Mehta SB, Banerji S, Millar BJ, Suarez-Feito JM Current concepts on the management of tooth wear: part 1. Assessment, treatment planning and strategies for the prevention and the passive management of tooth wear. Br Dent J. 2012; 212:17-27 https://doi.org/10.1038/sj.bdj.2011.1099
Loomans B, Opdam N, Attin T Severe tooth wear: European Consensus Statement on Management Guidelines. J Adhes Dent. 2017; 19:111-119 https://doi.org/10.3290/j.jad.a38102
Pindborg JJPhiladelphia, PA, USA: Saunders; 1970
Hammoudi W, Trulsson M, Smedberg JI, Svensson P Clinical presentation of two phenotypes of tooth wear patients. J Dent. 2019; 86:60-68 https://doi.org/10.1016/j.jdent.2019.05.028
Mehta SB, Loomans BAC, Banerji S An investigation into the impact of tooth wear on the oral health related quality of life amongst adult dental patients in the United Kingdom, Malta and Australia. J Dent. 2020; 99 https://doi.org/10.1016/j.jdent.2020.103409
Mehta SB, Loomans BAC, van Sambeek RMF Managing tooth wear with respect to quality of life: an evidence-based decision on when to intervene. Br Dent J. 2023; 234:455-458 https://doi.org/10.1038/s41415-023-5620-4
Manuel ST, Kundabala M, Shetty N, Parolia A Asthma and dental erosion. Kathmandu Univ Med J (KUMJ). 2008; 6:370-374 https://doi.org/10.3126/kumj.v6i3.1714
Mehta SB, Banerji S The prevention of tooth wear. Dent Update. 2020; 47:813-820
von Gonten AS, Rugh JD Nocturnal muscle activity in the edentulous patient with and without dentures. J Prosthet Dent. 1984; 51:709-713 https://doi.org/10.1016/0022-3913(84)90421-9
Baba K, Aridome K, Pallegama RW Management of bruxism-induced complications in removable partial denture wearers using specially designed dentures: a clinical report. Cranio. 2008; 26:71-76 https://doi.org/10.1179/crn.2008.010
Restoring a smile: full-mouth rehabilitation of an elderly patient IDP Kulathunga WPAW Goonathilake Dental Update 2025 51:6, 412-416.
Authors
IDPKulathunga
BDS (Sri Lanka)
BDS (Sri Lanka), MD in Restorative Dentistry (Colombo, Sri Lanka), Senior Registrar in Restorative Dentistry, Institute of Oral Health, Maharagama, Sri Lanka
BDS (Sri Lanka), MD in Restorative Dentistry (Colombo, Sri Lanka), Consultant in Restorative Dentistry, Colombo South Teaching Hospital, Kalubowila, Sri Lanka
Tooth wear is a significant problem in the ageing population and has increased in prevalence over the last century owing to the increase in life expectancy. Further, with the advances in dentistry, people tend to retain more of their natural dentition until the seventh or eighth decade of their lives and leading to an increased number of people with tooth wear. A certain degree of physiological tooth wear is inevitable over a lifetime as a result of the continuous function of the dentition.
CPD/Clinical Relevance: A removable prosthesis, used in patients with severely worn teeth, is cost-effective compared to other prosthetic options and can be easily maintained hygienically.
Article
The predicted percentage of adults presenting with severe tooth wear has been reported to increase from 3% at the age of 20 years, to 17% at the age of 70 years. Therefore, there is a tendency to develop more tooth wear with age.1 The highest prevalence of tooth wear is shown by males (70%) than females (61%) according to the adult dental health survey carried out in the UK in 2009.2
A study by Lambrecht and co-workers in 1984 found that the physiological tooth wear is 29 µm/year for molars and 15 µm/year for premolars.3 When this wear rate accelerates owing to various exogenous and endogenous factors acting alone or together, there is progressive tooth wear. According to Loomans et al, pathological tooth wear is defined as an atypical type of wear for the age of the patient that causes pain or discomfort, functional problems, or deterioration of aesthetic appearance, and which, if it progresses, may give rise to undesirable complications of increasing complexity. The wear process is often multifactorial with an interplay among the processes of erosion, attrition, and abrasion.4 This aetiological classification was proposed by Pindborg in 1970.5 where the delineation of each aetiology is questionable clinically. Severe tooth wear could result from a mechanical cause, a chemical cause, or a combination of both. However, Hammoudi et al have proposed that erosion to be the leading cause of tooth wear.6
Higher levels of tooth wear have been found to have a significant effect on oral health-related quality of life.7 The commonest problems in patients include sensitivity or pain owing to the exposure to dentine, difficulty in chewing and eating, and psycho-social impact.4 Aesthetic concerns are the most common reasons for referral to secondary care settings where patients are motivated to seek professional care owing to impaired appearance and function.8
The vertical dimension of occlusion (OVD) is the vertical dimension when the maxillary and mandibular teeth occlude each other.9 In dentate patients with generalized tooth wear, interocclusal space can be gained with increased OVD. This height depends on patient tolerance, restorative technique, and properties of the chosen restorative material. If the tooth wear is not compensated by dento-alveolar growth, the restorations of increased OVD are well tolerated by the patient.10 Dento-alveolar compensation can be identified through careful examination of resting vertical dimension (RVD), freeway space (FWS) and OVD. If dento-alveolar compensation occurs, with the presence of normal RVD, FWS and OVD, enhanced OVD and a change of FWS may be required. This is well tolerated by dentate patients when compared to edentulous patients.10
The diagnosis is made by identifying whether the tooth wear is pathological or physiological. The management plan should be decided on several factors: extent of tooth wear; the potential for progression; the patient's reaction to treatment; and the presence of symptoms. Monitoring and counselling may be the preferred option in the absence of functional and aesthetic issues.11
The management of generalized tooth wear could be carried out with a confirmative or reorganized approach. The former option is applicable when the existing OVD is satisfactory and the occlusion is stable, whereas the latter approach is considered when the existing occlusion is unstable and/or undesirable, the available space is inadequate, or the aesthetics are impaired.10 As the centric relation is reproducible, it is generally accepted to reorganize the occlusion, to have an anterior–posterior jaw relationship with a new intercuspal position (ICP) coinciding with the RCP.12
The following clinical report enumerates the management of a patient with severe non-carious tooth surface loss thought to be a result of attrition and erosion.
Case report
A 75-year-old male patient presented to the restorative dentistry unit at the Institute of Oral Health, Maharagama, Sri Lanka complaining of the inability to eat efficiently owing to their worn teeth. He had experienced several episodes of intermittent mild pain from some of the lower teeth for the previous few years and had neglected to receive any dental treatment. He presented with a removable partial denture (RPD) replacing his missing UL1 and which he had been using for over 20 years.
He was a diagnosed asthmatic patient who used drugs and steroid inhalers during exacerbations of breathing difficulty. Although the patient had mentioned that he was not exhibiting parafunctional habits, his wife stated that she had noticed visible and audible bruxes at night. He consumed a low-sugar diet and occasional acidic or carbonated drinks. His oral hygiene practices were satisfactory, with good manual dexterity but overzealous brushing. He had a marked generalized yellowish tooth discolouration as a result of ageing, which he was not worried about at all. His main consideration was to get his teeth back to functioning comfortably.
Examination and investigations
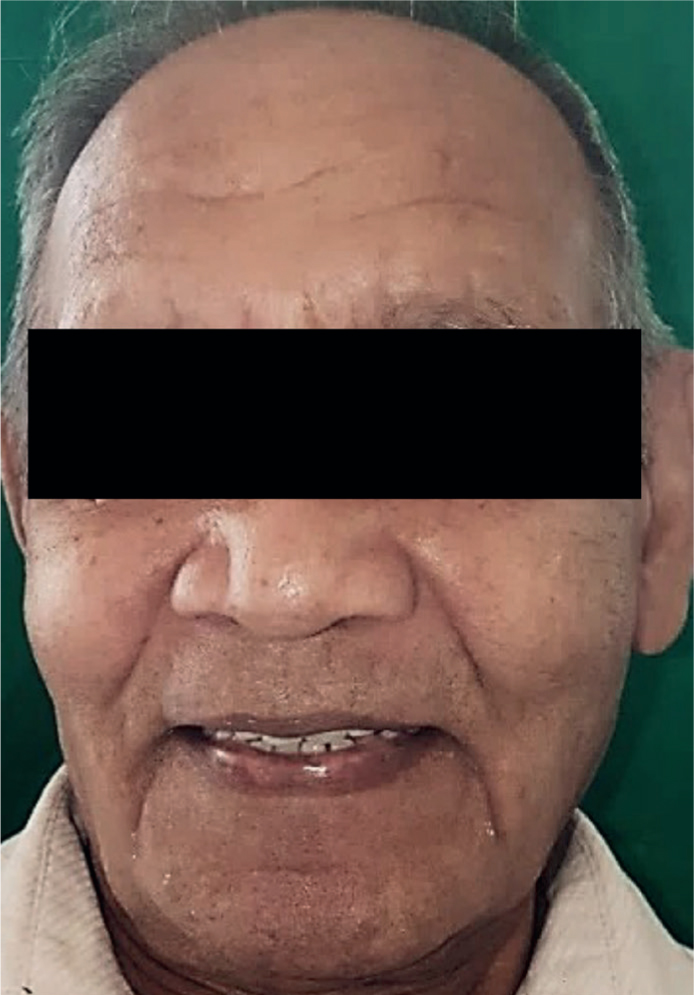
His extra-oral facial appearance revealed overclosure of the mandible accompanied by a noticeable reduction of lower facial height (Figure 1). The OVD was reduced and FWS was increased by 4 mm. Although he had a class 1 skeletal relationship, he showed a pesudoprognathism of the mandible owing to habitual anterior positioning of the mandible.
Figure 1. Pre-operative facial view showing the reduced lower facial height and creased mouth commissures.
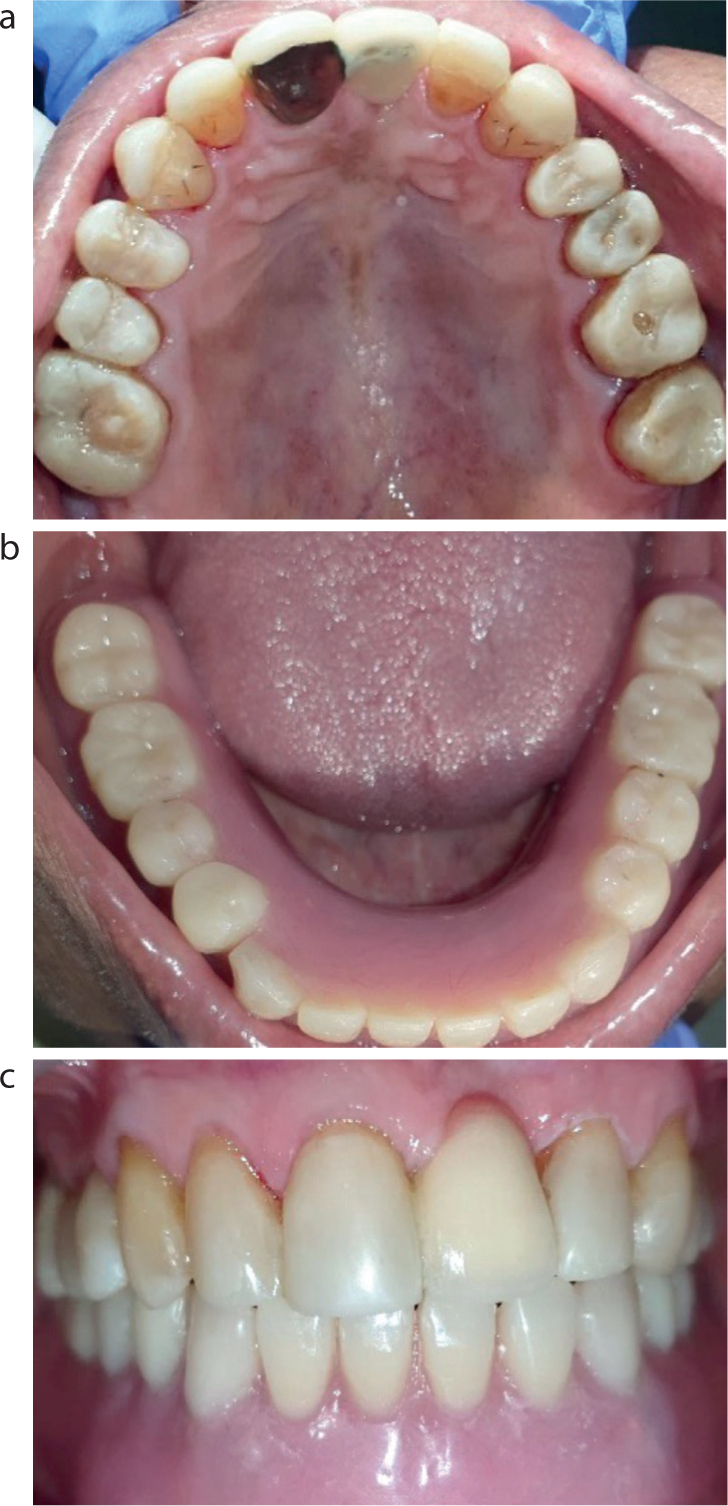
The Basic Periodontal Examination revealed a score of 2 in the upper sextants due to the presence of calculi, and a score of 0 in the lower arch (Figure 2). The teeth UR1–UR6 and UL2–UL7 were present in the upper arch, with the retained roots of UR7 and UR8 (Figure 2b). Deep proximal cavities with food packing were noticed on UL6 and UL7. He had severely worn LL1–LL5, LR1–LR5 and LR7 in the lower arch (Figure 2c). None of the teeth showed mobility, associated sinus formation or abscesses; however, LR3 and LR5 demonstrated tenderness to percussion.
Figure 2. Pre-operative intra-oral views. (a) Labial view showing flat worn teeth with sharp edges. Note the interdigitating worn teeth. (b) Upper occlusal view showing flattened cusps and erosive lesions. (c) Lower occlusal view. Almost all teeth were worn, exposing the tooth pulp.
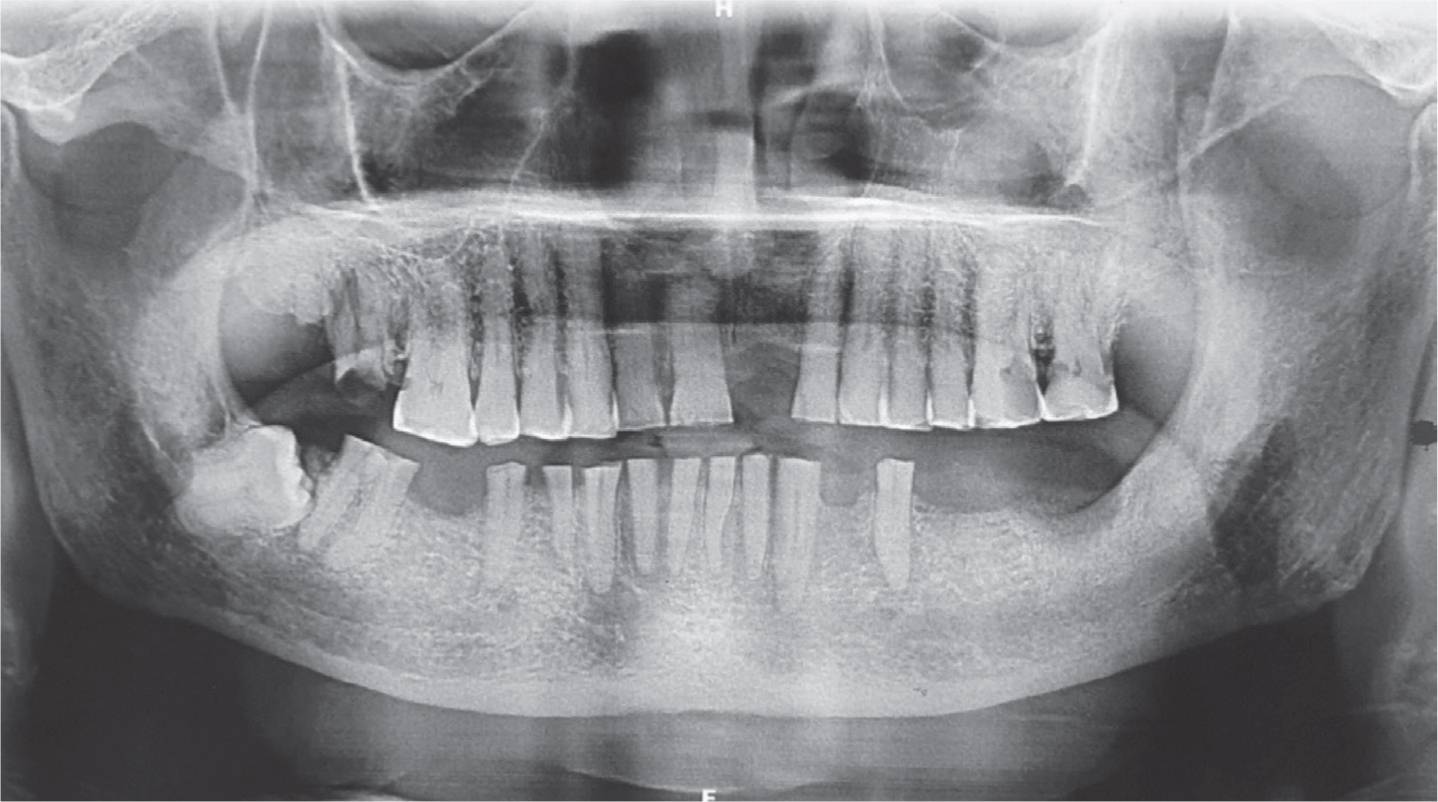
Both upper and lower occlusal surfaces were flattened out with no remaining occlusal anatomical details. Occluding surfaces of the lower teeth were polished, showing well-defined wear facets matching the corresponding opposing arch dentition (Figure 2). They displayed attrition with exposure of the pulp cavities with complete loss of enamel and less than one-third of the coronal hard tissues of lower teeth remained (Figure 2a). The upper arch anterior teeth had less than one-third of tooth tissue loss incisally, with minimal dentine exposure (Figure 2a, b). There was no visibility of teeth during smiling. Pulp sensibility testing with an electric pulp tester failed to elicit any response on UL6, UL7 and all the mandibular teeth. The dental panoramic view was supplemented with several peri-apical radiographs (Figure 3).
Figure 3. Pre-operative dental panoramic view.
Treatment planning
The patient was informed the following treatment options:
Restorative options: direct composite restorations of upper worn teeth or indirect restorations with porcelain fused to metal/zirconia crowns;
Prosthetic options: upper RPD, an implant-supported single crown or RBB for the replacement of UL1, Lower tooth supported metal-based overdenture.
He was reluctant to go ahead with invasive procedures owing to his age and very keen on preserving his existing dentition. Therefore, the patient was informed regarding possible treatment options. As a single-tooth replacement was needed for the upper arch, an RBB was felt to be the best option rather than a metal-based RPD. Finally, resin composite restorations for worn teeth, RBB on UL1 and a lower tooth-supported overdenture were decided. Full mouth rehabilitation through reorganizing the existing occlusion was planned to achieve a new ICP in the increased OVD at RCP.
Prevention and treatment procedure
The patient was educated regarding the possible aetiological factors for his tooth substance loss. As his dietary history revealed a certain amount of erosive food consumption, which could contribute to non-carious tooth substance loss, he was educated on reducing consumption of acidic and carbonated food. The Modified Bass brushing technique and dental flossing were demonstrated and he was advised to use a soft-bristled toothbrush. He was instructed to rinse his mouth thoroughly following inhaler usage for his asthma. Full-mouth scaling and polishing were followed by fluoride varnish application to help self-practice oral care.
Extraction of the retained roots at the UR7 and UR8 teeth were carried out under local anaesthesia. In a subsequent visit, a facebow recording was taken and casts were mounted in a semi-adjustable articulator. A primary wax-up was made for an adjusted OVD. The provisional denture was fabricated to this new OVD, which had increased by 4 mm. This vertical height was verified in rest position with consideration given to facial muscle relaxation, phonetics, aesthetics and swallowing ability. A provisional acrylic overdenture was made at the new OVD and its tolerability assessed at follow-up visits. Meanwhile, root canal treatments were carried out on UL6, UL7 and lower teeth using endo motor (Endo-Mate AT, NSK, Japan).
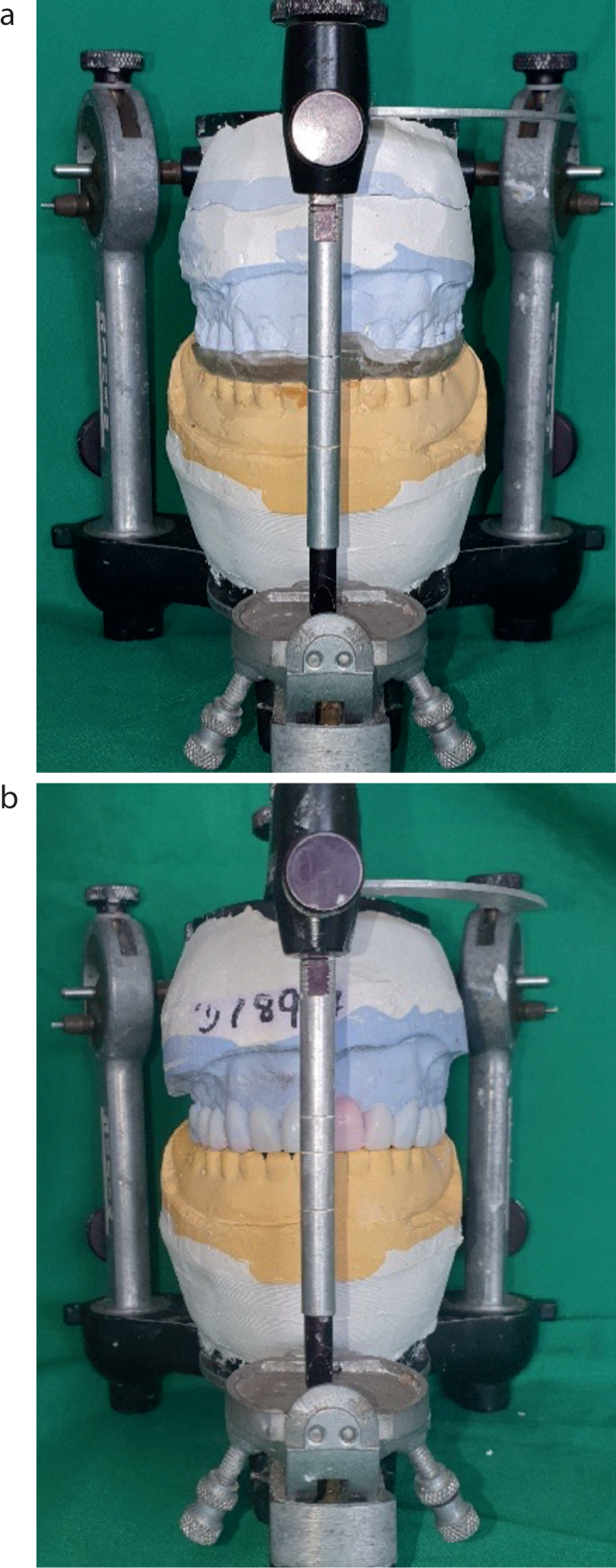
During follow-up visits, the patient showed good tolerance to the prosthesis. A facebow recording was obtained and a second series of diagnostic casts were mounted to a semi-adjustable articulator. The OVD had to increased by an additional 2 mm in order to provide restorations to the upper teeth. Therefore, an acrylic splint was used to check the patient's adaptability to this additional height (Figure 4a). He showed a good tolerance with the given diagnostic splint. Maxillary teeth diagnostic wax-up was made according to the correct morphology using the adjusted height (Figure 4b).
Figure 4. Articulated study models on a semi-adjustable articulator. (a) Further increased OVD by 2 mm using acrylic splint. (b) Diagnostic wax-up for the increased OVD.
The upper teeth wax-up was duplicated and a vacuum-formed matrix was constructed to use for direct composite resin restorations of the worn teeth. This matrix helped in rebuilding the correct morphology of the teeth for their given height with less chair time. This matrix was used for the direct resin restorations on upper teeth. A new provisional upper acrylic partial denture was constructed to replace UL1.
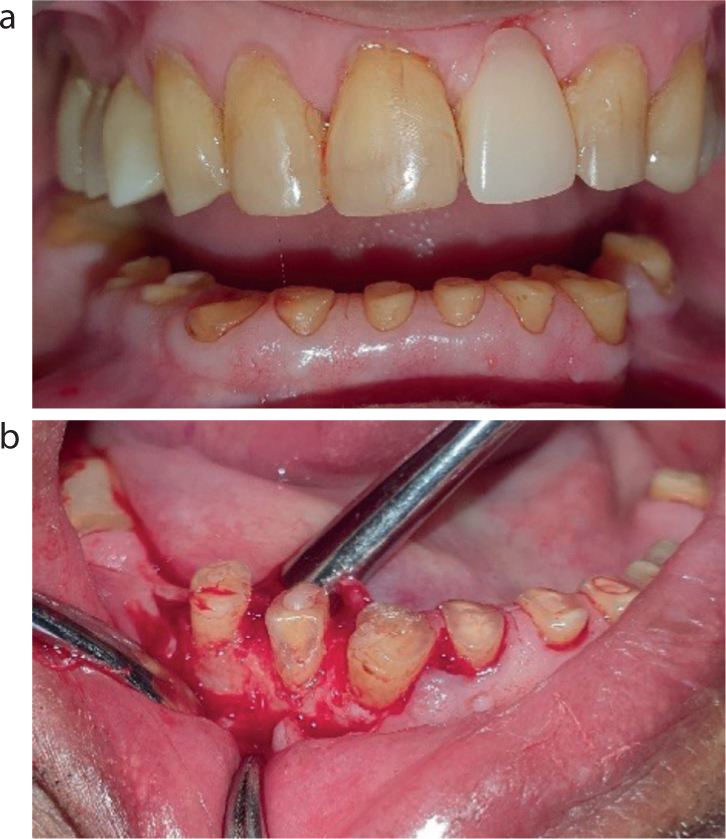
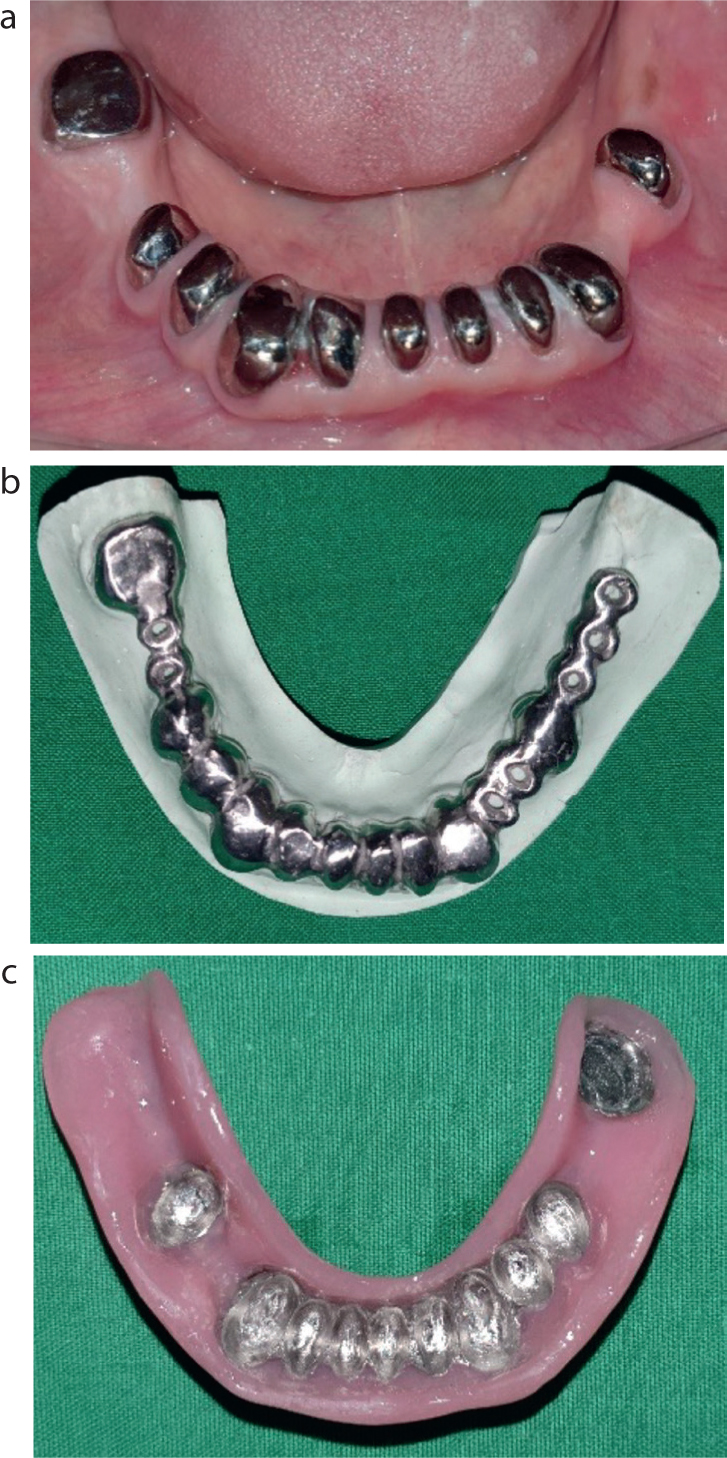
A crown lengthening procedure was carried out for LR3, LR4 and LR5 as the tooth structure was less than 2 mm (Figure 5). After an adequate healing period, the teeth were prepared to a dome shape, 3 mm above the gingival margin and cast metal copings were provided for lower teeth (Figure 6). Construction of an upper RBB for UL1 and the lower definitive metal overdenture were simultaneously carried out in the following visits. After fine adjustments, the final processing of the lower overdenture and RBB were performed, and the finished RBB was cemented using an adhesive luting cement (Multi-Link N, (Ivoclar Vivadent, Liechtenstein) (Figure 7).
Figure 5. Crown lengthening surgery. (a) LR3–LR5 showing the reduced crown height. (b) Crown lengthening.Figure 6. Construction of the lower metal overdenture. (a) Cemented metal copings on root canal-treated lower teeth. (b) Metal framework for the overdenture. (c) Impression surface of the finished overdenture.Figure 7. Post-operative intra-oral views. (a) Upper occlusal view with resin restorations and resin-bonded bridge of UL1. (b) Lower occlusal view with overdenture in situ. (c) Labial view.
Finally, the overdenture retention, stability and occlusion were checked prior to the delivery. The patient was extremely happy and immensely satisfied with the aesthetics and functional improvement, and reported a markedly improved quality of life (Figures 8 and 9).
Figure 8. Post-operative dental panoramic view.Figure 9. Satisfied patient with his happy smile.
Discussion
Oral rehabilitation of patients with non-carious tooth surface loss (NCTSL) requires strategies that address all the factors relevant to the aetiology and pathogenesis of the condition. Therefore, management should always start with prevention, and in most cases, prevention is the only management strategy. However, in cases with symptoms, prevention is important together with restorative stages and long-term maintenance care.
The immunosuppression and anti-inflammatory effects of steroidal medications and oral environmental changes, such as reduction of salivary flow rate, increased salivary pH, drugs containing sugary substitutes and dryness of the mouth, make asthmatic patients more susceptible to caries, periodontal disease, oral candidiasis and erosion. Therefore, such patients need to be advised to rinse their mouth thoroughly after medication usage.13 Although most literature is inconclusive about the relationship between erosive tooth wear and asthma medication, several studies present evidence that asthmatic medications can place the patient at risk of dental erosion by reducing salivary protection against extrinsic or intrinsic acids.13 Therefore, these patients are in a higher-risk group for dental erosion prophylactic cover with fluoride therapy may be indicated.14 Furthermore, patients with erosive tooth wear concerns may benefit from concentrated fluoride therapy. Therefore, a fluoride gel or varnish application was indicated for this patient for the prevention of caries, as well as erosive tooth wear management.15
The bruxofacets are a typical feature of bruxism (flat, smooth, shiny areas with sharp edges) and the resulting erosion contributed to accelerated tooth wear.9 Generally, the use of a night guard is recommended for nocturnal bruxists.4 The literature suggests that nightly use of dentures during sleep is associated with reduced sleep bruxism levels.16 An acrylic overdenture could be a good option for planning an increased OVD and which can be used for the purpose of wearing during sleep, as described by Baba and co-workers.17 The same denture can be used as the provisional denture during the stabilizing period.
The commonest clinical problems associated with worn dentition are aesthetics, pain, loss of function, reduced inter-occlusal space and poor compliance of elderly patients for continuous attendance for treatments.3 In the current case, the patient's function was impaired. His sagittal facial view revealed mandibular pseudo-prognathism, which is a feature of OVD loss and overclosure. Although aesthetics was not much of a concern, his reduced occlusal vertical dimension without dento-alveolar compensation gave a clue for the rapidity of the tooth wear, which needed to be addressed with active treatments.
Tooth-retained overdentures have several advantages, including a patient's feeling of remaining dentate through the preservation of the natural teeth,18 minimizing alveolar bone resorption, keeping sensory feedback and proprioception intact and greater stability, retention and support.19 Additionally, the overdenture can resist the high occlusal forces directed by an opposing natural dentition,18 which was a similar finding in the current case. An overdenture constructed with a metal base can improve fracture resistance and use of acrylic teeth can act as a kind material for the opposing natural teeth.20
In the current case, all the upper arch teeth had a considerable amount of remaining enamel with exposed dentine. With the improvements in adhesive dentistry, and the availability of superior resin composite materials, adhesive restorations have become the mainstay of restoring worn teeth. It is cost effective and non-invasive compared to ceramic restorations. According to Hemmings et al, the failure rates of direct composite restorations over 36 months were relatively low in composite restorations. Direct composite restorations could be successfully used in cases where 50–75% of the crown height has been lost.20 Therefore, direct resin composite restorations were selected with the help of a custom-made vacuum-formed thermoplastic matrix.
Patients undergoing this kind of advanced restorative treatment should be aware of possible failures. Patients treated for tooth wear are heavily restored, and dental caries and periodontal diseases could be worsened owing to the presence of multiple restorations. Reliable recall will help prevent such diseases and prevent restoration failures.21 Therefore, this patient was educated regarding the importance of review and maintenance care, and recalled every 6 months.
Conclusion
Restoration of an extremely worn dentition presents a greater challenge to the dentist. According to evidence, tooth wear is growing in prevalence and severity in seniors who are living longer. The mystery of excellent outcomes is keyed to accurate diagnosis with the help of a detailed history, examination, and investigations. The various treatment modalities will be unique for each patient. However, the goal of any treatment should be patient satisfaction by achieving acceptable aesthetics and satisfactory function.