Raghoebar GM, Meijer HJ, van't Hof M, Stegenga B, Vissink A A randomized prospective clinical trial on the effectiveness of three treatment modalities for patients with lower denture problems. A 10 year follow-up study on patient satisfaction. Int J Oral Maxillofac Surg. 2003; 32:498-503
Critchlow SB, Ellis JS Prognostic indicators for conventional complete denture therapy: a review of the literature. J Dent. 2010; 38:2-9
Critchlow SB, Ellis JS, Field JC Reducing the risk of failure in complete denture patients. Dent Update. 2012; 39:427-436
Thomason JM, Feine J, Exley C, Moynihan P, Müller F, Naert I Mandibular two implant-supported overdentures as the first choice standard of care for edentulous patients – the York Consensus Statement. Br Dent J. 2009; 207:185-186
van Waas MA The influence of clinical variables on patients' satisfaction with complete dentures. J Prosthet Dent. 1990; 63:307-310
Field J The best of YDC 2011 – Communication; removable prosthodontics. Riskmatters. 2011; 21:7-8
Massad JJ, Cagna DR Vinyl polysiloxane impression material in removable prosthodontics. Part 1: edentulous impressions. Compend Contin Educ Dent (Jamesburg, NJ, 1995). 2007; 28:452-459
McCord JF, Grant AA Registration: stage I – creating and outlining the form of the upper denture. Br Dent J. 2000; 188:529-536
McCord JF, Grant AA Registration: stage II – intermaxillary relations. Br Dent J. 2000; 188:601-606
Porwal A, Sasaki K Current status of the neutral zone: a literature review. J Prosthet Dent. 2013; 109:129-134
McCord JF, Firestone HJ, Grant AA Phonetic determinants of tooth placement in complete dentures. Quintessence Int. 1994; 25:(5)341-345
McGee GF Tooth placement and base contour in denture construction. J Prosthet Dent. 1960; 10:(4)651-657
Friedman S Principles of setups in complete dentures. J Prosthet Dent. 1969; 22:111-130
Srivastava V, Gupta N, Tandan A, Kaira LS, Chopra D The neutral zone: concept and technique. J Orofacial Res. 2012; 2:42-47
Pound E, Murrell GA An introduction to denture simplification. Phase II. J Prosthet Dent. 1973; 29:598-607
Pound E Esthetic dentures and their phonetic values. J Prosthet Dent. 1951; 1:98-111
Lammie G Aging changes and the complete lower denture. J Prosthet Dent. 1956; 6:450-464
McCord JF, Grant AA Registration: stage III – selection of teeth. Br Dent J. 2000; 188:660-666
Sutton AF, McCord JF A randomized clinical trial comparing anatomic, lingualized, and zero-degree posterior occlusal forms for complete dentures. J Prosthet Dent. 2007; 97:292-298
Kimoto S, Gunji A, Yamakawa A, Ajiro H, Kanno K, Shinomiya M Prospective clinical trial comparing lingualized occlusion to bilateral balanced occlusion in complete dentures: a pilot study. Int J Prosthodont. 2006; 19:103-109
Sutton AF, Glenny AM, McCord JF Interventions for replacing missing teeth: denture chewing surface designs in edentulous people. Cochrane Database Syst Rev. 2005; (1)
Pietrokovski J, Starinsky R, Arensburg B, Kaffe I Morphologic characteristics of bony edentulous jaws. J Prosthodont. 2007; 16:141-147
The glossary of prosthodontic terms. J Prosthet Dent. 2005; 94:10-92
Gahan MJ, Walmsley AD The neutral zone impression revisited. Br Dent J. 2005; 198:(5)269-272
Beresin VE, Schiesser FJ The neutral zone in complete dentures. J Prosthet Dent. 1976; 36:356-367
Fahmy FM, Kharat DU A study of the importance of the neutral zone in complete dentures. J Prosthet Dent. 1990; 64:459-462
Barrenas L, Odman P Myodynamic and conventional construction of complete dentures: a comparative study of comfort and function. J Oral Rehabil. 1989; 16:457-465
Raja H, Saleem M Neutral zone dentures vs. conventional dentures in diverse edentulous periods. Biomedica. 2009; 25:136-145
Makzoume JE Complete denture prosthodontics for a patient with Parkinson's disease using the neutral zone concept: a clinical report. Gen Dent. 2008; 56:e12-16
Rehmann P, Zenginel M, Wostmann B Alternative procedure to improve the stability of mandibular complete dentures: a modified neutral zone technique. Int J Prosthodont. 2012; 25:506-508
Ohkubo C, Hanatani S, Hosoi T, Mizuno Y Neutral zone approach for denture fabrication for a partial glossectomy patient: a clinical report. J Prosthet Dent. 2000; 84:390-393
Wee AG, Cwynar RB, Cheng AC Utilization of the neutral zone technique for a maxillofacial patient. J Prosthodont. 2000; 9:2-7
Cagna DR, Massad JJ, Schiesser FJ The neutral zone revisited: from historical concepts to modern application. J Prosthet Dent. 2009; 101:405-412
Jum'ah A, Nixon P Neutral zone in complete dentures: systematic analysis of evidence and technique. Smile Dent J. 2011; 6:8-12
Lynch CD, Allen PF Overcoming the unstable mandibular complete denture: the neutral zone impression technique. Dent Update. 2006; 33:21-26
Porwal A, Jain P, Biradar SP, Nelogi S, Naveen H Neutral zone approach for rehabilitation of severely atrophic ridge. Int J Dent Clinics. 2010; 2:53-57
Chandra SS Management of a severely resorbed mandibular ridge with the neutral zone technique. Contemp Clin Dent. 2010; 1:36-39
Managing the unstable mandibular complete denture – tooth placement and the polished surface Peter Clarke A Johanna Leven Callum C Youngson Dental Update 2025 43:7, 660-670.
Authors
PeterClarke
DCT in Restorative Dentistry, Liverpool University School of Dentistry, Pembroke Place, Liverpool L3 5PS, UK (pete.t.clarke@gmail.com)
Constructing satisfactory conventional mandibular complete dentures is often challenging in comparison to the upper counterpart partially due to differences in the anatomy of the denture-bearing area. This problem is exaggerated in the atrophic mandible, where supporting structures are frequently ill-defined and suboptimal in quality. Implant-retained prostheses offer well recognized benefits but are not always a feasible options, so conventional methods must be relied upon. The importance of impression quality and registration has been reviewed previously. This article aims to discuss the influence of tooth placement, the polished surfaces and the neutral zone on the success of lower dentures.
CPD/Clinical Relevance: This article highlights the importance that polished surface contouring and tooth prescription can have on the outcome of lower dentures. Techniques for assessing and recording the neutral zone are explained, along with alternative occlusal schemes.
Article
Almost every practising dentist will be aware of the problems and challenges that arise when trying to provide a mandibular complete denture successfully. In comparison to the upper arch, the anatomy is less favourable and the patient may have previously had a satisfactory upper denture paired with a number of unsuccessful lower counterparts. This is an all too common scenario and most of the emphasis of previous articles relates to the importance of impression techniques and jaw registration. This paper aims to discuss some of the elements surrounding the polished and occlusal surfaces when managing the less stable mandibular complete denture.
In 2009, it was recorded that 6% of the English population wore complete dentures1 and it has been estimated that a third have difficulty wearing mandibular dentures satisfactorily.2 This equates to approximately one million patients. In a number of these cases, the lower denture-bearing area is grossly resorbed with little height or width from which to gain stability or retention. Managing these patients can often be extremely difficult and the outcome is not always favourable. The literature surrounding the prognostic indicators of mandibular complete denture success has been reviewed in detail elsewhere, along with options and clinical tips to help overcome these issues.3,4
Much of the modern literature focuses on implant-related therapies. As the predictability of implants has improved greatly (and with accumulating amounts of associated evidence), the use of a two-implant retained mandibular overdenture has been deemed the treatment of choice for the unstable lower complete denture.5 Unfortunately, in some circumstances this is not always feasible and conventional methods must be relied upon. Table 1 outlines a number of potential inhibitory factors to implant use.
Potential Inhibitory Factors to Implant Therapy in the Edentulous Patient
Patient unwilling to undergo surgical procedures/long-term maintenance
When faced with an unstable mandibular complete denture it is important to look at the factors that can be modified and those elements that cannot. These can be broken down into those which are clinically-based and those which are patient-based. From a patient perspective, there will always be a number of patients who cannot or will not adapt to their new denture (which has been noted to be greater in the mandibular complete denture3). The patient's ability to adapt to wearing dentures is one of the overriding factors in patient satisfaction; if he/she is unable to do so, it will inevitably fail.6 Therefore, it is important to try to modify the patient's expectations, prior to construction of the denture, in an attempt to improve the patient's acceptance. Ultimately, the clinician should aim to educate the patient on: the potential difficulties, treatment options, possible lifestyle modifications and likely outcome of the presenting scenario.7
From a clinical viewpoint, the technical aspects that are going to affect the success of the mandibular denture are essentially: the impression, the registration, the prescription and placement of the teeth and polished surfaces. Optimizing these elements will give the patient the best opportunity to learn to adapt to the new prosthesis. Both the impression taking and registration stages have been reviewed recently, but the prescription of tooth placement and consideration of the ‘neutral zone’ (or ‘zone of reciprocal force’) has not received the same attention. This article will address in more detail the prescription of teeth and polished surfaces.
Impression taking and registration
Accurate impression taking and jaw registration undoubtedly contribute to provision of any successful denture and even more so when the anatomy is unfavourable. In these difficult stages, if greater attention to detail is not given, then inaccuracies that will affect the overall retention and stability are likely to be introduced. Table 2 serves to provide a brief summary of the important factors in both impression taking and jaw registration as a supplement to the main focus of the article. Further information and clinical tips can be found elsewhere.4,8,9,10
Impression Taking
Complete coverage of the denture-bearing area (especially extending to retromolar pad and into distolingual sulcus)
Ensures maximum stability and retention. The retromolar pad demonstrates less resorption than the alveolar bone over time and therefore may provide an area of increased sulcus depth. Good distolingual extension in this region provides anchorage to resist lateral displacement.
Correct flange extensions
A well-adjusted and border moulded special tray will ensure optimum retention and stability. Adequately recording muscular attachments and mucosal movement will prevent over extension and provide the correct contour of flange to the functional sulcus, to optimize the peripheral seal.
Jaw Registration
Adequate freeway space
Without sufficient freeway space the patient may suffer discomfort, unusual occlusal interferences and lack the ability to function well with the dentures.
Even bilateral contact on record rims during registration process, whilst fitting surface seated properly
Helps record an accurate relationship of the mandible to the maxilla, allowing for accurate set up of denture occlusion with inclusion of fewer occlusal errors.
No excessive wax that will interfere with the surrounding soft tissues
This ensures the jaw relationship is recorded accurately and contouring of the polished surfaces prevents interferences with surrounding soft tissues during function that may lead to instability.
Passive registration process recorded on the terminal hinge axis (RCP)
Allows set up of occlusion in a reproducible and comfortable position for the patient, improving habituation to the new prosthesis.
Prescription of the teeth and polished surfaces
Incorrect positioning of the teeth and polished surfaces can lead to a number of problems, including poor phonetics and facial profile, as well as denture instability.11 Upper dentures generally allow for greater freedom in placement of teeth as the baseplate and underlying ridge are usually larger, thus being able to resist higher displacing forces. In contrast, positioning in the lower arch is more restricted, as the presence of the tongue narrows the neutral zone and a reduced denture-bearing area limits resistance to displacing forces. This statement is more relevant in atrophic mandibles as a reduced ridge height decreases resistance to lateral forces. Furthermore, a wide hypotonic tongue (commonly seen following prolonged periods of edentulousness) further reduces the width of the neutral zone, increasing the risk of muscular interference. Various recommendations for tooth placement and occlusal schemes have been advocated in the past which will now be discussed further.
Placement of teeth
Conventional biometric practice advocates placing the maxillary anterior teeth labial to the ridge to compensate for the inward pattern of maxillary bone resorption. Classically, the incisive papilla is used as a reference point and the labial aspect of the central incisors placed 8–10 mm anterior of the papilla.12 Maxillary posterior teeth should be set forward of the anterior aspect of the tuberosities.13 Teeth are set buccal to the ridge, ensuring that the palatal cusps contact the central fossae of the lower molars and transmit occlusal forces on to the crest of mandibular ridge.9 Full palatal coverage and the typically larger volume of residual ridge in the maxilla allows for greater freedom in tooth positioning without leading to instability.
In contrast, less freedom exists in the lower arch, particularly with atrophic mandibles. The frequently lower quality and reduced size of the residual ridge provides little resistance to both lateral and tipping forces produced during mastication. Various concepts and suggestions regarding tooth positioning have been proposed in order to increase stability. Commonly, it is suggested that the posterior teeth are placed perpendicular over the crest of the residual ridge in order to gain direct opposition to compression from the supporting tissues.14,15,16 Pound suggested placing the lingual surfaces of the lower molars within a triangle formed between the mesial of the canine anteriorly and the most lingual and buccal points of the retromolar pad distally (Figure 1). The proposal being that stability is aided and the natural relationship of the teeth to the tongue and retromolar pad is maintained.17 Other variations do not lie much outside this zone, some suggesting a lingual position, whilst others suggest a lateral position over the buccal shelf to compensate for the pattern of mandibular bone resorption and provide greater tongue space.16,18,19 Furthermore, teeth should not extend as far distal as the retromolar pad as the compressible soft tissue and curvature of the mandible may lead to instability of the denture during function. If there is insufficient space, a premolar or molar may need to be omitted from the set-up.14,20
Figure 1. Pound's triangle for posterior tooth placement.
The lower incisors are also placed on the anterior aspect of the ridge.13 However, care must be taken that the teeth are not set excessively labially as this will produce a cantilever effect, may compromise lower lip activity, and lead to an anterior-posterior rock in function. Conversely, if set too far lingual, teeth will encroach upon the tongue space, resulting in a lisp.12
Ultimately, tooth positioning is dictated by what is functional and acceptable to the patient.
Occlusal schemes
The three main occlusal schemes are bilateral balanced, lingualized and monoplane occlusions. Bilateral balanced occlusion is commonly taught throughout the majority of UK teaching hospitals.
In this scheme, the posterior teeth are set up with the maxillary palatal cusps occluding with the opposing central fossa. The incorporation of antero-posterior and mediolateral compensating curves help provide non-working side contacts in lateral excursions and protrusion (balanced articulation), which are intended to aid stability during function and prevent Christensen's phenomenon (occurrence of a posterior open bite on mandibular protrusion).
The use of zero degree cusps in a monoplane occlusion has been suggested in the cases of the resorbed lower ridge and Class II div 1 or Class III skeletal bases to reduce instability caused by excursive interferences. At first glance this may seem sensible, but this set-up does not actually allow balanced articulation20 because the lack of cusp angles prevent contact being maintained during lateral excursions.
An alternative concept is that of lingualized occlusion. The basic principle involves angling the maxillary teeth so that only the palatal cusps contact during centric occlusion and lateral excursions. The mandibular tooth is selectively ground to produce a shallow central fossa and shallow cusps; this allows both balanced working and non-working contacts21 (Figure 2). It is thought to improve stability of the lower denture due to the reduction of lateral stresses and dislodging forces. Theoretically, occlusal forces are shifted to the lingual side of the ridge, thus improving stability during mastication22 (the buccal flange will act to brace against any tipping motions). The frequency of prematurities in comparison to bilateral balanced occlusion is also reduced, lowering the risk of the denture being dislodged during function.15
Figure 2. Demonstration of a lingualized occlusal scheme with an angled palatal cusp from (a) buccal and (b) mesial views, in comparison to (c) bilateral balanced occlusion. (d, e) The difference in the lower teeth is shown, with the flattened, shallow occlusal surfaces of lingualized occlusion on the left and the normal cusp pattern of the bilateral balanced occlusion on the right of both images.
A number of studies have investigated the potential differences in performance of different occlusal schemes. The results tentatively suggest that cusped teeth (bilateral balanced occlusion) and lingualized occlusion may improve mastication over 0 degree cusps,23 but there was no benefit in stability or masticatory function noted between lingualized or bilateral balanced occlusions.21,22 From a practical and clinical viewpoint, however, balanced lingualized occlusion is probably easier to achieve accurately than bilateral balanced occlusion and therefore can be recommended. One should remember in this instance though, when adjusting the articulation, that only the lower lingual cusp should be adjusted so as not to affect the occlusal vertical dimension (the upper buccal cusp will have been angled not to interfere with excursive movements).
Generally, a Class I incisal relationship is desirable but this may not be possible, depending on the individual's skeletal relationship. The opposing incisor teeth should not be in contact in the intercuspal position but will become involved in protrusion; this arrangement leads to a more stable prosthesis. Class III skeletal relationships are an exception to this, as an edge to edge relationship may be more appropriate for aesthetics and a balanced occlusion.14
Given the discrepancy between the pattern of resorption between the mandible and maxilla, ideal tooth positioning can be challenging. As the maxilla becomes narrower, the mandible becomes wider and often the posterior teeth will have to be set into crossbite to compensate for this.24
The neutral zone
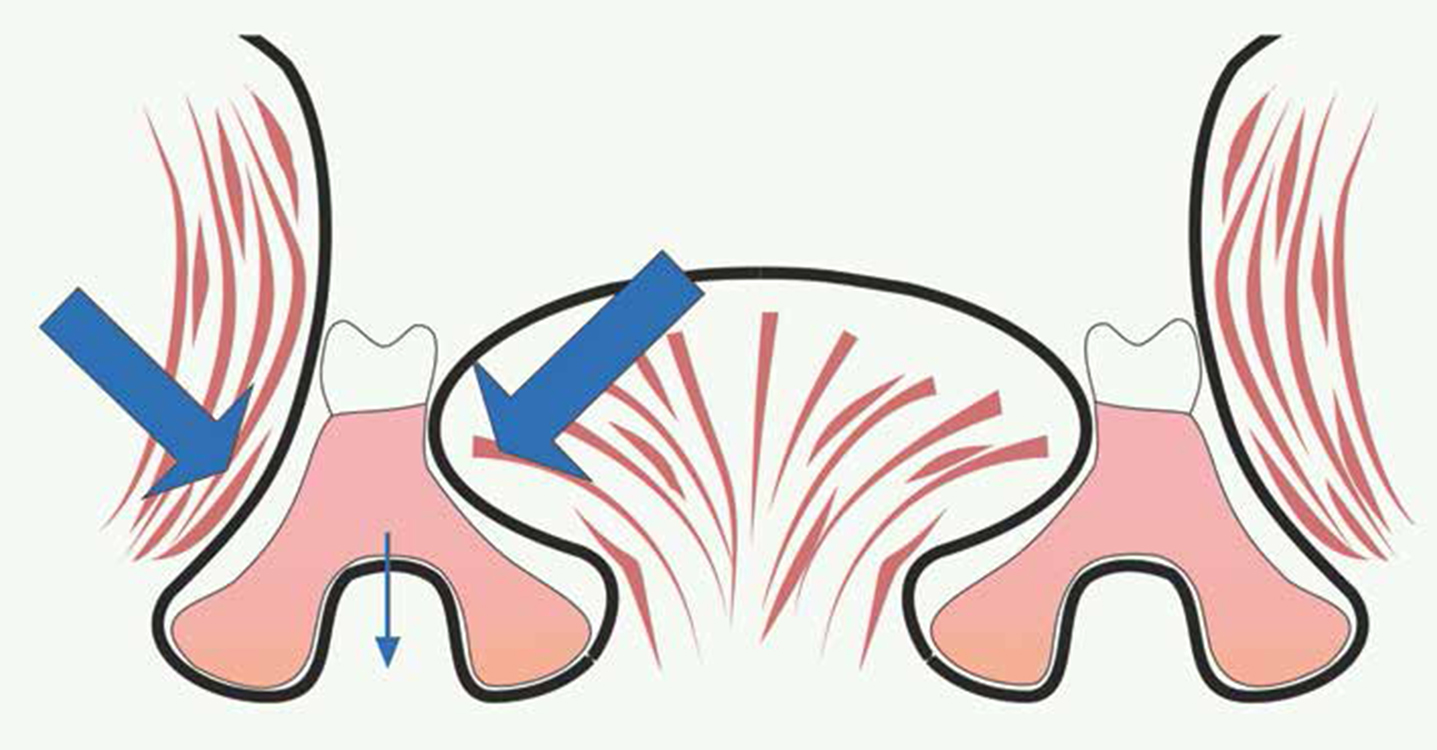
An alternative method of prescribing tooth positioning is the neutral zone technique. An additional benefit is that the entire polished surface position is outlined to the technician. The neutral zone is defined as the ‘potential space between the lips and cheeks on one side and the tongue on the other; that area or position where the forces between the tongue and cheeks or lips are equal’.25 An additional benefit is that the entire polished surface position is outlined to the technician. As with overextended flanges leading to instability, so can overcontouring of polished surfaces or inappropriate tooth positioning. Muscles with major influence on lower denture stability include: buccinator, the modiolus, mentalis, orbicularis oris, mylohyoid and the tongue.26 Furthermore, it has been proposed that suitable polished surface contouring can utilize muscle groups to stabilize the denture,27 particularly the tongue and buccinators (Figure 3). This has been advocated as one of the major stabilizing and retentive forces on dentures constructed on an atrophic mandible.26
Figure 3. Cross-sectional diagram demonstrating the actions of the buccinator and the tongue stablizing the lower denture.
The neutral zone technique is a useful tool in the clinician's armamentarium for treating the unstable lower denture, as well as having benefits in routine cases.11 Unfortunately, in an age of evidence-based dentistry, there is little high quality evidence to support the use of a neutral zone technique, but a good number of articles, including small interventional trials,28,29,30,31 case reports32,33,34,35 and review papers,11,27,36,37 demonstrate and discuss its benefits and success (including when the oral anatomy has been distorted or in neuromuscular disorders). The benefits reported included:
It has also been postulated that facial aesthetics are better, compared to teeth placed over the ridge in the atrophic mandible, as there is the correct support for the surrounding muscles.31 An argument against using this technique in the setting up of posterior teeth is that, by not positioning the teeth directly over the ridge during function, increased leverage (ie non-axial loading) will be produced, affecting stability. However, as long as the prosthesis is contoured correctly, the reciprocating forces of the tongue and cheeks should counteract these displacing forces.
Assessing the neutral zone
Assessing the neutral zone can be difficult and is not a skill that many clinicians have acquired. If the denture is stable at rest but displaces upon movement, it may be that the denture is either over-extended or lies outside of the neutral zone. The denture should be held in place and the patient asked to perform mandibular movements to assess any excessive interferences of the polished surface with the surrounding soft tissues visually; pressure indicating paste or light-bodied silicone can help here (Figure 4) (light bodied silicone will also demonstrate areas that are under-contoured). Alternatively, the denture can be seated and the direction of displacement at rest may give an idea of any neutral zone discrepancies. A common example is a supero-posterior displacement under the elastic recoil of the lower lip and modiolus region (Figure 5). This area is high risk for ‘over-bulking’ in the atrophic mandible because, following bony resorption, the mentalis attachment migrates towards the crest of the alveolar ridge.27 This often makes the neutral zone more lingual in comparison to when the patient was dentate. A more technical method of assessing the neutral zone includes taking a neutral zone impression then comparing this to the existing denture (a matrix could be made if there are minor differences). It may be worth mentioning at this point that, if the discrepancies are minor, then the adjustment of these areas may negate the need for a remake.
Figure 4. Light-bodied silicone being used as a check for over-contoured polished surfaces. The arrow points to an over-contoured area.Figure 5. Interference with lower lip causing denture to dislodge posteriorly at rest.
Recording the neutral zone
The theory of recording the neutral zone is simple. A volume of material is inserted on a stable base and various movements performed by the patient to shape the material defining the limits of the neutral zone. Recording of the neutral zone has been described in a number of ways,26,33,38,39,40 but conventionally is recorded using a special tray at a separate stage alongside the try-in of the upper denture26,38 (Figure 6). Table 3 and Figure 7 present the stages of recording a neutral zone impression. An alternative option is to record the neutral zone impression during registration on a lower wax rim that uses Manchester pillars10 (Figure 8). The process is the same as in Table 3, with the lower wax rim substituting for the special tray, although the number of appointments and overall cost is reduced. If desired, a second stage can be added and an impression taken of the polished surfaces alone at the try-in of the lower denture. In this technique, the teeth are set up with minimal supporting wax in the neutral zone defined by the initial impression; assuming that the tryin is suitable, an impression of the labial and lingual polished surfaces is taken on the try-in using a low viscosity silicone material. The polished surfaces are then contoured to this shape in the laboratory. If a suitable material is chosen for the initial impression, however, sufficient detail is likely to have been recorded and this stage is probably unnecessary.
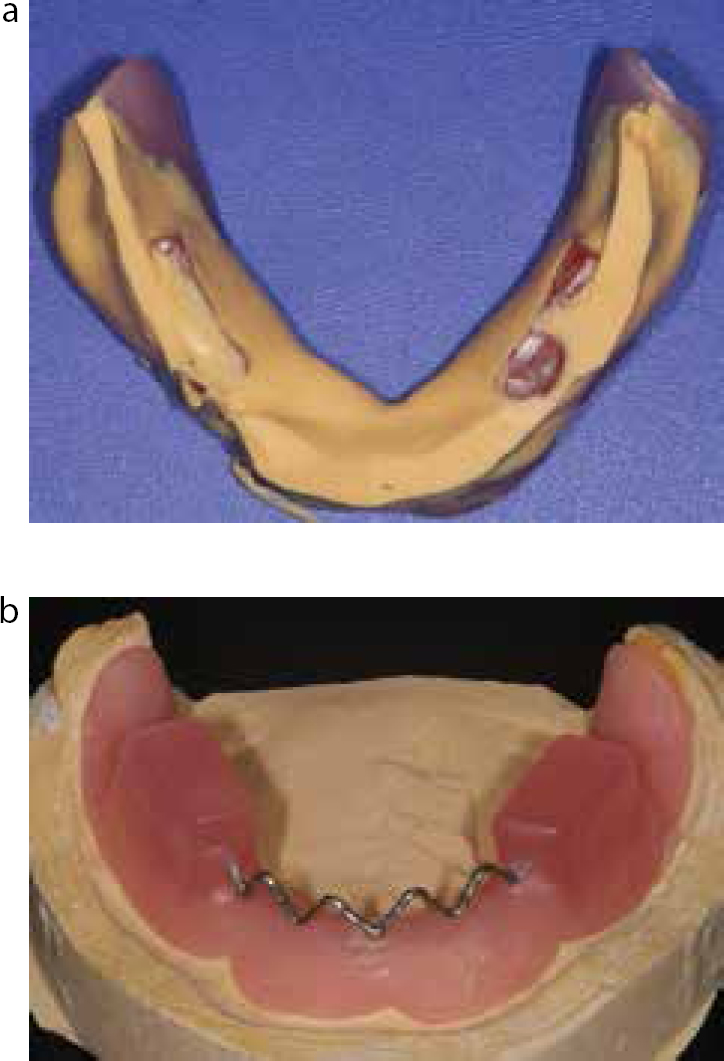
Figure 6. Examples of special trays used for recording the neutral zone.
Stages of Neutral Zone Impression
Special tray is tried in and checked to ensure no over extension or interference with surrounding soft tissues.
If required, adhesive is applied to the occlusal surface of the tray.
Material of choice is applied to the occlusal surface and the tray inserted into the patient's mouth in combination with upper try-in or patient's previous denture (common material choices are: medium-bodied silicone, tissue conditioners (eg Viscogel), impression compound, alginate).
Once inserted, the patient is asked to speak a variety of sibilants and perform a number of movements to define the limits of the neutral zone (if the patient has a sip of water first then it will produce a nice smooth finish to silicone impression materials). These tasks could include: swallowing, pursing their lips, opening wide, saying a number of simple sentences covering all articulatory phonetics, replicating a wide smile and moving the mandible side to side. It is important to say words with ‘o’ and ‘e’ sounds as this will maximally manipulate the modiolus; a particularly important anatomical structure in relation to patients with atrophic mandibles.
Once set, the impression is removed and assessed. If necessary, further adhesive can be applied and the impression sequence repeated to build the impression up to the correct OVD (this is generally only required for low viscosity silicones and care should be taken not to ‘over build’ the impression).
The impression is sent to the technician, who will create a putty matrix of the impression and set the teeth up to conform to the shape. The lower denture is then tried in as normal prior to finishing.
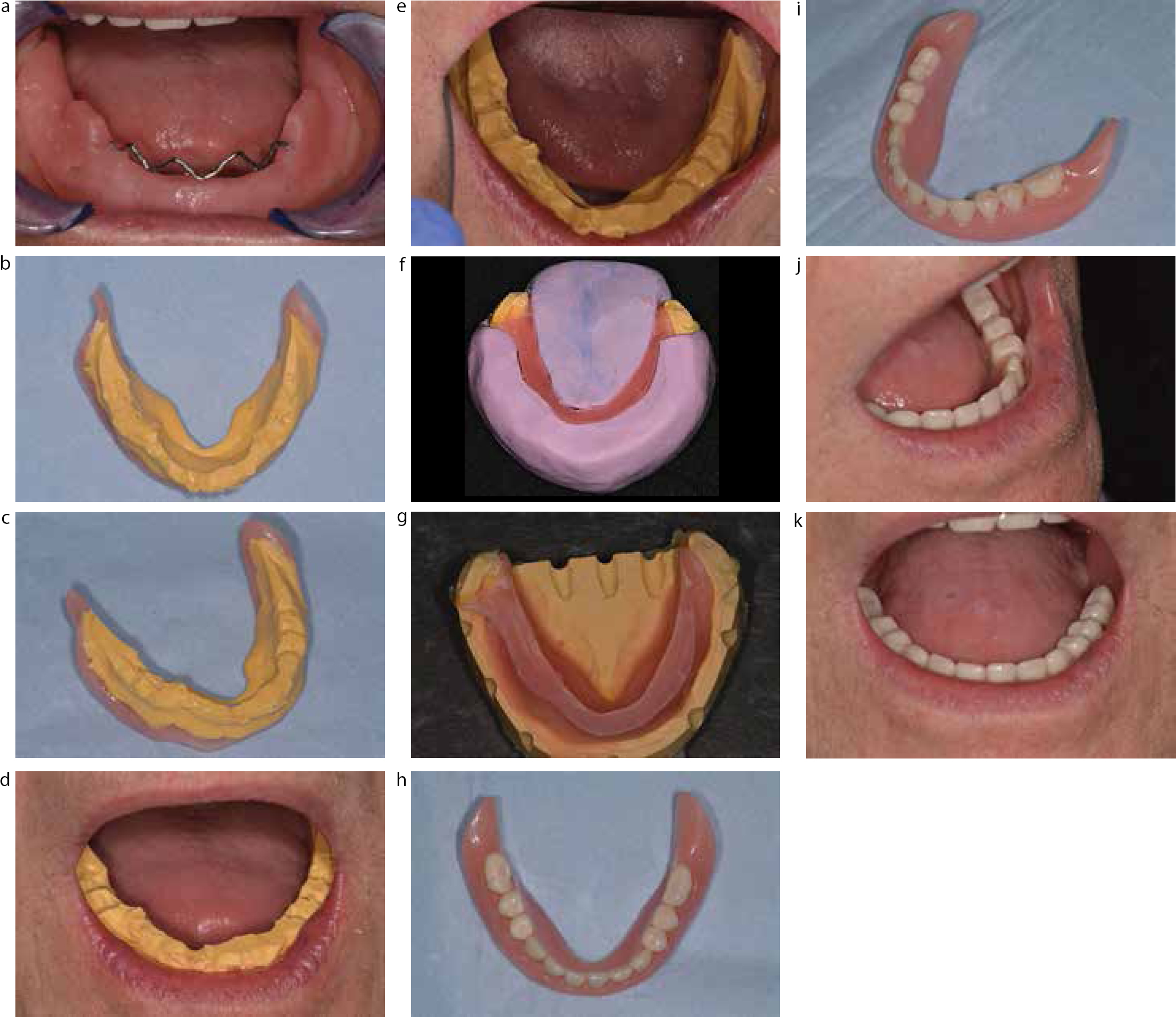
Figure 7. Stages of the neutral zone impression: (a) the tray in situ; (b, c) neutral zone recorded in medium-bodied silicone; (d, e) impression conforming to ‘the neutral zone’ intra-orally; (f, g) lab putty matrix and wax outline; (h, i) final prosthesis; (j, k)in situ.Figure 8.
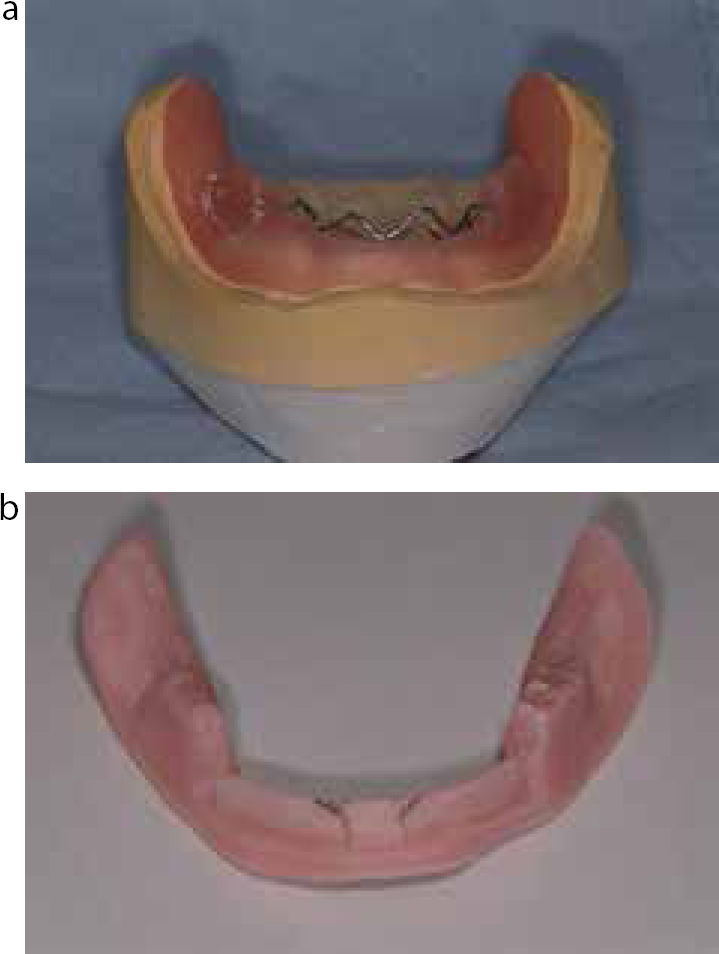
(a) Example of a neutral zone impression recorded on Manchester pillars. It is important that the baseplate is acrylic to ensure maximum retention. Furthermore, the width of the wax pillars needs to be minimal to reduce inaccuracies in the record (yet sufficient to maintain a satisfactory intermaxillary registration); this may sometimes be a compromise. (b) If desired, a central support structure for the impression can be added.
Conclusion
Managing the unstable lower denture can be very challenging and sometimes a stressful situation, especially when one feels that they have done everything possible for the patient and the result is still inadequate. For those patients, thought should be given to providing a two-implant retained overdenture, but if this is not possible (for whatever reason) then care should be taken to produce work that is as good as technically possible at each stage. Consideration should be given to the tooth positioning and the occlusal scheme, including considering use of a neutral zone impression technique to maximize stability. Recognition of the limitations of treatment is also fundamental and the patient needs to be made aware from the outset of treatment what is possible and where compromise needs to be made. With this as a starting point, the clinician may have an improved chance of achieving a reasonable outcome in a very difficult scenario.