Chicago, IL, USA: American Academy of Periodontology; 1989
Wiebe CB, Putnins EE The periodontal disease classification system of the American Academy of Periodontology – an update. J Can Dent Assoc. 2000; 66:594-547
1999 International International Workshop for a Classification of Periodontal Diseases and Conditions. Papers. Oak Brook, Illinois, October 30–November 2, 1999. Ann Periodontol. 1999; 4:(i)1-112 https://doi.org/10.1902/annals.1999.4.1.i
Caton JG, Armitage G, Berglundh T A new classification scheme for periodontal and peri-implant diseases and conditions – Introduction and key changes from the 1999 classification. J Clin Periodontol. 2018; 45:(Suppl 20)S1-S8 https://doi.org/10.1111/jcpe.12935
Dietrich T, Ower P, Tank M Periodontal diagnosis in the context of the 2017 classification system of periodontal diseases and conditions - implementation in clinical practice. Br Dent J. 2019; 226:16-22 https://doi.org/10.1038/sj.bdj.2019.3
Moore J, Wilson M, Kieser JB The distribution of bacterial lipopolysaccharide (endotoxin) in relation to periodontally involved root surfaces. J Clin Periodontol. 1986; 13:748-751 https://doi.org/10.1111/j.1600-051x.1986.tb00877.x
Nyman S, Westfelt E, Sarhed G, Karring T Role of “diseased” root cementum in healing following treatment of periodontal disease. A clinical study. J Clin Periodontol. 1988; 15:464-468 https://doi.org/10.1111/j.1600-051x.1988.tb01601.x
Smart GJ, Wilson M, Davies EH, Kieser JB The assessment of ultrasonic root surface debridement by determination of residual endotoxin levels. J Clin Periodontol. 1990; 17:174-178 https://doi.org/10.1111/j.1600051x.1990.tb01082.x
Tunkel J, Heinecke A, Flemmig TF A systematic review of efficacy of machine-driven and manual subgingival debridement in the treatment of chronic periodontitis. J Clin Periodontol. 2002; 29:(Suppl 3)72-81 https://doi.org/10.1034/j.1600-051x.29.s3.4.x
George MD, Donoly TG, Preshaw PM: Wiley-Blackwell; 2014
Golub LM, Lee HM, Greenwald RA A matrix metalloproteinase inhibitor reduces bone-type collagen degradation fragments and specific collagenases in gingival crevicular fluid during adult periodontitis. Inflamm Res. 1997; 46:310-319 https://doi.org/10.1007/s000110050193
Preshaw PM, Novak MJ, Mellonig J Modified-release subantimicrobial dose doxycycline enhances scaling and root planing in subjects with periodontal disease. J Periodontol. 2008; 79:440-452 https://doi.org/10.1902/jop.2008.070375
It is all too easy to think that nothing has changed in periodontology in the past 50 years. Self-performed plaque control, avoidance of the known risk factors and professional removal of deposits above and below the gum line have been the mainstay of periodontal management for decades. However, our understanding of what we actually need to do to the root surface to facilitate periodontal healing has changed dramatically in the past 50 years and advances in surgical technique and regenerative materials have made treatment more conservative, allowing us to predictably treat periodontitis.
CPD/Clinical Relevance: The changes in periodontal management during the 50 years that Dental Update has been in circulation are highlighted.
Article
As we celebrate 50 years of Dental Update, I will look at where we were in periodontology 50 years ago and where we are now, looking at treatment modalities that have come into, and gone out of, ‘fashion’.
I looked at the first edition of Dental Update to see whether there were any interesting articles that I could reference relating to periodontal disease management from that time. While I could not find a periospecific article, there was one called ‘Ledges and wedges?’ that discussed the role of food impaction and its role in periodontal disease. That alone shows we have come a long way in the past 50 years.
It is safe to say that the mainstay of periodontal management remains largely focused on the patient’s home care, together with the avoidance of the known risk factors, and professional non-surgical treatment.
During the past 50 years trends towards more or less aggressive treatments have been proposed, but with an improved evidence base.
Classification changes
The past 50 years has seen a number of significant changes in how we describe and diagnose periodontal disease. Having experienced two classification changes in my dental career, I understand and accept that some of the changes can often seem small, almost petty. However, when a classification system no longer fits with advances in understanding of disease aetiology and pathogenesis, we are obliged to change the way we classify and diagnose them.
The first comprehensive classification system was put together by the American Academy of Periodontology in 1989.1 Prior to this we were working with the overly simplistic two-category system made up of juvenile periodontitis and chronic marginal periodontitis.2 The 1989 classification (Table 1), was a significant improvement over previous systems, and described a much wider range of periodontal conditions. This reflected what was being seen at the time, and also introduced the concept of periodontal disease being affected by systemic medical conditions.
Table 1. 1989 AAP periodontal classification.
I
Early-onset periodontitis
A. Prepubertal periodontitis
1. Localized
2. Generalized
B. Juvenile periodontitis
1. Localized
2. Generalized
C. Rapidly progressive periodontitis
II
Adult periodontitis
III
Necrotizing ulcerative periodontitis
IV
Refractory
V
Periodontitis associated with systemic disease
This system, while a significant improvement on what had gone before, still had many shortcomings. One such example was related to age boundaries for certain types of disease. Knowing when a disease started is often impossible and terms, such as ‘juvenile’ or ‘pre-pubertal’ in a diagnostic system, became challenging. Clearly, this was unworkable, and the 1999 International Workshop for a Classification of Periodontal Disease and Conditions was convened to review it, with the workshop summary written up by Gary Armitage (Table 2).3
Table 2. 1989 AAP periodontal classification.
I
Gingival diseases
II
Chronic periodontitis
III
Aggressive periodontitis
IV
Periodontitis as a manifestation of systemic disease
V
Necrotizing periodontitis
VI
Periodontal abscess
VII
Perio-endo
VIII
Developmental/acquired conditions
One of the most notable changes from the 1989 classification to the 1999 classification was the removal of the concept of ‘refractory periodontitis’, essentially thought of as ‘disease that does not respond to treatment’. This was an important step, and acknowledges that we do not believe that there is ‘untreatable’ disease.
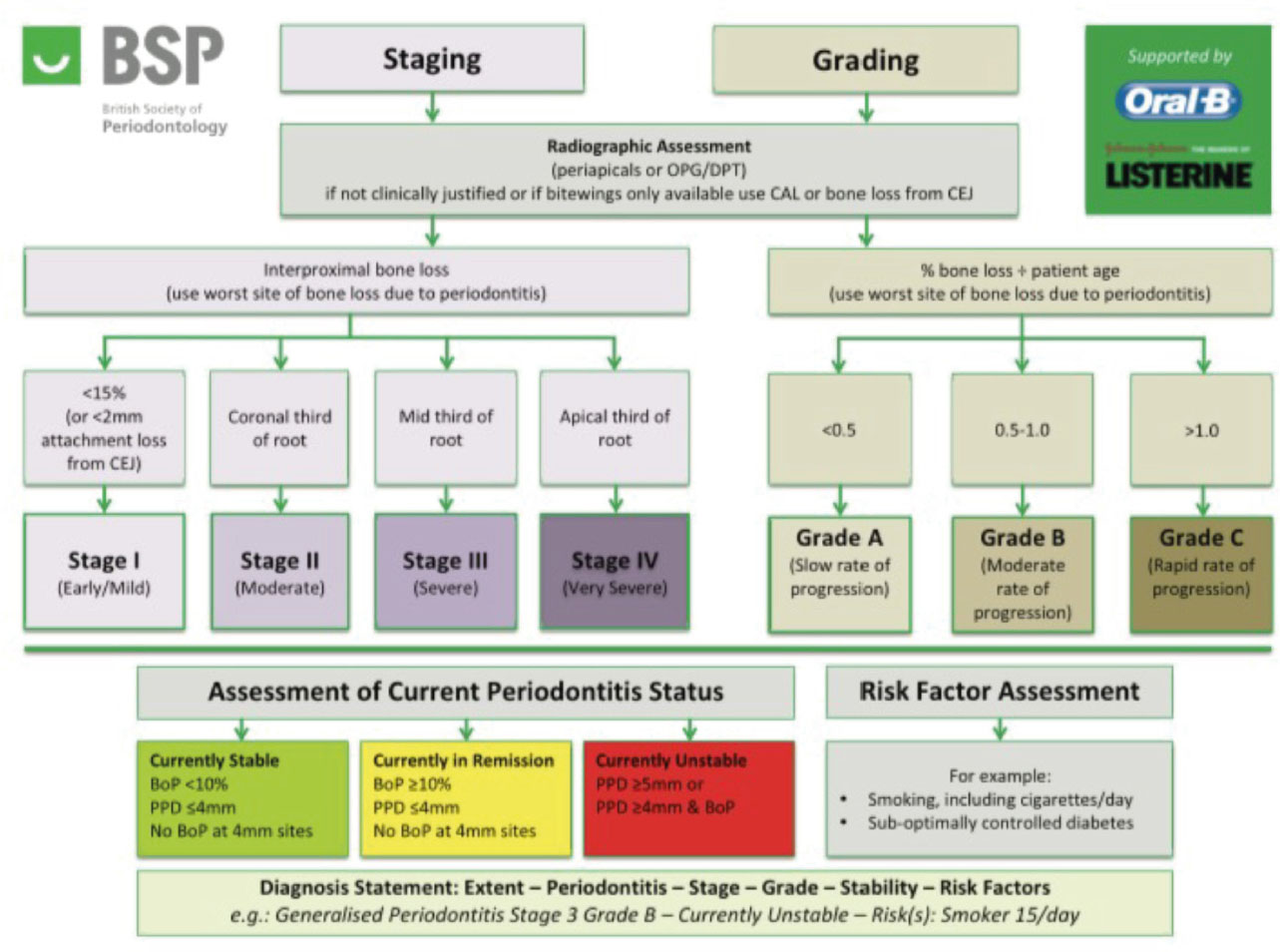
A much more comprehensive and logical system, it lasted for nearly 20 years before being replaced by the current system that was developed at the World Workshop in Periodontics 2017 and published in 2018.4 A simplified version was later released for use in UK practice by the British Society of Periodontology and Implant Dentistry in 2019 (Figure 1).5
Figure 1. The 2018 BSP implementation of the new classification.
This new classification, while using new staging and grading terminology, had lots of parallels with the 1999 system. One of the seismic shifts was the removal of the concept of ‘aggressive periodontitis’ through evidence indicating that both chronic and aggressive periodontitis are just two extremes of the same disease.
Treatment changes and trends
Instrumentation
While for many, periodontal treatment may not appear to have evolved significantly, the present author would beg to differ. From the 1970s through to the turn of the century, aggressive management of the root surface was still the non-surgical treatment modality of choice, with the removal of the biofilm, calculus and the ‘infected’ cementum, known as root planing. The justification for the removal of cementum was based on the theory that the bacterial endotoxin was embedded in, or bound to, this layer and if this was not removed it would impair disease resolution.
It was during the 1980s that people, such as Bernie Keiser, Jim Moore and Sture Nyman, started to question this rationale and carried out studies to examine the hypothesis.
Moore and Keiser6 showed that the bacterial endotoxin was superficially located and very easily removed. Using extracted periodontally compromised teeth, they were able to show that rinsing of the root surface removed 39.52% of the endotoxin and polishing removed a further 59.73% leaving minuscule amounts of endotoxin to be removed by the aggressive root planing concept.
Similar research around the same time from the Gothenburg group7 supported these findings, and this era should have been the beginning of the minimally invasive periodontal movement. Sadly, it took many years for the global periodontal community to accept this.
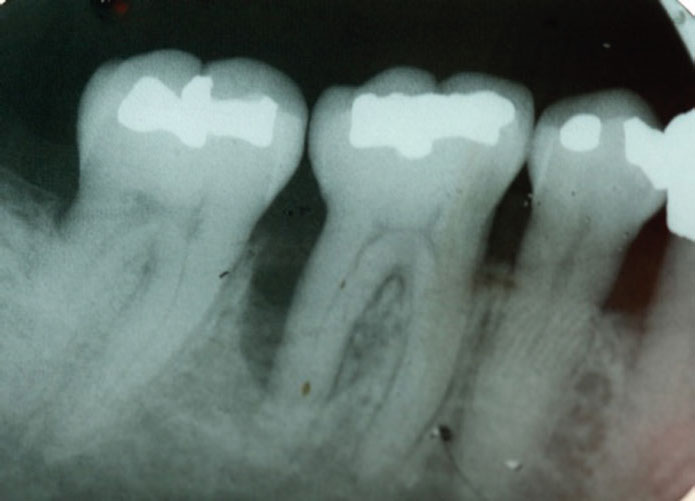
Further work by Cheetham8 and Smart9 led to the coining of the term ‘debridement’, the less aggressive management of the root surface using ultrasonic instruments that were more conservative of the tooth structure. Figure 2 shows the iatrogenic damage caused to a tooth by traditional root planing.
Figure 2. Iatrogenic damage caused by root planing.
Despite this growing evidence base, many clinicians still advocated the need for hand instrumentation as part of periodontal disease management, with many advocating that a ‘blended approach’ was best. However, the recent European S3 Treatment Guidelines4 has finally put this debate to bed with their guideline that asked the question about the superiority of hand instrumentation, ultrasonic instrumentation or a blended approach of the two. Their guideline, that had unanimous support from the experts at the highest level of recommendation, states:
‘We recommend that subgingival periodontal instrumentation is performed with hand or powered (sonic/ultrasonic) instruments, either alone or in combination.’
No one treatment modality is better in terms of clinical outcomes, but we know that ultrasonic debridement is less aggressive, less fatiguing on the operator and can be completed in a shorter time frame making it more efficient.10
Preshaw11 sums up the current thinking very nicely in the opening chapter of the text book, Ultrasonic Periodontal Debridement:
‘Root planing cannot be justified as a treatment concept … put more simply, it is not possible to remove all the calculus, we do not wish to remove the cementum and, therefore, root planing does not have a place in modern periodontal therapy.’
Local delivery antimicrobials
Intra-pocket medicaments were very popular in the 1990s and early 2000s, with local delivery antimicrobials and antibiotics being used regularly as an adjunct to non-surgical treatment. Several of these medicaments still exist, but the evidence base for their use is increasingly unimpressive. A large systematic review by Matesanz-Perez,12 looking at local delivery chlorhexidine, tetracycline and metronidazole agents, showed average additional pocket depth reductions of 0.407 mm and attachment gain of 0.310 mm over non-surgical treatment alone, changes that would not be considered clinically significant.
The S3 Guidelines4 updated this review and their open recommendation, at the lowest level of recommendation, was:
‘Specific locally administered sustainedrelease antibiotics as an adjunct to subgingival instrumentation in patients with periodontitis may be considered.’
Figure 3. A significant infra-bony defect on the distal aspect of LR6.Figure 4. Bony infill following surgical management with Emdogain.
Systemic antibiotics
The use of systemic antibiotics in the management of periodontitis has always been slightly controversial. With the increased awareness for the need for antibiotic stewardship, the clinical decision to use systemic antibiotics needs be restricted to cases where it will have the greatest impact.
The recent S3 Guidelines4 made two recommendations relating to systemic antibiotics and periodontal management:
Due to concerns about patients’ health and the impact of systemic antibiotic use to public health, its routine use as an adjunct to subgingival debridement in patients with periodontitis is not recommended.
The adjunctive use of specific systemic antibiotics may be considered for specific patient categories (eg generalized periodontitis stage IIl and IV in young adults).
The British Society of Periodontology and Implant Dentistry has recommended that systemic antibiotics should only be prescribed for the management of periodontitis by Level 2 and 3 practitioners.
Host modulation therapy
For decades, treatment of periodontitis focused on the aetiological and anatomical factors caused by the disease, that is, the deep pocket. The turn of the century saw the promotion of a host modulating agent in the form of sub-antimicrobial doses of doxycycline (SDD). The 20-mg dose of doxycycline twice a day is significantly below the level required to inhibit bacterial growth, and, as such, is not acting as an antibiotic. At this level, the drug has been shown to inhibit collagenase activity, an important part of tissue destruction in inflammatory disease.
In a large multicentre trial, Preshaw17 showed that there were statistically significant improvements in pocket depth reduction when SDD was used as an adjunct to non-surgical treatment compared to non-surgical therapy alone in deep sites. However the gains, when SDD was used as an adjunct to root planing, were approximately 0.5 mm for 3–9 months of the drug, for which the clinical significance was questioned. The EFP S3 treatment guidelines4 recommend not to use this adjunct.
Periodontal surgery
The 1970s and 1980s were eras of very surgically driven treatment, with much of the surgery proposed being resective in its nature, for example resected flaps, apically repositioned flaps and osseous re-contouring. The primary endpoint was elimination of any deep pockets that could harbour the initiating pathogens, facilitating an environment that was conducive to effective home care.
As our understanding of the disease improved, and surrogate markers for disease activity, such as bleeding on probing, became better understood, the rationale for surgical intervention was questioned. In a lecture in 1997, Jan Lindhe stated:
‘There is no established correlation between probing pocket depth and presence or absence of disease. Symptoms other than increased probing depth should be present to justify surgical therapy – that is subgingival inflammation.’
This was an important statement from a man as influential as Lindhe, because there has been a tendency towards surgical management on any pocket over 4 mm regardless of the inflammatory status. The British Society of Periodontology and Implant Dentistry in their 2018 paper on the UK implementation of the new classification5 stated:
‘…it is important to note that a higher probing depth of 5 mm or 6 mm in the absence of bleeding may not necessarily represent active disease…’
This period also saw a significant increase in the research on regenerative surgical treatments, whereby the lost cementum, ligament and bone in vertical bone defects is regenerated.
The American Academy of Periodontology Position Paper on Periodontal Regeneration11 defined periodontal regeneration as:
‘Periodontal regeneration is defined histologically as regeneration of the tooth’s supporting tissues, including alveolar bone, periodontal ligament, and cementum over a previously diseased root surface.’
Clinically, treatment outcomes following regenerative therapy can only be assessed using surrogate measures because we do not have the ability to histologically assess the presence of new cementum, PDL and alveolar bone. The surrogate endpoints used routinely when assessing regenerative outcomes are evidence of bone fill radiographically and clinical attachment level gain.
Using concepts developed in orthopaedic surgery, Melcher13 outlined the concept of needing to exclude unwanted cell types from the vertical bony defect to allow the desired cells and biological tissues to fill the defect.
Much of the early regenerative periodontal therapy included using defect fillers and barrier techniques with nonresorbable and, later, resorbable membranes, and combinations of the two as described in Sanz and Giovannoli.14 Following thorough debridement of the root and bone defect, guided-tissue regeneration relies on exclusion of the soft tissues from the defect to prevent epithelial downgrowth and connective tissue ingress. This in turn provides a space for a stable blood clot to form, in the absence of soft tissue, in the hope that the clot will mature into the desired hard tissue, with or without periodontal ligament.
The 1990s saw a new regenerative product enter the market in the form of enamel matrix proteins (EMPs), commercially known as Emdogain (Straumann, Basel, Switzerland). This product was quite unique in that it did not use the concept of a physical barrier, but aimed to harness the biology of cementogenesis using proteins extracted from porcine developing tooth germs.15
While both treatment modalities can be predictably used in infra-bony defects to reduce pocket depths and improve radiographic bone levels, we are still unable to regenerate the periodontium when the bone loss is horizontal. Let us hope that the next 50 years can change that.
Summary
A number of things have not changed in periodontal management in the past 50 years and are unlikely to change in the next 50 years. Immaculate home care by the patient, avoidance of the known risk factors and leading a healthy lifestyle remain non-negotiable factors for the successful management of periodontitis.
What has changed in the past 50 years is the move away from medicaments. Medicaments appear to play a very limited role in periodontal management, with the exception of systemic antibiotics in a very specific subset of periodontitis patients, and which would usually be provided by a specialist as part of their treatment plan.
Our non-surgical approaches should be less aggressive and more conservative of tooth tissue because it is clear that we can achieve the same clinical outcomes with less destructive treatment modalities. They are also likely to be more efficient and less fatiguing for the operator.
Non-surgical treatment remains the bedrock of periodontitis management, and the decision to move to surgery should only happen when non-surgical options have been exhausted.
Surgery, where possible, should be regenerative rather than resective, but resective surgery still has a place for those deep and non-responding sites.