Dental radiography is usually straightforward; however, a few patients do offer a greater challenge to the dentist aiming to achieve diagnostic images. Ironically, it is frequently these tricky patients where a good quality radiograph will be of greatest use when treatment planning. This article has been written primarily to provide some tips aimed at increasing the likelihood of achieving a diagnostic image for a patient who finds the procedure difficult and includes some techniques that can be applied to all patients having a dental radiograph taken.
CPD/Clinical Relevance: Achieving good quality radiographs is essential to aid in both diagnosis and treatment planning.
Article
Dental radiography is an essential component of undergraduate training. All newly registered dentists must have obtained the knowledge and skill to undertake intra-oral imaging and produce a good standard of dental panoramic tomograph (DPT) as an undergraduate. Subsequent working environments (from vocational trainee onwards) will have an influence on whether a dentist's skill in radiography is enhanced by frequent practice, maintained by a modest degree of practice or gradually lost as little or no practice of radiography is undertaken.
Achieving good quality radiographs is essential to aid in both diagnosis and treatment. Taking dental radiographs is usually a straightforward procedure; however, a few patients do offer a greater challenge to the dentist aiming to achieve diagnostic images. Ironically, it is frequently these tricky patients where a good quality radiograph will be of greatest use when treatment planning. This article has been written primarily to provide some tips aimed at increasing the likelihood of achieving a diagnostic image for a patient who finds the procedure difficult and includes some advice that can be applied to all patients having a dental radiograph taken.
Patients who find dental radiography challenging fall into one or more of the following categories:
Anatomical: very small mouth, tori present or missing teeth;
Learning differences;
Patient's mobility challenges: limited movement, eg congenital or certain chronic diseases.
Each of these categories will be discussed in turn. The final part of this article will detail less commonly used techniques that should enhance the likelihood of achieving a diagnostic image.
1. Physical issues
Gag (pharyngeal) reflex is a protective mechanism to ensure that the airway remains clear of obstruction. In dental imaging it is common to find those with a hypersensitive reflex find it challenging to tolerate the imaging holders and/or receptor being placed in their mouth. The most sensitive areas are usually the soft palate and the posterior lateral third of the tongue.1
When imaging a patient for whom gag reflex is likely to be an issue, equipment preparation and operator composure are key. Have the patient sitting upright with their chin slightly down to prevent the receptor slipping to the back of the mouth where it is more likely to initiate the gag reflex.
Some patients have already concluded that it will not be possible for them to comply with dental imaging as soon as the subject is mentioned. This is when the dentist and nurse must remain quietly confident, offering re-assurance that the patient's concerns can be carefully managed, and imaging will be successfully achieved. Often, those with the most severe problems wish an attempt to be made as they are aware of the advantage the images will have on their treatment planning.
In addition to preparing the receptor and holder, have the dental unit switched on, exposure selected, tube head close to the patient and the collimator in the correct orientation. It may seem contradictory to use intra-oral holders in this situation; however, personal experience has shown that for most patients, if the gag reflex can be overcome with distraction techniques, the paralleling method causes least distress for the patient, producing a more diagnostic image. This is purely due to the reality that many practitioners have lost their skill at producing good quality bisecting angle images as a result of the move to paralleling.
The two distraction techniques that have proven most effective within the imaging department are asking the patient to raise their lower leg so that their knee is straight, holding it in that position for the duration of the radiograph being taken, and secondly, to concentrate on their breathing. For the gag reflex to be initiated respiration must be suspended, so in theory if the patient is breathing continually, they will avoid gagging. The gag reflex is often worse when a patient is tired2 or fatigued, therefore, consider taking radiographs early in the day and, if practicable, before a prolonged session of dental treatment.
When using the paralleling technique take great care to prevent the holder and receptor contacting the tissues until the last possible moment. This is particularly important when imaging maxillary molars. Gently place the holder almost in the midline of the mouth, once the correct mesio-distal placement is obtained, bring the receptor into contact with the palatal tissues in one gentle movement. If you require several images, begin with the anterior teeth, leaving maxillary molars until last.
Employing the bisecting angle technique (see section 5) may be more acceptable to a patient with a strong gag reflex as a method of achieving periapical radiographs. The technique relies on the patient holding the receptor in the correct position and maintaining this for the 10–20 seconds it takes for you to position the tube head and make the exposure. Often the patient will subconsciously allow the receptor to move to a ‘more comfortable’ position, which is less likely to affect their gag reflex. This results in a non-diagnostic image and a repeat exposure, causing further distress to your patient, therefore stress the importance of maintaining the receptor position where you have placed it. Touching your finger on the area of the patient's palate that will be in contact with the receptor should demonstrate to the patient where they need to immobilize the receptor and may also desensitize the tissue for a short time.
The use of topical local anaesthetic to reduce the sensitivity of the patient's mouth has been well documented.3 Lidocaine ointment 5% or lidocaine 10-mg spray are two such preparations described in the British National Formulary4 for use in dental practice. The author is not registered to prescribe medicines so does not have personal experience of using such preparations.
If you have only limited practice in using the bisecting angle technique, you must question whether you can justify an attempt on a patient who finds dental imaging distressing.
Tongue
Several patients have a very strong tongue over which they have no conscious control. Unfortunately, this makes positioning a radiographic holder quite challenging, particularly noticeable when taking bitewing images. Asking the patient to put their tongue into the opposite cheek is not usually the best option as in doing this the muscle becomes more rigid, causing greater resistance to holder placement. For periapical images, take time to ensure the imaging receptor is seated securely within the biteblock to reduce the potential for it becoming dislodged by the patient's tongue.
A very small number of patients have a tongue reflex that is so strong that it proves impossible to place an X-ray holder into their mouth. If imaging is essential to aid diagnosis, then a DPT is your compromise.
Low pain tolerance
Taking radiographs for patients who have a low pain threshold is almost always achievable. Once you have explained what is involved, impress on your patient that you understand their anxiety and will do your best to minimize any discomfort to them. Exercise similar care as you would for patients with a strong gag reflex. It is always in your patient's best interest to achieve a diagnostic image without having to have a second attempt. If you feel it is appropriate, then explain this, because you are likely to gain a greater degree of co-operation.
If you intend to take bitewings or images of mandibular molars using phosphor plates, run your thumb and forefinger along the free edge of the barrier envelope, telling your patient that this may soften the plastic of the envelope. There is no proof as to its efficacy, but experience has shown this results in gaining the psychological upper hand. When you have placed the biteblock in contact with the occlusal surface of the mandibular teeth, ask your patient to bring their teeth together slowly, allowing the floor of the mouth to relax.
If the image you require is of a single tooth, consider whether a smaller receptor might be used. It is possible, with careful positioning, to image a molar tooth with a size 0 phosphor plate using the paralleling technique (Figure 2).
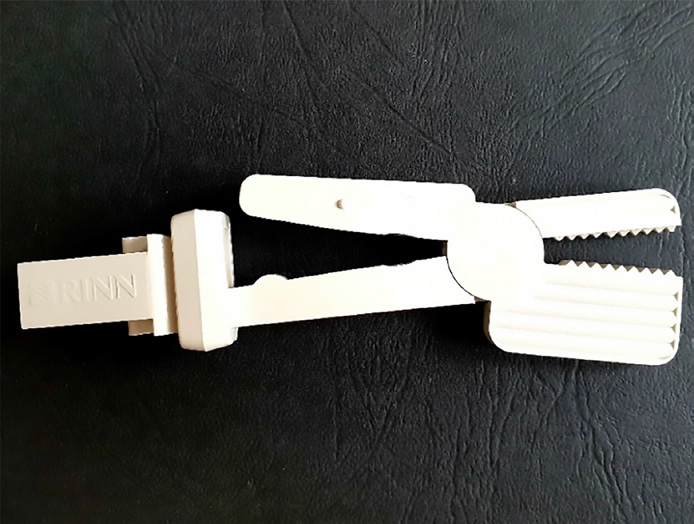
Figure 1. RINN Snap-A-Ray.
Trismus
When taking intra-oral radiographs it is essential that the patient is able to open their mouth to allow the holder and receptor to be positioned correctly. Patients suffering from trismus, therefore, require modification to the standard imaging techniques.
To obtain a periapical radiograph, the most likely modification is to use a bisecting angle technique (see section 5). Before commencing, ensure that your patient will be able to open their mouth enough to allow them to place their finger in their mouth to stabilize the receptor. An alternative to this would be the use of scissor-like holder such as the RINN Snap-A-Ray (Rinn Corporation, York, PA, USA) (Figure 1). Either end of the device can hold a phosphor plate (or film), with your patient stabilizing the device by holding the opposite end. Be mindful that the toothed end of the holder may cause permanent damage to the area of the phosphor plate with which it is in contact.
Figure 2.
(a) Size 2 plate, the corners have become bent on the palate. (b) Size 0 plate (in portrait orientation) has been used to image UR6.
Where mouth opening is severely restricted you may still be able to image incisors and canines using a modified occlusal technique (see section 5). This technique generally works well when using phosphor plates (or film), the additional thickness of solid-state detectors may make this examination more uncomfortable for your patient.
For bitewings, the use of bitewing tabs is an alternative option, although you will be relying on the patient's ability to self-position a size 2 (or size 1) plate with the tab attached. You must be certain that the receptor is in the correct position – the anterior edge of the plate should be adjacent to the middle of the first maxillary premolar. With the receptor in position, if you are unable to see the occlusal portion of the tab, centre the tube head approximately 1.5 cm posterior to the oral commissure in the line of the occlusal plane (+10) and parallel to the molar dentition.
2. Anatomical issues
Small mouth
It is usually possible to use standard size holders for adult patients with small mouths. Some adaption of technique may be required for periapical images of maxillary molars and anterior teeth along with bitewings.
When imaging maxillary molars, position the receptor close to the midline of the palate, exploiting the height of the palate at this point. If using a phosphor plate it is important to check that the plate does not become bent on the palate (Figure 2). Figure 2a demonstrates the corners of a size 2 plate being bent by the palate. By using a size 0 plate, despite the slightly greater length the decreased width has prevented the corners from becoming bent. If necessary allow the biteblock to tip slightly, anything below +20° should not have a detrimental effect on the image. It may be possible to obtain an image using a size 1 plate (placed in landscape orientation), although this is dependent on the length of the tooth's roots.
For imaging of incisors where a size 0 receptor in portrait orientation is too long and bending, consider using a modified occlusal technique (see later section). Bitewing images can be achieved using a size 1 receptor, although a small area of detail due to the smaller receptor size is lost. It will be necessary to use a paediatric bite block that accommodates the reduced width of the phosphor plate.
Tori
Tori are benign localized overgrowths of bone found in both the upper and lower jaws, resulting in an increased radio-opacity in the region.5
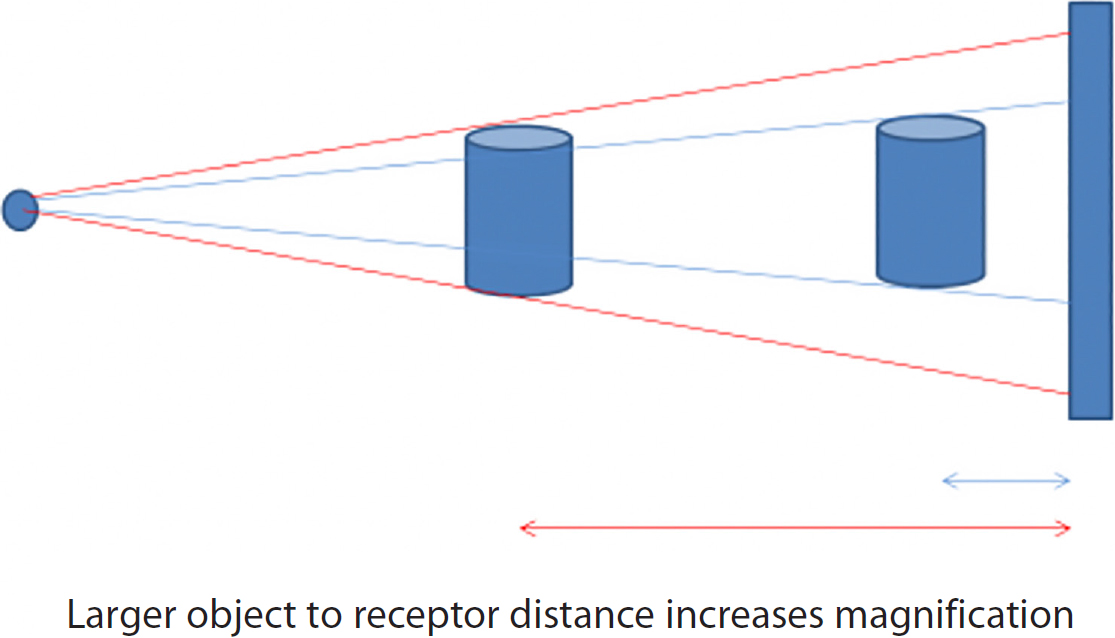
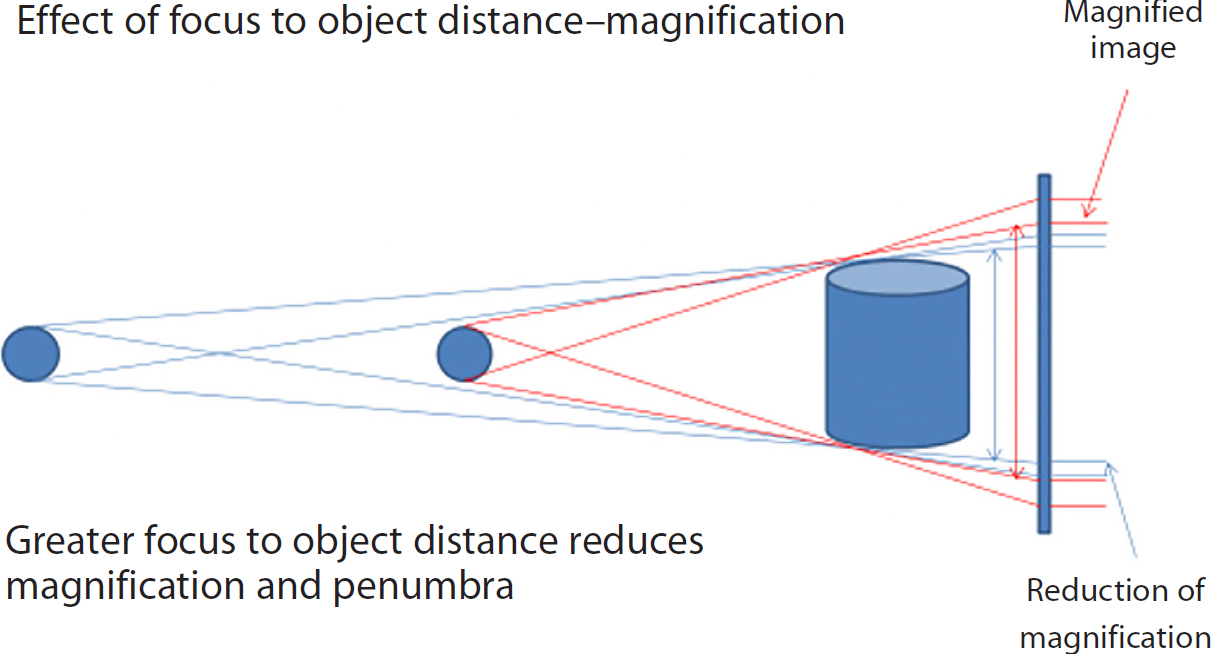
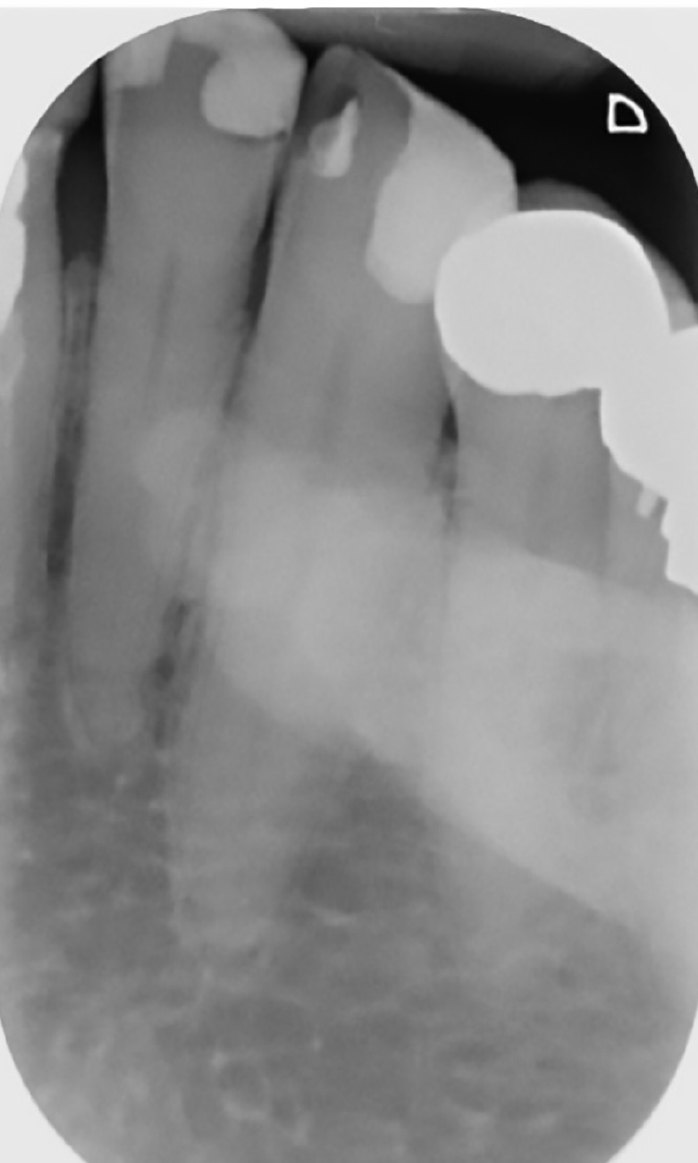
When taking images of a patient who has developed tori, the receptor must avoid resting on a torus. If a patient has a maxillary midline torus it may be necessary to place the receptor and bite block on the far side of the torus to prevent impingement on the tori and bending of the imaging plate. For patients with a mandibular torus the receptor and bite block must be placed lingually to the torus, so they avoid any impingement. In both cases, there will be a slightly larger object to receptor distance that will increase magnification (Figure 3). This change in geometry may mean some of the area you wish to image will not be included. To compensate for magnification, make a small increase to the distance between the tube head and the skin surface (Figure 4), simply by keeping the aiming ring approximately 0.5 cm further away from the patient's skin surface. Any tori will be visualized on the image as a radio-opaque region (Figure 5).
Figure 3. Magnification caused by increased object to receptor distance due to tori.Figure 4. Increasing focus to object distance reduces magnification of the object.Figure 5. Periapical radiograph of LL2, 3 and 4. The radio-opaque area partially obscuring the roots is caused by a torus.
Missing teeth
It can be challenging to achieve a diagnostic periapical image of a lone standing tooth, especially if there is no opposing tooth. This is found most often with mandibular premolars, canines and incisors. The absence of adjacent teeth often allows the tooth to realign at an oblique angle, requiring an educated estimation of the position of the apex in relation to the crown of the tooth. If there is no opposing tooth, but the patient has a well-fitting denture on the opposite arch encourage them to leave their prosthesis in situ. This should help to maintain the position of the biteblock once placed in the patient's mouth.
When placing the imaging receptor adjacent to the tooth of interest the receptor has a tendency to move clear of the tooth as soon as the patient closes their mouth to immobilize the bite block. To overcome this, reposition the biteblock to the area required, then ask your patient to hold the arm of the positioning device between their thumb and forefinger. Check that the biteblock remains in the region of interest, ensuring that the patient's hand will not obscure the image and is kept as far away from the X-ray beam as physically possible. (Think of the way one would hold the handle of a small china teacup). The very small dose of mostly scattered radiation to the patient's hand is justified by the potential reduction in overall dose as a repeat image should not be required. A cotton roll can also be used to stabilize the biteblock. This should be placed on the aspect of the biteblock facing away from the tooth being imaged (Figure 6).
Figure 6. The use of cotton roll to stabilize the biteblock when imaging a mandibular incisor. The arrow denotes the area where the patient could use their thumb and forefinger to immobilize the biteblock.
3. Learning differences
Many individuals with learning differences are able to co-operate while intra-oral dental radiographs are taken. It is often easier to use a modified occlusal technique for anterior teeth (see later section) as this is more comfortable and therefore more acceptable to this group of patients. Some patients with learning differences have a tendency to bite strongly on the imaging receptor, leaving permanent marking on the phosphor surface of the plate. The use of thin radiolucent card or unexposed, but processed, dental film can be used either side of the phosphor plate to lessen the potential for damage.
4. Patient's mobility issues
Any impairment to a patient's mobility has little effect on the outcome of dental radiography. Patient's with limited mobility of their upper limbs may not be able to immobilize the radiographic holder should this be deemed necessary (see section on missing teeth). You could ask the person's carer whether they would be willing to hold the holder in situ while the exposure is being taken. The Ionising Radiation (Medical Exposure) Regulations (IR(ME)R) 2017 requires that the carer is informed of the radiation dose they may receive during the procedure, and the risks that are associated with this.
5. Techniques
Bisecting angle radiographs
Owing to the current practice of using the paralleling technique, many practitioners will have limited or no experience of using the bisecting angle technique in dental radiography.
The bisecting angle technique relies on the patient holding the receptor in the correct position within their mouth. Although phosphor plates work well with the paralleling technique, they are more flexible and prone to bending than film packets, when being held in position by your patient's finger. Bending of the phosphor plate results in a distorted image. Supporting the phosphor plate with thin radiolucent card should reduce the likelihood of the plate becoming bent (Figure 7).
Figure 7. Radiolucent card to support phosphor plate.
Where the operator has limited experience of using this technique, it is possible to reduce the potential of cone cut from the rectangular collimator by temporarily exchanging this for a round collimator (Figure 8), to maintain the focus to skin distance. The operator must be mindful that this will increase the patient's dose of ionizing radiation and, therefore, should only be performed if deemed absolutely necessary to produce a diagnostic image. It is imperative that the patient's head is resting against the headrest with the occlusal plane parallel to the floor (Figure 9).
Figure 8. Round collimator on tube head.Figure 9. Patient's head in position for bisecting angle image.
The receptor is positioned in the patient's mouth on the lingual aspect of the tooth/teeth to be imaged, with 2 mm extending beyond the incisal or occlusal edges. The receptor should be in portrait orientation for incisors and canines; molars and premolars require the receptor to be in landscape orientation (Figure 10 a,b).
Figure 10.
(a) Position of phosphor plate for a bisecting angle image of the molar/premolar region. (b) Receptor in position to image maxillary premolar and molar teeth. The edges of the barrier envelope have been highlighted using white dashed lines.
Ask the patient to use the index finger of their opposite hand to support the receptor. The tube head should be set to allow the X-ray beam to pass through the selected area. The horizontal angle must be perpendicular to the interproximal contact areas of the teeth being imaged, the approximate vertical (bisecting) angle is shown in Table 1 below.
Teeth
Incisors
Canine
Premolar
Molar
Alternative
Maxilla↓
+45°
+50°
+40°
+30°
+55° -60°, position receptor as per occlusal
Mandible↑
-25°
-20°
-15°
-5°
-45° to -50°, position receptor as per occlusal
An alternative method for imaging anterior teeth is the use of a modified occlusal technique.
Modified occlusal technique
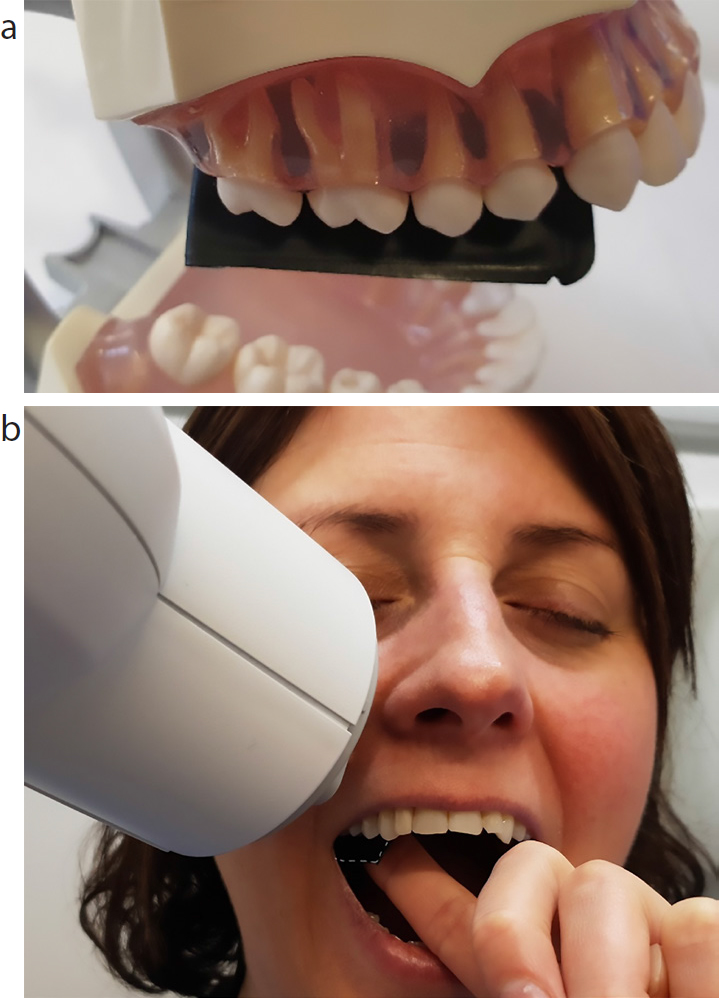
Ensure your patient's head is resting against the headrest, with the occlusal plane parallel, and sagittal plane perpendicular, to the floor. A size 2 imaging receptor is placed horizontally (as per an occlusal image) in to the mouth. The dimensions of the size 2 receptor are 31 mm × 41 mm. Align the longer side (41 mm) of the receptor to the long axis of the tooth under investigation (Figure 11). The tube head adjusted to +55° for upper teeth, with the central ray aligned to the tooth being investigated. This technique can also be used for mandibular teeth with the tube head adjusted to -45° to -50°, although the resultant images do not usually give as much bony detail as could be achieved from a paralleling image.
Figure 11. Position of phosphor plate using a modified occlusal technique to demonstrate maxillary central incisors. The smaller (31 mm) side of the receptor is visible.
Parallax
Parallax views can be useful to determine the relative position of two objects (eg separating out distal and buccal root canals). Traditionally this is performed by taking two separate images of one object, the angulation of the X-ray tube in relation to the object will be different for each exposure. This technique is usually adopted once the first image has been viewed, and the clinician requires further radiographic information to aid treatment. Not only is it necessary to decide which direction the X-ray beam should be in for the second image, it is also easy to be overzealous when selecting the degree of angulation. If repeat imaging is required at later date, it is virtually impossible to accurately reproduce the original images by correctly assessing the angle applied to the parallax view.
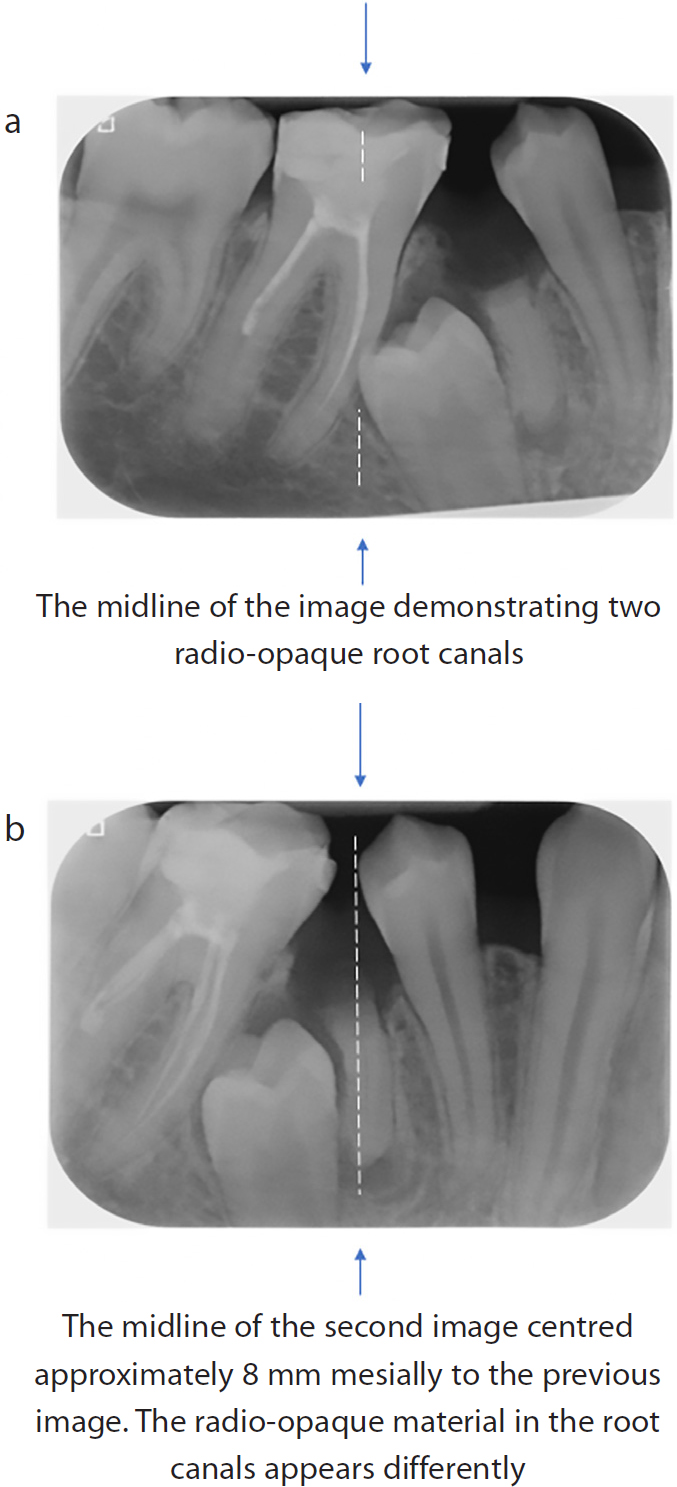
If the first image has been made using the paralleling technique, a simpler method is to determine the centre of the first image, then place the radiographic holder and receptor approximately 5–8 mm distal or mesial to this for the second image. Position the X-ray tube directly in line with the locator ring, do not apply any other angulation. This small adjustment should be enough to separate out the anatomy in the region of interest (Figure 12). Should the same image be required in future, it is easier for the operator to assess the required positioning of the holder, receptor and X-ray tube to obtain the desired image.
Figure 12.
(a, b) The effect of a small shift in the centring of parallel technique radiographs.
Exposure settings
Each unit is pre-programmed with average exposures for the region being imaged. When the unit was installed, a medical physicist will have determined the exposure settings that most closely match the required output from the unit, programming these in to your control panel.
In most instances these are exactly what is required, although occasionally, small adjustments to better suit the patient may need to be made. One of the most common reasons for altering the pre-set exposure factors is when imaging maxillary incisors. The X-ray beam may pass through the patient's nose. For patients who have developed rhinophyma (thickening of the nose), the apices of their incisors may not be visualized as clearly in comparison to their other teeth (Figure 13). A small increase in the exposure factors used should provide an image with an acceptable level of detail, allowing more scope when manipulating the image digitally once processed. The exposure increase required is no more than a one-step increase of the time factor (eg increase the time from 0.1 seconds to 0.12 seconds)
Figure 13. Peri-apical showing soft tissue of the nose superimposed on the apices of the maxillary central teeth (white arrows).
It might also be necessary to make a small increase or decrease to exposure factors when taking radiographs of patients who may have higher or lower bone density, respectively.
Digital processing uses algorithms to compensate for suboptimal exposure selection; however, if the radiation dose reaching the imaging receptor is too low, processing cannot compensate for this. The image would appear grainy and have low contrast. If the dose reaching the receptor is higher than required, the processing algorithms can adjust accordingly and the use of a dose higher than required usually remains unnoticed. There is, therefore, the potential to increase the exposure factors incrementally over time to a level that is higher than necessary for the examination being undertaken, yet the processing system (in the absence of dose readouts) does not alert the operator to the issue as the image will be of diagnostic appearance. This phenomenon is referred to as exposure creep.
Conclusion
Intra-oral imaging can be daunting for the new practitioner. Repeated practice will quickly allow skills and confidence to develop. It is hoped that having read this article, the practitioner will be empowered to use modified techniques on occasions where they would otherwise struggle to achieve a diagnostic radiographic image.