Sandler C, Al-Musfir T, Barry S Guidelines for the orthodontic management of the traumatised tooth. J Orthod. 2021; 48:74-81 https://doi.org/10.1177/1465312520977498
Levin L, Day PF, Hicks L International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: general introduction. Dent Traumatol. 2020; 36:309-313 https://doi.org/10.1111/edt.12574
Bourguignon C, Cohenca N, Lauridsen E International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent Traumatol. 2020; 36:314-330 https://doi.org/10.1111/edt.12578
Bach N, Baylard JF, Voyer R Orthodontic extrusion: periodontal considerations and applications. J Can Dent Assoc. 2004; 70:775-780
Andreasen JO, Andreasen FM Root resorption following traumatic dental injuries. Proc Finn Dent Soc. 1992; 1:95-114
Malmgren O, Goldson L, Hill C Root resorption after orthodontic treatment of traumatized teeth. Am J Orthod. 1982; 82:487-491
Reis A, dos Santos JE, Loguercio AD, de Oliveira Bauer JR Eighteen-month bracket survival rate: conventional versus self-etch adhesive. Eur J Orthod. 2008; 30:94-99 https://doi.org/10.1093/ejo/cjm089
Raghavan S, Abu Alhaija ES, Duggal MS White spot lesions, plaque accumulation and salivary caries-associated bacteria in clear aligners compared to fixed orthodontic treatment. A systematic review and meta-analysis. BMC Oral Health. 2023; 23 https://doi.org/10.1186/s12903-023-03257-8
Goymen M, Topcuoglu T, Topcuoglu S, Akin H Effect of different temporary crown materials and surface roughening methods on the shear bond strengths of orthodontic brackets. Photomed Laser Surg. 2015; 33:55-60 https://doi.org/10.1089/pho.2014.3818
Hemmings KW, Darbar UR, Vaughan S Tooth wear treated with direct composite restorations at an increased vertical dimension: results at 30 months. J Prosthet Dent. 2000; 83:287-293 https://doi.org/10.1016/s0022-3913(00)70130-2
Gulamali AB, Hemmings KW, Tredwin CJ, Petrie A Survival analysis of composite Dahl restorations provided to manage localised anterior tooth wear (ten year follow-up). Br Dent J. 2011; 211 https://doi.org/10.1038/sj.bdj.2011.683
Nohl FS, King PA, Harley KE, Ibbetson RJ Retrospective survey of resin-retained cast-metal palatal veneers for the treatment of anterior palatal tooth wear. Quintessence Int. 1997; 28:7-14
Andreasen FM, Pedersen BV Prognosis of luxated permanent teeth – the development of pulp necrosis. Endod Dent Traumatol. 1985; 1:207-220 https://doi.org/10.1111/j.1600-9657
Mirabella AD, Artun J Prevalence and severity of apical root resorption of maxillary anterior teeth in adult orthodontic patients. Eur J Orthod. 1995; 17:93-99
Alhadainy HA, Flores-Mir C, Abdel-Karim AH Orthodontic-induced external root resorption of endodontically treated teeth: a meta-analysis. J Endod. 2019; 45:483-489 https://doi.org/10.1016/j.joen.2019.02.001
Azim AA, Griggs JA, Huang GT The Tennessee study: factors affecting treatment outcome and healing time following nonsurgical root canal treatment. Int Endod J. 2016; 49:6-16 https://doi.org/10.1111/iej.12429
Sorensen JA, Martinoff JT Clinically significant factors in dowel design. J Prosthet Dent. 1984; 52:28-35
Camp LR, Todd MJ The effect of dowel preparation on the apical seal of three common obturation techniques. J Prosthet Dent. 1983; 50:664-666 https://doi.org/10.1016/0022-3913(83)90206-8
Maximiano GS, de Carvalho GM, Felipe Ferreira FFDC Comparative analysis of the biomechanical behavior of the maxillary central incisors restored with glass fiber post and cast metal post and core submitted to orthodontic forces: a study with finite elements. Am J Orthod Dentofacial Orthop. 2024; 165:46-53 https://doi.org/10.1016/j.ajodo.2023.06.025
Aimetti M, Garbo D, Ercoli E Long-term prognosis of severely compromised teeth following combined periodontal and orthodontic treatment: a retrospective study. Int J Periodontics Restorative Dent. 2020; 40:95-102 https://doi.org/10.11607/prd.4523
Artun J, Urbye K The effect of orthodontic treatment on periodontal bone support in patients with advanced loss of marginal periodontium. Am J Orthod Dentofacial Orthop. 1988; 93:143-148
Morris JW, Campbell PM, Tadlock LP Prevalence of gingival recession after orthodontic tooth movements. Am J Orthod Dentofacial Orthop. 2017; 151:851-859
Jati AS, Furquim LZ, Consolaro A Gingival recession: its causes and types, and the importance of orthodontic treatment. Dental Press J Orthod. 2016; 21:18-29
Slutzkey S, Levin L Gingival recession in young adults: occurrence, severity, and relationship to past orthodontic treatment and oral piercing. Am J Orthod Dentofacial Orthop. 2008; 134:652-656 https://doi.org/10.1016/j.ajodo.2007.02.054
Joss-Vassalli I, Grebenstein C, Topouzelis N Orthodontic therapy and gingival recession: a systematic review. Orthod Craniofac Res. 2010; 13:127-141 https://doi.org/10.1111/j.1601-6343.2010.01491.x
Mehta L, Tewari S, Sharma R Assessment of the effect of orthodontic treatment on the stability of pre-orthodontic recession coverage by connective tissue graft: a randomized controlled clinical trial. Quintessence Int. 2022; 53:236-248 https://doi.org/10.3290/j.qi.b2407815
The Adult Orthodontic–Restorative Interface. Part 3: Dental Trauma and Acquired Disease Robert Smith Christopher Stagles Graeme Bryce Dental Update 2025 51:11, 748-754.
Part 3 of this three-part series outlines the specific challenges associated with providing orthodontic–restorative treatment in adult patients experiencing dentitions injured by dental trauma or acquired disease.
CPD/Clinical Relevance:
Optimal management of patients with injured dentitions may necessitate a joint orthodontic–restorative approach.
Article
The dentition may incur injury, acutely via dental trauma, or chronically via the progression (or treatment) of diseases that include: dental caries, tooth wear (TW) and periodontitis. Injury may result in loss of tooth structure, impaired quality of enamel and dentine, endodontic disease, tooth displacement, and fracture. For traumatic injuries, orthodontics can aid dental rehabilitation, particularly for re-aligning luxated teeth (that were not repositioned following displacement) or for extruding teeth with crown fractures, to create sufficient coronal dentine for restoration. While orthodontic therapy may assist in the management of damaged teeth, it poses additional risks, which must be accounted for within the treatment planning process.1 This article outlines the challenges, and presents orthodontic–restorative treatment solutions for adult patients with injured dentitions.
Dental trauma
Approximately one-third of adults have experienced at least one episode of dental trauma2 and it is not uncommon for some patients to have suffered multiple traumatic insults to their adult dentitions. While trauma can have an immediate effect on both the dental and supporting tissues (Table 1), it may also initiate late-presenting conditions (including resorption, pulp necrosis and calcific metamorphosis), which can make both orthodontic and restorative care more complex.1
Crown fracture* is a fracture involving enamel and dentine
Crown–root fracture* is a fracture involving enamel, dentine and cementum
Root fracture is a fracture involving cementum, dentine and pulp
Alveolar fracture is a fracture of the alveolar bone
Extrusive luxation is displacement of a tooth out if its socket in the coronal direction
Lateral luxation is displacement of a tooth in a lateral direction, usually associated with fracture or compression of the socket wall
Intrusive luxation is displacement of a tooth in the apical direction into the alveolar bone
Avulsion is the complete displacement of a tooth from its socket
(adapted from Bourguignon et al3).*Where pulp is exposed, the prefix ‘complicated’ is added (e.g. complicated crown fracture, or complicated crown-root fracture).
Management of non-displaced teeth with reduced supragingival tooth structure
Teeth with uncomplicated crown fractures will often have sufficient tooth structure for bonding, although where such teeth need to be moved orthodontically, patients should be made aware that the application of orthodontic forces may lead to propagation of cracks and fractures. In turn, cracks/fractures may result in pulpal complications or discolouration (either due to ingress of extrinsic staining compounds via cracks, or from intrinsic sources secondary to pulpal complications).
For teeth with up to 50% loss of supragingival dentine, composite build-up is normally sufficient to restore the tooth function and aesthetics, as well as enable orthodontic bracket positioning (as applicable). For teeth with over 50% loss of supragingival dentine, composite build-up may not be predictable, particularly if the fracture line/cavity margin extends subgingivally. In such circumstances, there is a range of options that may be employed to expose additional supragingival tooth structure (Table 2). One option in such circumstances is orthodontic extrusion, and when coupled with crown lengthening surgery, may result in the exposure of sufficient supragingival dentine for predictable restoration (Figure 1). Considerations for orthodontic extrusion of teeth include: adequacy of root length; periodontal health; quality of residual dentine; and, sufficient root diameter to avoid overly scalloped emergence profiles and unaesthetic ‘black triangles’. It may be difficult to bond orthodontic brackets to broken down teeth/roots: these may require a temporary build-up of the exposed portion of root with glass-ionomer cement or composite resin. For severely damaged teeth, root canal treatment +/- post placement and a temporary crown may be necessary to facilitate bracket positioning/bonding.
Treatment
Advantages
Disadvantages
Gingivectomy (via simple surgical excision, electro- or laser-surgery)
Increase in supragingival tooth tissue
Within healing phase, gingival tissue likely to ‘rebound’.No increase in supra-crestal tooth tissue, and restorative margins may impinge upon the supracrestal attachment.
Resective crown lengthening of both gingival and alveolar complex
Increase in supra-crestal tooth tissue, and re-establishment of supra-crestal attachment at a more apical position
If single tooth is crown lengthened in isolation, this may result in asymmetric aesthetic deficit or bony deficit, therefore, there is often the requirement to extend, and ‘blend-in’, the osseous re-contouring to adjacent teeth.
Orthodontic extrusion +/- subsequent resection of the periodontium
Movement of tooth to a more coronal position
Required treatment time can be up to 6-months for this single aspect of the care pathwayRequirement for appliance wearRequirement for suitable teeth for anchorageTooth may not move (e.g. if ankylosed)May require localized crown lengthening subsequent to orthodontics (if the dento-aveolar complex moves coronally with extruded root)The emergence of definitive restorations may be difficult to predict and can be overly scallopedRisk of black triangle spaces between restorations/crowns
Surgical extrusion (only suitable in cases of acute intrusion injury)
Efficient repositioning of intruded tooth
Not suitable in cases of delayed presentationPotential for damage to tooth via pressure from forceps (if tooth cannot be repositioned by hand)Requirement for splinting (post-repositioning)
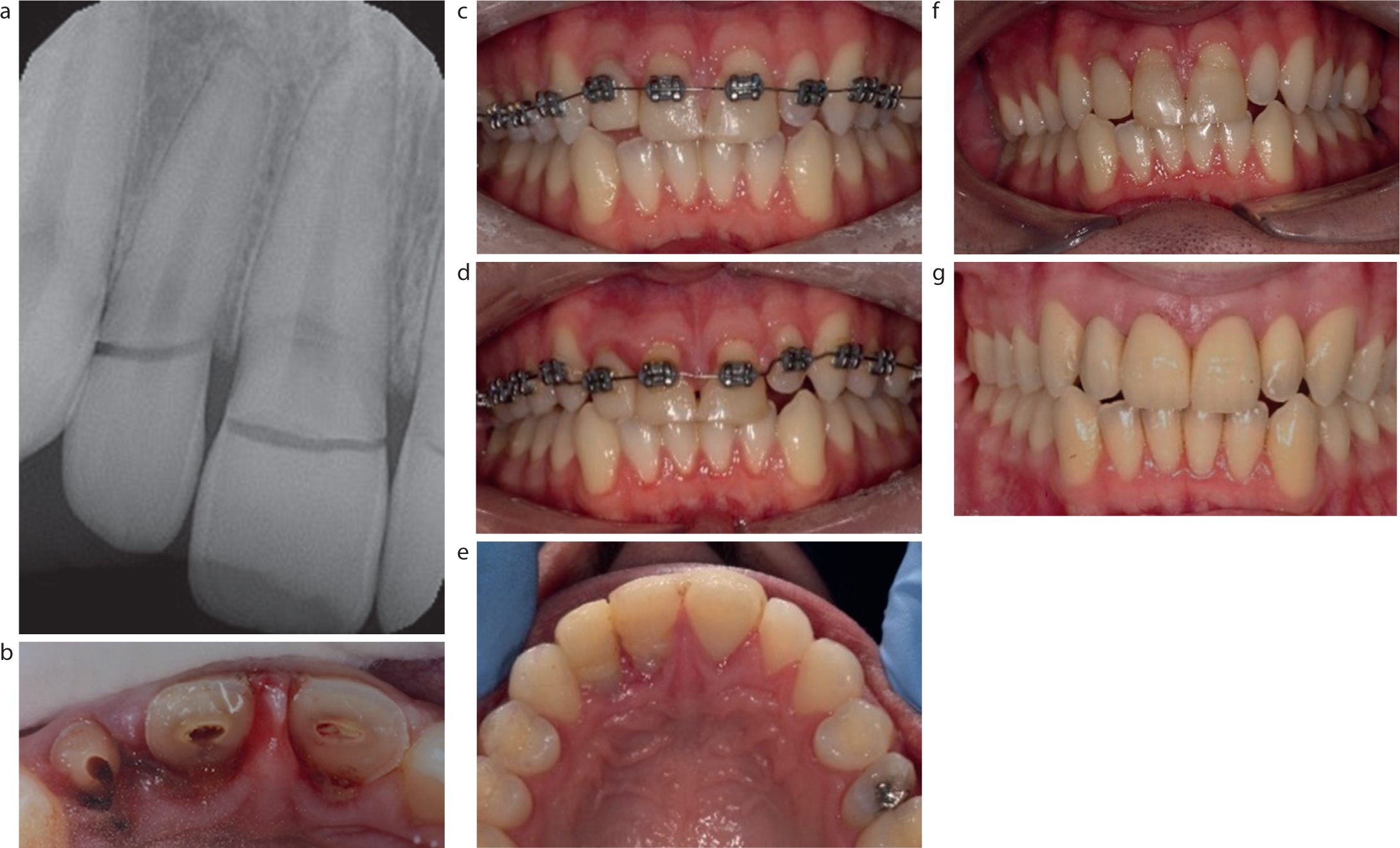
Figure 1.
(a–g) Trauma resulting in multiple crown root fractures, with subgingival margins. Managed with root canal treatment UR2, UR1, and UL1; temporary composite resin build-ups; and orthodontic alignment of maxillary arch with extrusion UR2–UL1. Subsequent crown-lengthening surgery and post/core lithium-disilicate crown placement UR2–UL2.
Management of traumatically displaced teeth
Displacement of teeth or root fractures may complicate or preclude predictable restoration. Available management options for such situations are summarized in Table 3. Orthodontics can reposition teeth that have suffered intrusive, extrusive or lateral luxations, which have not been managed appropriately immediately post injury. For orthodontic extrusion of teeth, the migration of the gingival margin and supporting alveolar bone crest is thought to be related to the speed of tooth movement. Rapid extrusion, with greater forces, is typically associated with minimal tissue migration (where the speed of tooth movement exceeds the physiological adaptation rate), whereas a slower movement will generally see the gingival crest move with the tooth crown;4 however, in practice, variable results can be seen (Figure 2).
Clinical situation
Potential restorative challenges
Pre-restorative management options
Extrusive luxation
Occlusal interferenceReduced crown-root ratio if significant tooth preparation required prior to restoring within golden proportions
Surgical repositioning (if feasible to manipulate root back into socket).Orthodontic intrusion
Lateral luxation
Occlusal instability and tooth movement
Surgical repositioning (if feasible to manipulate root back into socket)Orthodontic repositioning
Intrusive luxation
Reduced clinical crown heightLoss or apical migration of contact points between injured and adjacent teeth resulting occlusal instability and tooth movement
If ≤3 mm intrusion, allow spontaneous re-eruption. If no re-eruption within 8 weeks reposition orthodonticallyIf 3–7 mm intrusion, reposition surgically (ideally) or orthodonticallyIf >7 mm intrusion, reposition surgically
Avulsion
Bone resorption and gingival recessionOcclusal instability and tooth movement
Socket reconstruction surgery with particulate graft
Root fracture
Tooth mobilityEndodontic complications
Accept position of apical and coronal portionsExtraction +/- socket preservation
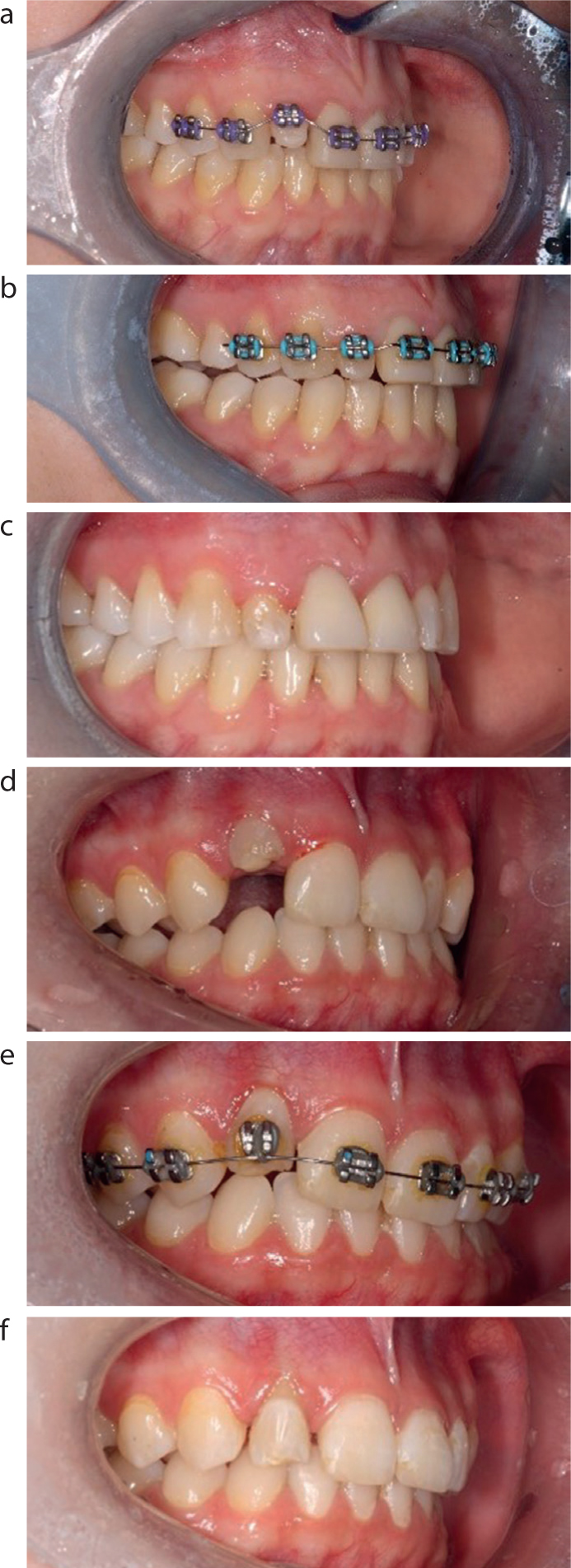
Figure 2.
(a–f) Two patients with intruded lateral incisors treated with similar straight wire mechanics and light nickel–titanium wires to extrude. Note differences in gingival margin at finish, despite comparable forces being used.
Traumatically compromised teeth are prone to resorption processes5 that include: external cervical resorption, surface resorption, replacement resorption, and inflammatory related root resorption (secondary to endodontic infection). Resorption is often asymptomatic and can be accelerated with orthodontic forces, leading to additional restorative complexities and/or tooth loss. For teeth assessed to have an increased risk of resorption, it is recommended that during orthodontic treatment, root length and morphology are monitored with radiographs at 6-month intervals; allowing intervention/alteration of the treatment as indicated by findings.6 Ankylosed teeth with replacement resorption cannot be orthodontically repositioned. Failure to diagnose ankylosis may result in unwanted anchorage, and consequently, during fixed appliance therapy, may lead to intrusion of the adjacent teeth. Conversely, on occasion, such anchorage can be used to the patient's advantage, for example, in cases when intrusion is required to reduce a deep overbite.
Dental caries and tooth wear
Dental caries and tooth wear (TW), along with invasive restorative interventions for management of these conditions, results in a reduction of coronal tooth structure. In the case of vital teeth, the properties of the remaining tooth structure may be altered via the physiological response of the odontoblasts to these insults, resulting in dentine sclerosis via deposition of secondary dentine. Such changes within the dentine, as well an overall reduction in enamel, negatively impact the quality of adhesive bonding procedures. However, in general, orthodontic brackets for fixed appliance systems can be predictably bonded to enamel, dentine or composite.7
Prior to embarking on a complex orthodontic–restorative care pathway it is paramount that the oral hygiene regimen is optimized and any primary disease is stabilized; particularly as the presence of orthodontic appliances adds to the oral hygiene maintenance burden. The use of clear orthodontic aligners (versus fixed appliances) may reduce plaque retention and the risk of decalcification.8 However, such appliances cannot be used in all clinical situations.
The adult patient will often present with pre-existing amalgam and ceramic restorations; materials that do not readily lend themselves to bonding of orthodontic brackets. Amalgam restorations that interfere with desired bracket positioning can be managed via either their replacement with composite, use of a banded attachment, or bypassing the tooth if minimal movement is required. Particular care should be taken within the application of orthodontic forces to unsupported cusps/coronal structure, as this may result in bulk fracture coupled with bracket debond.
Although ceramic brackets can be bonded to ceramic crowns using a silane coupling agent, the bond may repeatedly fail. In such cases, bonding may be more predictable if the ceramic crowns are removed and replaced with provisional laboratory- or chairside-constructed composite crowns (Figures 3 and 4).9
Figure 3.
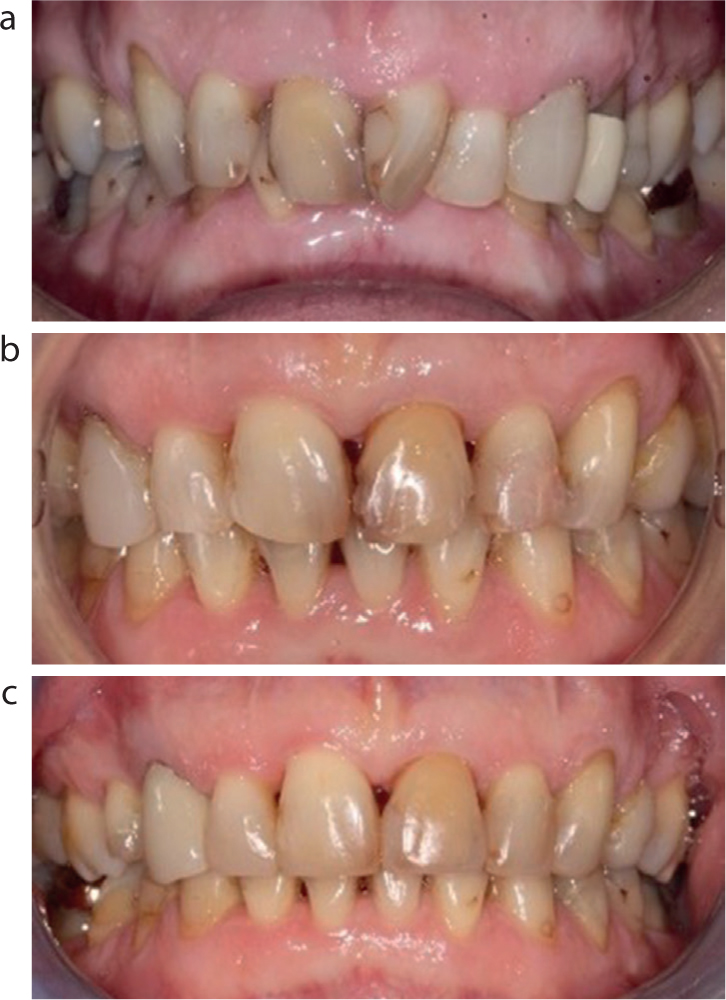
(a–c) Treatment of patient with a heavily restored dentition and attachment loss from previous periodontal disease. Teeth with the poorest prognosis were extracted and existing ceramic crowns were replaced with composite provisional crowns to facilitate bonding. Note the post-treatment black triangles present in both the maxillary and mandibular anterior sextants.Figure 4.
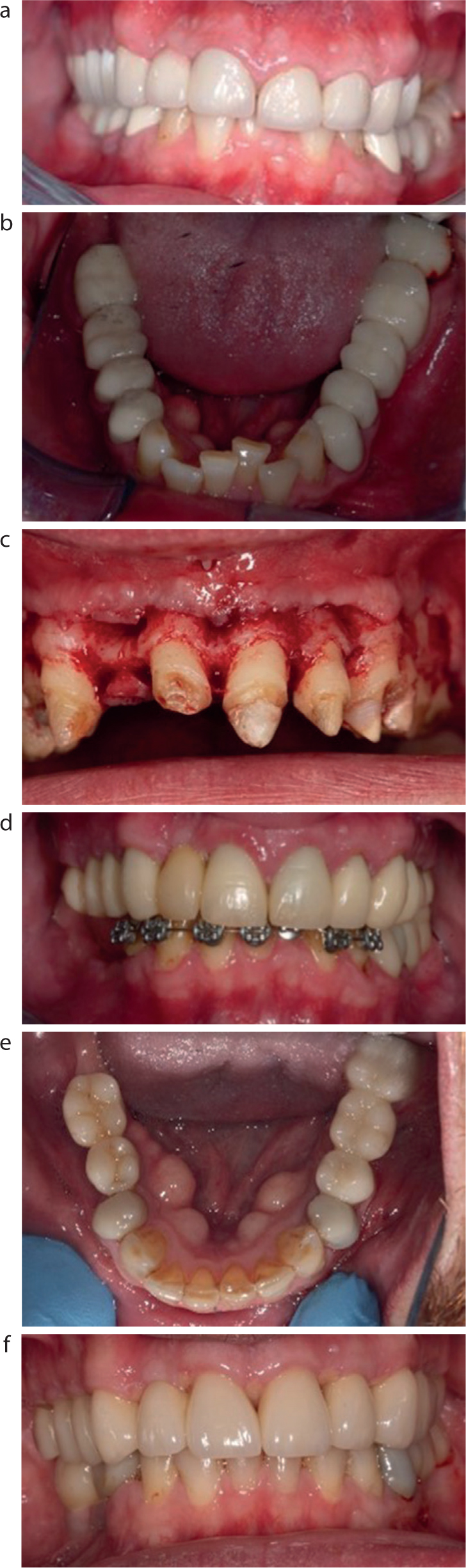
(a–f) Patient with multiple failed crowns and fixed bridges, complicated by a gingival cant and lower arch crowding. Treatment included crown-lengthening surgery, composite provisional crowns/bridges and orthodontic alignment of mandibular labial sextant. Definitive restorations were via implant-supported crowns to replace unrestorable LR5, LR6 and tooth-supported zirconia/ceramic crowns and bridges.
Provisional indirect composite restorations may also be indicated where there is pre-existing fixed bridgework, and/or the requirement to adjust the vertical dimension of the occlusion (Figure 4). A joint orthodontic–restorative approach will often offer the most predictable way of adjusting the pattern of occlusal forces exerted during lateral and protrusive excursive movements, ensuring they are sufficiently controlled to improve the survival of the definitive restorations and surrounding teeth.
It is now accepted that localized TW, with loss of inter-occlusal space, can be managed restoratively using either direct or indirect restorations bonded at an increased vertical dimension, with re-establishment of occlusal contacts via vertical axial re-alignment.10-12 A restorative-only approach for TW becomes increasingly difficult with severe malocclusion, particularly with inter-incisal relationship discrepancies, and orthodontics may improve the predictability of the subsequent definitive restorations.
In mild Class II incisor relationship cases with a 3–5 mm overjet, anterior contacts can be achieved using composites applied to both the labial and palatal surfaces of the mandibular and maxillary anterior teeth respectively. For overjets beyond this limit, there becomes an increased requirement for restorations with thick, overly contoured palatal surfaces, which can cause lisping and present difficulties with cleaning (Figure 5). Orthodontic therapy to reduce an overjet or improve angulation of the incisors in the adult patient will often require camouflage of the skeletal base, typically via extraction of premolars, retraction of the upper anterior teeth and/or proclination of the lower labial segment.
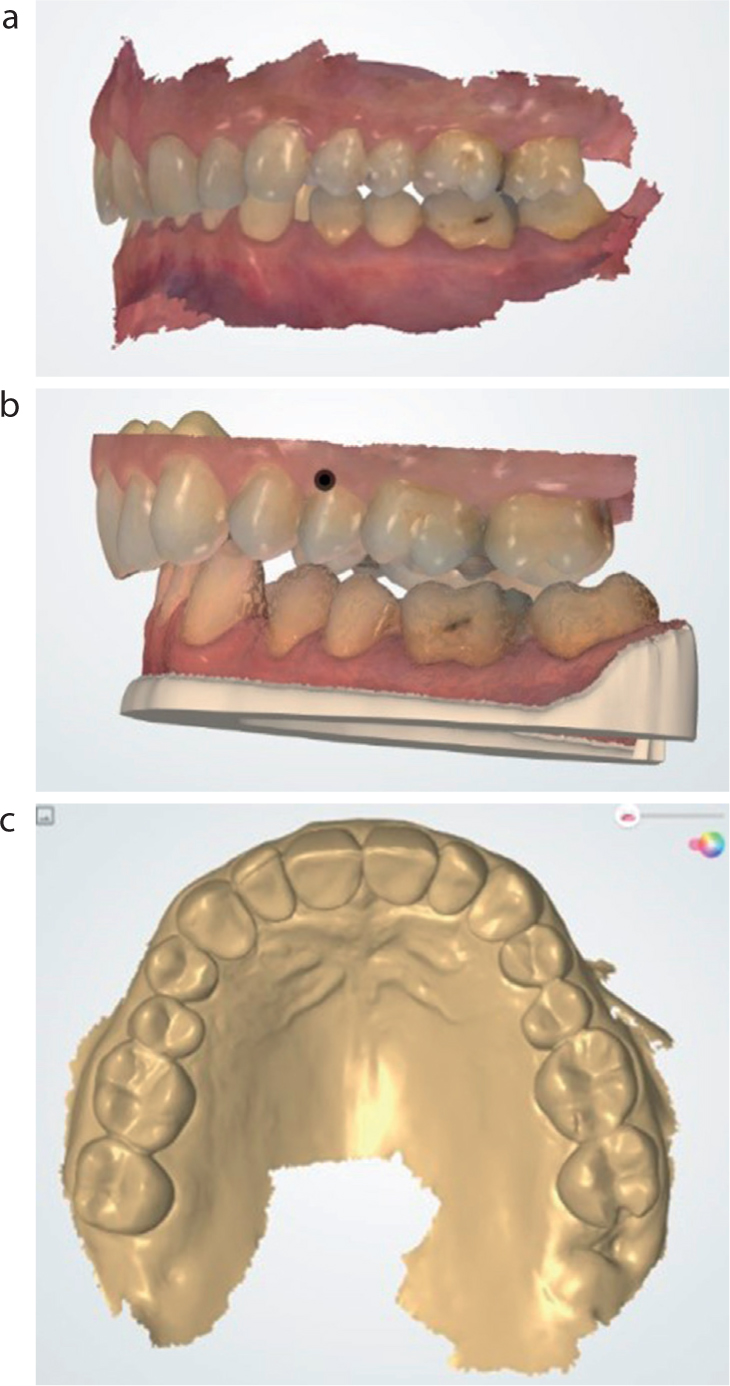
Figure 5.
(a–c) Digital work-up for palatal veneers for a patient with a Class II division 2 occlusion with palatal TW. Note the increased overjet incurred by the mandible moving to its retruded axial position and the subsequent thickness of the palatal veneers from UR3 to UL3. This scheme was mock-trialled in the patient, who subsequently elected for pre-restorative orthodontic alignment, with upper premolar extraction, to reduce the overjet and subsequent size of palatal veneers.
Where management of TW is required in Class III incisal relationships (particularly with ‘edge-to-edge’ incisors, or postured reverse overjet), there is a requirement for a minimum depth of 2 mm of restorative material thickness both in the labio-palatal/lingual and vertical dimensions. Subsequently, restorations may be overcontoured, with resultant negative impact on aesthetics and speech. For patients who can achieve an edge-to-edge incisal contact, orthodontic appliances can procline the upper labial segment, to re-establish a positive overjet, and achieve sufficient space for restorations to restore lost tooth structure (Figure 6). Proclination and increased arch width will result in additional spacing which should be accounted for within the restorative phase of the plan. If the patient is not able to achieve an incisal edge-to-edge contact, then orthognathic surgery is usually required to modify the skeletal base and facilitate occlusal realignment.
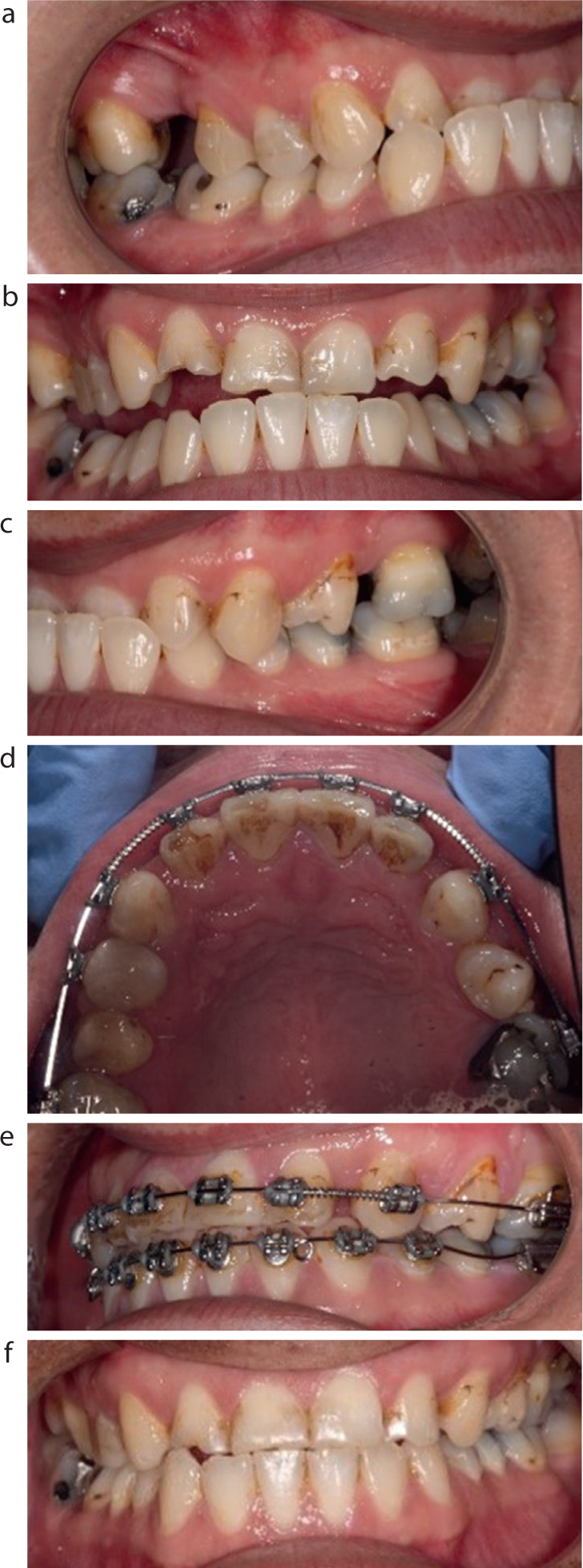
Figure 6.
(a–f) Patient with uneven anterior TW associated with Class III occlusion. Orthodontic treatment to procline upper labial segment and reduce overbite to facilitate direct composite restorations. Rotated premolars were not corrected to minimize space creation in the upper arch.
Endodontic disease
Damage to tooth structure, or displacement of teeth, may lead to pulp necrosis and apical periodontitis,13 which increases the risk of orthodontic-induced root resorption (OIRR).14 However, successfully treated apical periodontitis (via root canal treatment) does not increase the risk of OIRR.15
As outlined in the first article of this series, surrogate measures of pulp and peri-apical status should be used to identify any endodontic related problems, which where present, should be managed via root canal (re)treatment (as applicable) prior to embarking on orthodontic treatment. However, radiographic evidence of healing outcome may not be determinable until 12-months post-operatively.16 Therefore, clinical judgement should be applied as to the timing of commencement of orthodontics. There is also a risk of gutta percha being left within the peri-radicular tissues as the root apex resorbs during movement (Figure 7). This complication can be avoided by obturating short of the terminus, normally to around 1–2 mm from the radiographic apex.
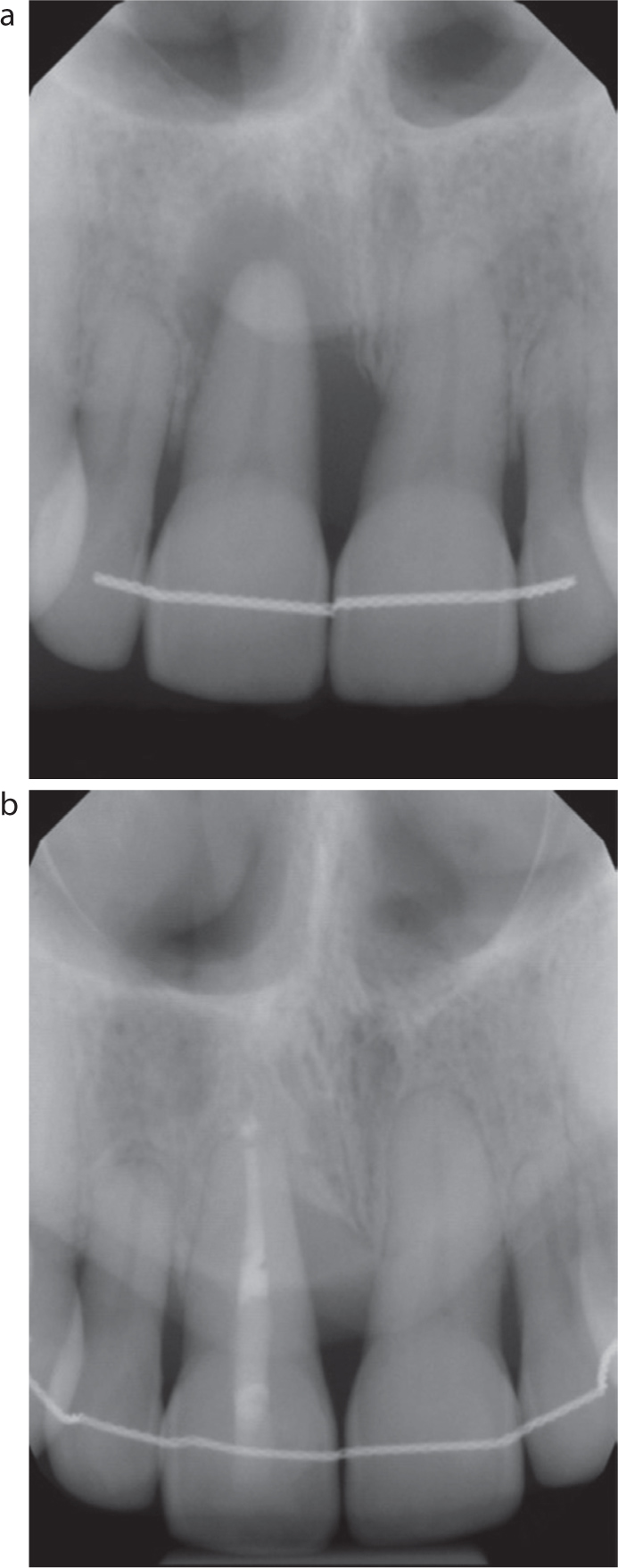
Figure 7.
(a,b) Long cone peri-apicals showing perio-endo involvement of right maxillary central incisor. Root canal treatment and professional mechanical plaque removal achieved partial resolution of the radiolucent lesion. Note the OIRR apical resorption on the maxillary incisors, including the UR1 with associated root filling material outwith the root canal following orthodontic tooth movement.
Where a post is indicated, its length should be at least equal to the height of the crown,17 and 5 mm of root filling should be maintained apically to preserve the seal.18 Root filled teeth with post-retained crowns can be orthodontically moved19 as long as the post is centred within the canal space and has sufficient diameter and extension to avoid debond. Conversely, posts that are too long, generally over two-thirds of the root diameter, or are divergent from the canal space, are at increased risk of root fracture from fixed orthodontic appliances. Restorative modification of the crown-root angle should also be accounted for in the bracket positioning, to ensure that the desired three-dimensional movement is achieved.
Periodontal disease and loss of supporting alveolar bone
In patients with clinical attachment loss secondary to periodontitis, orthodontic treatment can be predictably provided once their periodontal condition has been stabilized.20 Prior to initiation of orthodontic treatment, the patient must be able to demonstrate excellent plaque control, and periodontal health should be regularly (re)assessed via bleeding scores and six-point pocket charting during treatment.
A reduction in bony support is seen in advancing age and comorbidities, and the magnitude of orthodontic forces and vectors must be modified accordingly. Reduced alveolar bone levels move the centre of resistance of the tooth to a more apical position, which in-turn requires more cervical bracket positioning, and/or the use of light forces, and smaller wires to prevent the full expression of the bracket prescription. However, in general, orthodontic tooth movement can be safely employed even in cases with severe attachment loss.21
Following orthodontic treatment, bonded retainers are used for splinting periodontally compromised teeth, stabilizing the ‘jiggling forces’ that can be exacted on teeth via regular insertion and removal of removable retainers. However, the use of bonded retainers must be balanced against increased complexity of patient-delivered plaque control, and the associated propensity for calculus retention associated with fixed retainer wires.
Loss of supporting periodontal soft tissues
There are conflicting views regarding the role that orthodontic therapy may play in gingival recession. Some researchers found a weak correlation between orthodontic treatment and recession,22 while others have advocated that recession can be treated with orthodontics.23 On balance, it is likely that orthodontic therapy can exacerbate recession,24,25 particularly if teeth are being proclined26 or moved bodily, closer to the envelope of alveolar bone. Risk factors for gingival recession include: reduced height of keratinized mucosa (<2 mm), thin gingival phenotypes, high frenal attachments (that displace the gingival margin upon tension of the lip or cheeks), and a more buccal positioning of teeth within the arch. Pre-orthodontic therapies for high-risk sites may include soft tissue augmentations such as free gingival grafts or coronal advancement flaps (with or without connective tissue grafts).27 If tooth extraction is required as part of the orthodontic plan, for example a requirement to removal a single lower incisor, the most compromised tooth should be chosen (which may include teeth that have suffered the greatest amount clinical attachment loss/gingival recession).
Summary
Adult orthodontic care is challenging even within the unrestored dentition. Acquired damage to the tooth and supporting structures increases the complexity and risks of providing care and may reduce the predictability of achieving the desire outcome. Meticulous case assessment and planning is recommended for successful outcomes.