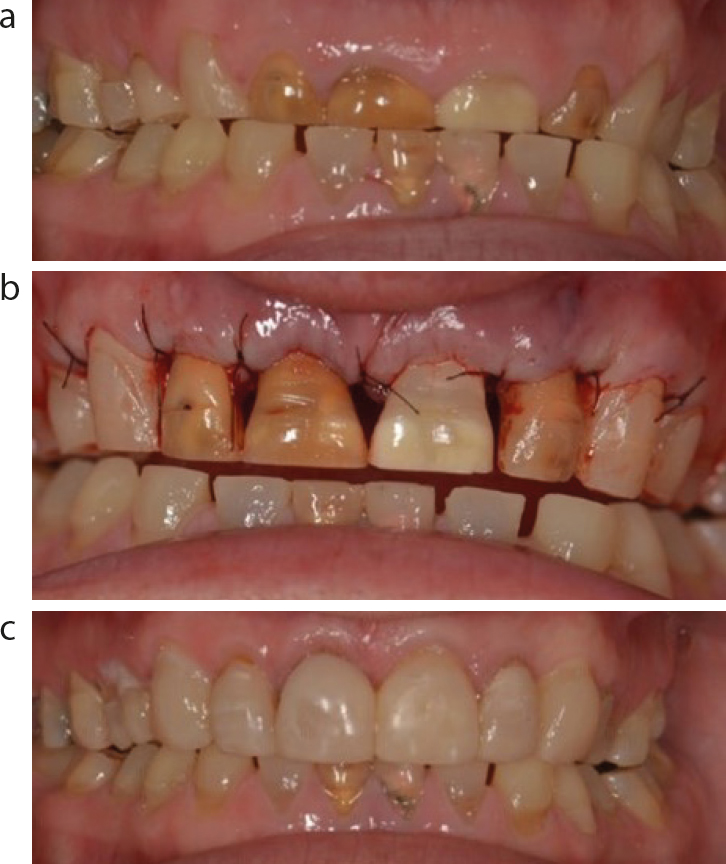
Figure 6.
(a–c) Amelogenesis imperfecta complicated by tooth wear (attritional) and Class III incisal relationship. Managed with crown-lengthening to aid orthodontic bracket placement, non-vital bleaching UR2 UR1 UL2 and direct composite veneers.
DI is associated with a range of dental features that include short roots, bulbous pulp horns, opalescent grey/bluish coronal discolouration, early tooth surface loss, dental caries and endodontic complications.35 Tooth movement is extremely challenging for this patient cohort, owing to the short roots, difficulties with bonding to tooth structure and high frequencies of endodontic complications. Subsequently, orthodontic provision for these patients (whether adolescent or adult) is rarely reported, and is likely to have limited utility, with treatment limited to restorative-only approaches as previously described.
Summary
Older patients with developmental dental anomalies can be particularly challenging to manage owing to a delayed presentation or the failure of previous care. A combined orthodontic–restorative approach can be used to achieve functional and aesthetic outcomes while preserving dental tissues. The preferred restorative care plan should be agreed at an early stage, because this will inform the tooth movements required, and the relative risk, complexity and duration of the overall treatment package.
The third article in this series outlines the challenges and presents orthodontic–restorative treatment solutions for adult patients with compromised and injured dentitions.