Kassab MM, Cohen RE. The etiology and prevalence of gingival recession. J Am Dent Assoc. 2003; 134:220-225
O'Leary TJ, Drake RB, Crump PP, Allen MF. The incidence of recession in young males: a further study. J Periodontol. 1971; 42:264-267
Vehkalahti M. Occurrence of gingival recession in adults. J Periodontol. 1989; 60:599-603
Baker P, Spedding C. The aetiology of gingival recession. Dent Update. 2002; 29:59-62
Patel M, Nixon PJ, Chan MF. Gingival recession: Part 1. Aetiology and non-surgical management. Br Dent J. 2011; 211:251-254
Wennström JL. Mucogingival therapy. Ann Periodontol. 1996; 1:671-701
Tugnait A, Clerehugh V. Gingival recession – its significance and management. J Dent. 2001; 29:381-394
Al-Wahadni A, Linden GJ. Dentine hypersensitivity in Jordanian dental attenders. A case control study. J Clin Periodontol. 2002; 29:688-693
Lawrence HP, Hunt RJ, Beck JD. Three-year root caries incidence and risk modeling in older adults in North Carolina. J Public Health Dent. 1995; 55:69-78
Smith RG. Gingival recession. Reappraisal of an enigmatic condition and a new index for monitoring. J Clin Periodontol. 1997; 24:201-205
Zalkind M, Hochman N. Alternative method of conservative esthetic treatment for gingival recession. J Prosthet Dent. 1997; 77:561-563
Carvalho W, Barboza EP, Gouvea CV. The use of porcelain laminate veneers and a removable gingival prosthesis for a periodontally compromised patient: a clinical report. J Prosthet Dent. 2005; 93:315-317
Morgano SM, Verde MA, Haddad MJ. A fixed-detachable implant-supported prosthesis retained with precision attachments. J Prosthet Dent. 1993; 70:438-442
Günay H, Geurtsen W, Lührs AK. Conservative treatment of periodontal recessions with class V-defects using gingiva-shaded composite – a systematic treatment concept. Dent Update. 2011; 38:124-132
Alani A, Maglad A, Nohl F. The prosthetic management of gingival aesthetics. Br Dent J. 2011; 210:63-69
Hannon SM, Colvin CJ, Zurek DJ. Selective use of gingival-toned ceramics: case reports. Quintessence Int. 1994; 25:233-238
Blatz MB, Hürzeler MB, Strub JR. Reconstruction of the lost interproximal papilla: presentation of surgical and nonsurgical approaches. Int J Periodontics Restorative Dent. 1999; 19:395-406
Davis LG, Ashworth PD, Spriggs LS. Psychological effects of aesthetic dental treatment. J Dent. 1998; 26:547-554
Palmer RM, Ide M, Floyd PD. Clinical guide to periodontology: part 3. Multidisciplinary integrated treatment. Br Dent J. 2014; 216:567-573
Beckett HA, Wright PS. Construction of a gingival mask in association with an implant-retained fixed maxillary prosthesis – a case report. Eur J Prosthodont Rest Dent. 1993; 2:57-60
Greene PR. The flexible gingival mask: an aesthetic solution in periodontal practice. Br Dent J. 1998; 184:536-540
Barzilay I, Irene T. Gingival prostheses – a review. J Can Dent Assoc. 2003; 69:74-78
Clark D. Restoratively driven papilla regeneration: correcting the dreaded ‘black triangle’. Tex Dent J. 2008; 125::1112-1115
Gopakumar A, Sood B. Conservative management of gingival recession: the gingival veneer. J Esthet Restor Dent. 2012; 24:385-393
Blair FM, Thomason JM, Smith DG. The flange prosthesis. Dent Update. 1996; 23:196-199
Hickey B, Jauhar S. Gingival veneers. Dent Update. 2009; 36:422-428
Wray D, McCord JF. Labial veneers in the management of desquamative gingivitis. Oral Surg Oral Med Oral Pathol. 1987; 64:41-42
Aguiar GP, Jham BC, Magalhães CS, Sensi LG, Freire AR. A review of the biological and clinical aspects of radiation caries. J Contemp Dent Pract. 2009; 10:83-89
L'Estrange PR, Strahan JD. The wearing of acrylic periodontal veneers. Br Dent J. 1970; 128:193-194
Mekayarajjnanoth T, Kiat-amnuay S, Sooksuntisakoonchai N, Salinas TJ. The functional and esthetic deficit replaced with an acrylic resin gingival veneer. Quintessence Int. 2002; 33:91-94
Cura C, Saraçoglu A, Cötert HS. Alternative method for connecting a removable gingival extension and fixed partial denture: a clinical report. J Prosthet Dent. 2002; 88:1-3
Ellis SG, Sharma P, Harris IR. Case report: aesthetic management of a localised periodontal defect with a gingival veneer prosthesis. Eur J Prosthodont Rest Dent. 2000; 8:23-26
Aswal GS, Nair CK, Vishwanath G, Vishwanath S. Split impression technique to fabricate acrylic gingival veneer. Int J Res Dent. 2014; 4:109-116
Taylor C, Roudsari RV, Jawad S, Ashley MP, Darcey J. The aetiology and management of labial and vertical migration of maxillary incisors: ‘do you catch my drift?’. Br Dent J. 2014; 216:117-123
Martinez-Canut P, Carrasquer A, Magan R, Lorca A. A study on factors associated with pathologic tooth migration. J Clin Periodontol. 1997; 24:492-497
Towfighi PP, Brunsvold MA, Storey AT, Arnold RM, Willman DE, McMahan CA. Pathologic migration of anterior teeth in patients with moderate to severe periodontitis. J Periodontol. 1997; 68:967-972
Shifman A, Laufer BZ, Chweidan H. Posterior bite collapse – revisited. J Oral Rehabil. 1998; 25:376-385
Watkinson AC, Hathorn IS. Occlusion in the aetiology and management of upper anterior tooth migration. Restorative Dent. 1986; 2:56-61
Selwyn SL. An assessment of patients with periodontally involved migrated incisors. J Dent. 1973; 1:153-157
Witter DJ, Creugers NH, Kreulen CM, de Haan AF. Occlusal stability in shortened dental arches. J Dent Res. 2001; 80:432-436
Proffit WR. Equilibrium theory revisited: factors influencing position of the teeth. Angle Orthod. 1978; 48:175-186
Oh SL. An interdisciplinary treatment to manage pathologic tooth migration: a clinical report. J Prosthet Dent. 2011; 106:153-158
Gaumet PE, Brunsvold MI, McMahan CA. Spontaneous repositioning of pathologically migrated teeth. J Periodontol. 1999; 70:1177-1184
Jacobson N, Frank CA. The myth of instant orthodontics: an ethical quandary. J Am Dent Assoc. 2008; 139:424-434
The aesthetic prosthodontic management of periodontally involved teeth Dominic P Laverty David Green JJ Jansen Van Rensburg Dental Update 2025 45:9, 828-840.
Authors
Dominic PLaverty
ACF/StR in Restorative Dentistry, Birmingham Dental Hospital
There are a number of aesthetic issues that may occur as a result of periodontal disease and/or its management and it is a common motivation for patients to seek treatment, particularly when it affects the anterior teeth due to their prominence within the dentition. Clinicians and patients are becoming increasingly aware of the importance of the periodontal/muco-gingival tissues to provide an aesthetic smile and, as a result, this has led to the development of both surgical and prosthodontic techniques to improve or maintain the dental aesthetics. The aim of this article is to provide an overview of the prosthodontic solutions available to improve the aesthetics of retained periodontally involved teeth.
CPD/Clinical Relevance: To present an overview of the prosthodontic solutions available to improve the aesthetics of retained periodontally involved teeth.
Article
A number of aesthetic issues may occur as a result of periodontal disease and/or its management and these are a common motivation for patients to seek treatment,1 particularly when the anterior teeth are affected due to their prominence within the dentition.
Patients are becoming more aesthetically aware and are now seeking dental care not just to attain or maintain oral health but also for aesthetic reasons. It has been shown that an aesthetic smile improves patients' self-confidence and ability to interact in society and those that don't have what society perceives as a ‘normal smile’ may lead to a lack of confidence or self-esteem.2 Clinicians and patients are becoming increasingly aware of the importance of the periodontal/muco-gingival tissues to provide an aesthetic smile; a result of which has led to the development of both surgical and prosthodontic techniques to improve or maintain the dental aesthetics.3
There are a number of aesthetic issues that may present around periodontally involved teeth. These include pathological tooth movement leading to drifting or spacing of teeth (Figure 1), gingival recession leading to long clinical crowns, exposed root surfaces, exposure of restorative margins and the loss of the interdental papilla creating undesirable ‘black triangles’.
Figure 1. Compromised aesthetics after successful periodontal treatment with exposed root surfaces and loss of the interdental papilla leading to ‘black triangles’ interdentally of the upper and lower anterior teeth.
Once a patient has been diagnosed with periodontal disease, appropriate management should be initiated to minimize the loss of the periodontal tissues and the potential aesthetic issues that may ensue, alleviating the need for treatment in the first instance, which will never truly replace these lost tissues. These aesthetic issues may be managed in a variety of ways which include; periodontal, orthodontic or prosthodontic treatments, or a combination of these.4
Before consideration is given to any aesthetic treatment, the patient should be periodontally stable and able to maintain meticulous oral hygiene. If this is not the case, the treatment should be deferred, otherwise these treatments can be detrimental and exacerbate the periodontal condition, which in turn will result in early aesthetic failure of the treatment provided.
This article will discuss the aesthetic issues that present as a result of periodontal disease and a variety of prosthodontic solutions that can be utilized by clinicians to provide aesthetic improvement.
Gingival recession
Gingival recession has been defined as a clinical condition in which the marginal periodontal tissues are located apical to the cemento-enamel junction (CEJ), with concomitant exposure of the root surface.5 It is a common condition within the population,4,6 has been shown to be more prevalent with increasing age, and can occur in patients with both good and poor standards of oral hygiene.7,8
The aetiology of gingival recession is often multifactorial and includes:
Self-inflicted or iatrogenic causes including restorative, periodontal or orthodontic treatment.9,10
Figure 2. Localized gingival recession as a result of an overzealous toothbrushing habit.Figure 3.
(a, b) Gingival recession as a result of a traumatic overbite.
Gingival recession in periodontal patients is caused by the loss of the supporting bone around the tooth through an inflammatory reaction,5 resulting in apical migration of the soft tissue margin.8 These patients are likely to show generalized signs of recession on all surfaces of the teeth.7
Gingival recession can result in pain from dentine hypersensitivity,11 root caries,12 abrasion,13 fear of tooth loss14 and unfavourable aesthetics,14 particularly when this affects the teeth within the aesthetic zone and is especially true in patients with a high lip line that results in excessive gingival display.
The aim of the treatment for gingival recession should be to address the patient's concerns, which may be functional, related to sensitivity and/or due to aesthetics. Treatment options for gingival recession include:
Surgical augmentation;
Orthodontics; or
Prosthodontic treatment.
Surgical management of gingival recession is technique sensitive and can be unpredictable, particularly when the defect is severe and extensive involving multiple teeth. For some patients, surgery and orthodontics may not be amenable, acceptable or desirable and may be contra-indicated. In these cases, an alternative and more suitable option may be prosthodontic treatments which includes:8,11,15,16,17
Composite resin restorations;
Pink ceramics or pink composite resin restorations;
Removable gingival veneers.
Selecting the most appropriate aesthetic prosthetic treatment for teeth with gingival recession in the anterior region can be challenging. Careful assessment of the patient's lip line, gingival position and anatomic crown length are important factors to attain good aesthetic results.11
Patients with a high smile line, excessive gingival recession and loss of the interdental papilla with associated ‘black triangles’ can present obstacles to achieving an aesthetic outcome. The use of articulated study casts and wax-ups of the proposed restorations can help the clinician, patient and laboratory visualize the proposed end results to see whether treatment is amenable and acceptable to the patient before proceeding.
The aesthetic prosthodontic management of periodontally involved teeth
Pink composite
The use of a gingival shade composite to match adjacent soft tissues was first described by Zalkind and Hochman in the management of a cervical defect.11 Pink composite can be used to eliminate dentine hypersensitivity and to restore the lost gingival tissues aesthetically by placing pink composite directly onto the exposed root surface.8,18 The pink composite in this position restores the anatomical size of the crown of the tooth and minimizes/alleviates the long clinical crown height present.
This technique is minimally invasive, can be easily modified and replaced, and is particularly useful around crowned teeth with exposed root surfaces, thus alleviating the need for crown replacement.19 However, use of composite is technique sensitive and can be challenging due to difficulties in moisture control around the gingival tissues as a result of gingival crevicular fluid; it can also be a challenge to ensure that there are no ledges/overhangs of the restoration, which can act as a plaque retentive factor and lead to further recession.3 To minimize this, gingival retraction techniques (Figure 4) can be used and careful manipulation of the composite is required. In the two cases shown (Figures 5, 6 and 7), GC Composite Primer (GC Corporation, Tokyo, Japan) was used (which helps rebuild the inhibition layer for bonding between composite layers and also can be used to lubricate the instruments and reduce the composite ‘sticking’ to the instruments), along with GC Gradia Brush Flat No 1 (GC Corporation, Tokyo, Japan) (Figure 8) and very thin-bladed composite instruments to manipulate the composite, which is particularly useful at the gingival margin.
Figure 4. Gingival retraction using retraction cord prior to direct pink composite placement.Figure 5.
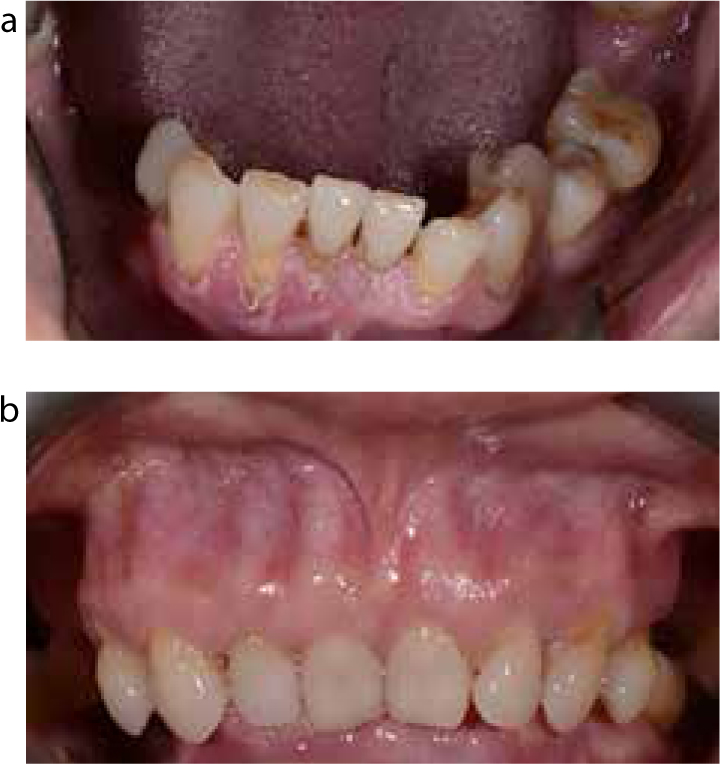
(a, b) Pre-op views prior to direct pink composite placement of upper and lower anterior teeth.Figure 6.
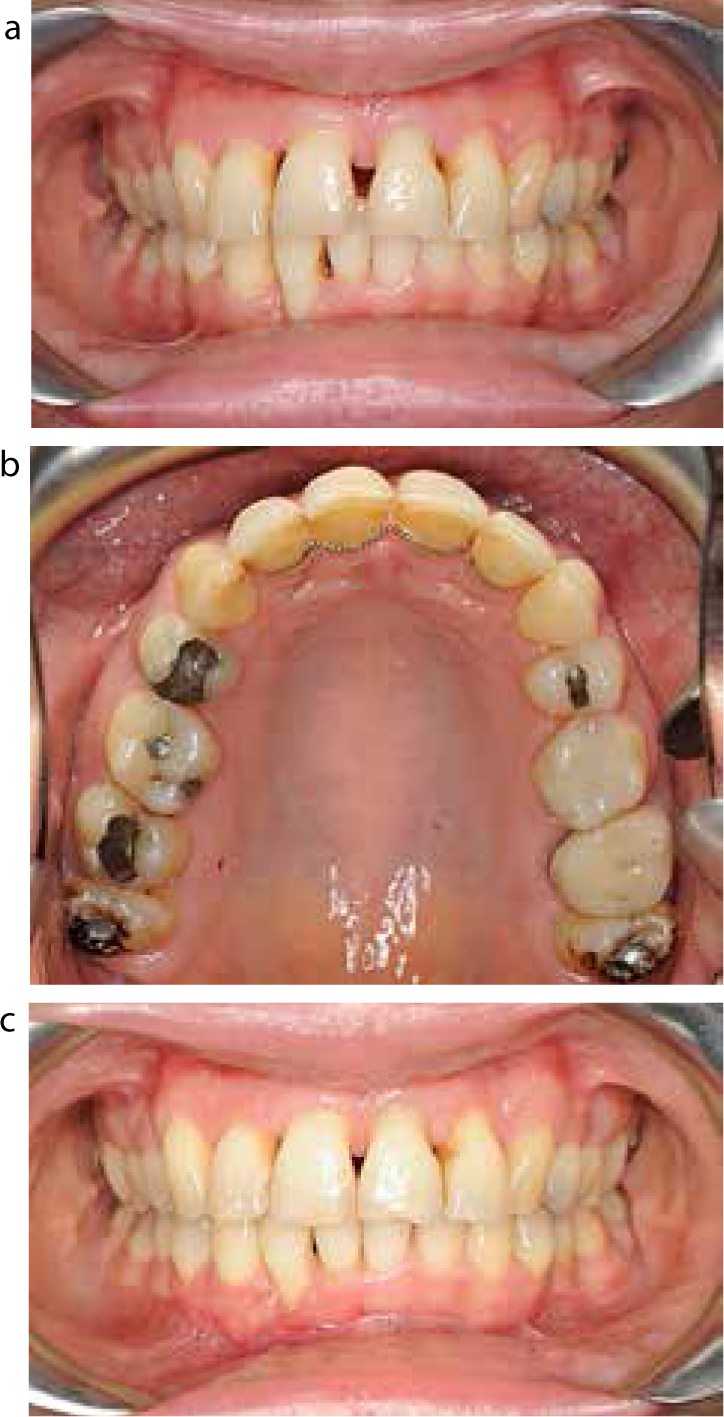
(a–c) Immediate and 18 months post-op views of direct pink composite placement of upper and lower anterior teeth using Gradia Gum Shade Composite GC (GC Corporation, Tokyo, Japan).Figure 7.
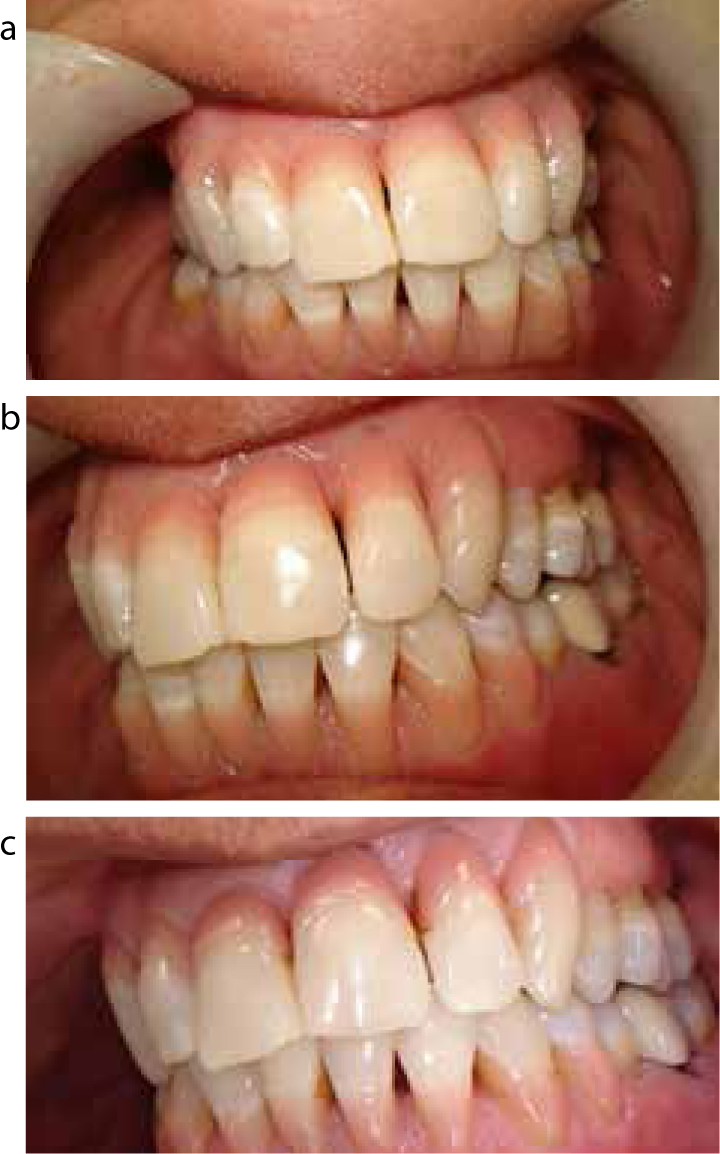
(a, b) Pre- and post-op views of direct pink composite placement of upper anterior teeth using Gradia Gum Shade Composite GC (GC Corporation, Tokyo, Japan). Note the teeth were splinted with everStick Perio GC (GC Corporation, Tokyo, Japan), a fibre-reinforced composite splint, prior to composite placement.Figure 8.
(a, b) GC Composite Primer (GC Corporation, Tokyo, Japan) and GC Gradia Brush Flat No 1 (GC Corporation, Tokyo, Japan) which can be useful to manipulate composite on direct placement.
There are some aesthetic issues with using pink composite for the treatment of gingival recession; one of the main issues being the lack of shades available.8 The lack of shades and the limits of this treatment modality may not provide the desired aesthetics and may be aesthetically undesirable for some patients. Careful case selection and a mock trial in the mouth can help assess these potential aesthetic issues before proceeding with treatment. One way to assess this is to place a small amount of the pink composite onto the root of the tooth and light curing without any preparation of the tooth to assess the shade matching and the rough aesthetics briefly before proceeding (Figure 9).
Figure 9. Mock-up using different shades of Gradia Gum Shade Composite GC (GC Corporation, Tokyo, Japan) to assess the most appropriate shade prior to definitive placement. Three different shades were used: shades G21, G22 and G23. After curing the three ‘mock-up’ restorations it was clear that the shade G23 blended in the best with the patient's shade of gingiva.
Pink porcelain
Where extra-coronal restorations are provided for teeth with recession, gingival coloured/pink porcelain can be incorporated into extra-coronal restorations.16,20 This may, however, lead to excessive tooth tissue removal and also lead to the restorative margins being placed onto the root dentine as the preparation extends down onto the root surface.
The clinical process involved is the same as for any extra-coronal restoration, except that a clinical decision of where the laboratory should place the pink porcelain should be communicated clearly to the laboratory and careful cementation of the extra-coronal restoration is required to ensure that the cement lute doesn't encroach on the gingival margin/sulcus.3 The technical work by the laboratory needs to be carefully carried out like any other extra-coronal restoration to ensure an optimal marginal fit without any ledges, as this can act as a plaque retentive factor and lead to further recession.
The use of extra-coronal restorations can be excessively destructive of tooth tissue and can compromise pulpal health,3 and they are also more difficult to refurbish and replace in comparison to direct restorations. There can also be aesthetic issues associated with the use of pink porcelain which is the same as with direct pink composite, which includes the lack of pink porcelain shades and the potential unpleasing aesthetics that it provides; again, this should be discussed and envisaged with the patient before preparation of the tooth/teeth.
Composite resin restorations
Composite can be used to cover sensitive root dentine or used to modify the shape/contour of the teeth. Using composite on the root surface will inevitably lead to longer clinical crown height which may not be aesthetically acceptable to all patients. It can also be used to modify the contour/shape of the teeth and may be particularly useful where there has been loss of the interdental papilla. By reshaping the contours of the teeth, the contact point can be lengthened and located more apically, which in turn will reduce the embrasure/‘black triangles’ and, in some cases, can allow the coronal displacement of the interdental gingiva.21,22
However, there are limits to what this technique can achieve and it is often only used in milder cases when few teeth are involved. A more optimal outcome may be achieved with use of gingival veneers or pink composite, where gingival recession is extensive or generalized through the dentition.
Gingival veneer
Gingival veneers, also termed gingival masks,23 gingival slips, flange prostheses24 and removable gingival prostheses,15 are a removable prosthesis worn on the labial aspect of the dental arch, which aims to restore the muco-gingival contour and aesthetics in areas where periodontal tissues are deficient.25 They may be used to replace tissue lost as a result of periodontal disease, surgical periodontal procedures, trauma, ridge resorption or traumatic tooth extraction, which can result in aesthetic and functional deficit.26
Gingival veneers are indicated in cases when the aesthetics are compromised, which include disproportionately elongated clinical crowns, visible crown margins and exposed root surfaces.27 They are particularly useful in patients that have lost the interdental papillae, leading to unsightly ‘black triangles’ between the teeth (Figures 1 and 10).28 Functionally, they can be used to improve speech and phonetics by reducing air escape through interdental spaces,23 and also act as a barrier to stop saliva passing interdentally, which can create foaming of saliva or spitting during speech.29 They are also particularly useful in patients where periodontal surgery to correct these deficits is not amenable, predictable, not wanted by the patient or contra-indicated.
Figure 10. Compromised aesthetics after successful periodontal treatment with exposed root surfaces, exposure of crown margins and loss of the interdental papilla leading to ‘black triangles’.
Gingival veneers can also be used to deliver local medicaments, which include desensitizing agents for the management of dentine hypersensitivity of exposed root surfaces,24 steroid medicaments against affected mucosa in patients with desquamative gingivitis,30 placement of fluoride supplements in head and neck cancer patients after radiotherapy who are at high risk of root caries,31 and can also be used to deliver periodontal dressings.32
Gingival veneers, however, are contra-indicated in patients with uncontrolled periodontal disease or incomplete periodontal therapy, an allergy to acrylic or silicone, poor manual dexterity or patients at risk of inhalation.23 They are also contra-indicated in patients who have a high caries susceptibility and those patients that are unable to maintain meticulous oral hygiene,23 as the veneer will retain more plaque like any removable prosthesis.
The prosthesis can be fabricated from composite resins, porcelain, acrylic (Figure 11) and silicone (Figure 12) materials. Traditionally, acrylic26 was the most commonly used material (Figure 13), however, silicone is becoming increasingly24 used due to its improved aesthetics and flexibility, which makes the prosthesis more comfortable for the patient to wear (Figures 14 and 15).29
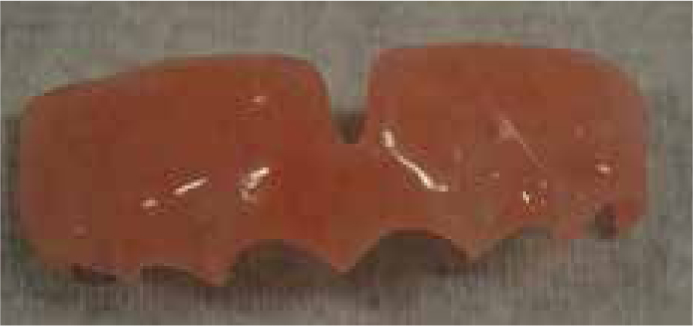
Figure 11. Acrylic gingival veneer.Figure 12. Silicone gingival veneer.Figure 13.
(a, b) Patient with and without an acrylic gingival veneer with sub-optimal fit, which the patient has struggled to cope with.Figure 14.
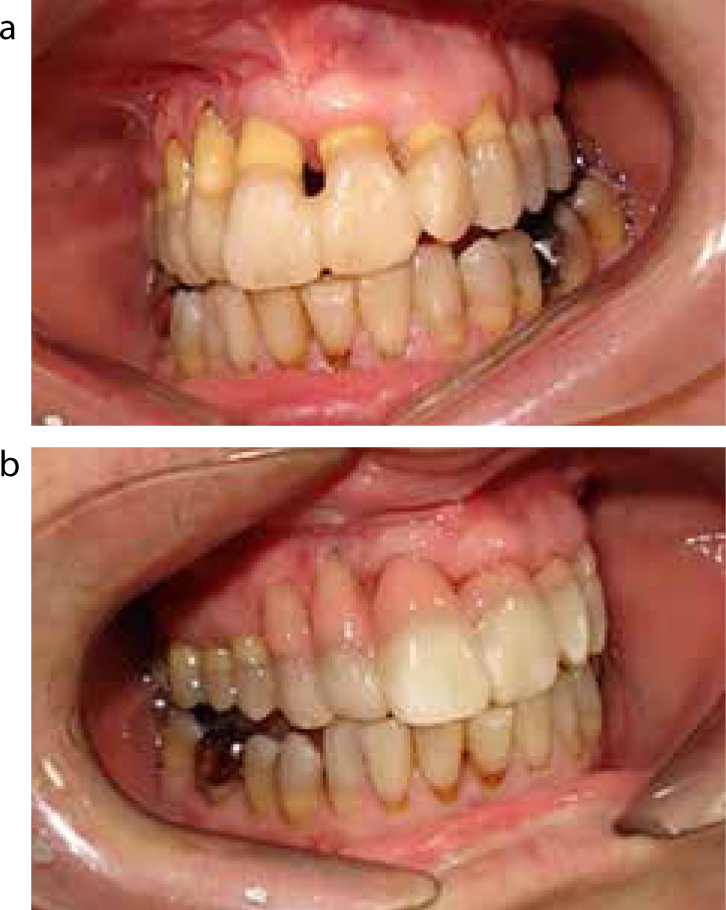
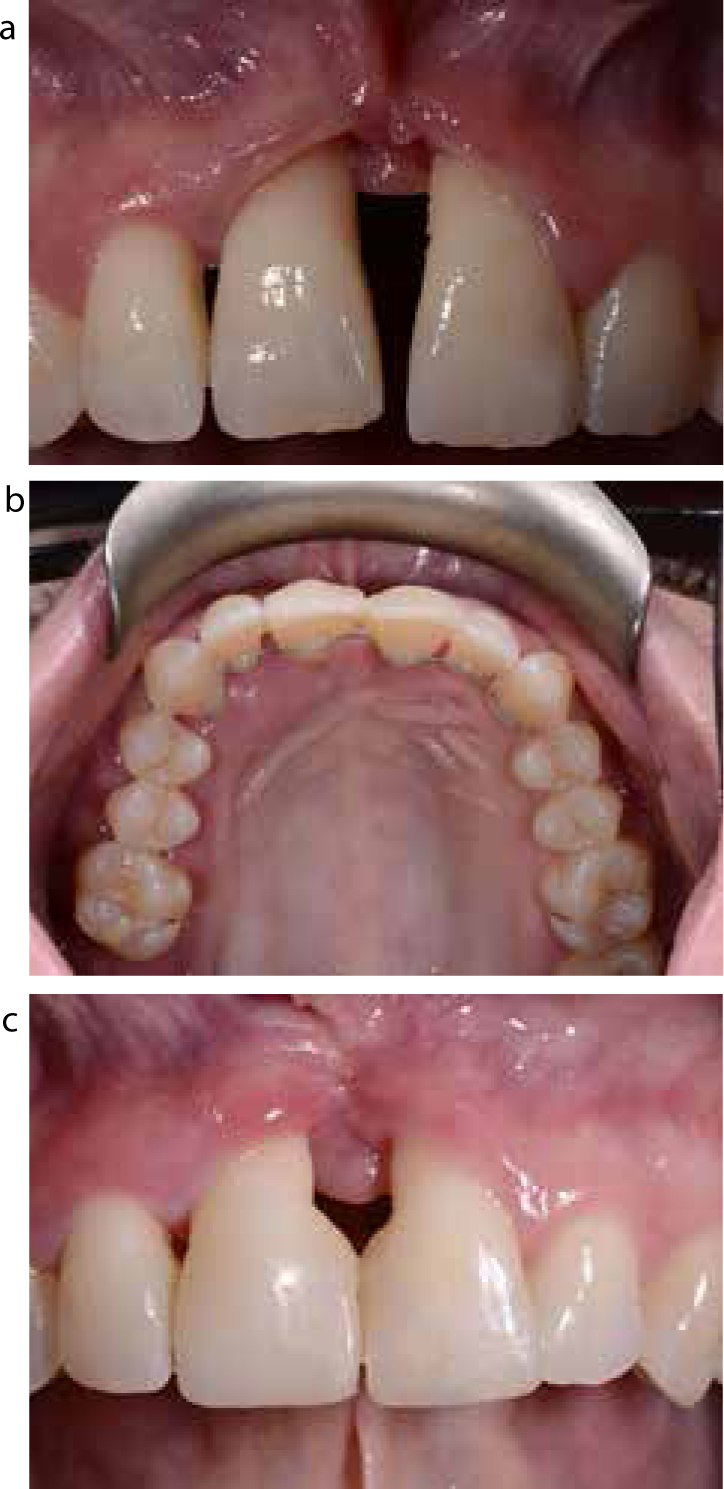
(a, b) Pre- and post-op views showing the use of a maxillary silicone gingival veneer in the management of ‘black triangles’, exposed root surfaces and visible crown margins. (Same patient as in Figure 10.)Figure 15.
(a–d) Pre-post-op views showing the use of upper and lower silicone gingival veneers predominately in the management of ‘black triangles’.
The gingival veneers are retained by mechanical and/or adhesive forces. Mechanically they are retained by engaging the interproximal undercuts24 and around the distal aspect of the terminal abutment teeth23 (Figure 16). Due to this, there should be a delay of at least three months after successful periodontal treatment to allow stabilization of the gingival tissues and the teeth, otherwise the veneers will become readily loose and non-functional.32 Gingival veneers can be used with the natural dentition or used in conjunction with fixed prosthesis,15 including implant-retained prostheses,27,33 and can even be incorporated into the fixed prosthesis using precision attachments to help retain the gingival veneer.27,34 However, this can be complicated and challenging both clinically and technically, particularly when it requires replacement.
Figure 16.
(a) Silicone and (b) acrylic gingival veneer showing engagement with the interdental spaces and distal abutment teeth. Note: due to the silicone properties of being flexible, the prosthesis is able to engage further into interdental space than with an acrylic veneer.
The gingival veneer can be fabricated either directly or indirectly.27 The direct technique involves construction of the gingival veneer chairside by the clinician. This technique is not commonly used to produce the definitive gingival veneer and is more commonly used to construct a temporary veneer or used for diagnostic purposes to assess the aesthetics and function with the patient prior to construction of a definitive indirect veneer.29 Silicone is often used for this technique32 and is placed directly and manipulated into the desired prosthesis. The indirect technique35 involves taking an impression that captures the interproximal spaces and the full depth and width of the sulcus for the span of the planned veneer (Figures 17, 18 and 19). This can be carried out using a modified stock tray or using a specifically designed special tray24,29,36 (Figure 20).
Figure 17. Putty (addition cure silicone) impression of palatal aspect of the teeth extended slightly past the extension of the proposed gingival veneer, which prevents the labial impression from engaging the undercut palatally and tearing on removal.Figure 18. Split impression technique: putty (addition cure silicone) palatal impression (light blue) to stop the impression material engaging the palatal undercut, and medium-bodied (addition cure silicone) labial impression (brown) in a special tray.Figure 19. Casting using the splint impression technique (from impression in Figure 18).Figure 20.
(a, b) Special spaced perforated ‘labial’ tray for gingival veneer. Note the perforations of the tray that help to retain the impression material mechanically in the tray on removal of the impression.
The gingival veneer is a relatively straightforward and predictable approach to replacing lost tissue architecture, especially when a large volume of tissue needs replacement, and has been shown to have little or no detrimental effect on the gingival tissues in the long term in motivated patients.15,29,36 However, the prosthesis is removable, which for some patients may not be acceptable, and aesthetics can be compromised in some patients due to a lack of shade availability of some of the materials (Figure 21). Overall, the prosthesis can offer a good long-term solution or be used as an interim solution for patients who may wish to have time to consider their options of more advanced and complex treatment.
Figure 21. Acrylic shade guide.
Pathological tooth migration
Drifting or spacing of the teeth, particularly the maxillary anterior teeth, is a frequent complaint of patients with periodontitis. Careful assessment and correct diagnosis of the cause is vital before treatment is embarked upon. Often the cause is multifactorial and may be related to: periodontal, orthodontic and/or restorative/occlusal causes.4 The position of teeth is maintained by a complex interplay of forces of both the hard and soft tissues, and when this equilibrium is lost, unwanted tooth movement can occur.37
This equilibrium can be disturbed by periodontal disease, which is the most influential factor related to unwanted tooth movement.37 Where this is directly attributed to periodontal disease, this can be termed pathologic tooth migration (PTM)38 and can create aesthetic and functional issues.
This unwanted tooth movement appears to have high prevalence, ranging from 30–55% in patients with periodontal disease1,39 and is a common motivation for patients to seek treatment.1 The aetiology of PTM appears to be multifactorial and includes the degree of periodontal bone loss,38 gingival inflammation,38 posterior overclosure or a lack of posterior support,4,40 occlusal interferences/trauma,37,41 patients with Class II malocclusions,42 patients with parafunctional habits,37 a shortened dental arch,43 and unfavourable soft tissues that exert pressure on the teeth.44
When dealing with patients with this condition the patient's concerns must be identified, which often include aesthetic and/or functional concerns or a concern that the condition will worsen. The most common concern is related to aesthetics, with complaints from periodontal patients being that teeth have moved into unusual positions or that spacing has appeared between the teeth as a result of splaying. Understanding what issues the patient has is important so that these can be incorporated into the decision-making process when planning treatment to see whether the patient's complaint/expectations can be met or not.
Treatment of PTM often requires a multidisciplinary approach, which includes periodontal, orthodontic and restorative treatment, depending on the periodontal involvement of the migrated teeth.45 The treatment can vary from extraction and replacement of the missing teeth at one extreme, to the spontaneous repositioning as a result of stabilization of the patient's periodontal condition.46 The most important factor before embarking on orthodontic or restorative treatment is that the patient is periodontally stable.
Extraction and tooth replacement with either: a removable prosthesis, fixed prosthesis or fixed or removable implant-retained prosthesis;
A combination of the above.
Figure 22.
(a–c) Pre- and post-orthodontic treatment to close diastemas of the upper and lower anterior teeth (upper fixed retainer in situ post-orthodontic treatment to prevent relapse) as a result of pathological tooth migration.
The restorative management is part of the focus of this paper and other available treatment options are discussed in other relevant articles.5,7,16,37 The restorative management can be used to camouflage the affected teeth or used to replace affected teeth that have been extracted. Camouflaging the teeth involves modifying the affected teeth to improve the aesthetics. This can be carried out with direct or indirect restorations. The ability to camouflage teeth restoratively is dependent on a number of factors, which includes the degree of displacement, the status of the current tooth (eg endodontically treated or not), and the position of the patient's smile line. Teeth that are excessively displaced outside of the prosthodontic envelope may not be amenable to prosthodontic modification and other alternative treatment options may need to be explored.37
This process can be planned more accurately with the use of articulated study casts which have been diagnostically waxed-up to help the clinician, patient and laboratory team visualize the proposed end results. It can assist in the assessment of whether the treatment is viable, the degree of modification of the teeth, and whether the treatment is acceptable to the patient before proceeding. Treatment, where possible, should be predictable, conservative and preserve healthy tooth structure.47
Direct restorations
Direct restorations of affected teeth can be carried out with the use of direct composite resin restorations. This is a minimally invasive conservative treatment option and can be used to recontour teeth and help close gaps between the teeth, including ‘black triangles’. However, as a result of the modification to close the diastema, the teeth often appear ‘squarer’ in appearance; despite this, the aesthetics of the teeth is often greatly improved (Figure 23). Use of direct composite is technique sensitive and can take considerable time clinically to carry out. Careful placement of the composite restoration is essential to ensure that there are no plaque retentive margins which can promote further gingival recession. There are also maintenance issues and the need for replacement or repair, like any other direct composite restoration. Bonding may also be an issue when placed onto cementum or dentine and, as such, may result in higher rates of restoration debond. A wax-up of the proposed addition to the teeth and construction of a stent can help assist the clinician in the placement of such restorations. In some cases, using tooth-coloured composite in this way may not be aesthetically acceptable and alternative options would need to be considered to restore the aesthetics.
Figure 23.
(a–c) Pre- and post-op views showing the use of direct composite to close the diastema between the upper central incisors which occurred as a result of splaying due to periodontal disease. The patient had a favourable low lip line so that the composite placement is minimized to allow optimal oral hygiene. (The upper anterior teeth were splinted with orthodontic wire and direct composite to minimize the mobility and prevent further splaying.)
Indirect restorations
Indirect restoration with the use of veneers and crowns can be used to help camouflage displaced teeth; however, this is a more destructive treatment option, but may be the only option where teeth have previously been restored with indirect restorations.37 When placing an indirect restoration, careful consideration must be taken. Drifting of the anterior teeth in periodontally affected patients leads to hyper-eruption and labial displacement (Figure 24). To bring these displaced teeth back into the dental arch with an indirect restoration, heavy preparation of the labial and incisal tooth surfaces may be required. This may not be possible with overly displaced teeth, with excessive tooth tissue removal leading to an increased likelihood of pulpal complications, weakening of the tooth structure making it liable to fracture, and compromising the retention and resistance form of the preparation. Therefore careful planning and discussions with the patient about these risks is required before proceeding with treatment.
Figure 24.
(a–g) Pre- and post-restorative camouflage of the UR2 using an indirect restoration as the tooth had migrated labially and incisally as a result of pathological tooth migration. The tooth was able to be brought back into the dental arch successfully.
Conclusion
Patients are becoming more aesthetically aware of their dentition and it is expected that patients will present to their general dental practitioner with aesthetic issues associated with periodontal disease. Treatment must be aimed at controlling and stabilizing the patient's periodontal condition before embarking on any aesthetic treatment, as this treatment can exacerbate or accelerate his/her periodontal condition or compromise or lead to failure of the aesthetic treatment provided. This aesthetic management can be challenging and may require the use of multiple dental disciplines. A variety of treatment options are available, including prosthodontic solutions, which have been briefly described in this article.