Hartzell TB. The operative and post-operative treatment of pyorrhea. Dent Cosmos. 1913; 55:1094-1101
Claffey N, Polyzois I., 5th edn. In: Lang NP, Lindhe J, Karring T (eds). Oxford: Blackwell Munksgaard; 2008
Nakib NM, Bissada NF, Simmelink JW, Goldstine SN. Endotoxin penetration into root cementum of periodontally healthy and diseased teeth. J Periodontol. 1982; 53:368-378
Ito K, Hindman RE, O'Leary TJ, Kafrawy AH. Determination of the presence of root-bound endotoxin using the local Shwartzman phenomenon (LSP). J Periodontol. 1985; 56:8-17
Heitz-Mayfield LJ. How effective is surgical therapy compared with non-surgical debridement?. Periodontology 2000. 2005; 37:72-87
Hujoel PP, Cunha-Cruz J, Loesche W, Robertson PB. Personal oral hygiene and chronic periodontitis: a systematic review. Periodontology 2000. 2005; 37:29-34
Sanz M, Teughels W. Innovations in non-surgical periodontal therapy: Consensus Report of the Sixth European Workshop on Periodontology. J Clin Periodontol. 2008; 35:3-7
Jepsen S, Deschner J, Braun A, Schwarz F, Eberhard J. Calculus removal and the prevention of its formation. Periodontology 2000. 2011; 55:167-188
Chapple ILC. Periodontal diagnosis and treatment – where does the future lie?. Periodontology 2000. 2009; 51:9-24
Guentsch A, Preshaw PM. The use of a linear oscillating device in periodontal treatment: a review. J Clin Periodontol. 2008; 35:514-524
Kocher T, Konig J, Hansen P, Ruhling A. Subgingival polishing compared to scaling with steel curettes: a clinical pilot study. J Clin Periodontol. 2001; 28:194-199
Eaton KA, Kieser JB, Davies RM. The removal of root surface deposits. J Clin Periodontol. 1985; 12:141-152
Caffesse RG, Sweeney PL, Smith BA. Scaling and root planing with and without periodontal flap surgery. J Clin Periodontol. 1986; 13:205-210
Buchanan SA, Robertson PB. Calculus removal by scaling/root planing with and without surgical access. J Periodontol. 1987; 58:159-163
Kepic TJ, O'Leary TJ, Kafrawy AH. Total calculus removal: an attainable objective?. J Periodontol. 1990; 61:16-20
Robertson PB. The residual calculus paradox. J Periodontol. 1990; 61:65-66
Stillman PR. The management of pyorrhea. Dent Cosmos. 1917; 59:405-414
Aleo JJ, De Renzis FA, Farber PA, Varboncoeur AP. The presence and biologic activity of cementum-bound endotoxin. J Periodontol. 1974; 45:672-675
Aleo JJ, De Renzis FA, Farber PA. In vitro attachment of human gingival fibroblasts to root surfaces. J Periodontol. 1975; 46:639-645
Jones WA, O'Leary TJ. The effectiveness of in vivo root planing in removing bacterial endotoxin from the roots of periodontally involved teeth. J Periodontol. 1978; 49
Nishimine D, O'Leary TJ. Hand instrumentation versus ultrasonics in the removal of endotoxins from root surfaces. J Periodontol. 1979; 50:345-349
Fine DH, Morris ML, Tabak L, Cole JD. Preliminary characterization of material eluded from the roots of periodontally involved teeth. J Periodontal Res. 1980; 15:10-19
Hughes FJ, Smales FC. Immunohistochemical investigation of the presence and distribution of cementum-associated lipopolysaccharides in periodontal disease. J Periodontal Res. 1986; 21:660-667
Moore J, Wilson M, Kieser JB. The distribution of bacterial lipopolysaccharide (endotoxin) in relation to periodontally involved root surfaces. J Clin Periodontol. 1986; 13:748-751
Nyman S, Westfelt E, Sarhed G, Karring T. Role of “diseased” root cementum in healing following treatment of periodontal disease. J Clin Periodontol. 1986; 13:464-468
Hughes FJ, Smales FC. The distribution and quantitation of cementum-bound lipopolysaccharide on periodontally diseased root surfaces of human teeth. Arch Oral Biol. 1990; 35:295-299
Cheetham WA, Wilson M, Kieser JB. Root surface debridement – an in vitro assessment. J Clin Periodontol. 1988; 15:288-292
Smart GJ, Wilson M, Kieser JB. The assessment of ultrasonic root surface debridement by determination of residual endotoxin levels. J Clin Periodontol. 1990; 17:174-178
Cobb CM. Clinical significance of non-surgical periodontal therapy: an evidence-based perspective of scaling and root planing. J Clin Periodontol. 2002; 29:22-32
Tunkel J, Heinecke A, Flemmig TF. A systematic review of efficacy of machine-driven and manual subgingival debridement in the treatment of chronic periodontitis. J Clin Periodontol. 2002; 13:72-81
Ioannu I, Dimitriadis N, Papadimitriou K, Sakellari D, Vouros I, Konstantinidis A. Hand instrumentation versus ultrasonic debridement in the treatment of chronic periodontitis: a randomized clinical and microbiological trial. J Clin Periodontol. 2009; 36:132-141
Bollen CML, Mongardini C, Papaioannou W, van Steenberghe D, Quirynen M. The effect of a one-stage full-mouth disinfection on different intra-oral niches. Clinical and microbiological observations. J Clin Periodontol. 1998; 25:56-66
Mongardini C, van Steenberghe D, Dekeyser C, Quirynen M. One stage full-versus partial-mouth disinfection in the treatment of chronic adult or generalized early-onset periodontitis. 1. Long-term clinical observations. J Periodontol. 1999; 70:632-645
Quirynen M, Mongardini C, Pauwels M, Bollen CML, Van Eldere J, van Steenberghe D. One stage full-versus partial-mouth disinfection in the treatment of chronic adult or generalized early-onset periodontitis. 2. Long-term impact on microbial load. J Periodontol. 1999; 70:646-656
Koshy G, Kawashima Y, Kiji M, Nitta H, Umeda M, Nagasawa T, Ishikawa I. Effects of single-visit full-mouth ultrasonic debridement versus quadrant-wise ultrasonic debridement. J Clin Periodontol. 2005; 32:734-743
Eberhard J, Jervøe-Storm P-M, Needleman I, Worthington H, Jepsen S. Full-mouth treatment concepts for chronic periodontitis: a systematic review. J Clin Periodontol. 2008; 35:591-604
Wennström JL, Tomasi C, Bertelle A, Dellasega E. Full-mouth ultrasonic debridement versus quadrant scaling and root planing as an initial approach in the treatment of chronic periodontitis. J Clin Periodontol. 2005; 32:851-859
Zanatta GM, Bittencourt S, Nociti FH, Sallum EA, Sallum AW, Casati MZ. Periodontal debridement with povidone-iodine in periodontal treatment: short-term clinical and biochemical observations. J Periodontol. 2006; 77:498-505
Del Peloso Ribeiro É, Bittencourt S, Sallum EA, Nociti FH, Goncalves RB, Casati MZ. Periodontal debridement as a therapeutic approach for severe chronic periodontitis: a clinical, microbiological and immunological study. J Clin Periodontol. 2008; 35:789-798
Eley BM, Soory M, Manson JD., 6th edn. London: Churchill Livingstone: Elsevier; 2010
van der Weijden F, Slot DE. Oral hygiene in the prevention of periodontal diseases: the evidence. Periodontology 2000. 2011; 55:104-123
Schwarz F, Aoki A, Sculean A, Becker J. The impact of laser application on periodontal and peri-implant wound healing. Periodontology 2000. 2009; 51:79-108
Soukos NS, Goodson M. Photodynamic therapy in the control of oral biofilms. Periodontology 2000. 2011; 55:143-166
Petersilka GJ. Subgingival air-polishing in the treatment of periodontal biofilm infections. Periodontology 2000. 2011; 55:124-142
Periodontitis is a complex disease that has both oral and systemic consequences. The treatment of periodontitis may be both surgical and non-surgical but, in recent years, there has been a shift towards managing disease non-surgically in preference to surgery. Fundamental to all types of therapy is the patient's role in disease control, in the form of self-performed plaque control, and it is important that the patient understands this. Non-surgical periodontal therapy has a long history and has traditionally been carried out using a variety of hand and powered instruments, the objective being root surface disinfection by the removal of plaque, calculus and contaminated root cementum. However, over the last 30 years or so, it has become apparent that calculus does not cause disease, cementum does not become significantly infected and bacteria and their toxins are only loosely adherent to the diseased root surface. This has led to the development of less invasive instrumentation principles which may be better for patients, more cost-effective and more easily applied in different clinical settings.
Clinical Relevance: This paper aims to describe and justify a minimally-invasive approach to the management of the diseased root surface in periodontitis, to clarify the terminology used and to suggest how these principles may be applied in general practice.
Article
A paper (Wedges and Ledges?), in the first issue of Dental Update, discussed the role of food packing in periodontal disease. In the 40 years since then our understanding of the aetiology of periodontitis has increased enormously, and periodontitis is now recognized as one of the most complex of human diseases. In addition, there is also mounting evidence that periodontitis may play a significant role in general health, so that the effective treatment of periodontitis may be even more important than was once thought. Treatment of periodontitis may be non-surgical or surgical but, since the first issue of Dental Update, there has been a shift away from surgical treatment towards non-surgical management of disease. It is the aim of this paper to explore changing trends in non-surgical therapy and to make a case for the use of conservative, non-tooth destructive treatment techniques.
Many of the methods commonly used today to treat periodontal diseases have remained largely unchanged for decades. For example, in non-surgical periodontal therapy the process of root planing is still widely practised but it was described, and named, in the dental literature a century ago.1 Root planing involves the deliberate removal of tooth structure during periodontal instrumentation2 to render the root surface ‘hard’ and ‘smooth’ and is an invasive procedure since it involves the removal of tooth structure. Studies from the early 1980s, however, suggested that the intentional removal of cementum during root planing was not justified,3,4 and so the concept of less invasive non-surgical management of the diseased root surface was developed. The use of minimally-invasive techniques in restorative dentistry is now recognized as of increasing importance, and is often in the better interests of patients.
The case for non-surgical disease management
That non-surgical treatment is an effective method for treating chronic periodontitis (or indeed the less common aggressive form of disease) is not in doubt; a systematic review and meta-analysis published in 20055 reviewed the findings of three previous systematic reviews, published between 1993 and 2002, confirming that better treatment outcomes can be achieved by non-surgical means, when compared to surgical treatment, for moderate pockets (up to 6mm), while surgical treatment is only of greater benefit for deeper pockets in excess of 6mm. Although this appeared to show that deep pockets should be treated surgically, the authors pointed out that this latter finding is only applicable to 12-month post-treatment results and those studies that followed patients for 5 years or more found that, even for deep pockets, non-surgical therapy was as effective as surgical treatment.
However, fundamental to the successful management of disease by non-surgical means (or indeed surgical means for that matter) is the establishment, before any treatment is carried out, of optimal self-performed biofilm control.
The patient's role in disease control
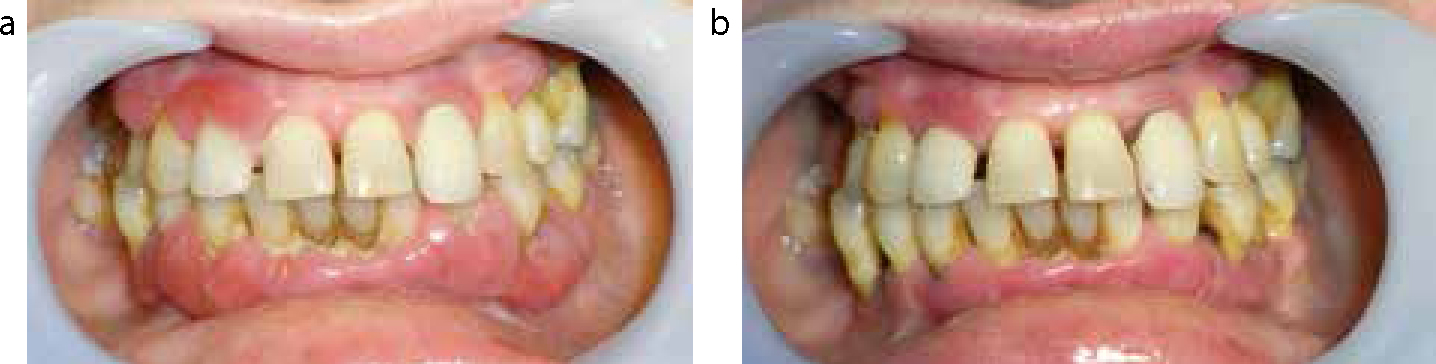
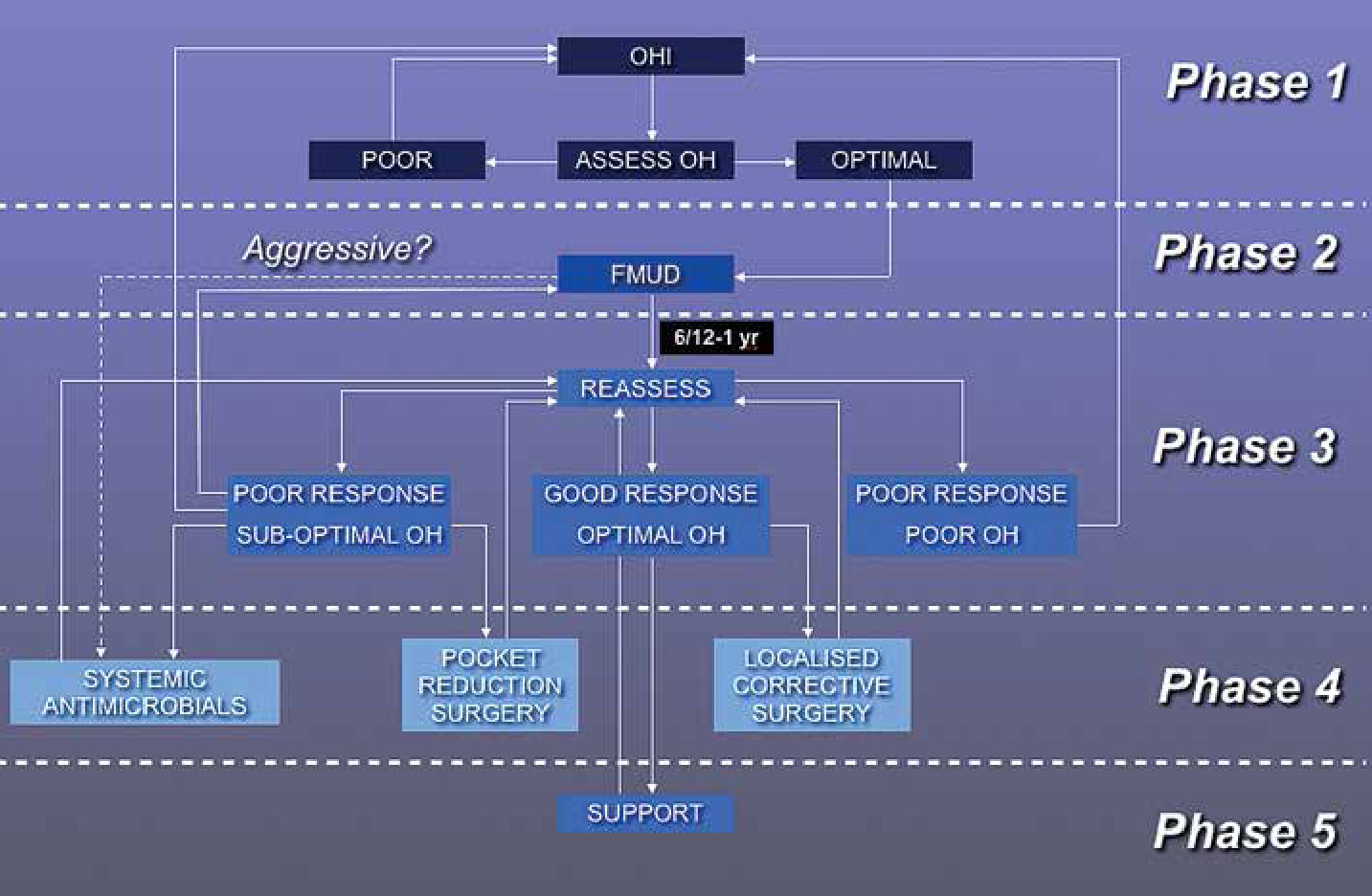
Although the evidence base for an association between personal oral hygiene and the control or prevention of chronic periodontitis is surprisingly weak (there are no randomized controlled trials to show such an association for instance),6 it is assumed that an adequate level of daily plaque control is a pre-requisite for successful periodontal therapy of any form. For example, the Sixth European Workshop in Periodontology in 20087 stated that: “It should be noted that the performance of optimal oral hygiene practices is an inseparable principle to be observed with any protocol of mechanical debridement”. The effects of good biofilm control before starting treatment can be dramatic (Figure 1), the goal being to establish an optimal supragingival environment prior to starting subgingival instrumentation. The reduction in marginal inflammation that results from a high standard of biofilm control has a number of benefits for both patients and clinicians: in the absence of inflammation, treatment can be more comfortable for patients and for operators it can be easier to carry out. Most importantly, however, during this oral hygiene phase (Figure 2), it is preferable not to carry out any form of instrumentation – the patients then learn that, through their own efforts, they can have a profound effect on the condition of their gums and thus ‘self efficacy’ is enhanced. The presence of supragingival calculus is not necessarily a barrier to the establishment of optimal plaque control, which suggests that calculus does not in itself cause inflammation.8
Figure 1.
(a, b) Three months of plaque control alone prior to any mechanical instrumentation. Note that the presence of both supragingival and subgingival calculus has not prevented resolution of the inflammatory lesions.Figure 2. A structured phased approach to periodontal treatment planning.
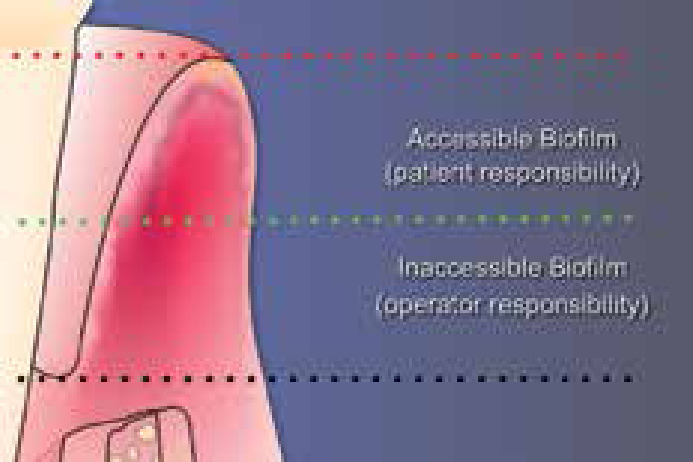
Patients' efforts are not restricted to the supragingival region and, as well as marginal and interdental plague control methods, patients should be shown how to clean subgingivally (Figure 3). In this way, patients can disrupt the accessible biofilm below the gingival margin, which leaves disruption of the less accessible biofilm one of the objectives of treatment (Figure 4). Traditionally, the other principle therapeutic objectives have included the removal of all subgingival calculus and any contaminated root cementum.
Figure 3. Subgingival plaque control with a single-tufted brush.Figure 4. Biofilm accessibility diagram.
Therapeutic objectives – changing approaches
While it is widely accepted that mechanical biofilm removal is the cornerstone of successful periodontal therapy,9,10 much emphasis in the past has been placed on the removal of all subgingival calculus deposits, and also on the removal of contaminated cementum by root planing with sharp hand instruments, a technique that was described in the dental literature in 19131 and which was illustrated in Egyptian hieroglyphics 4000 years ago.
The association of subgingival calculus with periodontal lesions has led to the assumption in the past that there is a cause and effect relationship between these two phenomena; a review of the evidence,8 however, has shown that calculus is the result of disease and not its cause and that periodontal healing occurs in the presence of calculus as long as the overlying bacterial biofilm is removed. Calculus is thus an inert material and its formation could perhaps be regarded as a protective mechanism, since it represents the calcification of potentially pathogenic biofilm. Therefore, clinically, it can be observed that, in the presence of optimal biofilm control by the patient, but in the absence of subgingival calculus removal (for example during the oral hygiene phase of treatment), healing of the periodontal lesion can take place and gingival shrinkage exposes previously subgingival calculus (Figure 5). The removal of calculus then becomes necessary for better access to the subgingival biofilm and for aesthetics. In the past, too much emphasis has been placed on complete calculus removal for disease control, both in training and practice, but such emphasis is misplaced and the focus should instead be on biofilm disruption by both patients and operators. In other words, plaque removal is more important than calculus removal.11 In reality, it is as well that complete calculus removal is less important than was previously thought because many studies have shown that complete calculus removal is rarely, if ever, achieved.12,13,14,15 One review16 showed that, even after 12–15 minutes of treatment per tooth, 63% of root surfaces still harboured residual calculus.
Figure 5.
(a–c) Optimal plaque control has resulted in gingival shrinkage and exposure of previously subgingival calculus.
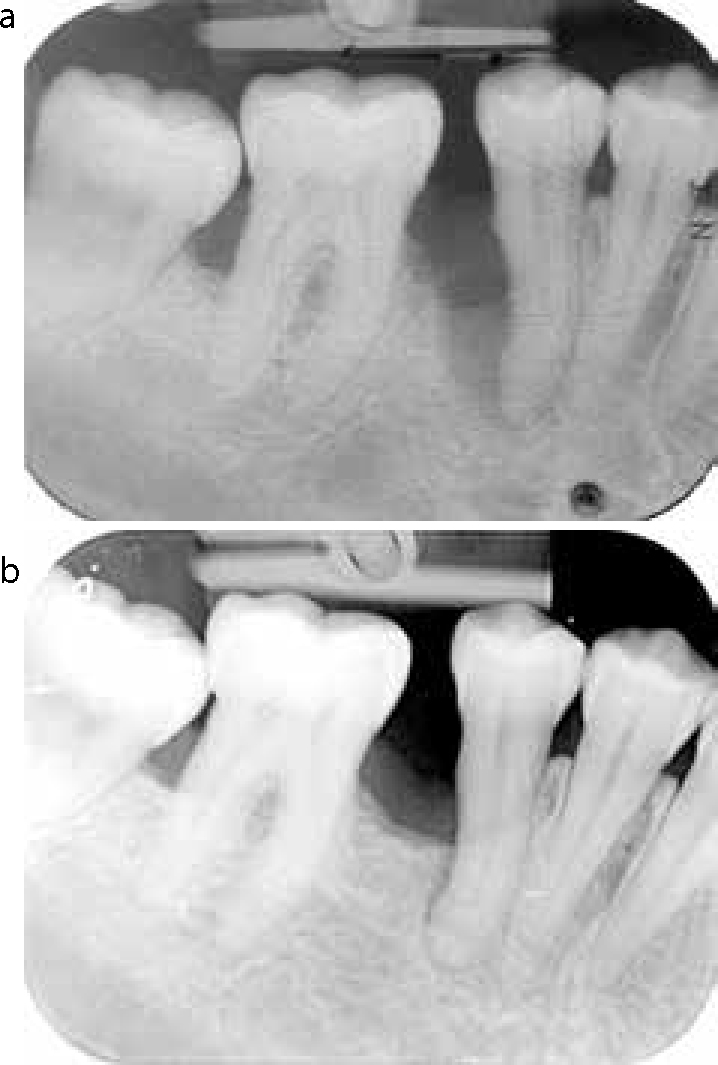
What then of the role of contaminated cementum in periodontal disease? Stillman, in 1917,17 described the need for planing of the root (or ‘skinning’ as it was sometimes called then) with instruments with “keen cutting edges… leaving this surface as clean as a billiard ball, and equally as well polished”, the goal being to remove the cementum layer which had been shown to be closely associated with bacteria and their toxins,18,19,20,21 or even, it was suggested, ‘deeply penetrated’ by bacterial endotoxin.22 This concept persisted for much of the 20th Century and the process of scaling and root planing (SRP), quadrant by quadrant under local anaesthetic, became the norm in non-surgical disease management, requiring considerable time and technical skill, the use of highly sharpened (and therefore damaging) hand instruments and significant post-operative discomfort for the patient. But, in the early 1980s, doubts started to be raised about the location of bacterial toxins on the root surface and the need for such invasive treatment, which could result in significant iatrogenic tooth surface loss (Figure 6). A number of studies at this time suggested that bacterial toxins were only loosely adherent to the root surface and could be removed by much lighter instrumentation which did not damage the root surface to the same extent.3,4,23,24,25,26 One in vitro study24 showed that over 99% of the bacterial contaminants could be removed by light instrumentation alone, without the need for cementum removal by root planing. This led to the concept of root surface debridement (RSD)27,28 as an alternative to root planing, the goal being the achievement of a biocompatible root surface without the removal of tooth structure. Thus it was shown that RSD had the potential to achieve the same level of root surface decontamination as root planing but with the advantages of conservation of tooth structure, shorter treatment time and greater patient comfort. In addition, the concept of RSD allowed for the exclusive use of ultrasonic instrumentation, since there was no need to remove cementum by hand planing. Furthermore, ultrasonic use has been shown to be as effective as hand instrumentation in terms of clinical and microbiological treatment outcomes29,30,31 and is much less technically demanding. The use of local anaesthesia is often unnecessary with such light instrumentation, thus reducing the potential for iatrogenic damage and this, combined with the shorter treatment time, also permits a full-mouth treatment approach, as opposed to quadrant by quadrant treatment, which has been shown to yield better treatment outcomes.32,33,34,35,36 The term ‘full-mouth ultrasonic debridement’ (FMUD) has been used to describe this type of non-surgical therapy35 in which full-mouth treatment is carried out using ultrasonic instrumentation exclusively and with a debridement technique rather than a planing approach. Over time, and with consistent patient adherence, stable results can be readily achieved (Figure 7), often with spontaneous healing of vertical bone defects (Figure 8). Several studies have directly compared the minimally invasive FMUD approach, comprising a single visit of less than one hour, with the traditional SRP approach of 3–4 hours of root planing, by quadrant with local anaesthesia, over four visits.37,38,39 In each case, the treatment outcomes were identical, leading one author39 to state that: “periodontal debridement…may be assumed as a viable approach to deal with severe chronic periodontitis”. This has led the Sixth European Workshop (2008) to recognize that there is a need to investigate the impact of different mechanical debridement protocols on patient-centred outcomes and cost-effectiveness.7
Figure 6. An extensively root planed tooth showing iatrogenic tooth surface lossFigure 7.
(a, b) This patient presented with extensive periodontitis and drifting of the UL1 due to inflammatory oedema of the palatal tissues. (c, d) The patient 4 years later after non-surgical therapy (FMUD) and supportive care. Note the spontaneous repositioning of UL1 as the inflammatory oedema has subsided. No orthodontics was carried out.Figure 8.
(a, b) Bone infill at LR5 following 2 years of non-surgical treatment (FMUD) and supportive care.
Clarity or confusion?
The difference between root planing (RP) and RSD would seem to be clear; RP has been defined as: “…a technique of instrumentation by which the ‘softened cementum’ is removed and the root surface is made ‘hard’ and ‘smooth’…” and RSD as “… removal of plaque and/or calculus from the root surface without the intentional removal of tooth structure”.2 The difference has recently been further clarified by the inclusion of the term ‘Periodontal Debridement’ in the National Library of Medicine's Medical Subject Headings (MeSH) database where it is defined as: “Removal or disruption of dental deposits…without deliberate removal of cementum as done in root planing and often in dental scaling”. Despite this apparent clarity in terminology and treatment objective, the term RSD is often used synonymously, and erroneously, with RP40,41 and hand instruments (planing instruments) are often used, and taught to be used, as debridement instruments. This is analogous to using a highly sharpened sharp wood plane to clean a wood surface without removing any of the wood itself. Partly this confusion arises from a resistance, in some quarters, to the idea of achieving periodontal health by minimally-invasive approaches. There may be a number of reasons for this; traditional SRP is effective so there is a reluctance to change position, which is always unsettling. In addition, SRP has been in use for so long that educational programmes (especially in hygienist training) and practices have evolved on the back of these concepts and industry has responded by manufacturing and selling the tools needed to treat patients in these ways.
Future developments
There is a growing evidence base that it is disruption of the biofilm, both by patient and clinician, rather than calculus or cementum removal, that is the key to controlling periodontal diseases.9,42 The patient's role in this process is clearly crucial. Professional interventions that concentrate on biofilm disruption, with minimal effects on tooth structure, are being investigated in the form of laser instrumentation,43 the use of photodynamic disinfection44 and air polishing devices,45 and hold out the prospect of achieving periodontal stabilization with minimal harm to the patient and more cost-effectively than traditional methods.