Chapple ILC. Periodontal diagnosis and treatment – where does the future lie?. Periodontology 2000. 2009; 51:9-24
Van Dyke TE. The management of inflammation in periodontal disease. J Periodontol. 2008; 79:1601-1608
Baker P, Needleman I. Risk management in clinical practice. Part 10. Periodontology. Br Dent J. 2010; 209:557-565
Chapple ILC. Periodontal disease diagnosis: current status and future developments. J Dent. 1997; 25:3-15
Armitage GC. Development of a classification system for periodontal diseases and conditions. Ann Periodontol. 1999; 4:1-6
Loe H, Anerud A, Boysen H, Smith M. The natural history of periodontal disease in man. The rate of periodontal destruction before 40 years of age. J Periodontol. 1978; 49:607-620
Loe H, Anerud A, Boysen H, Morrison E. Natural history of periodontal disease in man. Rapid, moderate and no loss of attachment in Sri Lankan laborers 14 to 46 years of age. J Clin Periodontol. 1986; 13:431-440
O'Dowd LK, Durham J, McCracken GI, Preshaw PM. Patients' experiences of the impact of periodontal disease. J Clin Periodontol. 2010; 37:334-339
Jonsson B, Ohrn K, Oscarson N, Lindberg P. The effectiveness of an individually tailored oral health educational programme on oral hygiene behaviour in patients with periodontal disease: a blinded randomized-controlled clinical trial (one-year follow-up). J Clin Periodontol. 2009; 36:1025-1034
Jonsson B, Ohrn K, Oscarson N, Lindberg P. An individually tailored treatment programme for improved oral hygiene: introduction of a new course of action in health education for patients with periodontitis. Int J Dent Hyg. 2009; 7:166-175
Preshaw PM. Periodontal disease and diabetes. J Dent. 2009; 37:S575-S577
Tomar SL, Asma S. Smoking-attributable periodontitis in the United States: findings from NHANES III. National Health and Nutrition Examination Survey. J Periodontol. 2000; 71:743-751
Heasman L, Stacey F, Preshaw PM, McCracken GI, Hepburn S, Heasman PA. The effect of smoking on periodontal treatment response: a review of clinical evidence. J Clin Periodontol. 2006; 33:241-253
Nasry HA, Preshaw PM, Stacey F, Heasman L, Swan M, Heasman PA. Smoking cessation advice for patients with chronic periodontitis. Br Dent J. 2006; 200:272-275
Fiore MC, Jaen CR, Baker TBRockville, MD: US Department of Health and Human Services, Public Health Service; 2008
Ramseier CA, Warnakulasuriya S, Needleman IG Consensus Report: 2nd European Workshop on Tobacco Use Prevention and Cessation for Oral Health Professionals. Int Dent J. 2010; 60:3-6
Needleman I, Warnakulasuriya S, Sutherland G Evaluation of tobacco use cessation (TUC) counselling in the dental office. Oral Health Prev Dent. 2006; 4:27-47
Campbell HS, Sletten M, Petty T. Patient perceptions of tobacco cessation services in dental offices. J Am Dent Assoc. 1999; 130:219-226
Kinane DF. Single-visit, full-mouth ultrasonic debridement: a paradigm shift in periodontal therapy?. J Clin Periodontol. 2005; 32:732-733
Eberhard J, Jepsen S, Jervoe-Storm PM, Needleman I, Worthington HV. Full-mouth disinfection for the treatment of adult chronic periodontitis. Cochrane Database Syst Rev. 2008; 1
Sanz M, Teughels W. Innovations in non-surgical periodontal therapy: Consensus Report of the Sixth European Workshop on Periodontology. J Clin Periodontol. 2008; 35:3-7
Fardal O, Johannessen AC, Linden GJ. Tooth loss during maintenance following periodontal treatment in a periodontal practice in Norway. J Clin Periodontol. 2004; 31:550-555
Fardal O. Periodontal maintenance – overcoming the barriers. Dent Update. 2011; 38:38-48
The treatment of periodontitis is a complex process that can last for many years. Successful management of this common inflammatory condition necessitates team work by the patient, dental hygienist and dentist. A variety of complex skills are required including, not only the necessary clinical skills, but also excellent communication, education and motivation of patients. Above all, time is required to treat the condition properly, and successful outcomes depend heavily on engaging with and empowering the patient to manage his/her condition. Patients need to be active partners in the management of their periodontitis (supported by the dental team), and this will only happen if the time is spent to educate them on their role. Communication is essential for successful management, and behaviour change is always required of patients. Strategies for working effectively with a dental hygienist, and a suggested treatment protocol are presented to help dentists develop more effective methods of treating periodontitis.
Clinical Relevance: This article gives practical guidance on how to manage patients with periodontitis as well as working within the dental team to achieve the best clinical outcomes.
Article
The aim of this paper is to give practical guidance for busy general dental practitioners, dental hygienists and dental therapists to help them manage periodontitis more effectively. The successful management of periodontitis requires significant amounts of time to be spent with patients, and also depends heavily on the patients' involvement in managing their condition. Patients need to be active partners in the process, working together with the dental clinician, and this mandates the clinician to spend time with patients, to educate them on their role.
What is periodontitis?
This may seem a surprising question – we can all recognize periodontitis when we see it in our patients, but it is useful to consider briefly current concepts of disease. We all know that periodontitis is initiated by the bacterial biofilm (ie subgingival plaque), but that is far from being the full story. Current thinking about the nature of periodontitis is captured in these statements taken from recent publications in the periodontal literature:
‘Periodontitis is more accurately characterised as a non-resolving inflammation that is ineffective in eliminating the initiating pathogens’.1
‘Periodontitis is an inflammatory disease initiated by oral microbial biofilm… it is the host response to the biofilm that destroys the periodontium’.2
The recognition that the inflammatory response is responsible for the majority of the tissue breakdown helps to explain why some people are more susceptible to periodontitis (even if they have good oral hygiene), why periodontitis can seem to run in families (because aspects of immune and inflammatory responses can be genetically determined), and why some people appear to be relatively resistant to developing periodontitis, despite the fact that they might have very poor plaque control.
Taking the history
Start with the presenting complaint – what are the patient's concerns? Unfortunately, the signs and symptoms of advanced periodontitis present late in the disease process, by which time there may already be extensive attachment loss. Patients will often mention bleeding gums (their gums may have bled for so long that they think it is almost normal), but this does not discriminate between gingivitis and periodontitis. Sometimes, patients will mention gaps appearing between teeth, or mobile teeth – both of these can be indicative of advanced disease. Unfortunately, periodontal treatment alone may not remedy these concerns, and the patient should be made aware of this from the outset.
Ask about any previous periodontal treatment. Unfortunately, it can be difficult to understand exactly what treatment a patient has had. Patients may report ‘deep cleaning’ being done, but if this involved a small number of very short appointments, then how useful was it? Nonetheless, this information may be relevant to the treatment planning process.
Ask about any family history of periodontal problems. This is particularly important in suspected cases of aggressive periodontitis.
Record a full medical history. The most relevant aspects to periodontology are smoking, diabetes and medications (eg medications that can be associated with drug-induced gingival overgrowth). For smokers, record the number of cigarettes per day and the number of years of smoking. For ex-smokers, record when they quit, for how many years they smoked, and the number of cigarettes per day. In people with diabetes, ask about their level of control: is it good or poor? What was their most recent glycated haemoglobin score (HbA1c)? (HbA1c is used to assess diabetes control over the preceding 2–3 months, and levels <7.0% indicate good glycaemic control.)
Periodontal examination
In most dental practices, the initial examination of a new patient will be done by the dentist. It is essential that the dentist assesses the periodontal tissue by recording the BPE (Basic Periodontal Examination). Detailed guidance on how to conduct the BPE is available on the British Society of Periodontology (BSP) website (www.bsperio.org.uk), and the scoring codes are shown in Table 1. The BPE should be recorded for all new patients. For patients with codes 0, 1 or 2, the BPE should ideally be recorded at each dental appointment, and at least annually. For those with BPE codes of 3 or 4, detailed periodontal charting is necessary (often this will be done by a dental hygienist or dental therapist):
Code 3: record full probing depths (6 sites per tooth) in the sextant(s) where the code 3 was recorded.
Code 4: record full probing depths throughout the entire dentition.
Clinic findings
Interpretation of BPE score
0
No pockets >3.5 mm, no calculus/overhangs, no bleeding after probing (black band completely visible).
Code 0 represents health. No periodontal treatment is indicated.
1
No pockets >3.5 mm, no calculus/overhangs, but bleeding after probing (black band completely visible).
Code 1 represents gingivitis. Oral hygiene instruction (OHI) is required.
2
No pockets >3.5 mm, but supra- or subgingival calculus/overhangs (black band completely visible).
Code 2 represents gingivitis plus other factors (eg calculus, overhangs). Perform OHI, and remove local factors including supra/subgingival calculus.
3
Probing depth 3.5–5.5 mm (black band partially visible, indicating pocket of 4–5 mm).
Code 3 represents early/moderate periodontitis. Record full probing depths for the affected sextants. Provide OHI and root surface debridement (RSD).
4
Probing depth >5.5 mm (black band entirely within the pocket, indicating pocket of 6 mm or more).
Code 4 represents advanced periodontitis. Record full probing depths for entire dentition. Provide OHI and RSD.
*
Furcation involvement.
* Is added to the numerical score for the sextant to indicate presence of a furcation.
Notes: (i) use the WHO probe to record the BPE; (ii) interpretation of BPE scores depends on factors unique to the clinical situation, and clinicians should use their skill, knowledge and judgement when interpreting BPE scores; (iii) the BPE score is not a diagnosis.
The detailed charting in cases of periodontitis is essential not only for the diagnosis, but also to assess the response to periodontal treatment. The periodontal examination should also include an assessment of oral hygiene, though detailed plaque scoring is not essential at this stage (it may be more useful later on in the treatment to give more detailed information about oral hygiene techniques that the patient needs to perform).3 However, bleeding on probing (BOP) should be assessed: absence of BOP is a predictor of periodontal stability,4 though the situation can be confusing in smokers who typically present with less BOP. Individual mobility scores should be recorded for any mobile teeth, as well as furcation involvements.
Radiographs
As a general rule, radiographs should be taken for periodontal assessment in cases with BPE codes of 3 or 4. The choice of radiographs depends on the clinical situation. Horizontal bitewings are taken routinely for caries assessment, and will additionally give an indication of early alveolar bone loss, but will not be useful in advanced cases. Vertical bitewings overcome this disadvantage, but do not usually show the apices of the teeth. Periapical radiographs are probably the most useful for the majority of practitioners to assess alveolar bone levels, and they also provide information on apical status and endodontic/restorative treatment needs. Modern panoramic machines also provide good quality information and show the entire dentition. In all cases, a radiographic report must be entered in the patient's notes that describes the extent (eg 20%, 50%) and pattern (eg regular, irregular, horizontal, vertical) of the bone loss.
Diagnosis
Once the clinical and radiographic examinations have been performed (together with any other special investigations such as vitality testing or occlusal examination) the diagnosis should be recorded using the current periodontal classification criteria (Table 2).5 The most commonly encountered diagnoses in general dental practice are likely to be gingivitis or chronic periodontitis. Around 10% of the UK adult population suffer from advanced chronic periodontitis, which is typically slowly progressing. Practitioners should be alert to the possibility of aggressive periodontitis. This condition is much rarer (certainly less than 1% of the population) and is characterized by rapid attachment loss, familial aggregation, and severe disease presenting in younger individuals (usually <35 years old). There may be very little plaque or calculus present. Aggressive periodontitis may be localized (affecting first molars and incisors plus no more than two other teeth), or generalized.
Gingival diseases (eg plaque-induced gingivitis)
Chronic periodontitis
Aggressive periodontitis (localized or generalized)
Periodontitis as a manifestation of systemic diseases (eg neutropenia, leukaemia)
Communicating with patients is probably the most important part of managing periodontitis. It would be of very limited benefit to see a patient every 3 months to perform lengthy episodes of root surface debridement if the patient is not performing any oral hygiene practices at home. Therefore, although it may sound glib, the first thing to do is to communicate with the patient. Unfortunately, this takes time, but we must spend this time with our patients if we (and they) are going to manage periodontitis successfully. Unlike many other forms of dentistry, the outcomes of periodontal treatment depend hugely on the patient's management of his/her condition. We should show the patient the probing chart, and explain the radiographs to them. Periodontitis is a chronic inflammatory disease, and its management must be considered a chronic (ie life-long) process. Patients must be aware of this from the outset and it is important to stress that there is no ‘quick fix’.
Responsibilities have to be clearly defined, for both the patient and the clinician, when treating periodontitis. Patient responsibilities include attending for appointments, and achieving a high standard of oral hygiene. Clinician responsibilities include explaining the disease process, educating the patient on his/her role in managing it, providing excellent clinical treatment (eg oral hygiene instruction and root surface debridement), and maintaining and monitoring the patient, as well as referring for specialist opinion when necessary.
‘Personalized biofeedback’ is an important technique in educating patients about how to manage their periodontitis. In simple terms, this means making it relevant to patients and their clinical situation. This should include positive feedback messages, such as linking improved oral hygiene in a particular area of the mouth to reduced gingival inflammation in the same area (eg after using a single tufted toothbrush at imbricated lower incisors). These messages can be extremely powerful for patients as they develop self-efficacy in managing their disease.
Changing the patient's behaviour
A partnership between the patient and clinician is required to treat periodontitis, in other words, the patient needs to be more than just a passive receiver of treatment. We need the patient to be ‘on our side’ if we (and they) are going to manage the condition effectively. The first step is to adopt a sympathetic and caring attitude. Explain that we are not all equally susceptible to periodontitis6,7 (many patients think that periodontitis is ‘their fault’). Periodontitis is an unpleasant and distressing condition with multiple negative impacts on daily living, social interactions and quality of life,8 and a dismissive or negative attitude by the clinician will not help.
Ideally, we want patients to develop self-efficacy in managing their periodontitis. Self-efficacy is a concept used in psychology which refers to an individual's belief in his/her ability to perform a particular task. Successful treatment of periodontitis involves:
Structured patient education and empowerment;
Establishing treatment needs and setting goals;
Personalized biofeedback (eg reductions in gingival bleeding and probing depths);
Frequent recall, and the involvement of various members of the dental team, particularly dental hygienists. Structured education programmes have been introduced and shown to be effective in the management of periodontitis.9,10
In order to develop self-efficacy, several steps are required, all of which take time. First, the patient must understand the disease, and there is no option but to discuss the disease process in detail (Table 3). We must also explain to patients that their role in managing their periodontitis is fundamental to the success of treatment. If patients can experience improvements in their gingival health as a result of their own actions, this can be a very powerful symbol which will help them develop self-efficacy. Another step towards self-efficacy involves developing concrete plans with patients for how they will manage their condition, particularly in respect to plaque control. We need to establish a time of day when it will be convenient for the patient to spend the required time performing oral hygiene techniques. It doesn't necessarily need to be just before bed, but ideally it should be at the same time every day, so that it becomes a routine. It is perfectly acceptable for a patient to perform just one episode of really good oral hygiene per day (typically lasting 5–10 minutes for a patient with periodontitis), including brushing (manual or powered), interproximal cleaning, and use of the single-tufted toothbrush. It could be when a particular radio or TV programme comes on, or it could be after dropping off children at an evening activity. It doesn't matter as long as it is regular, so that oral hygiene becomes linked to a particular daily event. Oral hygiene instruction should be primarily about instituting behaviour change. There is no point spending time explaining the intricacies of angulation of toothbrush bristles against the gingival margin if we don't put in place a plan of when, and for how long, the patient should be performing oral hygiene procedures. It is important to document the oral hygiene instruction given, and patient compliance with this instruction, carefully.
Explain the disease process in detail, but at a level that is suitable:
‘Periodontitis results from the body's reaction against the bacteria in plaque. This leads to the development of inflammation in the gums, which results in the gum receding, pockets (spaces) developing between the gum and the tooth (which are harder to keep clean), and bone receding as the gums recede, leading to looseness of the teeth’.
Explain, in particular, the importance of risk factors like smoking:
‘Smoking affects the immune system so that gum disease is worse in smokers. Quitting smoking is one of the most important things that someone can do to improve their gum condition’.
Explain the importance of patient-performed oral hygiene:
‘It's not fair, but given that you have this condition, you need to work harder than the average person at keeping your teeth clean. That can mean spending a good 5–10 minutes in the bathroom every day using all sorts of brushes. You need to become an expert toothbrusher – a gold medallist at the toothbrushing Olympics’.
Written information should be given to the patient. This can include information leaflets about periodontitis (for example, those provided by the BSP, www.bsperio.org.uk). It can be particularly useful to give the patient a print-out of clinical photographs showing oral hygiene products being used correctly in their own mouth (Figure 1). A simple digital camera is sufficient, with the reception staff dropping the photos into a template that can then be printed on a colour printer and given to the patient at the end of the appointment. This is much more relevant and memorable for the patient than a session with a toothbrush and study model, and by printing the information out, the patient is much more likely to act upon it afterwards.
Figure 1. An instruction sheet showing the patient how to use oral hygiene products in his/her own mouth is a great visual reminder for patients of how to do the job properly.
Risk management
Risk management is an extension of behaviour change. The two major risk factors for periodontitis are smoking11 and diabetes.12
Smoking was suggested to be responsible for more than half the cases of periodontitis in an epidemiological study in the USA.13 Smoking has multiple negative impacts on aspects of immune functioning and inflammation, leading to increased periodontal tissue destruction, and more limited outcomes following periodontal treatment compared to non-smokers.14 These negative impacts include reduced gingival blood flow, impaired white cell function, impaired wound healing, and increased production of inflammatory mediators in the periodontal tissues. Bleeding on probing is frequently less evident in smokers, and some patients, upon quitting smoking, are alarmed to find that they have increased gingival bleeding. This is actually a good sign, indicating that blood flow to the tissues is increasing, with greater potential for healing, but patients need to be warned about this in advance and advised not to worry.
Members of the dental team have an important role to play in helping patients to quit smoking, which should be viewed as a process rather than a single event. Many dental hygienists have received training in smoking cessation, but even if members of the dental team are not specifically trained for this task, they should follow the ‘A, A, R’ regime:
Ask: about smoking status;
Advise: about the harmful effects of smoking on the periodontium;
Refer: to a specific smoking cessation clinic.
Quit rates 12 months after stopping smoking are about 3% if the patient uses willpower alone, and about 5% if there is brief intervention by a clinician. The quit rates rise to about 20% if the patient attends a smoking cessation clinic, and similarly high quit rates have been achieved by dental hygienists.15 Helping a patient to quit smoking is an enormously rewarding aspect of professional life. The majority of current smokers actually want to quit smoking, and it is evident that combining treatments (eg nicotine replacement therapy (NRT), bupropion, Champix) with behavioural support is more likely to be successful in smoking cessation.16 Repeated interventions, support and maintenance are likely to be required.
Informing patients of the consequences of tobacco use is an ethical, medical and legal obligation.17 However, dental professionals sometimes feel that patients might be offended by discussion about smoking cessation, particularly if the dental clinician is asking the questions repeatedly. Consequently, only 33–50% of dental professionals ask about smoking habits and even fewer document that they have asked.18 On the other hand, evidence suggests that patients expect to be asked about their smoking habits by dental professionals and do not feel offended.19 Given the harmful effects of smoking on the periodontal tissues, we should feel confident in asking questions about smoking status, and we can make things easier by using non-threatening forms of words such as ‘I wouldn't be doing my job properly if I didn't ask you about whether you are still smoking’.
Non-surgical instrumentation
It may come as a surprise that instrumentation is mentioned only now – this is deliberate, to emphasize the importance of communication, behaviour change and risk management. Treatment of most forms of periodontitis will commence with non-surgical instrumentation. In the past, this was referred to as ‘scaling and root planing’, which meant planing the root surface to remove the outer layer of cementum, a strategy that we now recognize as being overly aggressive, unnecessary, and that can result in considerable sensitivity post-treatment.
Modern instrumentation techniques are better described as ‘root surface debridement’ (RSD) to indicate a gentler form of treatment. The aim of RSD is to disrupt and remove the plaque biofilm to reduce the bacterial challenge, thereby reducing inflammation in the periodontal tissues. Plaque retentive factors such as calculus and overhangs should be removed at the same time (and this will also improve access for cleaning by the patient). RSD is a technically demanding procedure for the clinician. No differences in effectiveness have been demonstrated between hand instruments or powered scalers (ultrasonics or sonics), but powered instruments are faster, and current treatment strategies focus on using ultrasonics to disrupt the biofilm, utilizing overlapping, multiple light strokes of the instrument.20
Similarly, no differences in effectiveness have been demonstrated between ‘traditional’ treatment strategies (eg instrumentation on a quadrant-by-quadrant basis at two week intervals) and ‘full-mouth’ debridement strategies.21 Furthermore, the use of subgingival antiseptics (eg irrigation with chlorhexidine) does not predictably or significantly improve the outcomes of full-mouth treatment approaches. Therefore, all three treatment modalities (ie quadrant-by-quadrant RSD, full-mouth RSD plus chlorhexidine, full-mouth RSD without chlorhexidine) can be used in the treatment of periodontitis.22 Clinicians should choose the mode of treatment according to the needs and preferences of the patient, and the logistic settings (eg availability of time in appointment book and patient work commitments). It is important to remember that non-surgical periodontal treatment is, on the whole, a very effective form of treatment, as long as time is taken to do it properly. Also, it should be noted that optimal oral hygiene is an inseparable principle to be observed with any instrumentation protocol.22
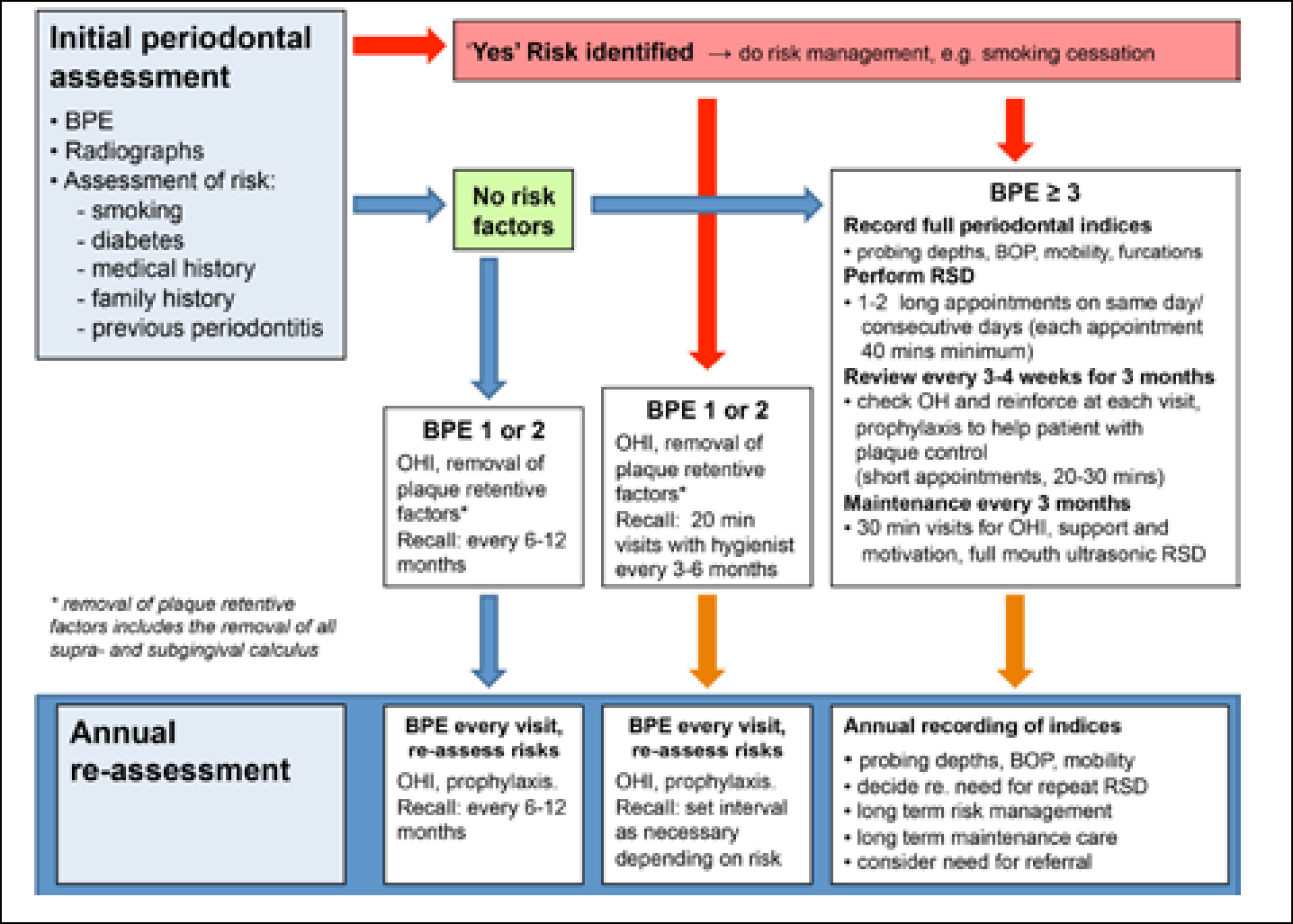
Although the outcomes of these different treatment modalities can be expected to be similar in terms of probing depth reductions, we do consider that there can be useful additional benefits following a full-mouth RSD approach. For example, the patient is aware immediately of positive outcomes, such as reduced bleeding and frequency of abscesses, dramatic improvements in gingival inflammation, and a big improvement in how his/her mouth feels. A suggested scheme for providing periodontal therapy utilizing a full-mouth RSD protocol is shown in Figure 2.
Figure 2. A suggested sequence for the management of periodontitis utilizing a full-mouth root surface debridement (RSD) approach.
How to work with a hygienist
Dental hygienists and therapists are registered dental professionals who help patients maintain their oral health by preventing and treating periodontitis. They promote all aspects of good oral health practice to a wide range of patients and are highly skilled in the non-surgical management of periodontitis. The full scope of their practice is shown in Table 4.
Dental hygienists:
Plan the delivery of care for patients to improve and maintain their periodontal health via detailed assessment and monitoring, using periodontal indices and radiographs
Provide preventive care to patients by liaising with dentists over the treatment of caries, periodontitis and toothwear
Undertake supra- and subgingival scaling and root surface debridement using manual and powered instruments
Administer infiltration and inferior dental block analgesia
Use appropriate antimicrobial therapy to manage periodontitis
Adjust restored surfaces in relation to periodontal treatment
Apply topical fluoride treatments and fissure sealants
Place temporary dressings and re-cement crowns with temporary cement
Take impressions
Carry out oral cancer screening
Additional skills a hygienist may develop after appropriate training:
Tooth whitening to the prescription of a dentist
Prescribe radiographs
Administer inhalation sedation
Remove sutures after the wound has been checked by a dentist
Place rubber dam
Dental therapists can do the same as a hygienist, but in addition they can also:
Carry out direct restorations on permanent and primary teeth
Carry out pulpotomies on primary teeth
Extract primary teeth
Place pre-formed crowns on primary teeth
Historically, hygienists and therapists worked to a prescription, written by the dentist and reviewed annually. Recently, this changed and the now called ‘treatment plan’ written by the dentist remains valid for up to three years. At initial assessment, the examining dentist must confirm the date of the next reassessment with the hygienist, depending on the patient's clinical needs. However, the hygienist or therapist can recall the patient earlier, depending on his/her preventive or periodontal needs. Presently, hygienists and therapists do not carry out a patient's initial diagnosis or take overall responsibility for planning a patient's periodontal treatment; however, this is currently under review by the UK General Dental Council (GDC). Hygienists can run their own practice and accept referrals from nearby dentists, or they can work on a sessional basis within a dental team.
The treatment plan can be a simple statement, such as ‘provide routine oral care for this patient to ensure the prevention, treatment and maintenance of good oral health for the next three years’. Or, for more complex cases, a more detailed treatment plan is indicated, with a shorter interval until reassessment by the referring dentist. The treatment plan should contain:
The date the patient was assessed;
The diagnosis;
An outline or full treatment plan;
Reference to recall intervals (even if ‘as you see necessary’); and
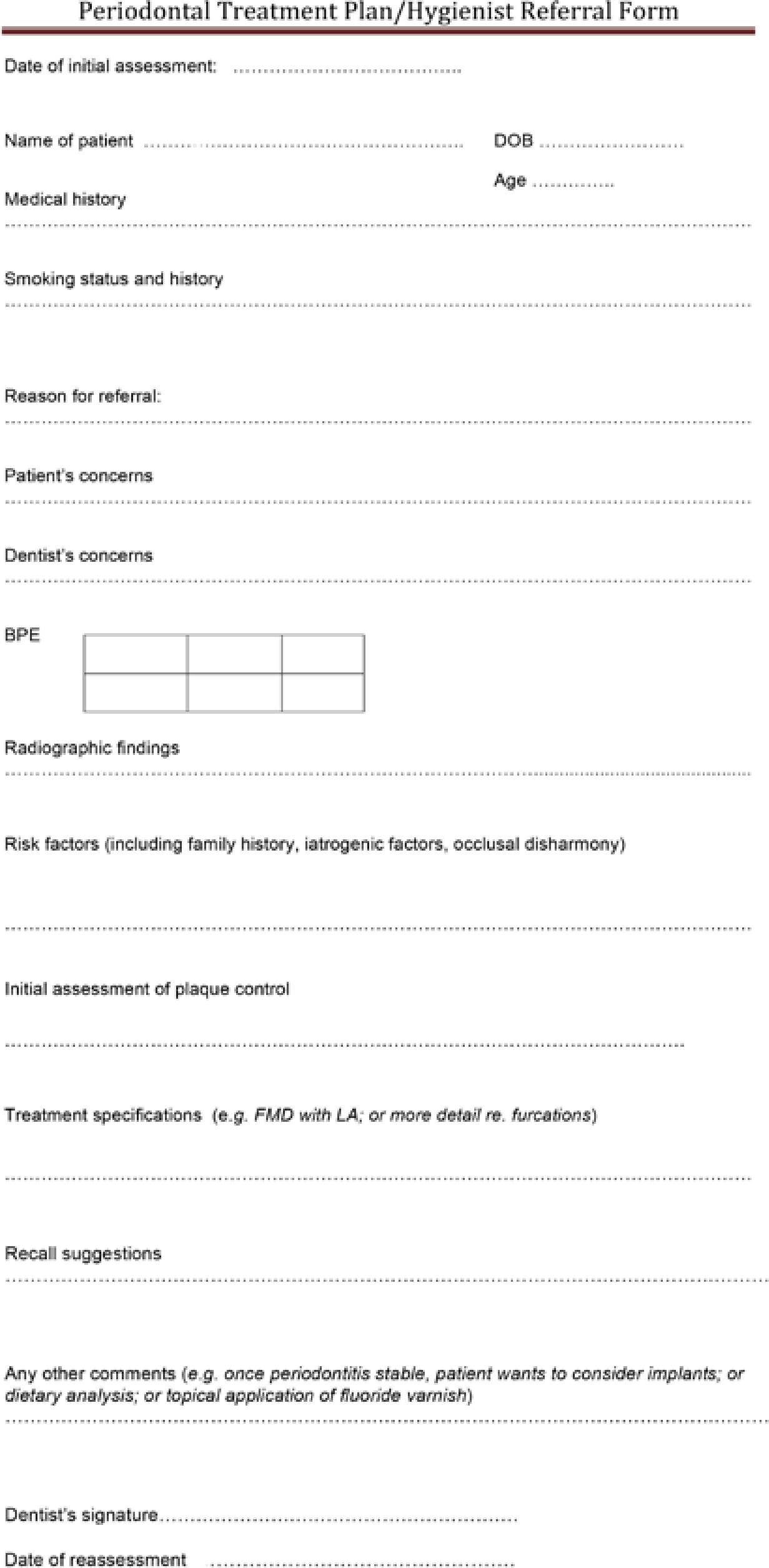
The date of the next reassessment by the dentist. An example of a detailed periodontal referral form is shown in Figure 3.
Figure 3. An example of a periodontal treatment plan/hygienist referral form.
The treatment plan is not just a legal document; it can be a vital form of communication. Effective communication is at the core of successful periodontal treatment. The importance of good communication between the clinician and patient has already been stressed; it is equally important to have good communication between the dentist and hygienist. Often, hygienists can be left a little ‘in the dark’ about what the dentist has already said to the patient, which can sometimes place the hygienist in a difficult position when he/she sees the patient. Face-to-face communication between dentist and hygienist is always best, but not necessarily possible during a busy practice session. Calling the hygienist into the consultation room and introducing him/her to the patient as someone who is highly skilled in treating periodontal disease is a great way to start, and validates the hygienist's role in the eyes of the patient. When this is not possible, providing extra information on the treatment plan, such as the reason for referral and patient's/dentist's concerns, is very useful and saves a lot of time in the hygienist appointment.
For many dental practices, the most cost-effective way to provide periodontal treatment is to employ a dental hygienist. But, sufficient time needs to be allocated to the hygienist to do the job properly. Is it really possible to treat periodontitis in 15 minute appointments every 3 months? Is it really possible to use ultrasonics safely without having a dental nurse? Trying to perform non-surgical management within an oppressively rigid or inadequate system is a sure way for the hygienist to end up demotivated and jaded. However, non-surgical treatment done well can produce really impressive results that please everyone; dentist, hygienist and, most importantly, the patient. Figure 2 shows a suggested protocol for providing periodontal therapy.
The initial assessment will be done by the dentist and will include the BPE, radiographs, and assessment of risk factors, as outlined above. Any identified local plaque retentive factors should be removed by the dentist at this stage. For patients with BPE codes of 3 or 4, the decision may then be to refer to the hygienist for treatment. At the first visit with the hygienist, probing depths would be recorded (as described above). The number and distribution of pockets ≥ 5 mm is then recorded – this will help to make decisions about the length of time needed to treat, the use of local anaesthetic, and can be used to set treatment targets (see below). Potentially, removal of supragingival calculus could also be done at this appointment, if it would allow for better access to interdental aids, and some simple oral hygiene instruction – which could be built on next time. Oral health education and promotion could be carried out by a dental nurse who has done the appropriate additional training. This would extend the ethos of a teamed approach to patient care, with the dentist at the lead. Dental nurses are often very keen to take on more patient interaction and this would reduce the time needed by the hygienist, possibly reducing the costs of the overall periodontal management.
The treatment sessions with the hygienist then occur. We recommend a full-mouth RSD approach with local anaesthetic and progressively detailed oral hygiene instruction. Throughout this process, there is a heavy emphasis on patient education, behaviour change, and modification of risk factors. Post-treatment probing should not be performed any earlier than 3 months after completion of the active periodontal treatment. During the first 3 months after the RSD appointments, the patient should be reviewed every 3–4 weeks (short appointments 20–30 minutes), however, during these appointments the patient's symptoms are discussed; oral hygiene is assessed and reinforced; and prophylaxis is performed to help patients with plaque control during the early healing phase.
At about 3 months following completion of initial therapy, a full probing chart is recorded to assess the outcomes of treatment. Decisions can then be made, in conjunction with the dentist on the long-term maintenance programme. Typically, patients are reviewed by the hygienist every 2–3 months in the maintenance programme.
It can often seem that patients with periodontitis cycle through episodes of treatment with no clear end-point in mind, which can be demoralizing for both the clinician and the patient. Setting targets for treatment can be useful, and probably the two most useful are bleeding on probing (BOP) scores and numbers of deep sites (≥5 mm). For example, achieving a BOP score of <20% would be a good target to aim for, but sometimes this can seem a bit esoteric to patients. A useful target is the number of deep sites remaining after initial therapy. After recording the pre-treatment periodontal indices, it is useful to highlight the deep sites (ie those that are ≥5 mm) on the chart and count them. This is a very simple measure of the extent of the disease, it can be recorded in the patient notes, and then a target can be set. For example, if a patient has 55 sites ≥5 mm pre-treatment, a suitable target could be to reduce this to <10 sites. This gives something to aim for, and a very important sense of achievement for the clinician and the patient once it has been achieved.
Periodontal maintenance care
Following the initial periodontal therapy, the patient enters periodontal maintenance care (also referred to as SPT – supportive periodontal therapy). This is usually best provided by a dental hygienist, and sufficient time should be allocated to the hygienist to provide the necessary treatment. Patients with periodontitis require sufficient time with the hygienist to provide the necessary maintenance care, and a typical periodontal maintenance programme might include 30 minute sessions (as a minimum) with the hygienist every 3 months for provision of full-mouth ultrasonic instrumentation, prophylaxis, motivation and empowering, and reinforcement of oral hygiene instruction. Full probing depths should be recorded on a regular basis to check for evidence of disease progression in the maintenance phase, usually annually. The importance of periodontal maintenance care is clear from studies which show that patients who receive appropriate maintenance lose very few teeth.23 Maintenance care is a life-long concept, and patients must be aware of that from the outset.24
When to refer
Sometimes, complexity of periodontal diseases may require intervention by specialists. Guidelines for when to refer patients for specialist care have been proposed by the BSP (www.bsperio.org.uk). These guidelines assess the complexity of a case based on BPE scores, together with aspects of the history to assign a Complexity Score of 1, 2 or 3 (Table 5). When referring a patient for periodontal treatment, it is important to include aspects such as the history, presence of risk factors, BPE scores/full periodontal indices (depending on the case), copies of radiographs (to avoid unnecessary exposure), details of treatment provided to date, as well as an assessment of the outcomes of that initial treatment. It is also important to be aware that, upon completion of treatment in a specialist centre, patients are usually discharged back to their referring GDPs for maintenance and supportive therapy.
Complexity Score 1Should generally be treated in General Dental Practice
BPE Score 1–3 in any sextant
Complexity Score 2May either be treated by the GDP or referred (depending on knowledge and skills of the GDP)
BPE Score of 4 in any sextant
Surgery involving the periodontal tissues
Complexity Score 3Will mostly be referred
Patients with BPE scores of 4 in at least one sextant, and one or more of the following factors:
– concurrent medical factor directly affecting the periodontal tissues (eg diabetes, medication);
– non-response to previous optimally carried out treatment;
Diagnosis of aggressive periodontitis as assessed either by severity of disease for age or based on rapid rate of periodontal breakdown
Patients requiring surgical procedures involving tissue augmentation or regeneration, including surgical management of mucogingival problems;
Patients requiring surgery involving bone removal (such as crown lengthening);
Patients requiring surgery associated with osseo-integrated implants.
Note: These complexity scores can be modified by the presence of other factors in the history (eg complex medical or dental history, smoking, special needs for dental treatment, mucogingival disease, history of head/neck radiotherapy, intravenous bisphosphonate therapy, immunosuppression, bleeding disorders). For up-to-date guidance, please see www.bsperio.org.uk
Conclusions
The management of periodontitis is not easy. It involves complex skills in a variety of techniques, including communication, education and empowering of patients, as well as the necessary clinical skills such as root surface debridement. Successful management of periodontitis depends heavily on engaging with and empowering the patient to manage his/her condition. Plaque control is the cornerstone of periodontal therapy, and will continue to be for the foreseeable future, as it is the tool by which to control inflammation in the periodontal tissues. Patients must become active partners in the process of treating their periodontitis, supported in this responsibility by the dental team.