Jhaveri H. The aberrant frenum. the father of periodontal plastic surgery. 2006; 29-34
Huang WJ, Creath CJ. The midline diastema: a review of its etiology and treatment. Pediatr Dent. 1995; 17:171-179
Dibart S, Karima M. Labial frenectomy alone or in combination with a free gingival autograft. In: Dibart S, Karima M (eds). Germany: Blackwell Munksgaard; 2006
Miller PD The frenectomy combined with a laterally positioned pedicle graft. Functional and esthetic considerations. J Periodontol. 1985; 56:102-106 https://doi.org/10.1902/jop.1985.56.2.102
Olivi G, Chaumanet G, Genovese MD Er,Cr:YSGG laser labial frenectomy: a clinical retrospective evaluation of 156 consecutive cases. Gen Dent. 2010; 58:126-133
Gontijo I, Navarro RS, Haypek P The applications of diode and Er:YAG lasers in labial frenectomy in infant patients. J Dent Child (Chic). 2005; 72:10-15
Coleton SH. Mucogingival surgical procedures employed in re-establishing the integrity of the gingival unit (III). The frenectomy and the free mucosal graft. Quintessence Int Dent Dig. 1977; 8:53-61
Ito T, Johnson JD. Frenectomy and frenotomy.St Louis, MO, USA: Mosby Wolfe; 1994
Archer WH. Oral surgery for a dental prosthesis, 5th edn. Philadelphia, PA, USA: Saunders; 1975
Kruger GO. Acquired defects of the hard and soft tissues of the face.St Louis, MO, USA: Mosby; 1984
Miller PD The frenectomy combined with a laterally positioned pedicle graft. Functional and esthetic considerations. J Periodontol. 1985; 56:102-106 https://doi.org/10.1902/jop.1985.56.2.102
Devishree Gujjari SK, Shubhashini PV. Frenectomy: a review with the reports of surgical techniques. J Clin Diagn Res. 2012; 6:1587-1592 https://doi.org/10.7860/JCDR/2012/4089.2572
Denonvillers M. Blepharoplastie. Bull Soc Chir Paris. 7:1856-1857
Burke M. Z-plasty. How, when and why. Aust Fam Physician. 1997; 26:1027-1029
Periodontology Specialist Trainee, Periodontology Unit, Centre for Host Microbiome Interactions, Faculty of Dentistry, Oral and Craniofacial Sciences, King's College London
There are various cases where Z-frenuloplasty, a specific Z-plasty technique, can be used, including prior to mucogingival surgery, to manage localized recession defects, pre-prosthetic surgery, post-orthodontic treatment, oral hygiene and ankyloglossia, to name a few. This case series demonstrates the versatility of the Z-plasty technique in oral surgery/periodontal procedures for a variety of indications, as well as describing the technique in detail. The frenectomy technique using Z-plasty for the removal of the abnormal labial frenum attachment is reliable, easy to perform, and provides excellent aesthetic results for a range of indications.
CPD/Clinical Relevance: An appreciation of the Z-plasty technique will allow for tissue healing by primary intention, reduces risk of tissue contractures, improves recovery time, and improves aesthetic results.
Article
A frenum is a mucous membrane fold that contains muscle and connective tissue fibres, attaching the lip and cheek to the alveolar mucosa, the gingivae, tongue and the underlying periosteum.1 Its primary function is to provide stability of the upper and lower lip and the tongue. An aberrant frenum causes gingival recession, either due to an interference in plaque control or due to a muscle pull. It also presents an aesthetic problem, and may compromise the orthodontic result in midline diastema cases, thus causing a recurrence after the treatment.2
The aberrant frena can be treated by frenectomy or by frenotomy procedures for aesthetic and functional reasons. Frenectomy is the complete removal of the frenum, including its attachment to the underlying bone, while frenotomy is the incision and the relocation of the frenal attachment.3
Z-plasty is a plastic surgery technique that is use to improve the functional and cosmetic appearance of scars. Z-frenuloplasty is the Z-plasty technique used on the frenulum, which helps to release scar contracture and relieve soft tissue tension. This case series demonstrates the versatility of the Z-frenuloplasty, or Z-plasty, in oral surgery/periodontal procedures for a variety of indications as well as describing the technique in detail.
Diagnosis of aberrant frena
Abnormal frena are detected visually by applying tension over the frenum to see the movement of the papillary tip or the blanch that is produced due to ischaemia in the region. Miller et al recommended that the frenum should be characterized as pathogenic when it is unusually wide, or when there is no apparent zone of the attached gingiva along the midline, or the interdental papilla shifts when the frenum is extended.4 Several complications due to pathogenic frena are displayed in Table 1, these are also indications for frenectomies. There are some syndromes associated with abnormal frena highlighted in Table 2.
Localized gingival recession with frenum attachment on marginal gingivae (high frenum attachment)
Midline diastema between two maxillary central incisors (low frenum attachment)
Ankyloglossia (tongue tie)
Interference with denture fabrication/wear
Loss of interdental papilla
Difficulty in maintaining adequate oral hygiene around teeth/implants
Malalignment of teeth
Ehlers–Danlos syndrome
Infantile hypertrophic pyloric stenosis
Holoprosencephaly
Ellis–van Creveld syndrome
Oro-facial-digital syndrome
Classification of frena
Placek et al classified the labial frenal attachments as mucosal, gingival, papillary and papilla penetrating, depending on the extent of attachment of fibres:3
Mucosal: when the frenal fibres are attached up to the mucogingival junction;
Gingival: when the fibres are inserted within the attached gingiva;
Papillary: when the fibres are extending into the interdental papilla;
Papilla penetrating: when the frenal fibres cross the alveolar process and extend up to the palatine papilla.
Treatment
Frenectomy can be carried out using routine scalpel techniques, electrosurgery or with lasers. Scalpel techniques carry routine risks of surgery, such as bleeding. The use of electrosurgery is indicated in patients with bleeding disorders, due to its efficacy, and mild bleeding and post-operative complications.5 However, it is associated with certain complications such as burns, interference with pacemakers and the production of surgical smoke. More recently, the use of a CO2 laser in lingual frenectomies has been reported as a safe and effective procedure with multiple advantages including, a simple procedure, reduced pain, bleeding and swelling, absence of post-operative infections and the presence of a small or no scar.6. However, complications include delayed healing compared to conventional surgical techniques and a reduced surgical precision, which can result in unintended laser-induced thermal necrosis.7
Since the conventional procedure of frenectomy was first proposed, a number of modifications8,9,10 of the surgical techniques, such as Miller's technique, Z-plasty and V–Y-plasty have been developed to solve the issues associated with an abnormal labial frenum. These frenectomy techniques are summarized in Table 3. This article focuses on the Z-plasty surgical technique, and is a compilation of a series of clinical cases.
Type of frenectomy
Indications
Advantages
Disadvantages
Classical conventional technique (Archer et al;11 Kruger et al12)
Midline diastema with aberrant frenum
Ease of surgical procedure
Longitudinal surgical incision and scarringLoss of interdental tissuesMay lead to clinical attachment loss and aesthetic concernsMay become a matter of concern in case of a high smile line exposing the anterior gingiva
No loss of interdental papilla and no scar tissue.Post-operatively, on healing, there is a continuous collagenous band of gingiva across the midline, that gives a bracing effect than the ‘scar’ tissue, thus preventing an orthodontic relapse Orthodontic stability without an aesthetic sacrifice
Timing: ideal time for performing this surgery is after orthodontic movement is complete and about 6 weeks before the appliances are removed14
Hypertrophy of the frenum with a low insertionAn inter-incisor diastemaA short vestibule
Allows for tissue healing by primary intentionImproves recovery timeReduces risk of tissue contractures
Flap necrosisHaematoma formationWound infectionSloughing of the flap caused by high wound tensionTrap-door effect (elevation of central tissue resulting from a downward contraction of a surrounding scar)Limited evidence currently on this procedure
V–Y-plasty
Used for lengthening the localized area, such as a broad frena in the premolar-molar areaTechnique to employ in a case of papilla type of frenal attachment
Allows for tissue healing by primary intention Improves recovery timeReduces risk of tissue contractures
Fails to provide satisfactory aesthetic results in the case of a thick hypertrophied frenumHaematoma formationWound infectionLimited evidence currently on this procedure
The classical frenectomy
First introduced by Archer11and Kruger,12 this approach was encouraged in midline diastema cases with an aberrant frenum to ensure the removal of fibre muscles that were allegedly connecting the orbicularis oris with the palatine papilla. This technique is an excision-type frenectomy that includes excision of the interdental tissues and the palatine papilla along the frenum. This classical technique leaves a longitudinal surgical incision and scarring, which may lead to periodontal problems and an unaesthetic appearance, thereby necessitating other modifications.
The Z-plasty
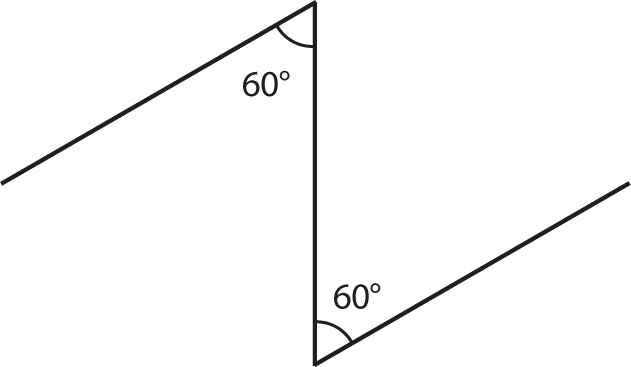
The Z-plasty is a plastic surgery technique used to improve the functional and cosmetic appearance of scars. It involves a central incision and creation of two triangular flaps of equal dimension that are then transposed (Figure 1).16 It breaks up the surgical band into a longer line that runs in zig-zag fashion, so that the tissue tensions are distributed in different directions to relieve the pull on the wound, mitigate against wound disruption and allow for better healing. Translating across to oral/periodontal surgery, the Z-frenuloplasty procedure enables the clinician to remove the fibrous band of frenum, as well as helps in vertical lengthening of the vestibule. The Z pattern is effective in dermatology procedures because it promotes the redistribution of tension on the skin, as well as the wound, and helps in healing along the skin lines.17
Figure 1. Schematic representation of incision lines for Z-plasty.
The technique is indicated when there is a hypertrophy of the frenum with a low insertion, which is associated with an inter-incisor diastema, and when the lateral incisors have appeared without causing the diastema to disappear, and also in cases of a short vestibule. The principle of Z-plasty was first described by Denonvilliers in 1856 for the release of an eyelid scar, and is now used in every part of the body.15
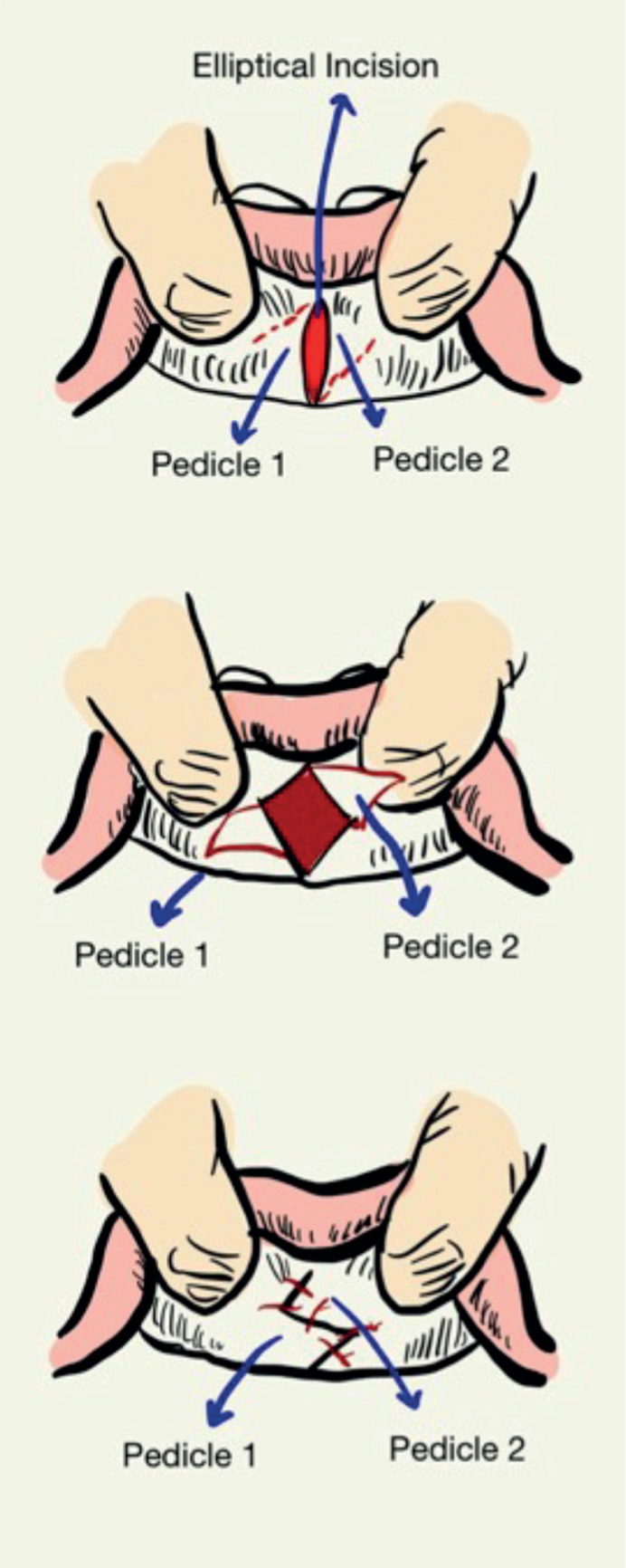
Excise fibrous tissue (frenectomy) or a make a simple incision through the frenum (frenotomy)
Make two oblique incisions at 60°
Undermine pointed flaps
Rotate points to close vertical incision horizontally
Figure 2. Z-plasty technique.
Basic Z-plasty flaps are created using an angle of 60° on each side. Classic 60° Z-plasty lengthens scars by 75%, while 45° and 30° designs lengthen scars by 50% and 25%, respectively.18 The Z pattern is effective as it promotes re-distribution of tension on the skin and the wound, along with healing along the skin lines. This provides a camouflaging effect and helps in minimizing scar formation.
Angles that are smaller than 60° are easier to transpose, but result in less lengthening and realignment of the scar to <90°. Angles larger than 60° should be avoided because the force required to transpose the flaps increases markedly, making closure of the wound difficult. The length of each of the pedicles of the Z-plasty must be precisely equal to the central incision over the original scar, or puckering at the corners will occur, and additional undermining and trimming of the flaps will be necessary to obtain proper closure. Precisely equal lengths and angles of the lateral arms are keys for obtaining proper flap closure after transposition in Z-plasty.
Case 1: pre-mucogingival surgery
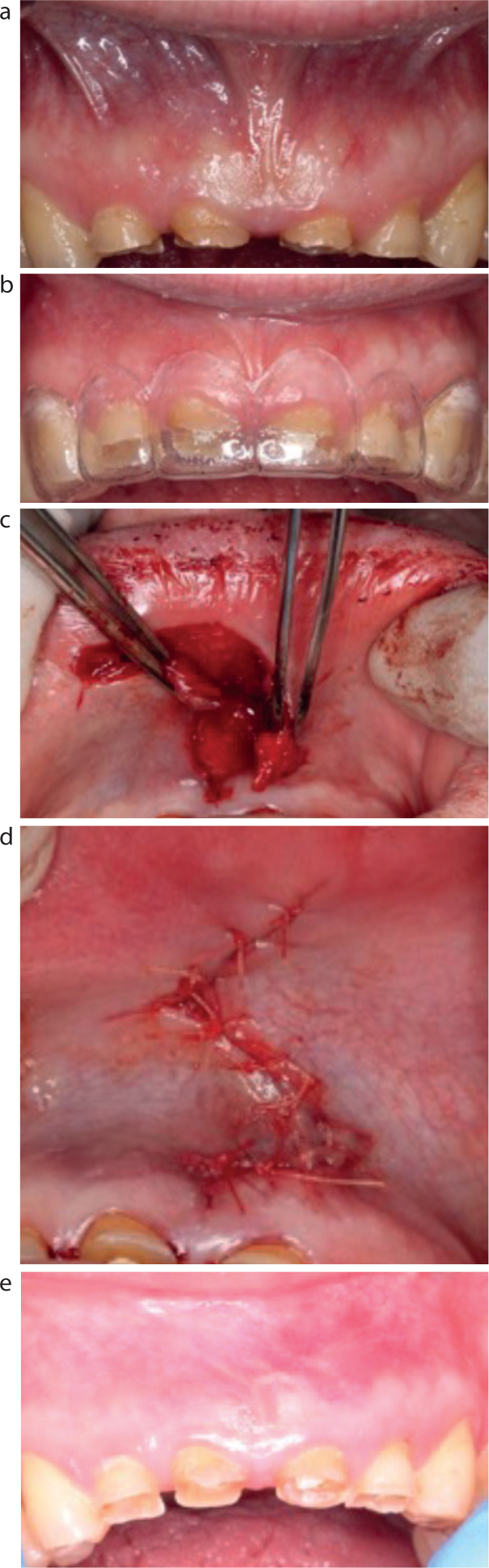
A 28-year-old male patient was referred for the management of his periodontitis. Part of the patient's concern was asymmetry of his maxillary anterior gumline. Following a period of periodontal stability and excellent plaque control, an assessment of the recession defect was made – removal of the frenum would aid in the long-term management. A frenuloplasty was completed, with an excellent outcome, 3 months prior to mucogingival surgery (Figure 3).
Figure 3.
(a) Pre-operative image demonstrating frenal attachment associated with UL3. A frenuloplasty was indicated prior to mucogingival surgery to manage the localized recession defect. (b) Initial vertical incision. (c) Z-shaped incisions. (d) Transposition of flaps and closure with sutures. (e) Post-operative healing at 3 months demonstrating horizontal orientation of scar. There has also been a small increase in keratinized tissue apical to the recession defect that aids subsequent mucogingival surgery.
Case 2: pre-crown lengthening
A 59-year-old male patient was referred for multidisciplinary management of his severe tooth wear. Following appropriate prosthetic planning, it was considered that the midline frenum would impinge on future crown margins with a resective crown lengthening surgery approach. Therefore, a Z-plasty frenotomy was completed successfully, 6 weeks prior to functional crown lengthening surgery (Figure 4).
Figure 4.
(a) Pre-operative image demonstrating high frenal attachment associated with significantly worn dentition. (b) Prosthodontic work up for future indirect rehabilitation demonstrating impingement of frenal attachment and requirement of frenuloplasty prior to a restorative crown lengthening procedure. (c) Peri-operative image demonstrating Z incisions. (d) Closure of Z-plasty. (e) The 3-month post-operative review, demonstrating minimal scar formation and successful re-orientation of muscle fibres.
Case 3: post orthodontic diastema closure
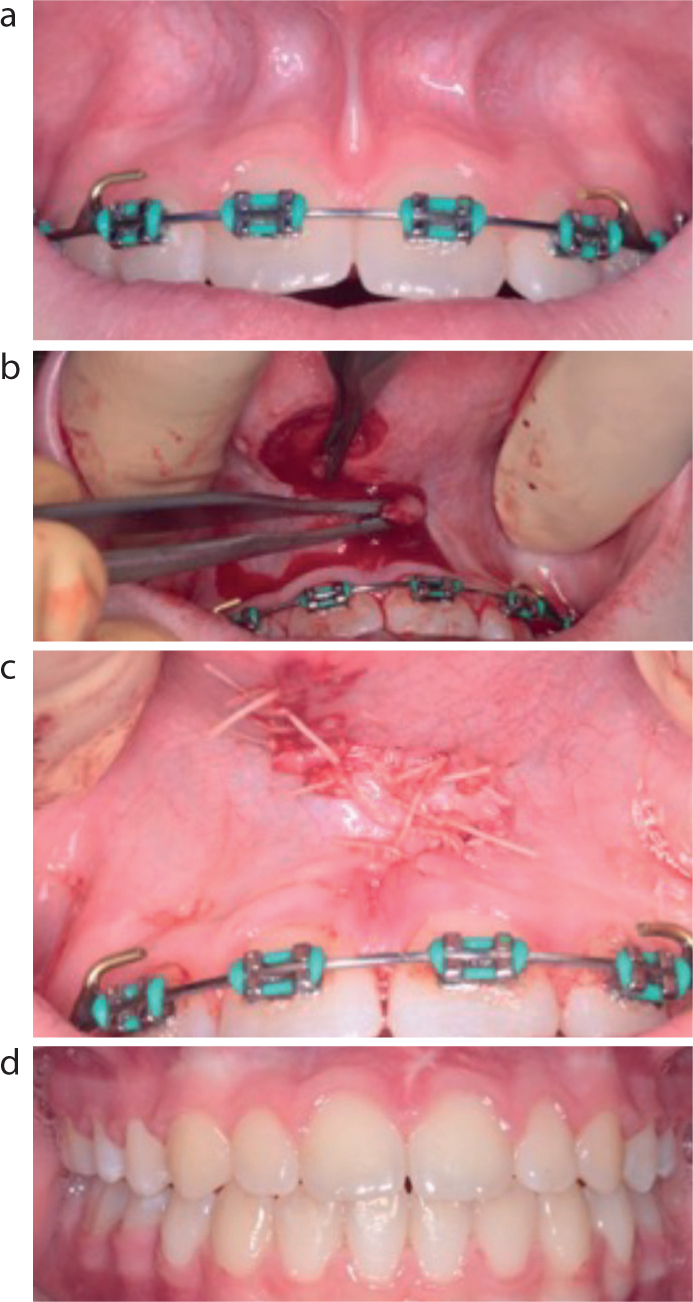
A 14-year-old patient was referred by her orthodontist for removal of the midline frenum prior to debonding following diastema closure, in order to reduce the risk of relapse (Figure 5).
Figure 5.
(a) Pre-operative image demonstrating high frenal attachment following diastema closure with fixed appliances. (b) Peri-operative image demonstrating Z-plasty incisions. (c) Closure of Z-plasty with sutures. (d) The 3-month post-operative review following debonding of fixed appliance, showing minimal scar formation and successful re-orientation of midline frenulum.
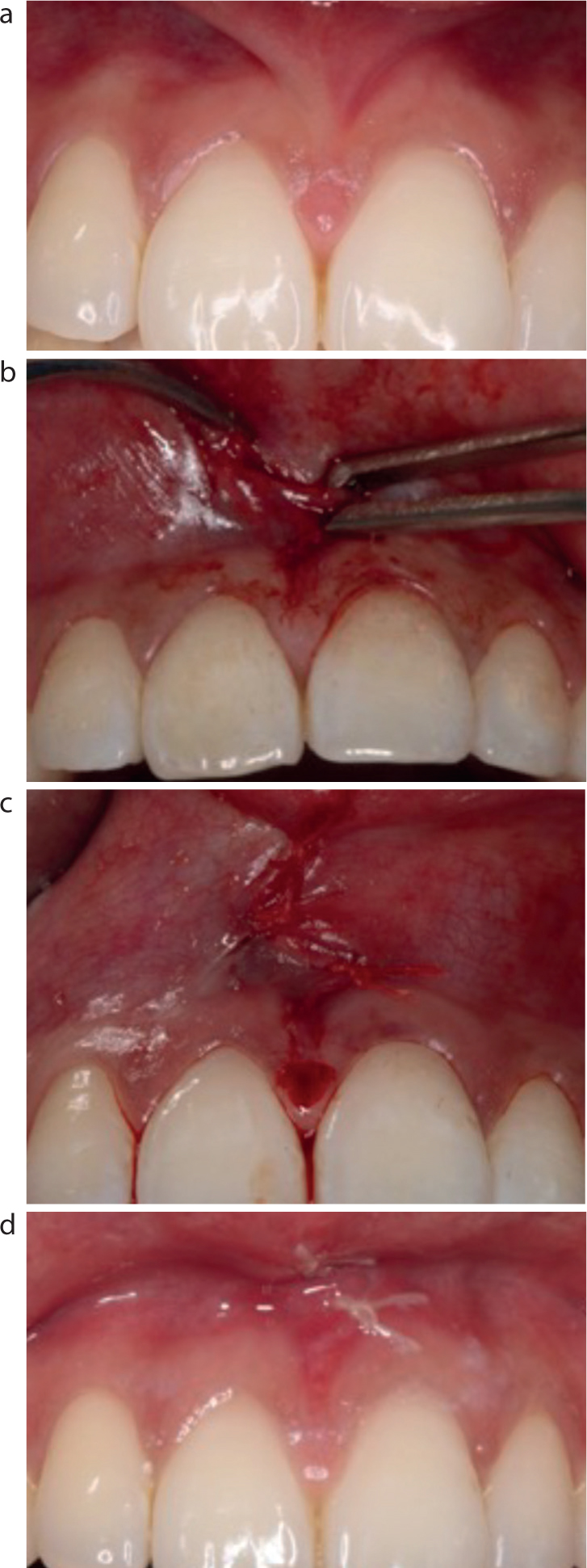
Case 4: assisting with oral hygiene
A 22-year-old female patient was referred for removal of the midline frenum due to persistent inflammation of the interdental papilla and subsequent difficulty maintaining optimal oral hygiene. The patient also reported being unhappy with the poor aesthetic appearance of the prominent frenal attachment on smiling. Following an oral hygiene review, and supragingival scaling of the upper central incisors, a Z-plasty frenectomy was completed successfully (Figure 6).
Figure 6.
(a) Pre-operative photo demonstrating high frenal attachment that was predisposing to inflammation of the midline papilla. The patient reported discomfort on cleaning. (b) Peri-operative image demonstrating transposition of the pedicles. (c) Immediately after the operation. (d) At the 2-week review, there is a favourable outcome with the patient reporting increased comfort with oral hygiene measures
Discussion
There are various cases where frenuloplasty can be used as demonstrated in the cases above including prior to mucogingival surgery to manage localized recession defects, pre-prosthetic surgery, post orthodontic treatment, oral hygiene reasons and ankyloglossia to name a few.
Post-operative instructions include the use of an antiseptic mouthwash (eg chlorhexidine 0.2%), soft diet and analgesics, as required. Sutures used are generally resorbable, but can be removed at the 1-week review with discharge as appropriate.
In line with obtaining valid informed consent for the procedure, it is important clear discussions on benefits and risks are had. The benefits of the procedure are very much case specific, and are evidenced in the cases presented above. Risks of the procedure are very much general surgical risks – that is pain, swelling, bleeding, infection, bruising as well as the possibility of recurrence of frenal attachment, although in the authors' experience, this has not occurred with a Z-plasty technique. There are limited data in the literature about the recurrence of frenum attachment from the other surgical techniques described; however, in theory, we believe there should be less risk of relapse with the Z-plasty technique due to the transposition of the flaps and the interruption of the direction of the fibres.
A frenum can become a significant issue if tension from lip movement pulls the gingival margin away from the tooth, or if the tissue inhibits the closure of a diastema during orthodontic treatment. While an aberrant frenum can be removed by any of the modification techniques that have been proposed, a functional and an aesthetic outcome can be achieved by a proper technique selection, based on the type of the frenal attachment.
Conclusion
The frenectomy technique using Z-plasty for the removal of the abnormal labial frenum attachment is reliable, easy to perform, and provides excellent aesthetic results for a range of indications.