References
Management of the extraction socket and alveolar ridge preservation
From Volume 46, Issue 2, February 2019 | Pages 151-156
Article

Extraction socket healing
Dental practitioners will be aware that, following extraction, the alveolar ridge undergoes significant changes. The biological processes and dimensional changes that occur have been well studied. These changes have an impact on the prosthodontic replacement of teeth and this has taken on increased importance with the increasing prevalence of dental implants. The morphology of the remaining alveolar ridge has a significant impact on implant treatment complexity and outcomes. An intact ridge can lead to low risk implant placement with the expectation of excellent aesthetic and functional outcomes, whereas severe atrophy of the ridge is associated with increased risk, particularly where vertical augmentation is required, as well as associated surgical morbidity, and potential for aesthetic compromise. The ITI group have developed an assessment system which includes general, systemic and local factors and their effects on treatment, including the deficient ridge (www.iti.org/SAC-Assessment-Tool). Significant soft and hard tissue augmentation immediately raises the overall treatment level to complex.
There has been a shift from the presence and satisfactory appearance of the prosthodontic tooth being accepted as a successful outcome of implant treatment, towards a greater demand for the peri-implant mucosa to harmonize with the remaining dentition. The most critical area to ensure ideal peri-implant tissue morphology is the anterior maxilla, particularly in those with level to high smile lines. ‘Pink aesthetics’ are crucial in these cases in order to obtain a natural appearance, recreating the morphology of the gingival tissues and alveolar ridge in the vicinity of the restoration. A ‘pink aesthetics’ score has been devised in order to assess outcomes for implant treatment objectively.1
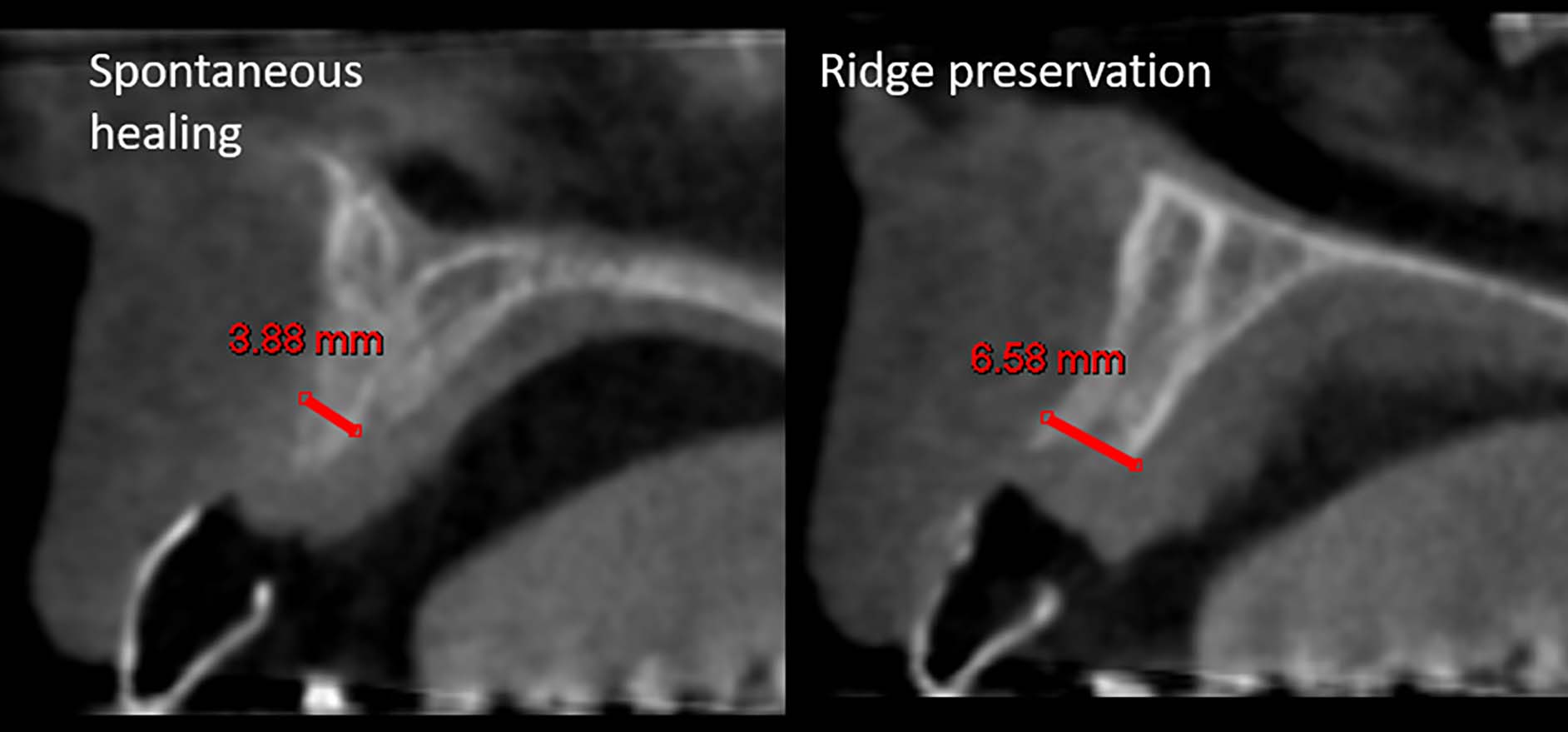
Misawa et al studied the changes in the alveolar process in maxillary incisors and premolars over 12 months using CBCT.2 This study determined changes in ridge width (hard tissue) at 3 points: 3 mm, 5 mm and 7 mm apical of the CEJ of the extracted tooth. The average reduction in width for all teeth in this study at 3 mm level was 62%. The remaining ridge width at this level was just 3.2 mm on average (Figure 1). These findings are in keeping with the observations which most clinicians will be familiar with following extraction. Ridge width reduction is particularly prominent, with the majority of the reduction occurring from changes on the labial/buccal aspect. Historically, implants were placed according to the availability of bone which often resulted in implants being placed in sub-optimal positions, particularly with regards to creating a natural emergence profile and peri-implant mucosa. This residual ridge morphology may impact on the possibility of placing the implant successfully with primary stability and in the ideal prosthodontic position. A staged grafting procedure may be introduced with the associated morbidity for patients, as well as increasing treatment time and level of invasiveness (Figure 2).


A recent systematic review of post extraction soft and hard tissue changes revealed, after examining 20 studies, a mean width reduction of hard tissue of 3.79 mm.3 This included a variety of sites throughout the maxilla and mandible. A percentage reduction in vertical ridge height was stated as 11%−22% and width as 29%−63% after 6 months. The study stated also that rapid reductions are seen in the first 3−6 months.
The progression of changes occurring within the alveolar ridge has been documented in an elegant human study by Schropp et al.4 In this study, ridge width measurements were taken at regular timepoints over a 12-month period. It concluded, in agreement with an earlier study,5 that two thirds of the ridge atrophy has occurred within the first 3 months.
Alveolar ridge preservation: history
Strategies for preserving the alveolar ridge have utilized a variety of materials, from artificial alloplastic materials, allogenic human derived grafts and animal xenografts. Membranes have been used, both resorbable and non-resorbable, as well as autogenous soft tissue grafts to enhance to gingival phenotype around the future restoration.
Initial attempts to maintain the alveolar ridge were focused on root retention, in order to maximize the stability of removable prostheses. The principle of socket preservation began in the 1980s, where the theory was based on material placed in the socket taking the ‘role’ of a root and maintaining ridge dimension.6 This effect would ideally allow osseointegrated dental implant placement with minimal additional surgical procedures.
Systematic reviews on alveolar ridge preservation
There have been a plethora of systematic reviews (SRs) on this topic. At least 14 have been produced over the past 8 years.
There has also been a ‘systematic review’ of the available systematic reviews.7 This used two quality assessments.8, 9 At the time of the publication, there were 12 suitable reviews assessed and the methodological and structural variations present between reviews were highlighted by the authors.
There is significant heterogeneity amongst the approach used by the systematic reviews. A large proportion have grouped different materials, for example alloplastics with xenografts, with vastly different performances, thereby diluting possible effects of very different materials in one overall analysis.
It may be simpler to judge the literature on this topic by reviewing the handful of high quality randomized controlled trials (RCTs) which commonly recur in many of these SRs, particularly when grouping specific materials and techniques together, thereby helping to identify true performance of specific treatment types for this topic: for example guided bone regeneration (GBR) with xenograft and resorbable membrane.
Having reviewed the multiple SRs, it was possible to isolate those papers which used GBR techniques with xenografts and crucially had a direct control group (unassisted healing).
Guided bone regeneration (GBR): xenograft versus controls
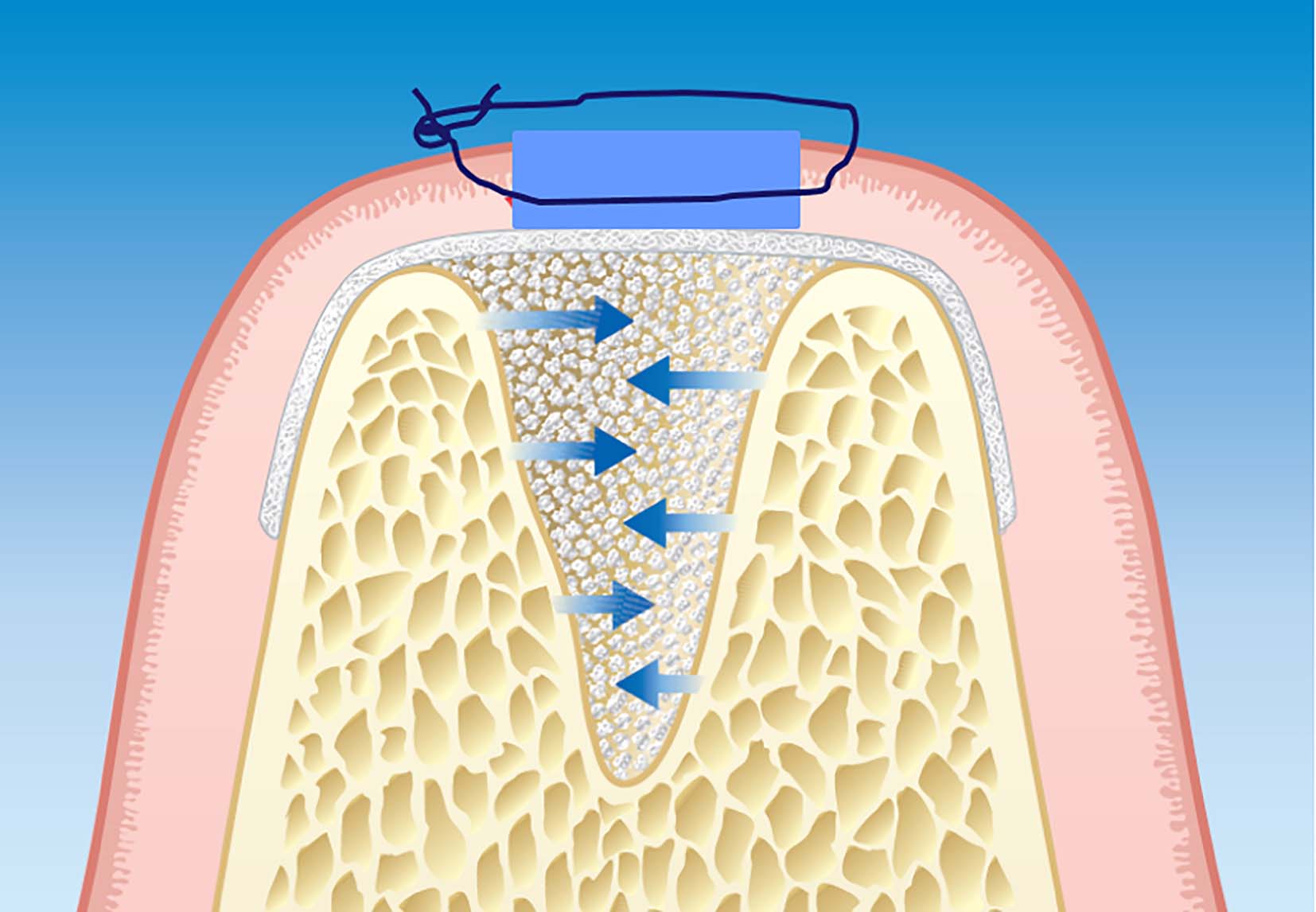
The most commonly used technique and material demonstrated in the literature used xenograft material to fill extraction socket with resorbable collagen membranes. The unrestorable tooth is extracted using suitable atraumatic instruments (eg periotomes) to preserve all alveolar bone possible. The socket space is filled with, in this instance, xenograft (eg bovine bone material) (not compressed) while a collagen membrane is ‘tucked’ under the soft tissue both buccally and lingually to prevent soft tissue ingress and maintain the stability of the clot/bone graft (Figure 3).
This technique can be performed without raising a full thickness flap, however, if there is uncertainty about the remaining buccal ‘bundle’ bone, a flap for visualization may aid more complex regenerative procedures.
Secondary intention healing with a ‘bioactive’ membrane, such as Bio-Gide® (Geistlich Pharma North America Inc), allows epithelial tissue to proliferate within and across the membrane leaving minimal complications. This reflects the relative success of GBR procedures using these materials, despite wound dehiscence. This is unlike non-resorbable membranes, eg polytetrafluoroethylene (PTFE), which may be ‘marsupialised’ by epithelium trying to exclude the ‘foreign’ material and may become contaminated and lead to infections.
This is comfortably the most commonly studied technique with multiple research studies including RCTs. There is a consistently demonstrated clinical benefit, for example, for hard tissue width. Avila-Ortiz et al have undertaken a meta-analysis of xenograft alone; the result of the meta-analysis concluded an average benefit above control-unassisted healing of 2.41 mm of ridge width.6
Barone et al have undertaken 3 RCTs in assessing this technique.10, 11, 12 These studies demonstrated 2−2.7 mm ridge width preservation, and 1.1−2.5 mm ridge height preservation, when compared to control sites, between 3 and 7 months after the healing period.
Furthermore, Cardaropoli et al used bovine bone mineral and a collagen membrane to preserve extraction sockets, when compared with control sockets in a RCT.13 A highly significant difference was noted between groups with a test group displaying 3.44 mm greater ridge width and 1.08 mm greater height. This study was undertaken on molars and premolars, possibly explaining the large values due to larger scale ridge dimensions.
Festa et al demonstrated significant benefits using a porcine xenograft along with a ‘soft cortical membrane’ in a split mouth study of contralateral premolars.14 The gain in dimension after ARP techniques were 1.9 mm for ridge width and 2.5 mm mid-buccal ridge height.
Some alloplastic materials have been demonstrated to provide successful ridge preservation15 and, as the development and refinement of these materials progresses, they may take over as the primary material, not only for preservation, but ridge augmentation GBR and periodontal guided tissue regeneration (GTR) procedures. As our understanding of biomaterials and growth factors involved in bone formation increases, the development of synthetic materials to aid this process can be expected in the future.
Socket seal
Recently, the concept of ‘socket seal’ has come into favour. This may involve the use of an autogenous free gingival graft (FGG) or a xenograft soft tissue ‘matrix’ being used to close the socket entrance. This may benefit the healing situation by achieving ‘primary’ closure, as well as increasing the quantity of keratinized tissue in the site. The overall procedure is similar to GBR, but rather than cover the socket with a membrane, an autogenous FGG is carefully sutured over the socket entrance, after de-epithelializing the tissue around the margin to ensure improved blood supply to the free graft.
Jung et al studied four groups, including control with unassisted healing.16 The test groups included a xenograft socket filled with a collagen matrix and a xenograft with an autogenous FGG and a beta tricalcium phosphate (β TCP) alloplastic material. This particular alloplastic material (β TCP) performed worse than the unassisted healing group, causing greater ridge atrophy. However, the xenograft materials again showed promising results compared to control healing, both when ‘sealed’ with collagen matrix (width 2.1 mm, height 0.5 mm) and when sealed with FGG (width 1.9 mm, height 1.7 mm).
The majority of studies on this topic look at dimensional changes in mm, however, a recent study by Araujo et al examined dimensional alterations in terms of percentage reduction of cross-sectional area.17 This study utilized a ‘socket seal’ approach: with a bovine xenograft socket filler material with an autogenous graft to seal the socket. Just 4 months following extraction, the control unassisted healing sites demonstrated a 25% reduction in the overall cross-sectional ridge area. The test socket seal and grafted sites showed only 3% reduction. These findings would suggest that this treatment counteracts a significant reduction in the hard tissue component of the edentulous ridge
Meloni et al directly compared the clinical performance and outcome of a socket seal procedure, using a bovine xenograft, providing a socket seal using an autogenous free gingival graft versus a xenograft soft tissue matrix.18 This study demonstrated the equal performance of the two groups, suggesting a benefit using the xenograft matrix in order to avoid a donor site, albeit demonstrating the success of both techniques in limiting ridge dimensional reduction.
The clinical decision is, of course, informed by the likely efficacy of the procedure and the successful outcome, however, other important factors, such as minimizing the level of invasiveness of the procedure, and cost, must also be factored into the most suitable approach.
Timing of implant placement with ARP
A negative implication to a GBR approach to socket preservation has been postulated as the increased time intervention required prior to placing an implant, compared to popular techniques such as immediate placement, or ‘early’ (6−8 weeks) placement. Traditionally, GBR techniques are allowed to heal for 6−9 months prior to any implant intervention.19 However, an extraction socket is a completely different defect morphology compared with, for example, horizontal augmentation of a knife-edge (Cawood Howell Class IV) edentulous ridge. The favourable ‘4-walled’ socket will heal with osteoblast and blood supply from 360° and the defect will ossify in a much shorter time. Cardaropoli et al demonstrated in a detailed, histologic, chronological study of the healing socket in animal studies, that just 30 days following an extraction, 88% of the socket volume was occupied by mineralized bone.20
Taking all this into account, an interesting recent in vivo study by Thoma et al looked at the significance of early implant placement into sites which had ridge preservation (GBR with xenograft/collagen membrane) at 4 weeks.21 The sites were compared with early implant placement unassisted healing. The study showed successful osseointegration and healing histologically of early implant placement 4 weeks following socket preservation. This is a pilot in vivo study, which needs to be corroborated clinically, but suggests promise in the principle of early fixture placement in sites having undergone ARP. Benefits gained may include reducing the need for GBR procedures, leading to more predictable minimally invasive surgery for patients due to a well-preserved alveolar ridge.
Implant-related outcomes
A systematic review by Mardas et al studied the outcome measures of ARP sites versus control on implant feasibility, need for further augmentation, survival rates and implant marginal bone levels.22 clinical benefits of ARP versus unassisted healing is limited and that further high quality RCTs are required to compare unassisted healing and socket preservation effects on implant outcome measures specifically. The study does suggest, from the available research, that the likelihood of further augmentation is significantly reduced, with ARP sites 6.7 times less likely to require augmentation compared with unassisted sites.
Conclusion
The field of research regarding extraction socket healing and socket preservation has a significant body of data, when compared to many others in dentistry. Clarity and consensus appears to have been achieved in the acceptance of the significant changes which occur to ridge dimension, with the majority of dimensional changes occurring within 3 months.
Techniques and materials for socket preservation have varied hugely from simple socket fill, to GBR, to socket seal, with materials ranging from different ‘man-made’ alloplastics, to xenografts, to allogenic materials. When looking purely, as this literature review has, at xenograft GBR techniques, the data shows a clear dimensional benefit in terms of particularly preserving ridge width (Figure 4). Extrapolating this data to improving implant outcomes and treatment has not been clearly demonstrated, although early data suggests that ARP can minimize the need for GBR techniques in addition to implant surgery, thereby improving the predictability of treatment and importantly minimizing discomfort and surgical interventions for our patients.