Soparkar CN, Patrinely JR, Cuaycong MJ The silent sinus syndrome. A cause of spontaneous enophthalmos. Ophthalmology. 1994; 101:772-778 https://doi.org/10.1016/s0161-6420(94)31267-x
Aramani A, Karadi RN, Kumar S A study of anatomical variations of osteomeatal complex in chronic rhinosinusitis patients-ct findings. J Clin Diagn Res. 2014; 8:KC01-KC4 https://doi.org/10.7860/jcdr/2014/9323.4923
Ihnat JM, Williams LC, Baum ED, Waldman EH Spontaneous resolution of silent sinus syndrome in a pediatric patient. Otolaryngol Case Rep. 2022; 25 https://doi.org/10.1016/j.xocr.2022.100485
Chang DT, Truong MT A child with silent sinus syndrome and spontaneous improvement after sinus surgery. Int J Pediatr Otorhinolaryngol. 2014; 78:1993-1995 https://doi.org/10.1016/j.ijporl.2014.08.002
Brandt MG, Wright ED The silent sinus syndrome is a form of chronic maxillary atelectasis: a systematic review of all reported cases. Am J Rhinol. 2008; 22:68-73 https://doi.org/10.2500/ajr.2008.22.3118
Babar-Craig H, Kayhanian H, De Silva DJ Spontaneous silent sinus syndrome (imploding antrum syndrome): case series of 16 patients. Rhinology.. 2011; 49:315-317 https://doi.org/10.4193/rhino10.103
Michelle L, Du AT, Abiri A, Kuan EC Clinical manifestations, management, and outcomes of primary silent sinus syndrome: a systematic review. Rhinology.. 2023; 61:297-311 https://doi.org/10.4193/rhin23.028
Rose GE, Sandy C, Hallberg L, Moseley I Clinical and radiologic characteristics of the imploding antrum, or ‘silent sinus,’ syndrome. Ophthalmology. 2003; 110:811-818 https://doi.org/10.1016/s0161-6420(02)01993-0
Petraroli M, Riscassi S, Panigari A Silent sinus syndrome and williams syndrome: two rare diseases found in a pediatric patient. Front Pediatr. 2020; 8 https://doi.org/10.3389/fped.2020.00211
Leidens N, Franco A, Santos MCJ Early-diagnosed silent sinus syndrome and cone-beam computed tomography in a pediatric patient: a case report. J Korean Assoc Oral Maxillofac Surg. 2020; 46:155-159 https://doi.org/10.5125/jkaoms.2020.46.2.155
Kerai T, Ganesan K Are changes in specific landmark anatomy on a panoramic image suggestive of maxillary sinus disease?. Dent Update. 2018; 45:977-984
De Grauwe A, Ayaz I, Shujaat S CBCT in orthodontics: a systematic review on justification of CBCT in a paediatric population prior to orthodontic treatment. Eur J Orthod. 2019; 41:381-389 https://doi.org/10.1093/ejo/cjy066
EzEldeen M, Wyatt J, Al-Rimawi A Use of CBCT guidance for tooth autotransplantation in children. J Dent Res. 2019; 98:406-413 https://doi.org/10.1177/0022034519828701
Yip CC, McCulley TJ, Kersten RC Silent sinus syndrome as a cause of diplopia in a child. J Pediatr Ophthalmol Strabismus. 2003; 40:309-311 https://doi.org/10.3928/0191-3913-20030901-16
Ibáñez Micó S, Armengot Carceller M, Martorell Aragonés A Atelectasia crónica maxilar: causa infrecuente de opacidad radiológica persistente [Chronic maxillary atelectasis: an uncommon cause of persistent radiological opacification]. An Pediatr (Barc). 2005; 63:169-171 https://doi.org/10.1157/13077461
Habibi A, Sedaghat MR, Habibi M, Mellati E Silent sinus syndrome: report of a case. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 105:e32-35 https://doi.org/10.1016/j.tripleo.2007.09.018
Mohindra S, Mohindra S Silent sinus syndrome in a female child with enophthalmos and diplopia. Int J Clin Rhinol. 2014; 7:40-42
Sen D, Arora V, Adlakha S, Miglani H The imploding antrum: an unusual case of nontraumatic painless enophthalmos. Indian J Ophthalmol. 2016; 64:786-788 https://doi.org/10.4103/0301-4738.195015
Keren S, Sinclair V, McCallum E Silent sinus syndrome: potentially misleading features that should be recognized. Can J Ophthalmol. 2023; 58:113-117 https://doi.org/10.1016/j.jcjo.2021.09.018
Dave M, Loughlin A, Walker E, Davies J Challenges in plain film radiographic diagnosis for the dental team: a review of the maxillary sinus. Br Dent J. 2020; 228:587-594 https://doi.org/10.1038/s41415-020-1524-8
Renton T, Durham J, Hill CM Oral surgery II: Part 2. The maxillary sinus (antrum) and oral surgery. Br Dent J. 2017; 223:483-493 https://doi.org/10.1038/sj.bdj.2017.858
Illner A, Davidson HC, Harnsberger HR, Hoffman J The silent sinus syndrome: clinical and radiographic findings. AJR Am J Roentgenol. 2002; 178:503-506 https://doi.org/10.2214/ajr.178.2.1780503
Chojdak-Łukasiewicz J, Paradowski B Facial asymmetry: a narrative review of the most common neurological causes. Symmetry. 2022; 14 https://doi.org/10.3390/sym14040737
Agrawal M, Agrawal JA, Nanjannawar L Dentofacial asymmetries: challenging diagnosis and treatment planning. J Int Oral Health. 2015; 7:128-131
Silent Sinus Syndrome: A Paediatric Condition Diagnosed in the Orthodontic Department Fiona Lourenco Daniel Tyler Nadine Houghton Dental Update 2025 51:9, 658-662.
Silent sinus syndrome (SSS) is defined as unilateral maxillary sinus hypoplasia and orbital floor resorption. This case report highlights a rare paediatric diagnosis of SSS during an orthodontic clinic. The diagnostic orthopantogram (OPG) and cone-beam computed tomography showed complete opacification of the left maxillary sinus. Following referral to the ear, nose and throat (ENT) department, a CT sinus confirmed SSS. Owing to the risk of facial asymmetry in a growing adolescent patient without surgical intervention, functional endoscopic sinus surgery will be used to manage this. This case highlights the importance of a thorough investigation of incidental findings.
CPD/Clinical Relevance: The clinical relevance of early diagnosis of silent sinus syndrome and its implications on facial symmetry is discussed.
Article
Soparkar et al proposed the term silent sinus syndrome (SSS), which is defined as unilateral maxillary sinus hypoplasia and orbital floor resorption.1 This presents as enophthalmos (posterior displacement of the eyeball) and hypoglobus (downward displacement of the eyeball) unrelated to surgery, prior trauma, congenital deformities or other symptoms. A negative pressure gradient is created via chronic obstruction of the osteomeatal complex within the maxillary sinus. The osteomeatal complex is a channel allowing airflow and mucociliary drainage from the anterior ethmoid air cells, the frontal sinus and the maxillary sinus into the middle meatus. This results in hypoventilation. The ipsilateral orbital floor bone is then resorbed, and the maxillary antrum bows.2,34
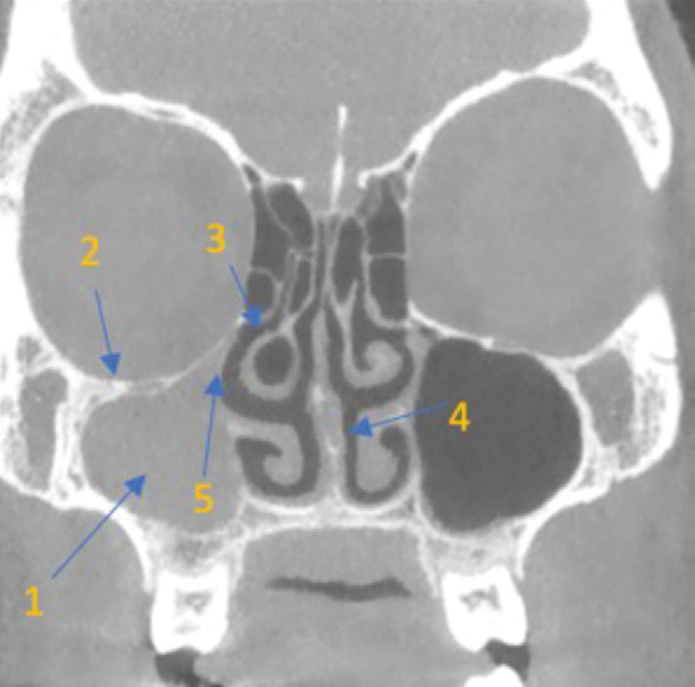
Several case reports or case series describe SSS in the adult population, as it is more common there than in the paediatric population.5,6,7 Unilateral maxillary sinus volume loss and opacification, depression of the ipsilateral orbital floor, blockage of the osteomeatal complex, septal deviation, and/or lateralization of the ipsilateral uncinate process are among the most common radiographic signs (Figure 1).8 Based on the severity of the case, treatment aims to improve sinus aeration. A functional endoscopic sinus surgery is usually the first-line surgical option. More complex cases may require septoplasty or orbital floor reconstruction.3 Some reports suggest spontaneous improvement of enophthalmos is possible.4 However, these are limited to an adult population. This case report discusses a 7-year-old boy who was diagnosed with SSS as an incidental finding during an orthodontic assessment.
Figure 1. Common radiographic signs of silent sinus syndrome. 1: unilateral maxillary sinus volume loss and opacification; 2: depression of the ipsilateral orbital floor; 3: blockage of the osteomeatal complex; 4: septal deviation; 5: lateralization of the ipsilateral uncinate process.
Case report
A 7-year-old boy was referred to the autotransplantation multidisciplinary team for an assessment for premolar transplantation to replace his poorprognosis upper central incisors. The patient had previously sustained a fall from his bicycle onto a pavement at the age of 6. During this, he avulsed his upper central incisors. The patient was seen by the oral and maxillofacial team in A&E, and he presented with an extraalveolar dry time of 1.5 hours, as well as apical root fractures of both teeth. The upper central incisors were replanted. The patient was advised regarding their poor prognosis, including risks of infection and resorption.
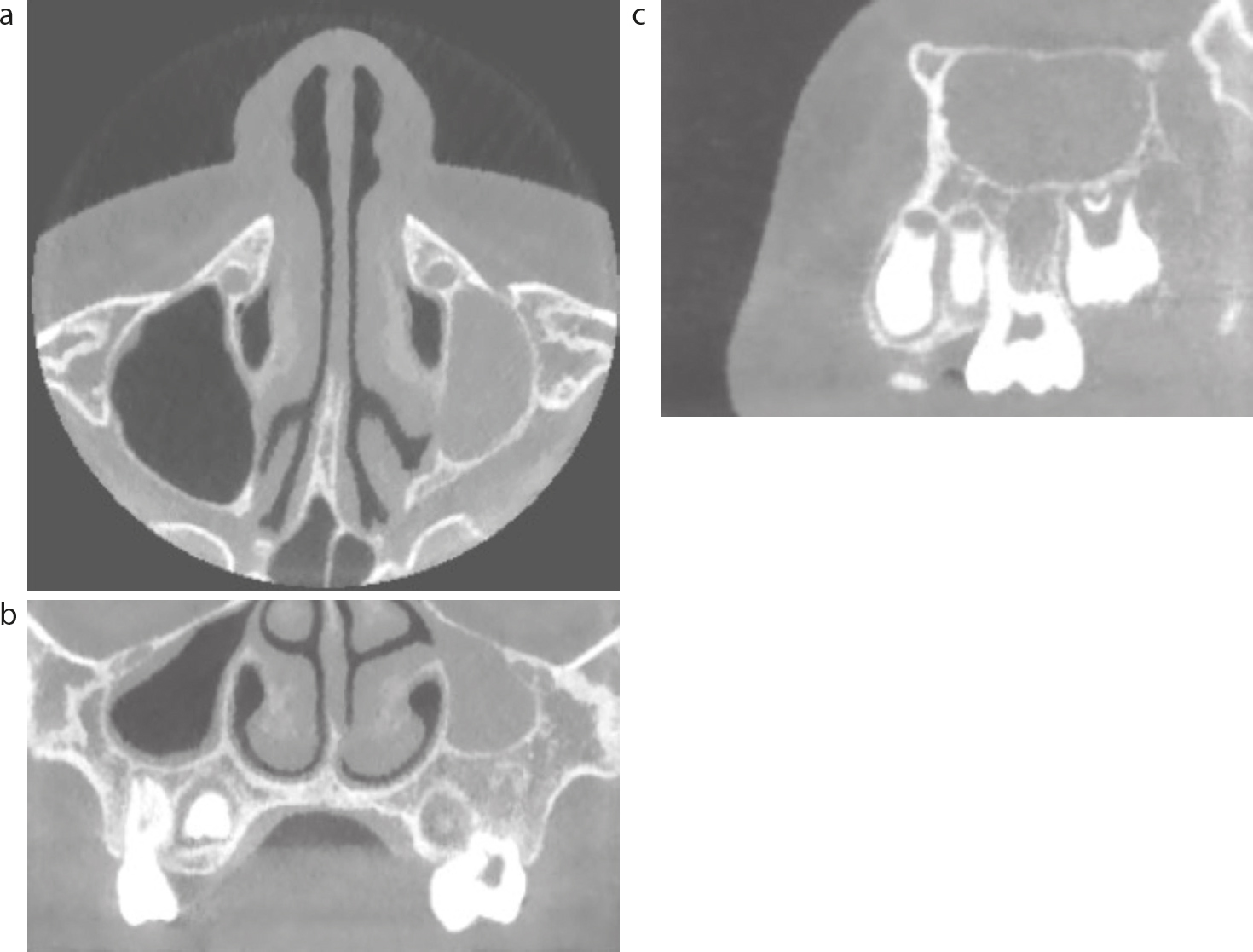
As part of the assessment for autotransplantation and orthodontic treatment, an OPT radiograph (Figure 2) was taken to assess the presence of unerupted teeth and root lengths. A CBCT (Figure 3) was taken to assess the root development and any curvature of potential donor teeth. The OPG and CBCT demonstrated a diminutive and completely opacified left maxillary antrum. No gross inferior displacement of the left orbital floor was demonstrated. This was felt to most likely represent a hypoplastic antrum with mucosal thickening; however, silent sinus syndrome or a more aggressive soft tissue mass could not be entirely excluded. On questioning, the patient did not report experiencing any sinus symptoms. There was no nasal blockage, discharge or pain. His sense of smell and taste was normal, and he had no eye symptoms. On examination, there was no facial asymmetry or enophthalmos. After gaining consent, the patient was then referred to ENT.
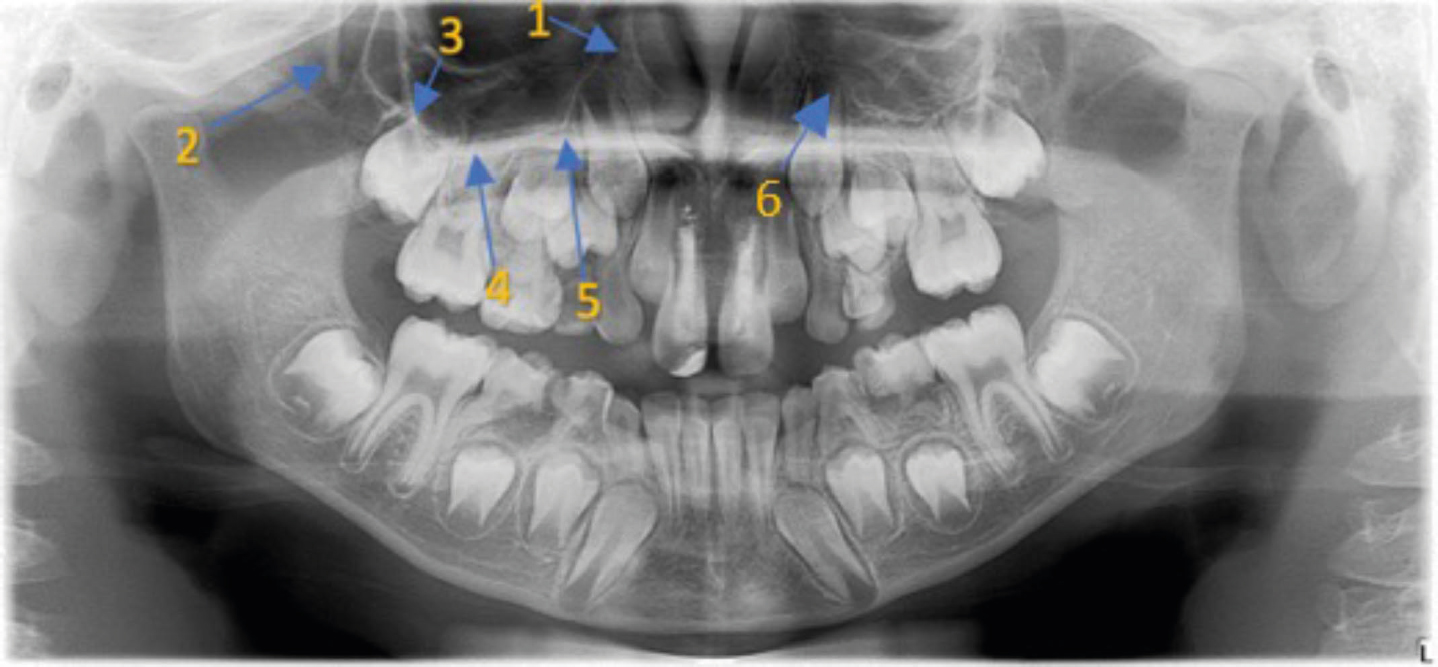
Figure 2. Six key structures on the panoramic radiograph to aid identification of maxillary sinus pathology. 1: anteromedial wall of the maxillary antrum; 2: pterygomaxillary fissure; 3: zygomatic buttress; 4: floor of the antrum; 5: hard palate; 6: radiopacity of the sinus (unilateral versus bilateral).Figure 3.
(a–c) Axial, coronal and sagittal CBCT views of the patient. This CBCT demonstrated a diminutive and completely opacified left maxillary antrum. No gross inferior displacement of the left orbital floor was demonstrated. This was felt to most likely represent a hypoplastic antrum with mucosal thickening; however, silent sinus syndrome or a more aggressive soft tissue mass could not be entirely excluded.
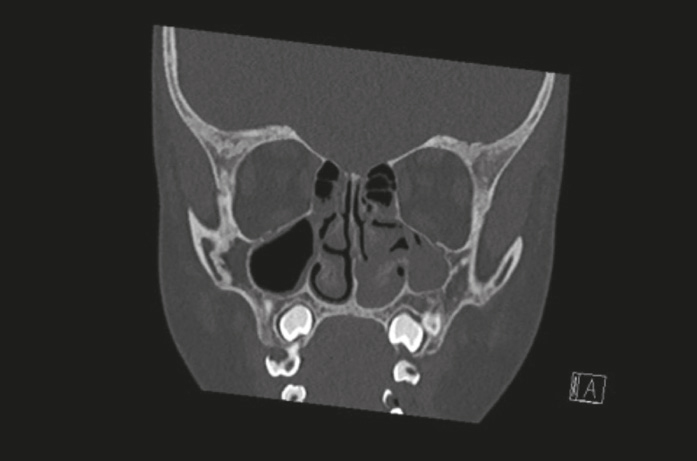
ENT clinical assessment confirmed no asymmetry to palpation in the maxillary area and no asymmetry related to his eyes. Anterior rhinoscopy was within normal limits and fibre-optic nasal endoscopy demonstrated that the septum was deviated into the area of the left middle meatus. There was no evidence of a mass, polyposis or discharge of the middle ear meatus. A CT sinus (Figure 4) confirmed SSS. The patient and parent were informed that although it was asymptomatic, there was a risk that, as the patient's mid-face grew, his un-aerated left maxillary sinus would grow at a lesser rate than the right. This can result in facial asymmetry andenophthalmos. Following discussions of advantages, disadvantages and risks with the patient and the parent, the patient was listed for a functional endoscopic sinus surgery (FESS) in addition to dental treatment. FESS involves the opening of the sinuses under direct visual assessment using minimally invasive techniques.9
Figure 4. Coronal view of the CT sinus carried out by ENT, which demonstrated silent sinus syndrome. The left maxillary sinus is small in relation to the contralateral right side. The middle turbinate appears to distort the uncinate process laterally which obstructs or narrows the maxillary ostium/osteomeatal complex.
Discussion
There is a paucity of case reports on SSS in prepubescent patients. Looking at the findings of a systematic review on SSS, out of the 153 articles included, only 12 featured paediatric cases (Table 1).7 Of these 12 cases, two reported SSS in children as young as 7-years-old. Chang et al described a case of a symptomatic 7 year old who attended due to headaches4 and Petraroli et al described a case of a finding of SSS in a patient with William's syndrome.10 Fonseca et al highlighted a case where a patient was referred to ophthalmology as a result of a unilateral divergent squint and poor vision since childhood. The orbital MRI picked up the signs of SSS. Although this patient had an endoscopic maxillary antrostomy, visual acuity and ocular motility were unchanged.11 This case report is the second SSS finding during a dental assessment. In the first case report, Leidens et al described a similar case in a patient who presented to the orthodontic department with enophthalmos (posterior displacement of the eyeball) and hypoglobus (downward displacement of the eyeball) alongside opacification of the maxillary sinus on the OPG. This was further confirmed with CBCT imaging that showed osteomeatal obstruction with bone deformity.12 This finding on the CBCT report shows the importance of careful assessment of any radiographic imaging as part of the patient assessment.
An OPG is an indispensable part of patient assessment to evaluate the dentition. It is vital to appropriately assess the maxillary sinus, which forms part of this image, based on the dimension requested. Clinicians should aim to identify six key structures on the panoramic radiograph to aid in the identification of maxillary sinus pathology:13
The anteromedial wall of the maxillary antrum;
The pterygomaxillary fissure;
The zygomatic buttress;
The floor of the antrum;
The hard palate;
Radiopacity of the sinus (unilateral versus bilateral).
Figure 2 shows the initial radiopaque changes of the left maxillary sinus of the patient above and outlines the key structures described above. This case highlights the importance of fully assessing OPT radiographs for incidental findings, including assessment of the sinus. When carrying out adjunct imaging such as CBCT imaging, clinicians must always ensure:
The smallest field of view selection that is required;
Choose the lowest possible resolution that will enable diagnosis to be reached;
Ensure appropriate shielding, if required;
Use the lowest combination of tube operating potential and tube current exposure time product.14
In the above case, CBCT imaging was vital to assess root length and development. Research has shown that CBCT imaging increases the treatment predictability in autotransplantation cases.15,16,17,18 In this instance, the CBCT imaging enabled an additional diagnosis. It is prudent to consider how further changes in guidance on the use of CBCT may identify other incidental findings.
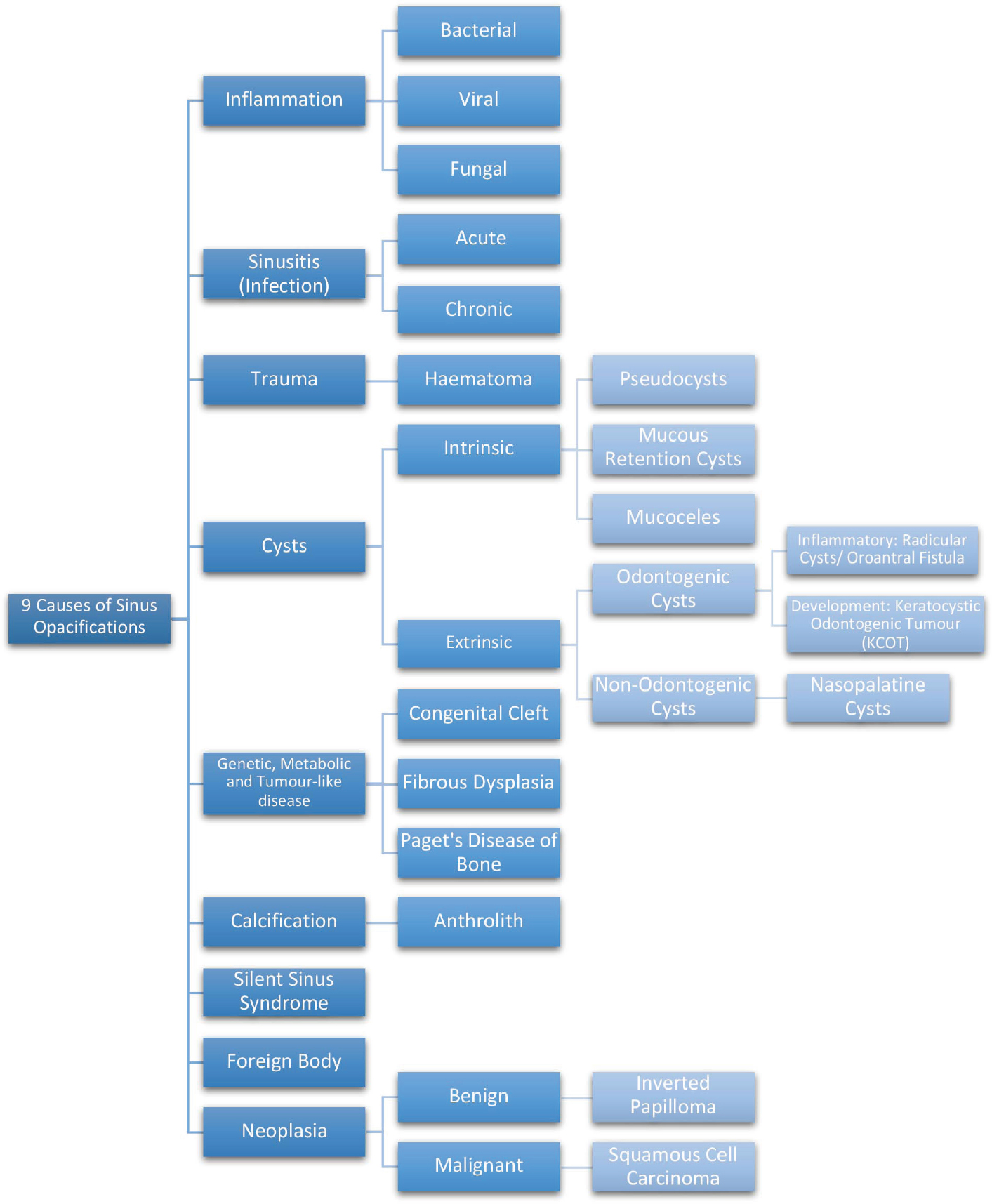
It is, therefore, also vital to consider the differentials for sinus opacifications. The flowchart (Figure 5) summarizes nine differential diagnoses that may cause changes to normal radiographic sinus anatomy. Some common examples are sinusitis (the most common), odontogenic cysts, mucoceles and mucous retention cysts. Some less common differential diagnoses include benign neoplastic disease such as an inverted papilloma (the most common benign neoplasm of the paranasal sinuses) or malignant changes that can cause a radiopaque appearance of the maxillary sinus.27,28,29,30 A full orthodontic assessment includes an analysis of facial asymmetry. As described, SSS can sometimes present as skeletal asymmetry. It is vital to consider the potential causes of facial asymmetry aside from the normal relative asymmetry prevalent in approximately 21–85% of the population.31 Lastly, this case involved the orthodontic, paediatric, ENT and OMFS departments, highlighting the importance of interdisciplinary management.32
Figure 5. A flowchart summarizing nine differential diagnoses that may cause changes to normal radiographic sinus anatomy.
Conclusion
Although SSS is commonly diagnosed in the adult population,4,5,6 this case highlighted the importance of appropriate assessment and differential diagnoses of paediatric patients presenting with similar symptoms. Facial asymmetry assessment is routine for all orthodontic patients. Although the child in this case did not present with facial asymmetry, it highlights the importance of an appropriate differential diagnosis, such as SSS, if presented with enophthalmos or facial asymmetry. Radiographic assessment is a vital addition to clinical assessment to aid treatment planning. It is essential to carry out thorough analysis and reporting of any radiographs taken. This case highlighted the importance of appropriately reporting on images within a clinician's scope and referring externally for reports when required. There is an increasing use of CBCT imaging to aid appropriate treatment planning in dentistry;33 this may increase incidental findings, such as SSS, and aid appropriate early diagnosis and management. Furthermore, where CBCT imaging is used, per current guidelines, clinicians should obtain a report from an appropriately trained dentist with ‘level 2’ training or a radiologist.33 Lastly, this case highlighted the importance of a multidisciplinary approach to provide patients with the best quality of care.