Crawford PJ, Aldred MJ, Clarke A Clinical and radiographic dental findings in X linked hypohidrotic ectodermal dysplasia. J Med Genet. 1991; 28:181-185 https://doi.org/10.1136/jmg.28.3.181
Witkop CJ, Brearley LJ, Gentry WC Hypoplastic enamel, onycholysis, and hypohidrosis inherited as an autosomal dominant trait. A review of ectodermal dysplasia syndromes. Oral Surg Oral Med Oral Pathol. 1975; 39:71-86 https://doi.org/10.1016/0030-4220(75)90398-9
Grover R, Mehra M Prosthodontic management of children with ectodermal dysplasia: review of literature. Dentistry. 2015; 5:2161-1122
Filius MA, Cune MS, Raghoebar GM Prosthetic treatment outcome in patients with severe hypodontia: a systematic review. J Oral Rehabil. 2016; 43:373-387 https://doi.org/10.1111/joor.12384
Yap AK, Klineberg I Dental implants in patients with ectodermal dysplasia and tooth agenesis: a critical review of the literature. Int J Prosthodont. 2009; 22:268-276
Wang Y, He J, Decker AM Clinical outcomes of implant therapy in ectodermal dysplasia patients: a systematic review. Int J Oral Maxillofac Surg. 2016; 45:1035-1043 https://doi.org/10.1016/j.ijom.2016.03.011
Basker RM, Davenport JC, Tomlin HR Prosthetic Treatment of the Edentulous Patient.: Palgrave Macmillan; 1991
Ahuja S, Cagna DR Classification and management of restorative space in edentulous implant overdenture patients. J Prosthet Dent. 2011; 105:332-337 https://doi.org/10.1016/S0022-3913(11)60064-4
Schnabl D, Grunert I, Schmuth M, Kapferer-Seebacher I Prosthetic rehabilitation of patients with hypohidrotic ectodermal dysplasia: a systematic review. J Oral Rehabil. 2018; 45:555-570 https://doi.org/10.1111/joor.12638
Filius MAP, Cune MS, Créton M Oral health-related quality of life in dutch children diagnosed with oligodontia. A cross-sectional study. Int J Environ Res Public Health. 2019; 16 https://doi.org/10.3390/ijerph16132371
Returning to foundation principles: oral rehabilitation of a child with ectodermal dysplasia and hypodontia Nidhi Parmar Rajkaran Singh Virdi Dental Update 2025 52:1, 61-66.
Ectodermal dysplasias (ED) are a group of genetic disorders, of which common oral presentations include severe hypodontia and conically formed anterior dentition. With the average ED patient missing 23.7 permanent teeth, the ramifications of severe hypodontia directly correlate with quality of life and treatment complexities. The aim of prosthodontic rehabilitation is to provide an age-appropriate dentition to aid aesthetics, phonetics, masticatory and psychosocial development, recommended for commencement at an early age, including support throughout life. This case report demonstrates a non-invasive, simple and predictable approach to the prosthodontic rehabilitation of a 9-year-old child with ED affected by severe hypodontia.
CPD/Clinical Relevance: Non-surgical prosthetic treatment can be a safe and predictable first-line treatment for the oral rehabilitation in patients with hypodontia.
Article
Ectodermal dysplasia (ED) is the term defining over 150 rare, inherited syndromes, with genetic defects in two or more ectodermal structures such as skin, hair, nails, exocrine glands, sebaceous glands, and teeth.1 The notable phenotypic signs and symptoms on which an ED diagnosis is made includes hypohidrosis, hypotrichosis, and severe hypodontia of both primary and permanent dentitions.2 Severe hypodontia is the agenesis of six or more teeth, with the exclusion of third molars, and it is reported that children with ED have, on average, 23.7 missing permanent teeth.3,4 Since severe hypodontia leads to hypoplasia of the alveolar ridges, there is a subsequent reduction in occlusal vertical dimension and impact on the lower vertical face height. This compromises facial aesthetics resulting in distinctive appearances comparable to edentulous patients who have not been restored, owing to increased labial folding and prominence of the chin. It should be noted that 80% of patients with ED exhibit additional oral anomalies, such as xerostomia, delayed eruption, microdontia, irregular shaped or malformed dentition, which pose further treatment complications.5
The effects of severe hypodontia directly correlate to an impaired quality of life that impacts on extra- and intra-oral aesthetics, phonetics, masticatory function and psychosocial difficulties. The oral rehabilitation of a child with ED requires early recognition and age-appropriate intervention. It has been shown that dental treatment as early as 3 years of age can aid psychosomatic development.6 The high treatment complexity requires the continued care by multidisciplinary teams including primary care practitioners, paediatric dentists, orthodontists, restorative dentists, prosthodontists, and occasionally maxillofacial surgeons. Management can vary from simple dental acclimatization, prevention and preservation of the current dentition, to complex oral rehabilitation with or without the aid of dental implants, depending on age and anatomy.7
This case report outlines the positive application of non-surgical prosthodontic treatment that can be delivered to paediatric ED patients who have been affected by severe hypodontia. It also highlights the appreciation of sound prosthodontic principles to optimise outcomes, in hopes to benefit dental clinicians and specialties involved in the care of these vulnerable patients.
Case report
A 9-year-old male patient presented at the Oxford University Hospitals, with parental concerns regarding replacement of missing teeth, to restore aesthetics, form, and masticatory function. He had undergone previous attempts at denture construction within hospital settings with limited overall use. Medically, he had hypohidrotic ED, with no other medical conditions.
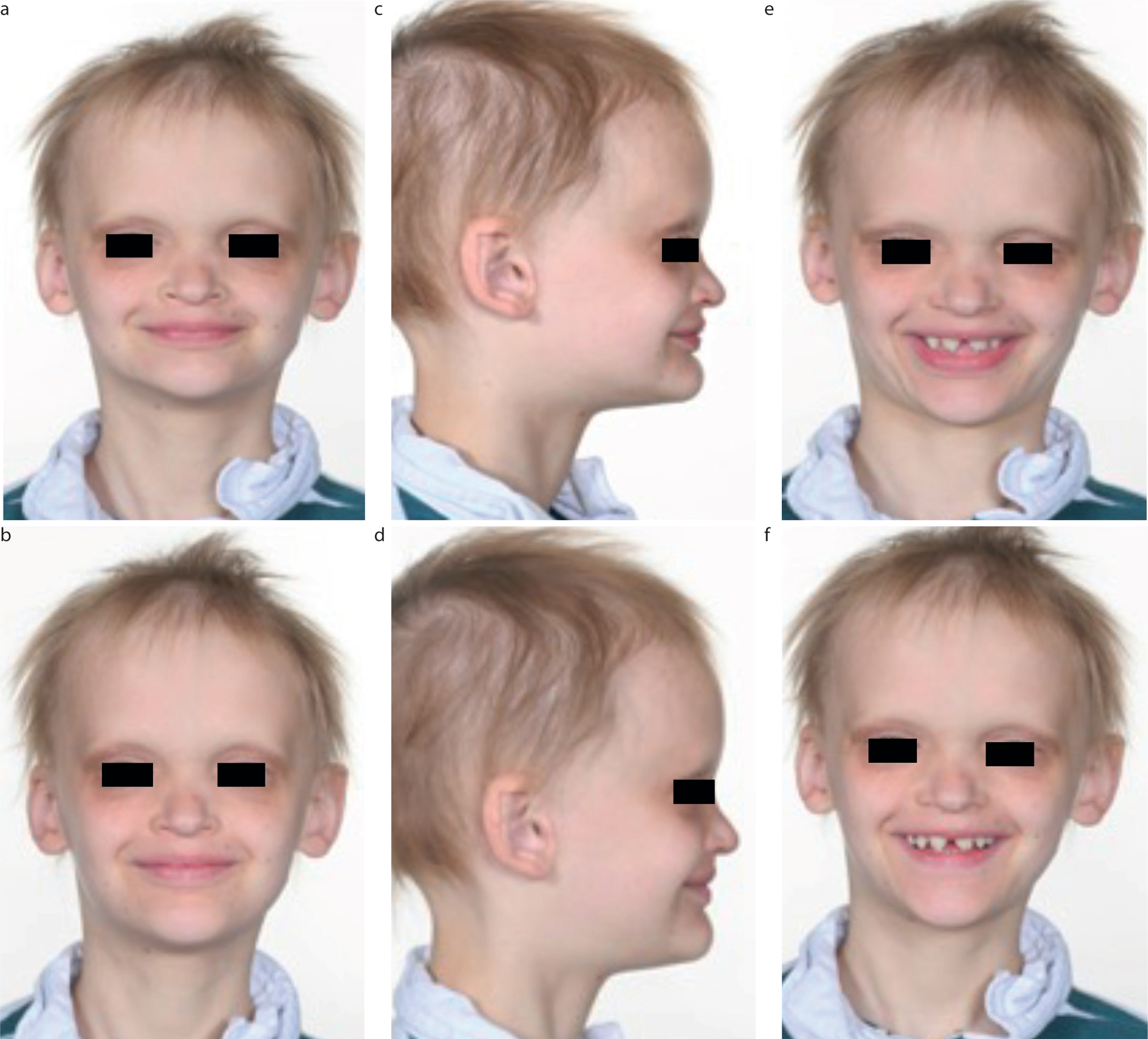
Upon clinical examination, the patient presented with features consistent with ED, which included frontal bossing, maxillary hypoplasia, mandibular retrognathia, dry skin, fine textured hair, nasal bridge depression and an endogenous tongue thrust at rest (Figure 1).6 He had a Class II antero-posterior skeletal relationship with a prominent pogonion. The vertical proportions exhibited a reduced lower anterior face height and Frankfort mandibular plane angle.
Figure 1.
(a,c,e) Extra-oral photos to show pre-operative Class II AP skeletal relationship, reduced lower facial height, retrognathic mandible, anterior open bite with thrusting tongue and (b,d,f) which are seen to be corrected once the prostheses are in situ.
Intra-orally, the patient's mandibular ridge was atrophic (Cawood and Howell Class V) and the maxillary ridge was fair in terms of height and width (Cawood and Howell Class IV). He had six permanent teeth only: the upper central incisors and canines and the lower canines (UR3, UR1, UL1, UL3, LR3, LL3). There was generalized spacing, and the canine dentition was conical in shape as well as splayed. He had marked Class II division I malocclusion, with overclosure. There was contact between the UR3 and LR3; however, the UL3 was in traumatic occlusion opposing gingivae when in maximal intercuspal position.
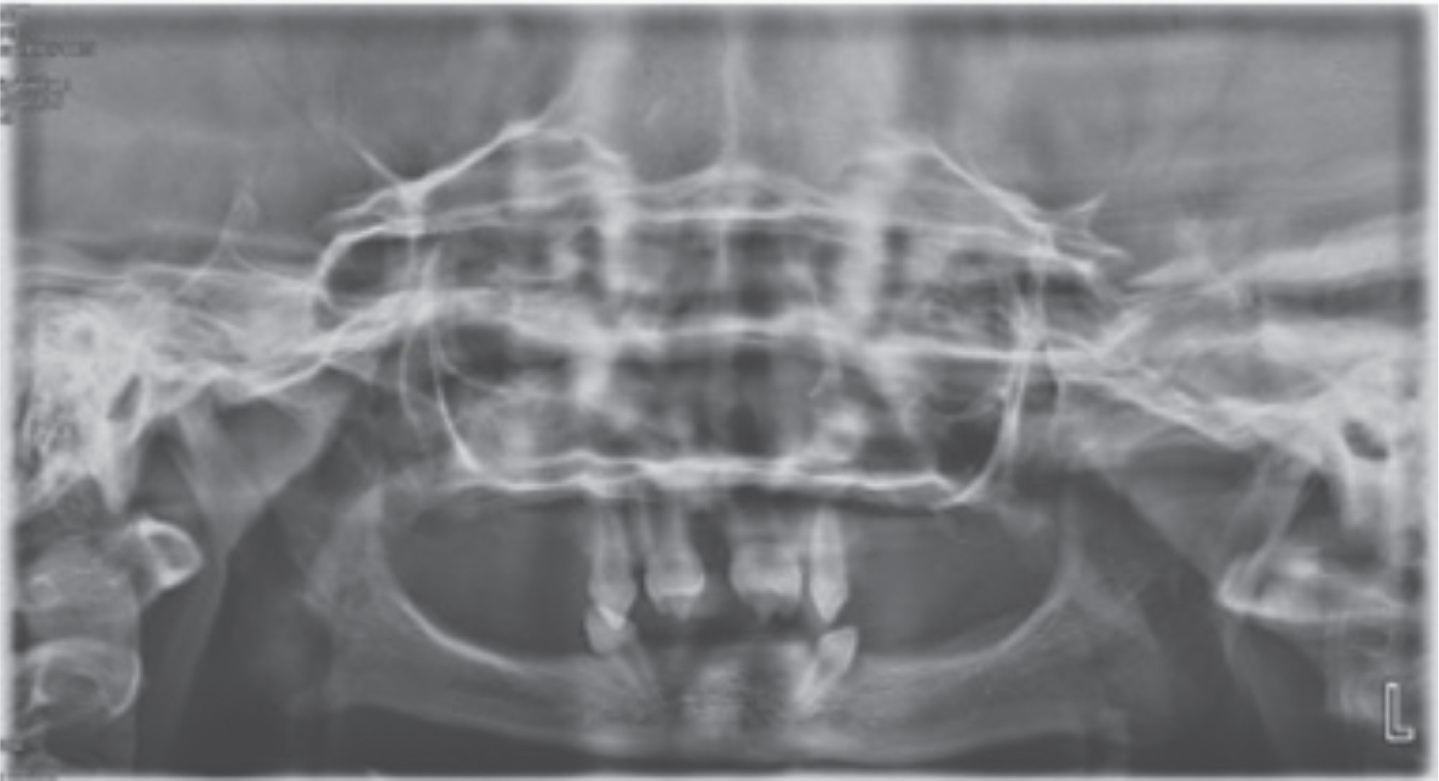
An orthopantomogram revealed the congenital absence of the majority of his permanent dentition (Figure 2). It also displayed the limited height of the maxillary ridge with proximity to the maxillary sinuses and atrophic mandible.
Figure 2. OPG to assess bone levels, dentition and presence of pathologies.
The following diagnoses were made:
Severe hypodontia of the UR76542, UL24567, LR765421, LL124567;
Atrophic dento-alveolar ridges;
Traumatic occlusion;
Conical-shaped canine dentition.
Following clinical and radiographic investigations, treatment options were discussed, and the patient and parent were happy to re-attempt construction of conventional removable upper and lower prostheses: upper partial acrylic and lower complete acrylic overdenture treatment owing to the pronounced distal inclination, conical tooth form, and lack of prosthetic space. Following due consideration, the patient was keen to preserve the aesthetics of his maxillary anterior teeth, which he felt was part of his identity, thus additive composite contouring or being incorporated in an overdenture design was ruled out. Additionally, interceptive orthodontics was taken into consideration if it were subsequently felt that denture retention was compromised and a bounded saddle required between the UR3–UR1 and UL1–UL3.
Oral rehabilitation with dental implants is a treatment option; however, as typically identified in ED patients including in this patient, there was insufficient alveolar height and width, and there was risk of iatrogenic damage to crucial anatomical structures, including the inferior dental nerve.7 If dental implants were to be considered, this would be likely to require extensive hard and soft grafting procedures and replanning. Furthermore, despite extensive grafting procedures this may still be sufficient to retain maxillary and mandibular dentures only owing to lack of a sufficient number of implants typically required for fixed implant bridgework.
Cases have been reported with early placement of dental implants in young individuals. This approach requires consideration and anticipation that the implants may become sub-optimally positioned with continued jaw development, and the risk of splinting or undermining jaw growth in a lateral relationship.8,9 Furthermore, the ability to tolerate complex, invasive procedures and the psychological impact on patients at an early stage in life may pose the risk of inducing dental anxiety and breakdown in long-term dental engagement, which should be at the forefront of the decision-making process.
Treatment
At the outset, clear and comprehensive explanations of the denture construction stages are required, and anticipated difficulties that may be experienced were discussed to include both the parent/guardian and patient (Table 1).
Stage
Denture stages
Common difficulties for paediatric ED patients
1
Primary impressions
Patient may be aware of the smells, tastes, pressure, or tugging sensation of the impression materials
Difficulty in matching standard stock trays to small jaw size, therefore will require additional impressions to construct special trays in order to allow adequate impression to be captured
2
Master impressions
A customized tray is used to further capture anatomical structures, boundaries, and detail
The patient may notice some warmth when using softened compound materials, such as green stick
The patient may become more aware of any extension owing to their delicate mucosal lining
3
Record blocks
A vertical dimension of occlusion more than the patient can tolerate and an increased freeway space may be required or gradually transitioned
4
Trial tooth set-up
This stage may require repeating if it does not meet both the clinician's and patient's expectations
5
Denture delivery
Awareness of dentures inside the mouth
The dentures intentionally designed to capture and extend into parts of the mouth to help with retention, they may feel large or provoke gag response
Patient may find that retention initially is poorer than expected, which is hoped to improve as they build their confidence and develop neuromuscular control of the dentures
Patient may initially develop a lisp or spit while talking
Reassurance that young patients can adapt quickly with a number of these issues being transient only
Patients will require ongoing close review initially
6
Denture review with adjustments as necessary
Appropriate adjustments include occlusal corrections and temporary relining
Preliminary impressions were captured using modified stock trays with impression compound to capture the full sulcus depth and critical denture bearing anatomy: the hamular notches within the maxilla and retromolar pad areas including lingual pouches within the mandible.10 A quick-setting rigid material is preferable to achieve this outcome, and in our experience, softened brown compound meets these requirements. Silicone putty may also provide some benefit.
Master impressions were completed using silicone impression materials within laboratory-made special trays. Instructions to the laboratory to improve tray design could include the following:
Flange extension should be 2 mm short of the full sulcus depth;
Spacer to allow for final impression material, in this case silicone;
Incisal and tissue stops. Ensure the tray seats down evenly and in the same position each time;
Handle design and bilaterial rests: provide a tripod of support;
The master trays were assessed intra-orally and the correct sulcus depth captured using green stick border moulding technique. Within the maxilla, further attention was given to fully covering the hamular notches, and within the mandible, the tray was adapted to extend at least half way up the retromolar pad areas, as well as extended into the lingual pouches.11 The master tray, after adjustments, should represent the expected final denture fitting surface when completed as point of reference.12 The definitive master impressions were completed using a combination of medium- and light-bodied silicone impression materials (Extrude Extra, Extrude Wash, Kerr, CA, USA). The combination of different consistencies of the silicone material allowed greater control in capturing detail, without overcompression of the mucosa.
Temporary acrylic baseplates and wax rims were constructed to assess the retention and stability and helped to identify whether further interceptive orthodontics would be required within the maxillary arch to help with denture retention by orthodontically creating bounded saddles. In this case, the temporary acrylic bases confirmed that retention was optimal and no additional orthodontic treatment required. Calipers were used to ensure that the overdenture exceeded the minimal denture base thickness of 2 mm.13 Attention was provided in identifying a freeway space that allowed a sufficient thickness of material over the LR3–LL3 overdenture abutments. The blocks were finally trimmed to respect the freeway space, occlusal plane parallel to the alar-tragus line, lingual space and musculocutaneous profile.
A trial set-up confirmed optimal aesthetics, phonetics and a balanced occlusal scheme deemed to be ideal, with confirmation from the patient and parent.
The definitive dentures incorporated Y-shaped roach stainless-steel clasps without modifying the teeth using resin material so as to respect the patient's wishes. The modification of teeth may have allowed for further enhancement of the denture retention. Denture care advice and potential challenges were reinforced with routine follow-up to ensure comfort and adaptation to the prostheses, which was successful, with positive impacts on function, aesthetics, and daily usage.
Discussion
The role of denture treatment in young patients with ED provides a removable and non-invasive strategy to restore form, function and aesthetics. A removable prosthesis also allows the clinician to adjust and adapt the denture as the patient grows, without embarking upon significant treatment and without impact on jaw development.6 Challenges arise in achieving stability and retention owing to the shape of teeth, lack of occlusal contacts, malocclusions, decreased vertical dimension, abnormal mandibular posturing, atrophic alveolar ridges and delicate mucosal lining. Additionally, it should be noted that significant anatomical landmarks are underdeveloped in a paediatric patient compared to an adult, notably the retromolar pads and the hamular notches are smaller, less dense and less pronounced.
The fabricating procedure of dentures for the young patient, although not highly complex, requires the implementation and knowledge of fundamental prosthodontic principles for successful treatment outcomes. Strategies, as highlighted above, during provision of treatment allowed for successful outcomes and control of each stage. Additional points for consideration are also highlighted below and may assist practitioners when delivering removable prosthetics for young patients with ED:
At the outset and throughout treatment, a comprehensive discussion explaining the treatment stages and potential challenges is crucial. This allows the clinician to bolster trust, set expectations, inform consent, and importantly, enhance the patient's ability to engage and accommodate to treatment, while preserving long-term trust.
To enhance retention and stability of the removable prostheses, treatment aims were to enhance the distribution of mucosal support by extending the denture base into anatomically acceptable oral landmarks. This included capturing of the hamular notches within the maxilla and extension at least half-way up the retromolar pad areas and into the lingual pouches within the mandible.14 Despite the lack of alveolar ridge height and shallow oral vestibule in contrast to an adult, the correct extension and sulcus depth captured by green stick border moulded special trays had allowed for ideal support, retention, and stability of the dentures (Figure 3).
Although the atypical conical anterior lower teeth were not suitable for removable partial denture stability, they were used as overdenture abutments, with the added benefit of locally preserving alveolar bone and increasing proprioception.15
The lower permanent canines were distally inclined within the mandible resulting in undercuts and loss of intimacy with the fitting surface to optimise retention. If suboptimal, the canines could be further modified with resin, and internal clasps could be added to the denture.
The wrought clasps were Y-shaped to increase the surface area for contact on the conical canines to aid retention (Figure 4). Composite additions would provide further undercuts for the clasp head.
Reassurance that common denture challenges, such as lisps during speech and gag reflexes, would be expected to resolve as the patient continues to accommodate to the dentures. We had found that a close review had helped to encourage this process with positive outcomes.
Prosthesis replacement is expected while the paediatric patient continues to grow and complete their craniofacial development. Reports stipulate an additional three further attempts may be required until development is completed when undertaking denture treatment at a young age.16 Additionally, modifications, such as relining or rebasing of the removable prostheses, is recommended in line with growth.7 To aid this journey, excellent communication with the patient's parents or guardians is imperative to help inform decision making.
Figure 3. Upper partial acrylic and lower complete acrylic overdentureFigure 4.
(a) Intra-oral photos to show pre-operative malocclusion and overclosure. (b) The complete denture prosthesis given to the patient alters the alveolar height, bettered the musculocutaneous profile, increased occlusal vertical dimension leading to an aesthetic outcome.
Patient's perspective
The increase in the occlusal vertical dimension allowed for a positive impact on the facial profile and lip support, maximizing the aesthetic outcomes (Figure 1). Improvement in speech and phonetics were evidenced, enhancing social integration and confidence, which is mirrored in current literature.17 Attention to the fundamental denture principles with anticipation of challenges at the outset, allowed for enhanced tolerance and adaptation to the dentures, after previous attempts with limited outcomes.
It is paramount that treatment in young patients is only proceeded with if a positive response is maintained from the patient in order not to detract from their perceptions of dentistry for the long term. The long-term rehabilitative care of an ED patient offers opportunities for multidisciplinary collaboration among primary care practitioners, paediatric dentists, orthodontists, restorative dentists, prosthodontists and maxillofacial surgeons.13 If this is felt to be negatively affected, the treatment should be strategically abandoned until of age and maturity in order for it to proceed without negative consequences.
Conclusion
The oral rehabilitation of an ED patient with severe hypodontia involves replacing multiple missing teeth, restoring sagittal and vertical skeletal relationships during craniofacial development to reinstate form and function. In turn, this will improve the patient's quality of life and social integration. Overall, non-surgical prosthetic treatment, when executed with an appreciation of anatomical structures and knowledge of growth and development, can be regarded as a safe and predictable first-line treatment modality for functional and aesthetic oral rehabilitation for this cohort of patients.