Unkovskiy A, Wahl E, Zander AT Intraoral scanning to fabricate complete dentures with functional borders: a proof-of-concept case report. BMC Oral Health. 2019; 19 https://doi.org/10.1186/s12903-019-0733-5
Koeppen RG, Mansueto MA Laboratory procedures for framework construction, 4th edn. In: Phoenix RD, Cagna DR, DeFreest CF, Stewart KL (eds). Hanover Park, IL, USA: Quintessence; 2008
Ali SA, Khalifa N, Alhajj MN Communication between dentists and dental technicians during the fabrication of removable partial dentures in Khartoum State, Sudan. Acta Stomatol Croat. 2018; 52:246-253 https://doi.org/10.15644/asc52/3/8
Bhola S, Hellyer PH, Radford DR The importance of communication in the construction of partial dentures. Br Dent J. 2018; 224:853-856 https://doi.org/10.1038/sj.bdj.2018.431
Akl MA, Stendahl CG Removable partial denture frameworks in the age of digital dentistry: a review of the literature. Prosthesis. 2022; 4:184-201 https://doi.org/10.3390/prosthesis4020019
Carr AB, Brown DT Initial placement, adjustment, and servicing of the removable partial denture, 13th edn. St Louis, MO, USA: Elsevier; 2016
Phoenix RD, Cagna DR, DeFreest CF, Stewart KL Delivering the removable partial denture, 13th edn. St Louis, MO, USA: Elsevier; 2016
Carr AB, Brown DT Repairs and additions to removable partial dentures, 13th edn. St Louis, MO, USA: Elsevier; 2016
Dawid MT, Moldovan O, Rudolph H Technical complications of removable partial dentures in the moderately reduced dentition: a systematic review. Dent J (Basel). 2023; 11 https://doi.org/10.3390/dj11020055
Abuhajar E, Ali K, Zulfiqar G Management of chronic atrophic candidiasis (denture stomatitis) – a narrative review. Int J Environ Res Public Health. 2023; 20 https://doi.org/10.3390/ijerph20043029
BDS, MDS (Prosthodontics), Maxillofacial Prosthetics Fellow, Department of Restorative Sciences, School of Dentistry, University of Alabama at Birmingham, USA
BSc (Hons), BDS, FDS RCPS, FCGDent, MRD RCS Ed, MClinDent, FDS RCS(Rest Dent), FDTFEd, FFD RCSI, FHEA, Head of School, Director of Clinical Dentistry, Peninsula Dental School, University of Plymouth
This two-part series provides a comprehensive guide to fabricating definitive metal partial dentures, addressing the challenges dental practitioners face in mastering prosthesis design. It aims to equip dental professionals with a thorough understanding of the theoretical foundations and clinical methods for effective metal partial denture fabrication. Part 2 covers removable partial denture (RPD) design philosophies, tooth preparation, secondary impressions, laboratory procedures, trial and final insertions, as well as post-insertion complications and their management. Additionally, four case scenarios are included to help readers apply the knowledge gained from both parts to design a metal partial denture.
CPD/Clinical Relevance: This series provides essential knowledge and practical techniques for designing and fabricating effective metal partial dentures.
Article
Part 1 of this series explored key elements, including indications, success factors, design principles, surveying techniques, workflow for fabrication and decision algorithms for metal partial dentures. In this part of the series, various philosophies of removable partial denture (RPD) designing, tooth preparation, secondary impressions, laboratory prescriptions, laboratory procedures, trial insertion and final insertion of RPDs are discussed.
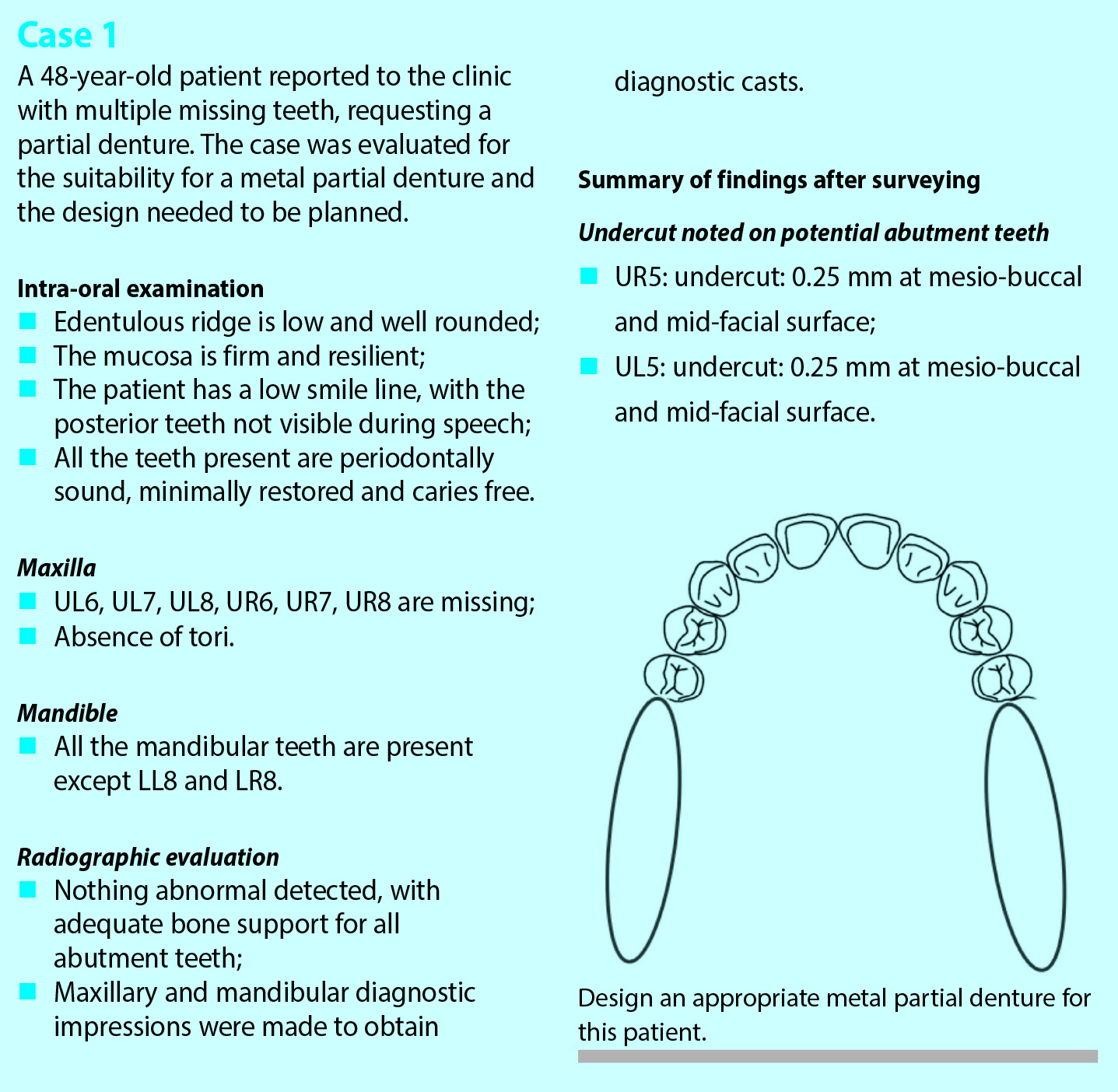
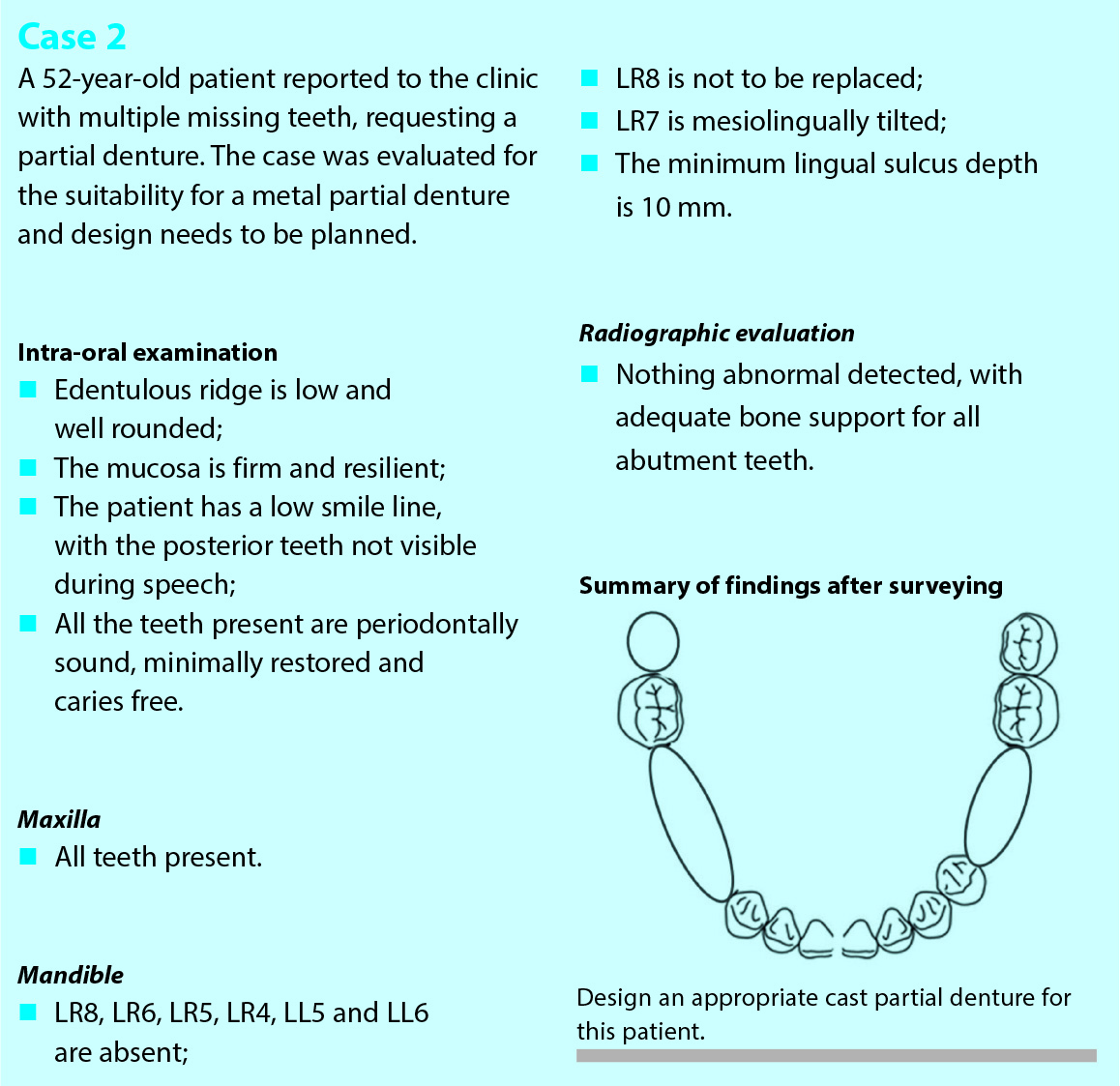
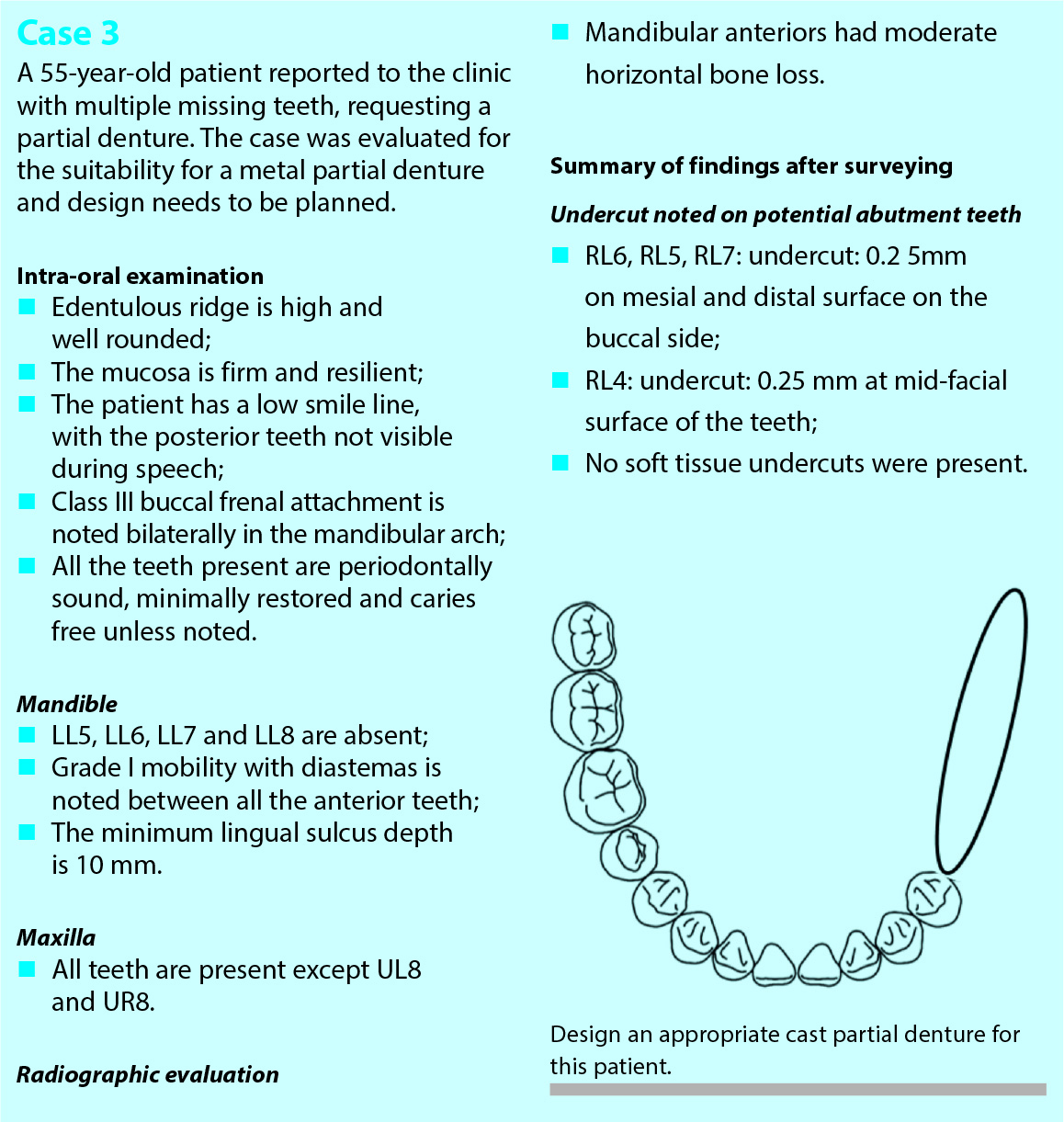
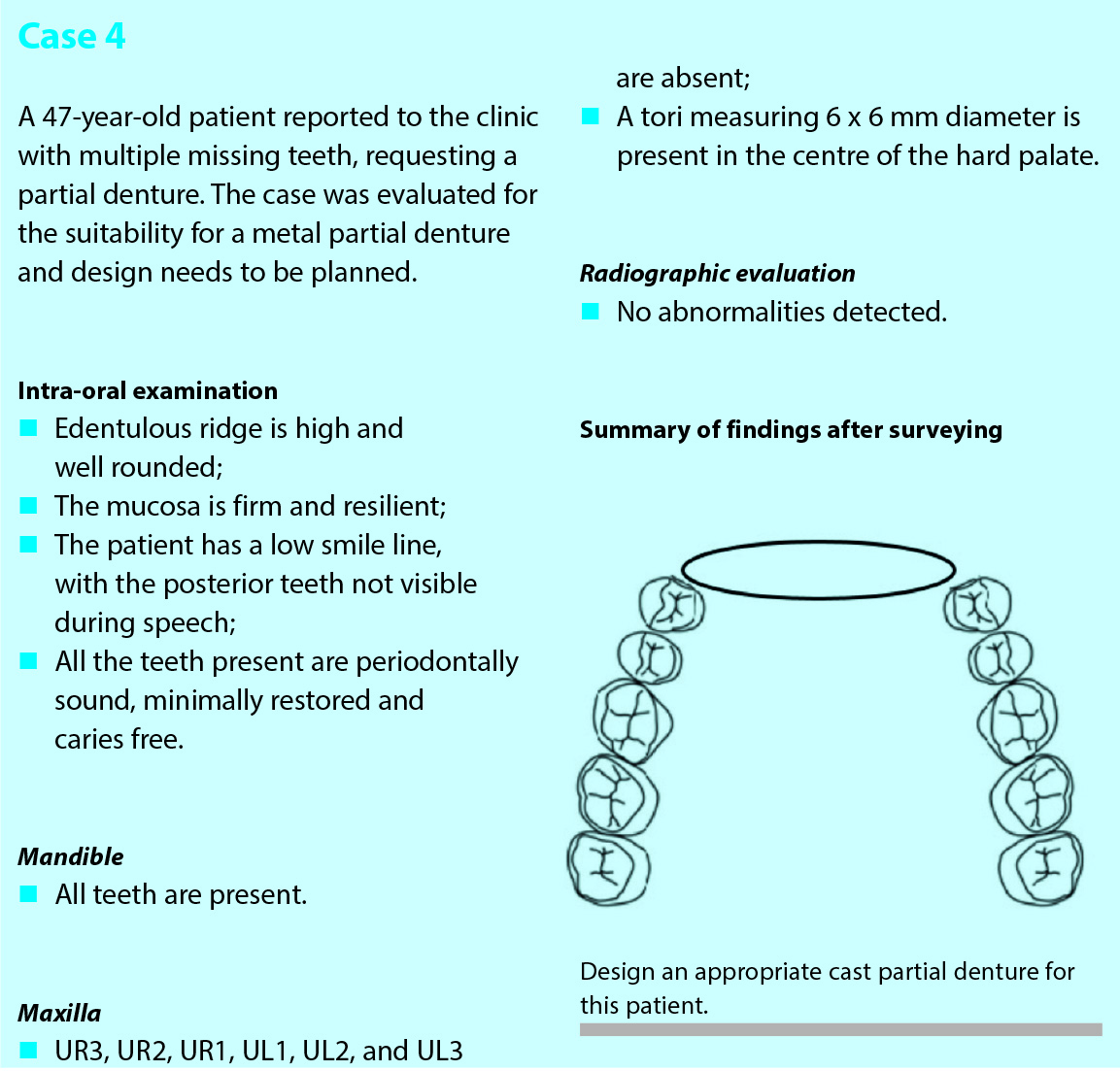
Case studies
The authors have presented hypothetical case scenarios for readers to solve, offering an opportunity to apply and practise the design concepts learned in the two parts of this article series. The four case studies can be found below.
Philosophy of designing RPDs
When designing a tooth tissue-supported prosthesis, there are diverse theories guiding the allocation of support between the edentulous ridge and remaining teeth. These are stress equalization, physiological basing and broad stress distribution.1,2 Stress equalization suggests using the resilient mucosa as a cushion, incorporating stress reducing features to transfer loads from abutment teeth to the edentulous ridge. Physiological basing relies on mucosal resilience, emphasizing equalization using impression techniques to record the anatomy under function. Broad stress distribution aims for rigidity in the partial denture framework, using connectors, rests, clasp assemblies, and coverage to minimize strain on abutment teeth. Combining these philosophies ensures an optimal balance between stability, comfort, and preservation of the oral tissues.1,2
Tooth preparation
Abutment preparations on sound enamel or existing restorations
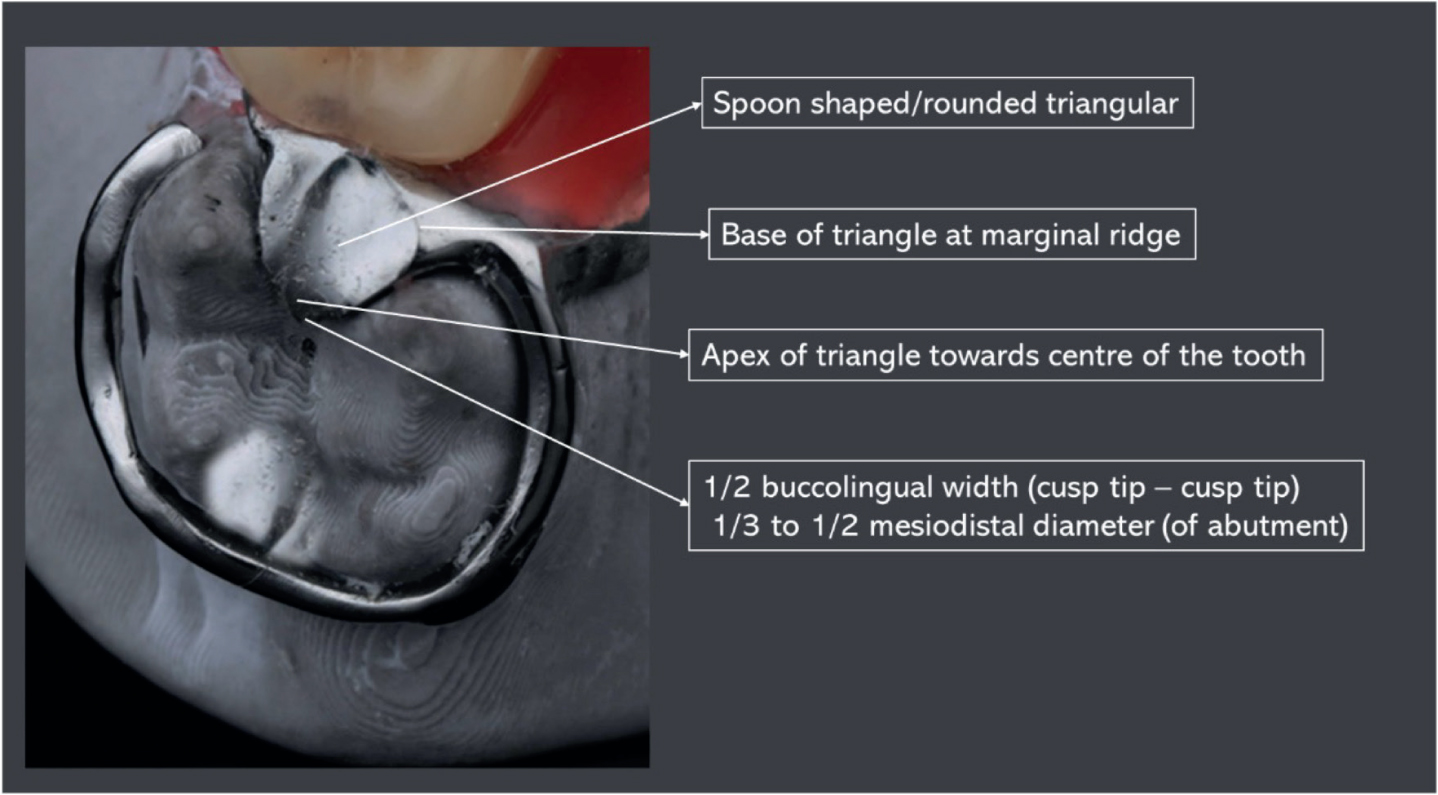
We recommend that tooth preparations in sound teeth do not compromise the integrity of the enamel and due consideration is given to the planned occlusion. The first step in tooth preparation should be to prepare the guide planes on the proximal surfaces of the abutment teeth to limit the path of insertion and withdrawal of the planned prosthesis while simultaneously improving frictional retention.3 It is advisable to verify the adequacy of preparations through a check-cast. Once the guide planes are placed, the rest seats can be prepared over the occlusal and/or cingulum surfaces.3,4 Finally, additional retentive features such as changing the height of contour on abutment teeth either by subtractive or additive techniques may be useful in some cases. Rounding off preparation margins is essential to eliminate sharp edges and unsupported enamel, reducing stress concentration in these areas.3 Ideal preparation features for the occlusal rests are outlined in Figure 1.
Figure 1. Ideal preparation features of an occlusal rest.
Abutment preparations for crowns with denture features (contoured crowns)
Contoured crowns must have suitable space for all planned components of the denture, for example guide planes, rest seats, undercuts, and space for minor connectors.3 Additional preparation of the underlying abutment tooth over the buccal and lingual walls as well as base of the occlusal rest seats must be incorporated.3
Secondary impressions for metal partial dentures
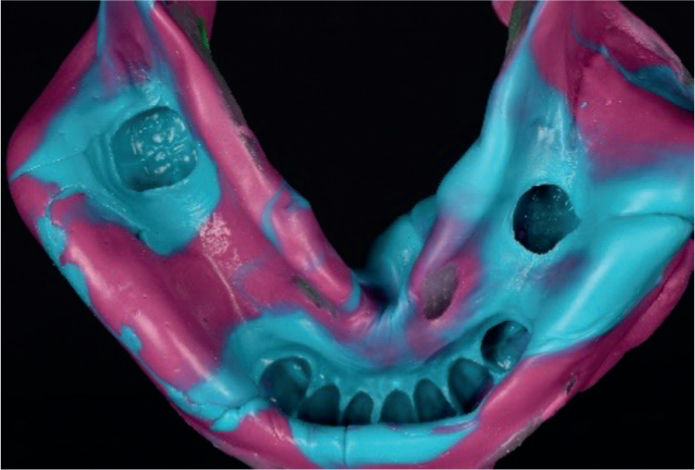
The single-stage impression technique is appropriate for a partial denture that is primarily tooth supported (Figure 2) because resistance to functional loading is provided predominantly by the teeth.5–7 This impression technique leads to a cast that captures the oral structures in their resting position.
Figure 2. Anatomic impression for Class III, modification I situation with optimal recording of the functional depth of sulcus.
This impression technique does not capture the soft tissues under loading conditions which will occur during normal function in the posterior portion of the denture in Kennedy class I and II scenarios. As a result, this may create uneven masticatory load distribution, increasing stress on abutment teeth and the bone beneath the distal extension area, potentially leading to bone loss and tooth mobility.5,6 For this reason, the functional impression technique (altered cast or Applegate technique6) is advocated for Kennedy class I and II situations. This technique aims to enhance denture base support, maintaining occlusal contact and minimizing denture base movement under load.5,6
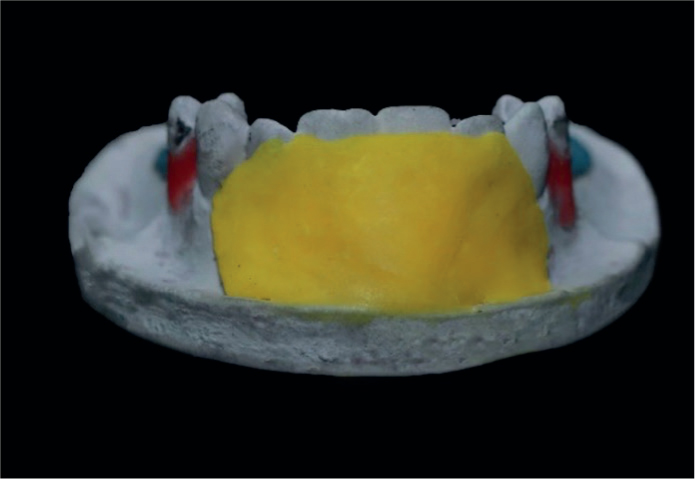
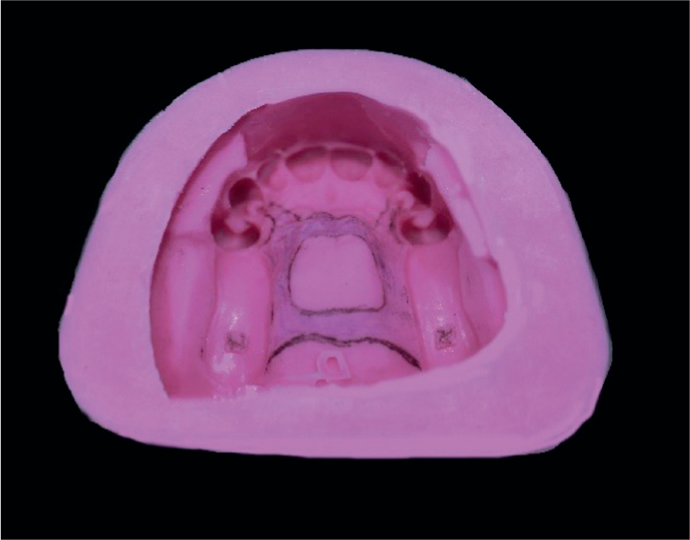
Functional impressions can be achieved through physiological impression techniques (McLean physiologic impression, functional reline method, fluid wax technique) and the selective pressure technique.6 For example, in the functional impression technique, a custom tray is made for the saddle area, and border molding is performed using a low-fusing compound. Subsequently, a functional impression is made using an appropriate secondary impression material that replicates the functional loading of the tissues. The secondary impression is re-inserted into the oral cavity, and an over-impression is made using alginate with a stock tray, capturing the anatomical impression simultaneously. This process is commonly known as the dual impression technique.6
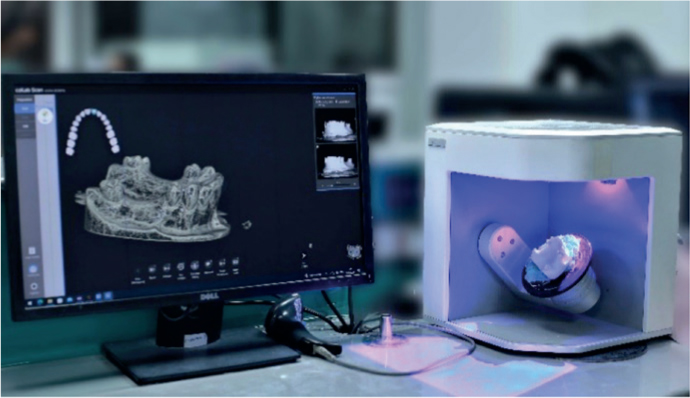
Secondary impressions for the digital workflow involve the use of an intra-oral scanner where the software subsequently combines the scans to generate a comprehensive full-mouth image.8 Intra-oral scanning is suitable for tooth supported cases (Kennedy class III and IV). However, it cannot adequately capture the physiological and functional extension in Kennedy class I and II cases.8,9 Therefore, in such cases, master casts generated using the conventional impression techniques are preferred, and these can then be scanned to generate STL files (Figure 3).
Figure 3. Scanning of master casts.
Dentist–laboratory relations
For achieving optimal outcomes it is crucial for the dentist and dental technician, or clinical dental technician to work cohesively as a team in the construction of removable partial dentures.10–13 The dentist bears the ultimate responsibility for the prescription encompassing the design and materials used in any partial denture fabrication.10
A written prescription (work authorization order) should always accompany any clinical information sent to the dental laboratory to ensure the final prosthesis conforms to the provided instructions. The prescription must effectively convey the positions of all components within the removable partial denture.12 To achieve this, the design of the removable partial denture should be illustrated and explained in detail as part of the prescription. The design diagram can be clarified by employing a color-coded system to distinguish between various components or functions of the RPD. There is no universally accepted colour coding and different countries follow different color schemes. However, the colour scheme must be mutually agreed upon by the dentist and technician to avoid confusion.11–13
The dentist needs to furnish the dental laboratory team with:
A detailed prescription delineating the desired prosthesis;
A meticulously surveyed diagnostic cast with a specific design;
A precisely articulated master cast that faithfully reproduces the existing hard and soft tissue contours.
Framework design and wax patterns
There are two methods of framework fabrication: analogue and digital.
Analogue method
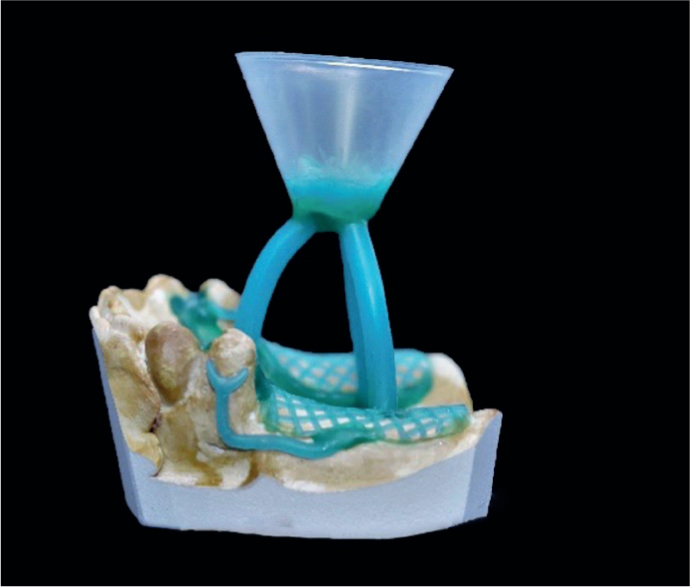
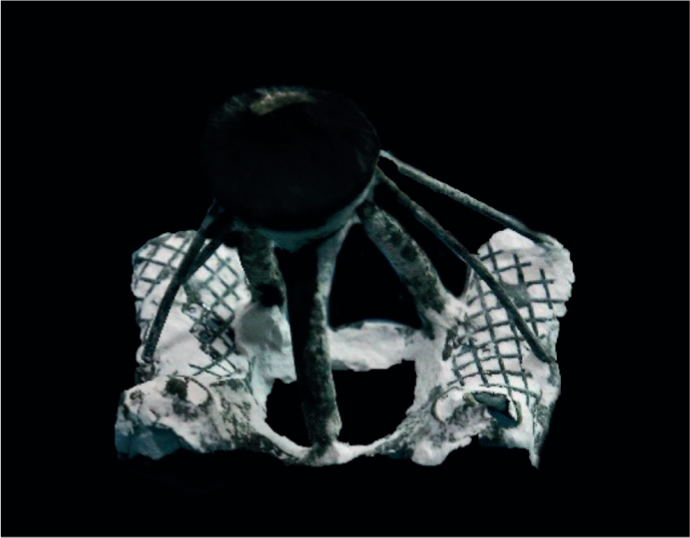
This method involves a conventional wax pattern fabrication, investing, casting and finishing of the framework.10 Before commencing with the construction of the framework, the dental laboratory technician must transfer the specified design from the diagnostic cast to the master cast. This includes transferring tripod points from diagnostic cast to master cast, surveying for marking the height of contour and locating suitable areas for retentive components (Figure 4). It is followed by placing wax to block out undesirable undercuts (Figures 5–7) and relief as required. The master cast is then duplicated in refractory material (Figures 8 and 9) and the framework is waxed-up according to the design on the duplicate cast using prefabricated patterns.
Figure 4. Locating the retentive undercuts.Figure 5. Parallel blockout.Figure 6. Shape blockout.Figure 7. Arbitrary blockout.Figure 8. Mould for cast duplication.Figure 9. Pouring of investment material.Figure 10. Sprue attachment.
The refractory cast is then invested, followed by wax burnout and casting in a chrome cobalt (Figures 10 and 11) or any other suitable alloy. The framework is finally finished and polished.
Figure 11. Casting.
Digital method
Advancements in digital technology, along with the rapid progress in computer-aided manufacturing methods and innovative materials, have opened new possibilities beyond traditional cast removable partial denture frameworks. Additive and subtractive protocols within computer-aided design and manufacturing (CAD/CAM) are being refined to surpass the limitations and inaccuracies associated with casting.14 Simultaneously, different resin-based polymers have emerged in the market to meet the growing need for more aesthetically pleasing clasp assemblies.14
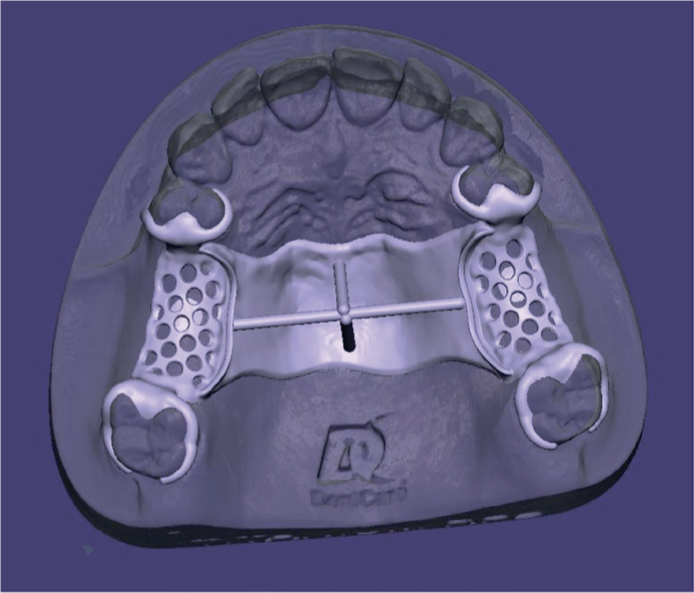
Various materials suitable for digitally fabricating frameworks including cobalt chromium, titanium, polyoxymethylene (acetal resin), polyamides, polyaryletherketone polymers (PAEK), aryl ketone polymers (AKP), and polyetheretherketone (PEEK). Cobalt chromium and titanium can be fabricated through conventional lost-wax methods or using milled/3D printed castable patterns employing techniques such as selective laser sintering (SLS) and selective layer melting (SLM).15 Milled patterns offer the advantages of eliminating the labour-intensive process of creating a refractory cast from the master cast and forming the wax pattern manually. Additionally, the milling process ensures consistent size and thickness based on the software design. Frameworks cast from CAD/CAM milled patterns typically require minimal adjustment, finishing, and polishing (Figures 12–14).14
Figure 12. Addition of spacer.Figure 13. Digital wax-up.Figure 14. Digital framework.
Try-in and insertion
The fitting of the framework involves both pre-clinical inspection and clinical adjustment, ensuring proper adaptation to the hard and soft tissues and conforming with the chosen occlusal scheme.1
Pre-clinical inspection
The clinician must inspect the framework to ensure that it follows the planned design and is accurately adapted to the master cast. If the framework does not fit the master cast accurately, it is highly unlikely that the framework will seat precisely intra-orally. Even the best-looking partial denture framework may not fit perfectly in the mouth and therefore must be adjusted intra-orally. A metal framework try-in appointment should be carried out at the earliest opportunity to minimize the chance of intra-oral changes such as tooth migration. Key evaluation criteria when assessing the fit of the framework on the master cast include checking for proper seating of rests, contact of reciprocal arms and proximal guide plates, intimate contact of major connectors with the cast, adequate distance of major connector from abutment teeth for hygiene purposes, ensuring uniform taper of clasp arms and proper finishing/polishing of the framework.10,15
Clinical adjustment
Inadequate seating of a framework may be due to binding against one or more of the abutment teeth. Identification of these areas can be facilitated by use of indicating media, such as paint on powders (Rouge with chloroform), spray type powders (Occlude), disclosing wax (Kerr), silicone impression materials or indicating medium (e.g. Fit Checker).15,16 Following identification of these areas, adjustment can be made with heatless stones, diamond burs, Brasseler E-Cutter burs, carborundum disks and coarse stones.
Only once the framework is seated completely can any occlusal interferences be evaluated. The most common location for occlusal interferences are the rests, indirect retainers and minor connectors. It is important to remember that the majority of cases will be restored in an occlusally conformative approach and as such the vertical dimension should remain unchanged by the framework and the interarch tooth contacts should be identical with and without the framework in the mouth. Following adjustment, any roughened surfaces should be smoothed and brought to a high polish. Knife-edge wheels, blue clasp polishers or other carborundum-impregnated points for chrome cobalt alloys may be used to remove scratches and bring the adjusted surface to a high shine quickly. For final polishing, tripoli placed on a bristle brush and rouge on a small diameter cloth wheel may be used.10
After adjusting the partial denture framework, it is essential to record the maxillomandibular relationship, and transfer this on to the articulator for facilitating setting of replacement denture teeth on the framework The teeth try-in is then done to assess aesthetics, speech, and functionality. Following try-in, final processing is done in the laboratory. The finished partial denture is delivered to the patient with necessary adjustments carried out on the day of placement and during the post-placement recall appointments.
Post-insertion complications and management of common issues
Complications associated with a new partial denture can be categorized into immediate, intermediate, and delayed for ease of comprehension. In the following section we have outlined some of the potential issues.
Immediate complications
Immediate complications arise during the insertion of the prosthesis and are commonly related to fit, peripheral extension, and the occlusion. Pressure indication paste, applied to the prosthesis's intaglio surface with a brush stroke pattern, helps identify pressure points for necessary adjustments, preventing future sore spots.15 Disclosing wax can reveal overextension in peripheral borders, with caution exercised to reduce it only if exceeding physiological limits. Adjustments of the denture occlusion should only commence after the prosthesis is fully seated in the patient's mouth, to generate harmonious contact in centric and eccentric positions and with natural teeth.15,16
Intermediate complications
Intermediate complications commonly involve component fractures. Patient mishandling often causes fractures, necessitating patient education on proper prosthesis care and usage. Fractured retentive clasp arms may result from improper design, and replacement with a wrought wire clasp can be achieved through soldering or embedding it into the framework.17 Fractured occlusal rests can be repaired by soldering a new rest, with consideration for rest seat modification if insufficiently prepared. Significant complications such as fracture of the major connector may require remaking the prosthesis.17
Delayed complications
Delayed complications may stem from physiological or pathological changes in the oral cavity or from changes to the metal partial denture through use leading to damage or wear of components.
In distal extension prosthesis cases, loss of retention may occur due to residual ridge resorption, necessitating prosthesis relining.18 Loss of natural teeth can be addressed by adding retentive tags on the major connector, but if an abutment is lost, the adjacent tooth's suitability must be evaluated for potential use as an abutment, incorporating necessary modifications into the existing denture or may require new prosthesis fabrication.17
Improper oral and denture hygiene maintenance and poor dietary control in certain patients may lead to problems such as the development of caries, periodontal disease and oral candidiasis. To mitigate these risks, it is important that every patient's treatment plan is personalized, addressing their specific risk factors for caries, periodontal and other oral disease processes through diet analysis and advice, a tailored oral hygiene and fluoride regime as well as specific medicaments to address other pathology such as antifungal treatments for oral candidiasis as necessary.19
Once the initial active phase of treatment has been completed it is equally important that a maintenance and monitoring plan is instigated with periodic recalls based upon the patient risk factors for ongoing support and treatment as required.
Conclusion
The field of removable partial prosthodontics stands at the intersection of mechanical and biological factors, requiring a meticulous blend of scientific understanding and clinical expertise. A thorough understanding of all the design principles along with meticulous examination, diagnosis, and treatment planning, plays a pivotal role in the success of removable partial denture. Above all, it is the utmost responsibility of the dentist to communicate effectively with the laboratory. The laboratory steps in the fabrication of metal partial dentures are just as crucial as the clinical procedures.
The unavailability of a single best design highlights the complexity of the decision-making process, with multiple acceptable designs often emerging for a given partially edentulous arch. Digital technology is being increasingly embraced in the field of prosthodontics as it has the potential to improve patient outcomes and reduce human operator error.