Wagner TP, Costa RS, Rios FS Gingival recession and oral health-related quality of life: a population-based cross-sectional study in Brazil. Community Dent Oral Epidemiol. 2016; 44:390-399
Sinha A, Madhavan S, Ravindra S, Bhat S. Gingival veneer: non esthetics to esthetic smile. J Dent Med Sci. 2014; 13:26-29
Ellis S, Sharma P, Harris I. Case report: aesthetic management of a localised periodontal defect with a gingival veneer prosthesis. Eur J Prosthodont Restor Dent. 2000; 8:23-26
Barzilay I, Irene T. Gingival prostheses – a review. J Can Dent Assoc. 2003; 69:74-78
Emslie R. A case of advanced periodontitis complex. Dent Practitioner. 1955; 5:432-433
Wray D, McCord J. Labial veneers in the management of desquamative gingivitis. Oral Surg Oral Med Oral Pathol. 1987; 64:41-42
Alani A, Maglad A, Nohl F. The prosthetic management of gingival aesthetics. Br Dent J. 2011; 210:63-69
Hickey B, Jauhar S. Gingival veneers. Dent Update. 2009; 36:422-428
Patel M, Nixon P, Chan MF. Gingival recession: part 2. Surgical management using pedicled grafts. Br Dent J. 2011; 211:315-319
Patel M, Nixon P, Chan MF. Gingival recession: part 1. Aetiology and non-surgical management. Br Dent J. 2011; 211:251-254
Allen E, Irwin C, Ziada H Periodontics: 6. The management of gingival recession. Dent Update. 2007; 34:534-542
Disease and related disorders – a report from the Adult Dental Health Survey 2009. 2011. www.ic.nhs.uk
Kassab MM, Cohen RE. Treatment of gingival recession. J Am Dent Assoc. 2002; 133:1499-1506
Antony V, Khan R. Gingival mask – restoring the lost smile. J Dent Med Sci. 2013; 5:20-22
Zalkind M, Hochman N. Alternative method of conservative esthetic treatment for gingival recession. J Prosthet Dent. 1997; 77:561-563
Choudhari P, Pillai A, Shetty S A novel technique of masking gingival recession. J Clin Diagnost Res. 2015; 9:ZD12-ZD14
Needleman I, McGrath C, Floyd P, Biddle A. Impact of oral health on the life quality of periodontal patients. J Clin Periodontol. 2004; 31:454-457
Cunliffe J, Pretty I. Patient's ranking of interdental ‘black triangles’ against the other common aesthetic problems. Eur J Prosthodont Restor Dent. 2009; 17:177-181
British Society of Periodontology. Good Practitioner's Guide to Periodontology. 2016. www.bsperio.org.uk
Patel M, Nixon P, Chan MF. Gingival recession: part 3. Surgical management using free grafts and guided tissue regeneration. Br Dent J. 2011; 211:353-358
Isler SC, Ozcan G, Ozcan M, Omurlu H. Clinical evaluation of combined surgical/restorative treatment of gingival recession-type defects using different restorative materials: a randomized clinical trial. J Dent Sci. 2018; 13:20-29
Lang NP, Adler R, Joss A, Nyman S. Absence of bleeding on probing. An indicator of periodontal stability. J Clin Periodontol. 1990; 17:714-721
Lai Y, Lui HF, Lee SY. In vitro color stability, stain resistance, and water sorption of four removable gingival flange materials. J Prosthet Dent. 2003; 90:293-300
This paper aims to present information about the provision of gingival prostheses or gingival veneers. These appliances are most commonly provided for patients with gingival recession and attachment loss. The paper will highlight the indications and advantages for providing prostheses, and inform the reader of the risks or complications that may arise. The clinical and laboratory stages will be explained and advice provided on maintenance. A case series will demonstrate some of the patient-related benefits and difficulties that can be encountered. A final aspect to the paper will present the results of a survey undertaken in the north-east of England, exploring the provision of these appliances in primary care.
CPD/Clinical Relevance: Good aesthetics relating to the gingival margin can be difficult to achieve and the use of gingival veneers may provide a solution.
Article
A gingival veneer is a removable prosthetic appliance that is worn to replace missing hard and soft tissues, most commonly in the aesthetical upper anterior region of the mouth. The missing soft tissue is often the result of destructive periodontal disease, and this can cause a multitude of concerns for a patient.1 The appliance aims to restore the mucogingival contour for the patient, which can significantly improve dental, gingival and facial aesthetics.2,3 The prosthesis can be made from a range of materials that include hard acrylic resins, or flexible silicone materials.2,4 It covers the alveolus, attached and non-attached gingiva and often extends bilaterally on the labial aspect of the maxillary teeth from the central incisors to the canines or first premolars.
Provision of gingival veneers is not a new treatment concept as it was first introduced in 1955 by Emslie in a post gingivectomy patient,5 where the gingival veneer was worn to mask the unpleasant appearance of gingival recession after the procedure. Historically, gingival veneers were used to replace lost periodontal tissues when other treatment modalities (eg mucogingival surgery or other regenerative surgery) were contra-indicated and showed unfavourable or unpredictable results.4 They have also been used as a delivery vehicle for topical medications in conditions such as hypersensitivity or desquamative gingivitis.6,7 Gingival veneers are generally considered to be a conservative, predictable and relatively inexpensive resolution to unsightly gingival recession in a stabilized periodontally healthy mouth.2,8
Aetiology
Gingival recession is defined as displacement of the gingival margin apical to the cementoenamel junction, with associated exposure of the root surface.9,10,11 In the most recent Adult Dental Health Survey, 73% of adults exhibited recession and vulnerable exposed root surfaces.12
There are a number of causes which can be characterized as either direct (mechanical/physical) influences or indirect, where inflammatory changes in the gingiva can result in recession.10,11 Direct influences of trauma causing recession can be subdivided into a number of different causes which include: inappropriate toothbrushing and flossing techniques, piercings and other foreign bodies, orthodontic tooth movements, unfavourable occlusal schemes, and prosthodontic appliances.11 There is often an underlying anatomical alveolar deficiency, such as a dehiscence or fenestration, that predisposes a patient to recession.9,11,13 Direct causes of recession, mainly from overzealous toothbrushing techniques, affect the buccal surfaces of teeth (Figure 1). Periodontitis is another common cause of recession and attachment loss, more commonly seen across all tooth surfaces. Recession as a result of periodontitis can be due to the disease process as well as its treatment (Figures 2 and 3).9,11
Figure 1. Patient with traumatic induced recession affecting teeth in the upper left quadrant from overzealous toothbrushing.Figure 2. Patient presents with generalized aggressive periodontitis with extensive deep pocketing and associated bleeding on probing. A fixed-fixed three-unit anterior bridge is present in the upper anterior region from UR1 to UL2.Figure 3. Non-surgical treatment of patient in Figure 2 results in significant recession and loss of interdental papilla. The margins of the three-unit bridge are clearly visible due to the extensive attachment loss.
Problems encountered by patients
As a consequence of periodontal disease, a patient may experience significant loss of interdental bone and, with it, loss of the interdental papillae. This can lead to wide, open embrasure spaces between the teeth, which give the appearance of ‘black triangles’.7,14 Patients also usually present with elongated crowns with root exposure and uneven gingival margins.15,16 All of these issues can lead to aesthetic problems for the patient, particularly if there is a high lip line.7, 13 (Figures 4 and 6)
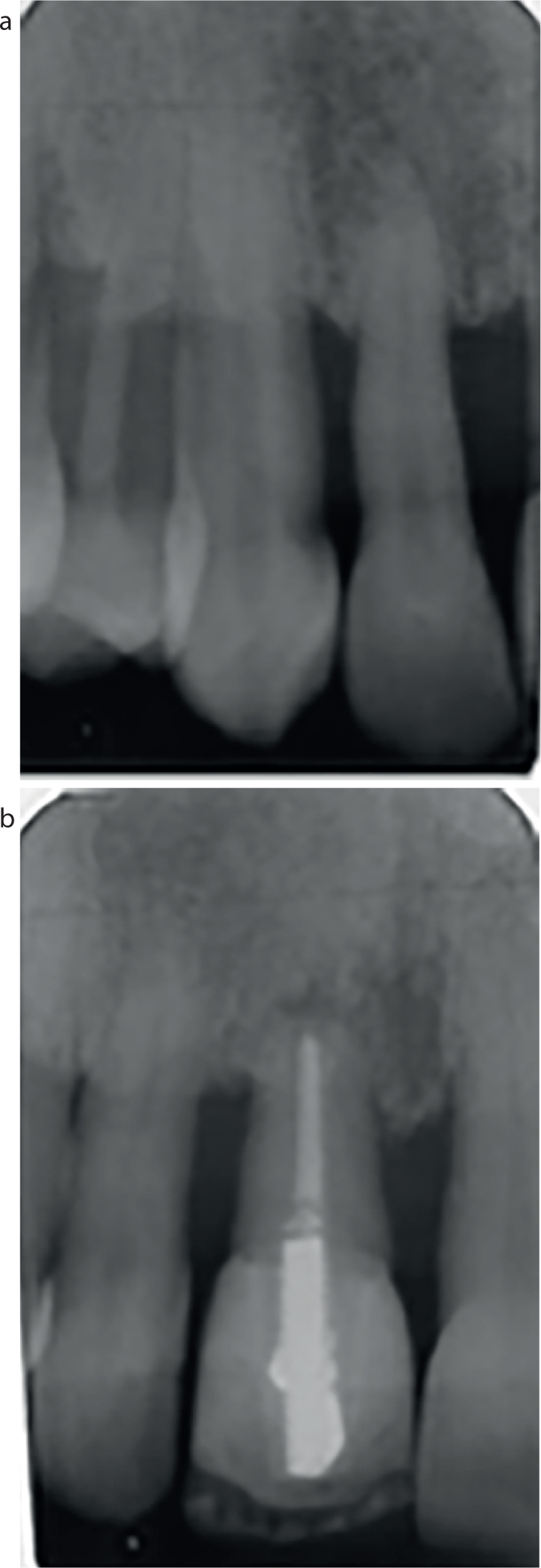
Figure 4. Loss of dental papilla has resulted in ‘black triangle syndrome’, which is extenuated with a high smile line.Figure 5.
(a, b) Upper anterior radiographs of patient in Figure 4 showing advanced bone loss, which has resulted in gingival recession. The endodontically treated upper right central incisor has dubious prognosis.Figure 6. Post-periodontal treatment response with significant loss of attachment and visible ‘black triangles’.
With increasing attachment loss, teeth may become mobile, drift and create diastemas inbetween the teeth; this can have effects on function, making it difficult to eat and chew food. The prognosis of severely affected teeth may be compromised in the long term (Figure 5). Due to drifting of teeth, the soft tissue support and profile may also be negatively affected.
Excluding the unsightly gaps, recession and root exposure can cause dental hypersensitivity to cold air and fluids.13 This can further impair self-performed oral hygiene measures, and can lead to difficulties when undertaking periodontal maintenance and treatment.14,15 Phonetic issues can also be reported due to air escape through the spaces.10 Furthermore, these spaces can also retain food deposits, with the need for a patient to clean interdentally frequently.
For some patients, there may be significant negative impacts on personal self-confidence and quality of life, as patients may feel less confident to smile.2,4 This could have negative psychological effects, as it could be a persistent reminder of their history of periodontitis.1,17 A study in Brazil showed that gingival recession directly affected Oral Health related Quality of Life, particularly when the upper anterior teeth are affected.1 A study conducted in 2009 revealed that below caries and crown margins, the presence of ‘black triangles’ were the third most disliked feature for patients.18
Management and treatment options
For a presenting patient with gingival recession the cause of the condition has to be identified and the aetiology addressed. The patient needs to be informed and fully advised about the condition. During this phase, clinical photographs, study models, and periodontal indices (including measurements of gingival recession) can be utilized to record and monitor changes.11 Oral hygiene advice and coaching techniques, in conjunction with periodontal treatment, are undertaken to stabilize their periodontal condition.11,19 Once stabilized, and depending on the cause, classification (Miller's)19 and severity of recession and attachment loss, there may be a number of treatment options available.2,7,9,14
Conservative treatment options
Direct conservative techniques utilizing composite resin can reduce or close wide embrasure spaces, alter the clinical crown shape, or be used to restore the cervical aspects of the teeth.7,9 Resin can either be tooth-coloured or there is a range of pink composite resins available for restorations at the cervical aspects.7,15
Alternative conservative approaches include the provision of indirect partial interproximal or labial porcelain veneers, or even the provision of full coverage extra-coronal restorations. The intentions of such treatment options are to lengthen the proximal contact areas and lower the initial contact point closer to the tip of the interdental papilla, thereby reducing the ‘black triangle’ appearance (Figures 6 and 7).
Figure 7. Post-restorative outcome of patient in Figure 6, with four linked porcelain fused to metal crowns UR2-UL2.
Mucogingival surgery
This treatment modality tends to be reserved for patients who demonstrate recession as a result of non-plaque induced lesions or stabilized periodontal conditions. Although there have been improvements in surgical managements in recent years, surgery can be unpredictable in certain cases.7,15,16 Several factors affect the outcome of periodontal surgery in these cases, which include the tissue biotype, the size and shape of recession, the Miller's classification19 of the defect and the condition of root surface.9 If this treatment option is to be considered, a full understanding of the diagnosis and classification of the defects, in conjunction with the predictability of treatment, is required. Furthermore, knowledge of a range of treatment options available is necessary as there is a multitude of surgical procedures that can be undertaken in certain clinical situations.9,11,20
Surgical options available can include coronal and lateral repositioned flaps, double papilla flaps and tunnelling flap procedures. All of these techniques can be utilized with the option of soft tissue grafting techniques, which can include autogenous connective or free gingival tissue grafts, allogenic or xenogenic grafts.11,13,20 With all these techniques, the tissue contour can be improved, giving the patient an amiable smile. Surgical root coverage procedures for minor defects offer the most predictable outcome, however, for more advanced recessive defects, where there has been loss of interdental bone with corresponding loss of papilla and keratinized tissue, the post-surgical aesthetic outcome with mucogingival surgery may be less predictable and provide only partial root coverage.4,14 In some cases, combined approaches may be necessary, with surgical procedures and direct or indirect restorative procedures.21
Removable prosthodontic treatment
Severe generalized recession as a result of periodontal disease can be managed with a relatively simple, conservative option, which involves replacing the lost periodontal tissue with a partial removable prosthesis (Figure 8). Gingival veneers are the preferred treatment if a large volume of soft tissue is in need of replacement and they can provide predictable cosmetic results.2,4,7,10
Figure 8. Same patient as in Figure 4 provided with a removable gingival veneer. A more pleasing aesthetic and functional result has been achieved, accepting the UR1 which is of guarded prognosis.
They may also offer a reasonable interim solution for patients and clinicians before considering more advanced and complex treatment.2,3,14
Case selection is vital and there are many factors to consider prior to providing the appliance.7,8 A thorough clinical assessment is required (Table 1), in addition to knowledge of the indications and contra-indications for providing such appliances (Table 2).
Assessment of
How
Why
Plaque control
Visual assessment of plaque levels, ideally with teeth disclosed.Appropriate plaque score demonstrated.
Only a patient with fully stabilised and treated periodontitis should be consid-ered for a gingival veneer. A patient needs to demonstrate that they can maintain their current dentition, knowing that any removable prosthesis can increase plaque formation.
Recession
Use a gradated periodontal probe to measure from the CEJ to the gingival margin.
It is necessary to have a baseline record of which teeth have recession and to what extent and severity.
Probing depth and attachment loss
Use a gradated periodontal probe to measure from the gingival margin to the base of any residual pocket.
Indicates the depth of the periodontal crevice/sulcus/pocket and, combined with the recession, this provides the attachment level/loss of attachment.
Bleeding on probing
Periodontal probing with a record of either bleeding or no bleeding recorded.
A bleeding score provides a record of gingival inflammation and it can also act as an indicator of periodontal disease, whereby the absence of bleeding is more indicative of periodontal health.22
Tooth mobility
Using two instruments, displace teeth in a bucco-lingual direction.
Severely mobile teeth may have a poor prognosis and may affect treatment planning. Providing a gingival prosthesis can sometimes help reduce mobility by bracing the teeth.
Indications
Contra-indications
Aesthetics
Mask exposed root surfaces
Reduce elongated crown height
Eliminate ‘black triangles’
Poor plaque control, gingival inflammation, mucogingival inflammation and irritation
Impaired speech due to air escape through wide embrasure spaces
Persistent periodontal disease or incomplete periodontal treatment
Root sensitivity
Allergy to prosthetic materials
Good oral hygiene
Increased caries risk
Can aid in application of topical medicaments to the gingiva
Poor manual dexterity
Foaming of saliva, spitting when talking
Failing restorations with micro-leakage
When there is a high risk involved in replacing crown/bridgework
Prominent labial frenum (however it is possible to correct surgically)
Loss of lip support
Risk of aspiration
Gingival veneers − clinical process
There are several types of gingival veneers reported in the literature.2,4,7,1415,16 These are categorized into removable or fixed, with further classification according to the materials. Flexible veneers are silicone-based, and rigid veneers can be made from pink acrylic or composite materials.
Flexible silicone veneers are more resistant to fracture in comparison to acrylic gingival veneers. However, silicone veneers may be more susceptible to staining from extrinsic causes.
The authors are not in favour of a fixed gingival veneer (eg fixed prostheses attached with gingival flange) as oral hygiene can be severely impeded and maintenance can be compromised.
Removable gingival veneers gain retention mechanically by utilizing undercuts inbetween teeth previously occupied by the interdental papillae, around extra-coronal restorations, or inbetween dental implants.7,14 Stability of the gingival veneer is also achieved by occupying the functional sulcus/vestibule. There is neuromuscular control from the pressure of the lips against the gingival veneer, and the natural capillary action formed by the saliva (cohesion) also partly contributes to retention of the veneer.14
The stages involved in the construction of a conventional removable gingival veneer are outlined in Table 3.
Clinical Stages
Technical Stages
Primary impression:
An initial impression is usually taken with a hydrocolloid material such as alginate in a standard stock tray.
The aim is to capture the functional sulcus with an appropriately extend-ed tray.
Disinfection of impression and send to laboratory.
Prescription for a sectional special tray:
Request tray with an anterior path of insertion, with incisal overlap.
Extending to at least distal aspect of canines or premolars.
Perforated or non-perforated design dependent on major impression material.
Major impression:
Try-in of special tray, with appropriate adjustments to allow for relief of frenal insertions, and modification to functional sulcus depth.
Appropriate extension and border moulding with self-supporting impression compound.
Blocking out of significant embrasures palatally with soft wax to prevent engagement of impression material interproximally.
Major impressions obtained of labial surfaces of teeth with elastomeric material.
Interproximal spaces and functional sulcus depth should be accurately recorded.
Disinfection of impression.
Gingival shade taking.
Completion of prosthodontic prescription.
Construction of gingival veneer:
Major impression cast in die stone.
Blocking out if any exceptionally large undercuts.
Model is trimmed wet and dried.
Extensions of veneer marked.
Model prepared with cold molt seal.
Polymethylmethacrylate acrylic is adapted to the model to the sulcus depth and extensions required.
The acrylic is pressure-cured.
The cured veneer is removed and trimmed.
Contouring, stippling and characterization is undertaken.
Staining is sealed with a surface sealant and light cured.
Steam clean and disinfection.
Delivery of appliance to clinic.
Fit of gingival veneer:
Pre-op visual assessment of veneer and cross check to prescription.
Removal of any obvious processing faults.
Try in of appliance:
There should be no blanching of the gingiva/soft tissues, or fitting surface discomfort. Provide appropriate adjustments once cause is identified.
Check retention with engagement of interdental spaces.
Check extensions of polished surfaces, distally and free border in functional sulcus.
Check relief in frenal regions during functional movements.
Check aesthetic outcome: shade and surface characteristics, new prosthetic gingival margin, lip support, appropriate reconstruction of lost tissue, visible acrylic during resting and active movements. Check phonetics.
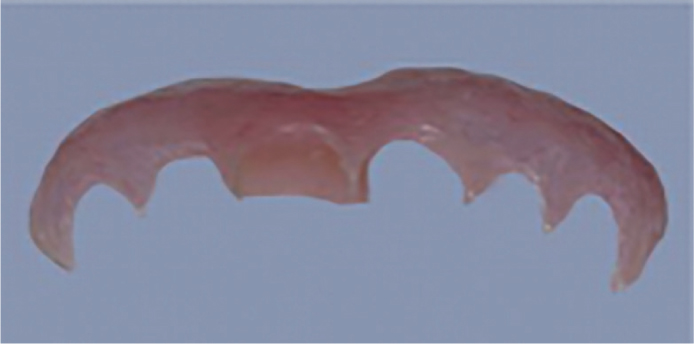
Gingival veneer prior to fitting.
Anterior view of veneer before fitting.
Anterior view of veneer after fitting.
Post-treatment advice:
Appropriate oral and dental hygiene, with correct use of interdental cleaning aids.
Appropriate prosthesis hygiene advice.
Oblique view of veneer after fitting.
Review appointment:
Review of gingival veneer, dentition and gingival health.
Advice following fitting appliance
Once provided, the prosthesis should be maintained as a conventional denture, however, extra care is required as it can be particularly fragile. It should always be removed at night before sleep and thoroughly cleaned.8 It can be washed with soap and water, gently brushed with a soft brush and also intermittently chemically cleansed with a non-abrasive denture cleanser (different cleaning solutions may be recommended for different material-based prostheses). If a brush is utilized, care is required so as not to damage the acrylic or silicone that intricately fits within the inter-proximal spaces. After cleaning, the appliance should be immersed in plain water to prevent dehydration and degradation of the materials. Dietary components and other extrinsic factors, such as smoking, can cause the appliance to stain and discolour. Silicone materials have been noted to be more prone to staining with coffee than acrylic.23 Advice regarding this should be given when fitting the gingival veneer.14,16
Review and maintenance
At initial review it is possible to assess how the patient has managed with the prosthesis. Comfort, speech, appearance, and personal wellbeing can be assessed, with the patient reporting the benefits of wearing the prosthesis. As well as reviewing the patient-related feedback, the dentition, gingival and periodontal health needs to be carefully re-assessed as per guidelines.19
It may be necessary to undertake adjustments to the fitting surfaces or inter-proximal areas if pain or trauma is reported. Adjustments may also be required to the extensions if impacting upon the functional sulcus depth. On some occasions, the addition of acrylic may be required in embrasure spaces or margins if they are not fully covered. If a flexible silicone prosthesis is provided, subtractive changes can be undertaken with a sharp blade or scissors.
Plaque accumulation with risk of dental caries or periodontal relapse is a cause for concern with the use of a gingival veneer, and therefore appropriate oral hygiene recommendations must be given and reviewed on a regular basis. If there are concerns that the prosthesis is going to affect the prognosis of the teeth, interventions need to be undertaken. It is not possible to withhold the appliance from a patient, however, advice can be given in a way so as to inform the patient of the significant risks and recommend that it may not be in his/her best interest to continue to use it. The authors recommend periodontal review and maintenance to be carried out as per BSP guidelines.19
Case series
Case 1
A 37-year-old patient was referred from his General Dental Practitioner (GDP) regarding gingival recession. The patient was wishing to explore whether surgery could be undertaken to cover his exposed roots. The patient was diagnosed with generalized aggressive periodontitis. The patient had been treated and was periodontally stable and in an appropriate periodontal maintenance programme. In addition to his aesthetic concerns, he also had complaints regarding sensitivity from the areas of root exposure. (Figure 9).
Figure 9.
Case 1: Severe generalized gingival recession with cervical abrasion.
Clinical examination revealed an excellent level of oral hygiene, with probing depths of less than 4 mm with minimal bleeding on probing. There was extensive generalized recession and attachment loss, with exposure of root surfaces. It would not be possible to achieve any predictable root coverage with mucogingival surgical procedures.
The patient was provided with a conventional hard removable gingival veneer in the upper anterior region from UR3−UL3 (Figure 10). He was delighted with the aesthetic outcome and also reported reduction in levels of sensitivity.
Figure 10.
Case 1: Gingival veneer made using acrylic on the master cast.
Case 2
A 73-year-old patient was referred for treatment in relation to severe localized chronic periodontitis. Extensive probing depths and suppuration with infrabony defects were associated with the bridge abutments (UR2, UL1) (Figures 11 and 12). Non-surgical and surgical treatment was undertaken to treat the disease, and occlusal adjustments made to the fixed-fixed bridgework replacing the UR1. Attachment loss due to periodontal disease was seen and, following treatment, there was extensive recession resulting in a poor aesthetic outcome (Figure 13). The patient also had significant food impaction in the region, with negative effects also on her speech.
Figure 11.
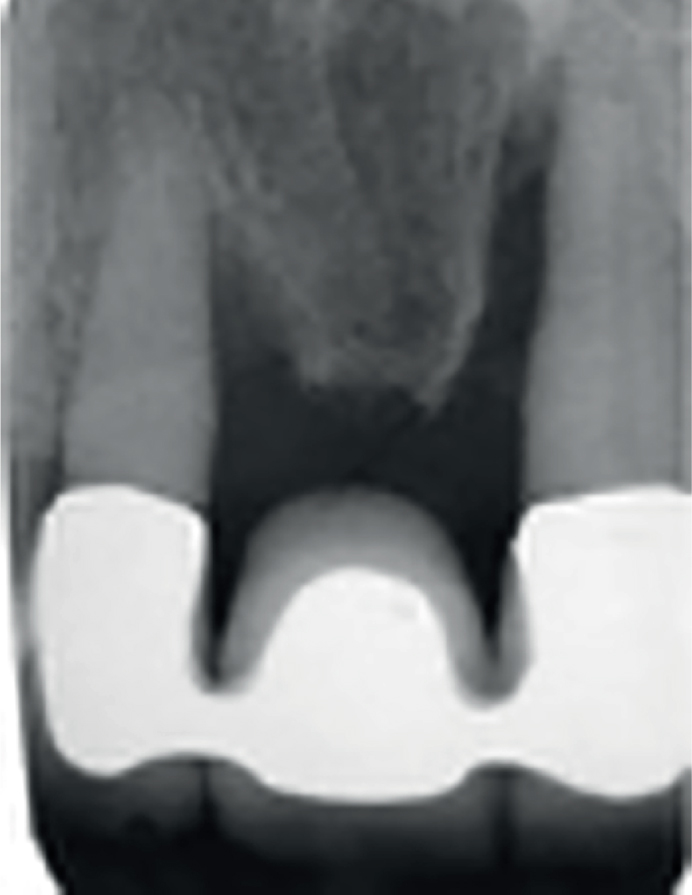
Case 2: Deep clinical probing depths associated with bridge abutments.Figure 12.
Case 2: Upper anterior radiograph of patient in Figure 11 showing infrabony defects associated with abutment teeth.Figure 13.
Case 2: The patient in Figures 11 and 12 shows severe attachment loss following non-surgical and surgical periodontal treatment.
A removable gingival veneer was prescribed, which extended from UR3 to UL3, with a permanent resilient lining/small silicone ‘bung’ in the extensive defect located under the pontic for the UR1 (Figure 14). An excellent aesthetic and functional outcome was achieved and the patient was delighted (Figure 15).
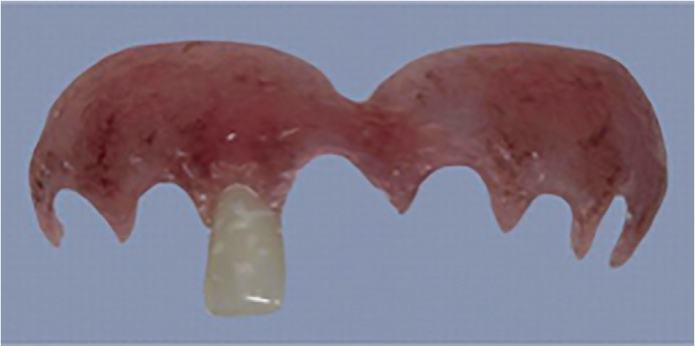
Figure 14.
Case 2: Gingival veneer made using acrylic with small resilient ‘bung’ to fit underneath bridge pontic.Figure 15.
Case 2: Same patient as in Figures 13 and 14 showing the gingival veneer in situ.
Case 3
A 40-year-old patient was referred for an opinion regarding his severe periodontitis. He was diagnosed with generalized aggressive periodontitis and received treatment involving non-surgical periodontal therapy with adjunctive oral systemic antibiotics. After stabilization of his condition he was left with severe recession, attachment loss, drifting and spacing in the upper anterior region (Figure 16). The post-periodontal treatment plan included occlusal equilibration to eliminate interferences and to allow for harmonious excursions, the lower anterior teeth (LR3− LL3) were splinted with composite and an orthodontic twist flexwire, and the upper central incisors were augmented and splinted with composite. A modified acrylic gingival veneer was then provided with an additional upper right lateral incisor incorporated to fill the diastema between the UR1 and UR2 (Figure 17). The patient was delighted with the outcome and continued to receive regular periodontal maintenance (Figure 18).
Figure 16.
Case 3: Severe attachment loss following non-surgical periodontal treatment.Figure 17.
Case 3: Acrylic gingival veneer with additional UR2 incorporated into the design.Figure 18.
Case 3: Post-treatment result of same patient as in Figure 16 which shows veneer in situ.
Gingival veneer survey
Background
Having highlighted the benefits in providing gingival veneers in secondary care/specialist practice, it was identified that there was little information and evidence as to the experiences for patients in general practice and a primary care setting. Equally, there is little understanding of the views of general dental practitioners as to whether this is a treatment modality that they would be happy to provide for their patients. With this in mind, a questionnaire was developed to explore the views of the local dentists in the north-east of England.
Methodology
One hundred and sixty five dental practices in the north-east of England were contacted by postal and electronic communication. Practices were asked to complete either a paper or an electronic copy of the gingival veneer questionnaire; this resulted in 76 (46%) responses in total. All entries were anonymous, however, the level of dental experience was specified in addition to the job title of the person completing the questionnaire. Some questions were deemed obligatory, requiring answers, and others questions were optional.
Specific areas that were being analysed for the purpose of this survey were knowledge of gingival veneers, general opinions of the prosthesis, production rates, costs of making the prosthesis (to patient and from the laboratory) and whether appliances were provided via the NHS or private treatment.
Results
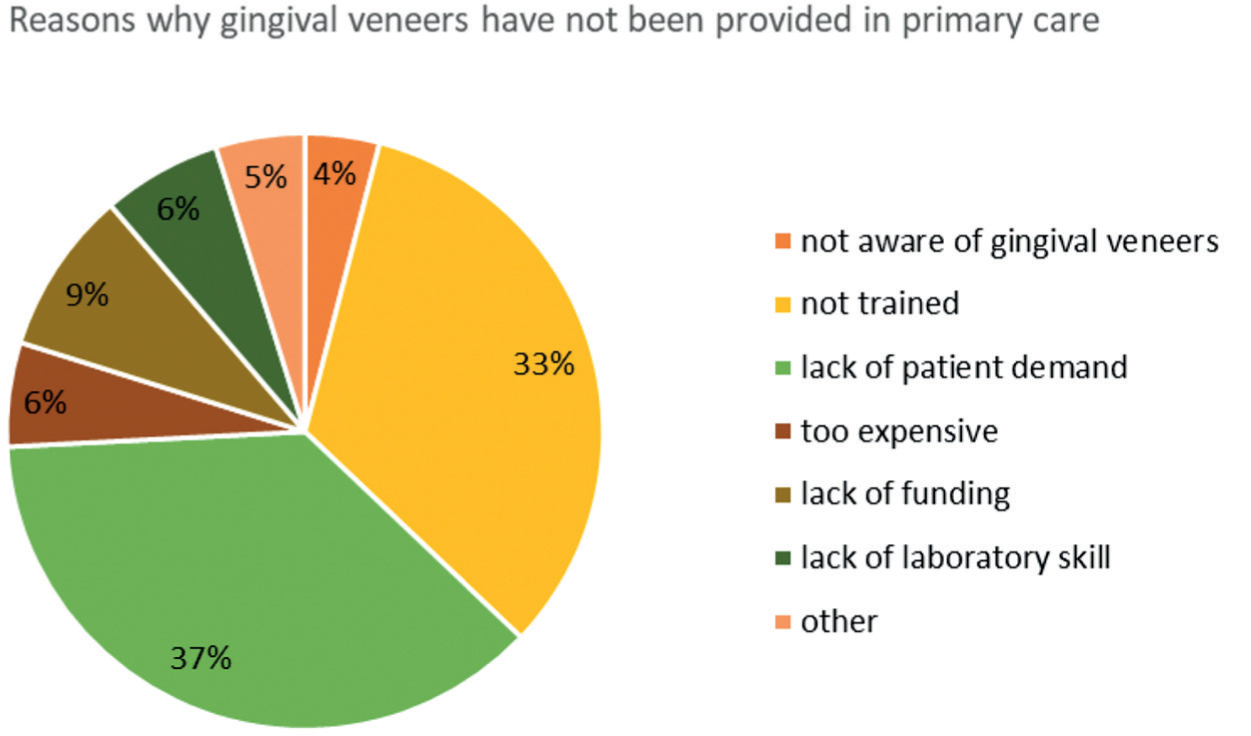
The results showed that most dentists in the region were aware of gingival veneers, with a minority of 4% not aware of these prostheses. Of the respondents, 13% had constructed and provided gingival veneers, and it was noted that prostheses were made less than once a year by all providing dentists. The reported main reason (37%) why gingival veneers were not provided by respondents who took part in our survey was due to lack of patient demand. Of dentists, 33% felt that they were not sufficiently trained to provide gingival veneers. Other reasons included lack of funding (9%), lack of laboratory skill (6%), and cost (6%) (Figure 19).
Figure 19. Pie chart showing reasons why dentists in primary care were not providing gingival veneers.
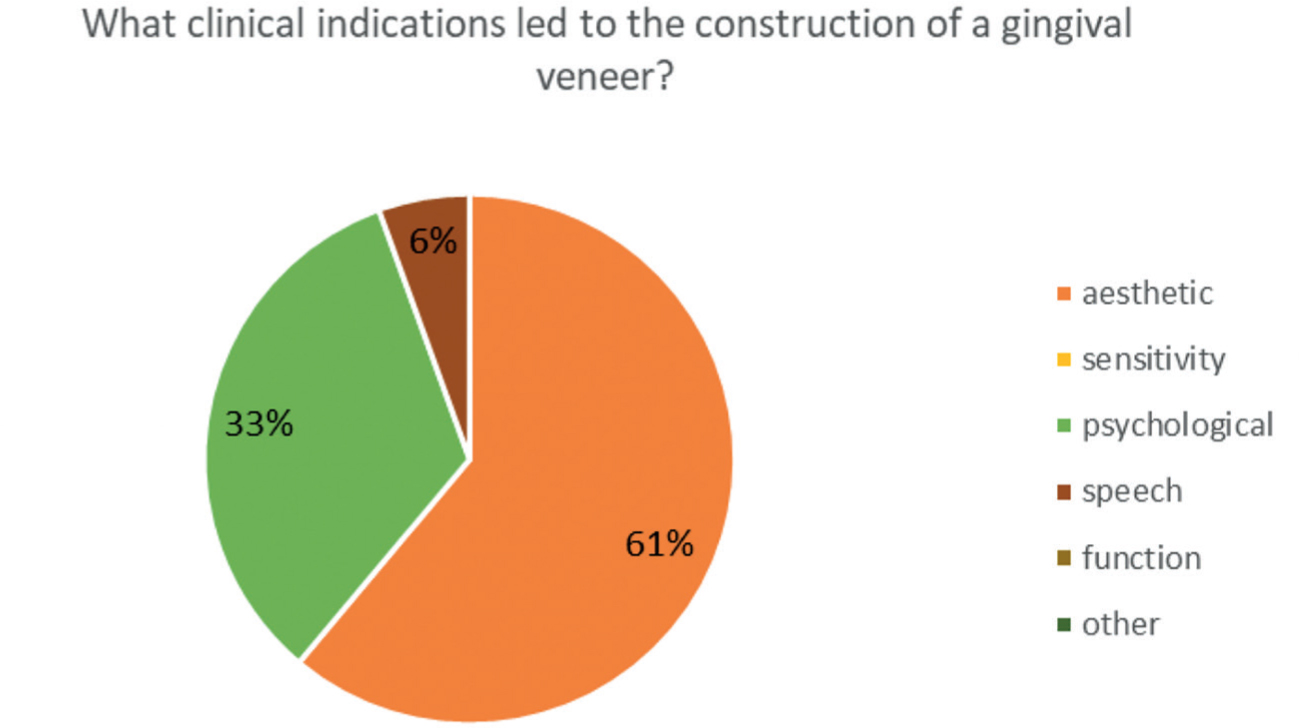
The most common indication for the provision of gingival veneers by dentists in primary care was to improve aesthetics. This was followed by psychological impact of gingival recession (Figure 20).
Figure 20. Pie chart showing clinical indications for providing gingival veneers.
Of the dentists who answered yes to providing gingival veneers in primary care, 17% were via a band 3 treatment of NHS payment scales (£222.50 at the time of questionnaire taking place), whereas private patient charges were between £150−£350. It was noted that the laboratory costs in making a gingival veneer varied greatly (range from £50−150). This variation in laboratory fee was reflected with the varying charges to the patient in providing the prosthesis in the private sector.
The results showed that three dentists (4%) had referred patients to Newcastle Dental Hospital for the provision of a gingival veneer and 67% stated that they would be interested in attending a training course on the provision of gingival veneers.
Discussion and conclusions
When auditing the provision of gingival veneers at Newcastle Dental Hospital an average of one veneer every month is provided. Positive patient feedback is received from patients, with improved functional and aesthetic outcomes. The construction and provision of such appliances is a relatively inexpensive treatment (costing £72 at NDH), with only three to four appointments required. Good case selection and careful impression techniques are a prerequisite for a successful outcome, in addition to detailed laboratory communication.
Considering the significant negative impact of recession, affecting a patient's quality of life,1,18 this treatment modality could be considered more frequently both in a secondary and primary care setting. The limiting factors for provision of treatment in the primary care environment seem to be in relation to training and economics. These factors should be easy to overcome with appropriate training and education for both clinicians and technicians. Our survey shows that the majority of primary care dentists (67%) who took part would be interested in a course about the provision of gingival veneers. The limiting factors for provision of gingival appliances in the secondary care setting is those of resource and manpower. Services are often limited as more referrals for complex treatments are being received and undertaken. Hospital cases tend to be treated on the basis of training need and education.
Questions may be raised in relation to gingival veneers such as, should patients be referred to a secondary care environment for the provision of a gingival veneer, or is it viable for them to be provided in primary care? With the current NHS dental contract placing importance on prevention, preservation and especially periodontal therapy, it may be felt that the provision of gingival veneers in primary care could be considered. This is particularly apparent as referral to secondary care may not be appropriate if restorative and periodontal services are under heavy demand. It also then poses the question, should gingival veneers be provided under the NHS or under the private contractual agreement? In many cases, the main indication is an aesthetic outcome, and on this basis, a private contract may be an acceptable approach; but equally, under a band 3 treatment, it may be deemed to be economically viable on an NHS contract.
In the current economic climate, with dentistry reorganizing its care pathways, there is much scope for gingival veneers to be considered to be provided in primary care as a simple and inexpensive treatment modality. This could achieve good aesthetic results, high patient satisfaction and improved quality of life for patients who meet the criteria for its indication. There is recognition that there would need to be appropriate training courses for general dental practitioners who would be keen to provide this treatment modality.