Benediktsdóttir IS, Wenzel A. Accuracy of digital panoramic images displayed on monitor, glossy paper, and film for assessment of mandibular third molars. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 2004; 98:217-222
Gijbels F, Sanderink G, Pauwels H, Jacobs R. Subjective image quality of digital panoramic radiographs displayed on monitor and printed on various hardcopy media. Clin Oral Invest. 2004; 8:25-29
Schulze RK, Schulze D, Voss K, Rottner M, Keller H, Dollmann K Quality of individually calibrated customary printers for assessment of typical dental diagnoses on glossy paper prints: a multicenter pilot study. Oral Surg Oral Med Oral Pathol Oral Radiol Endodontol. 2008; 106:578-586
Ibbott GS, Zhang Y, Mohiuddin M, Adams E. Reproduction of radiologic images on plain paper. Radiographics. 1998; 18:755-760
Otis LL, Sherman RG. Assessing the accuracy of caries diagnosis via radiograph: film versus print. J Am Dent Assoc. 2005; 136:323-330
Molander B, Gröndahl H-G, Ekestubbe A. Quality of film-based and digital panoramic radiography. Dentomaxillofac Radiol. 2004; 33:32-36
Digital dental radiography allows for exchange of images between primary and secondary care. However, it is common practice for radiographs to be printed out and attached to referrals. This study investigates the loss of diagnostic information of printed radiographs compared to the on-screen digital image. The best quality was achieved with images printed onto radiographic film or onto photographic paper with an inkjet printer. Laser and inkjet printer output onto 80 gsm office paper resulted in a loss of diagnostic information. Wherever possible, radiographs should be transmitted digitally between clinicians to maintain image integrity.
Clinical Relevance: This paper illustrates the potential pitfalls of printing radiographs to be sent with referrals.
Article
The introduction of digital panoramic radiographs in general dental practice allows for exchange of radiographic information between primary and secondary care. Unfortunately, this is not universally reflected in practice and many radiographs are printed out on standard office paper and attached to referrals. Most published work has concentrated on the quality of digital radiographs compared to film systems but a number of authors have investigated the quality of printed digital radiographs. Inkjet prints on glossy photographic paper and radiographic film demonstrate equivalent image accuracy to on-screen digital images1,2,3 and laser prints on office paper show acceptable image quality for medical CT scans in 90% of cases.4 Bitewing radiographs can be printed without loss of diagnostic information,5 but these can be easily enlarged many times, unlike panoramic radiographs. This study aims to establish if there is a loss of diagnostic information in a printed panoramic radiograph compared to the on-screen digital image.
Material and methods
Five different digital panoramic radiographs of dentate individuals with third molars present were printed using the following media and printers (Figures 1–5):
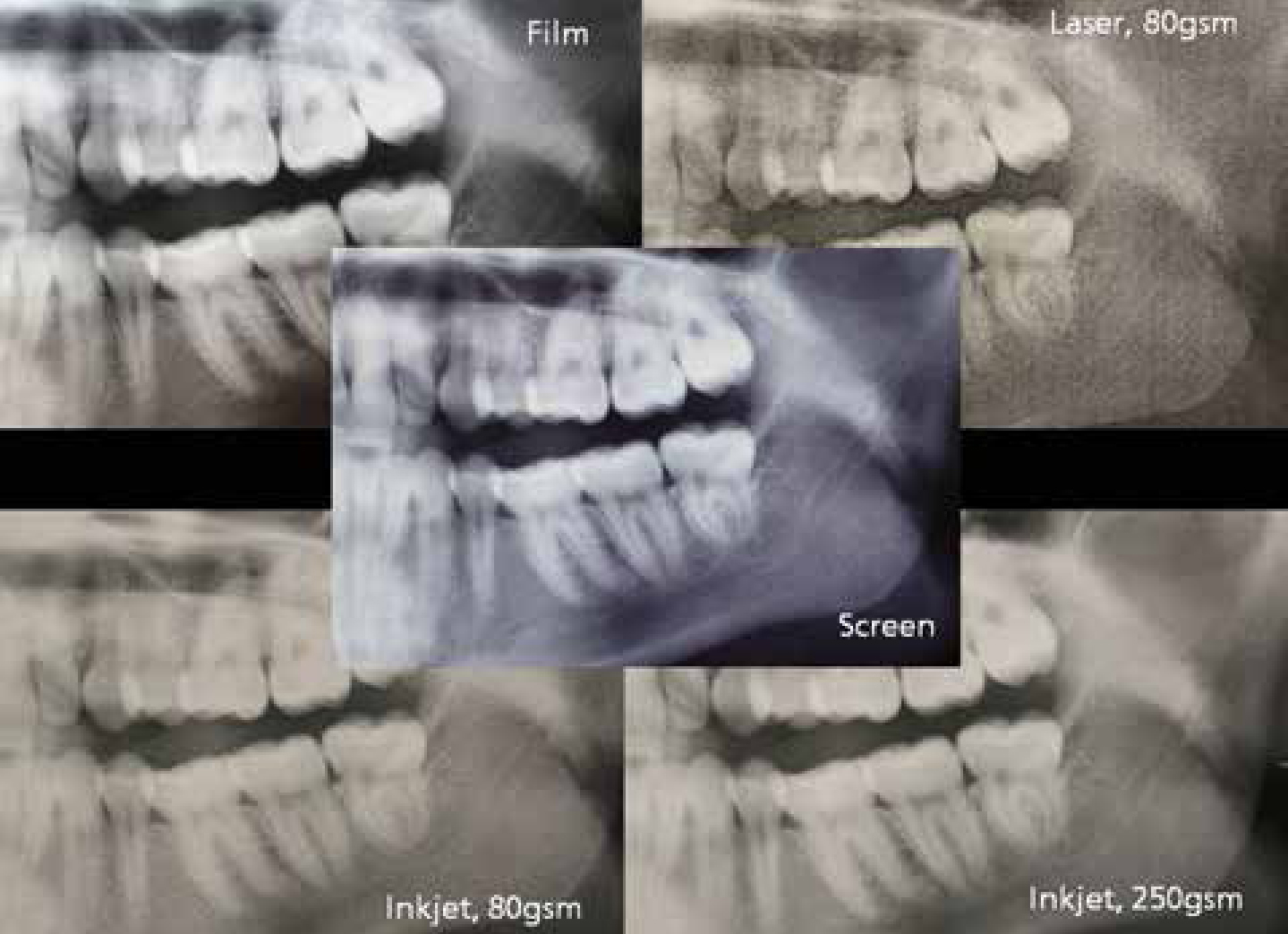
Figure 1. Inkjet printer on 250 gsm photographic paper.Figure 2. Inkjet printer on 80 gsm office paper.Figure 3. Laser printer on 80 gsm office paper.Figure 4. Medical dry laser on film.Figure 5. 19” LCD screen.
Fuji DryPix 5000 (Fuji, Japan) onto radiographic film (radiographic film);
Epson Stylus C45 (Seiko Epson Corporation, Nagano, Japan) set to normal quality onto Hewlett-Packard 80 gsm office paper (inkjet);
Epson Stylus Photo R2400 (Seiko Epson Corporation, Nagano, Japan) set to highest quality onto Epson 250 gsm A4 photographic paper (inkjet photo).
The visual grading system used by Molander et al6 to compare digital and film panoramic radiographs was adapted for this study to assess image quality objectively. Nine experienced dentists working in hospital oral surgery departments were recruited to assess the images.
Assessors were free to use any of the available tools in the MedView image viewing software (MedImage, Ann Arbor MI) to adjust image size or any other parameters. Viewing took place in quiet consulting rooms and assessors were free to adjust the lighting if required. A viewing box was provided for the radiographic film to be displayed. No time limit was set for viewing. (Figure 6)
Figure 6. Comparison of image quality between media.
They were asked to score the visibility of nine different anatomical structures (Table 1) in the printed image compared to the digital image on a 19” LCD screen (Hewlett Packard L1906 at 1280 x 1024 resolution). Assessors were asked to concentrate on the visibility of the anatomical structures rather than the overall aesthetics of the image or any pathological features. The anatomical structures are shown in Table 1 and the visual grading scores in Table 2. The mean score of each image was calculated and the statistical method used for comparison was the Wilcoxon sign rank test.
Anatomical structures rated by assessors
Lower and anterior border of maxillary sinus
Periodontal bone level, upper jaw
Periapical structures, upper jaw
Trabecular bone, upper jaw
Mandibular canal and mental foramen
Periodontal bone level, lower jaw
Trabecular bone, lower jaw
Mandibular third molars
Overall rating
Rating compared with digital image on screen
Numerical score
Much worse
1
Worse
2
Equal
3
Better
4
Much better
5
Results
The highest quality image was achieved with radiographic film, followed by inkjet photo printouts. Both were rated as higher quality than the on-screen digital image. Laser and inkjet printouts onto 80 gsm office paper both performed poorly, and were rated as worse than the digital image. Results are shown in Table 3.
Print Technology
Mean Visibility Rating (±SD)
Radiographic film
3.88 (0.64)
Inkjet photo
3.14 (0.71)
Inkjet
2.00 (0.60)
Laser
1.90 (0.51)
Discussion
The results show that printed radiographs have the potential to be more highly rated for visibility of anatomical structures than a digital image. However, this was only the case for images that were printed onto costly film or photographic paper with a high quality inkjet printer. This is not representative of the radiographs typically received with referrals, which are more commonly printed onto office paper using an inkjet or laser printer. These modalities were poorly rated by all observers and there was significant loss of diagnostic information.
The preference of the observers for high resolution printed images (inkjet photo and radiographic film) is perhaps due to the ability to view these hard copies without the need to pan and zoom the image. Office monitors have around 100 dots per inch forming the LCD matrix, whereas high quality inkjet and radiograph printers are capable of printing several thousand dots per inch. In order to see the same amount of detail as in the printed image, the viewer should zoom into the digital image to overcome the relatively low resolution of the display.
Wherever possible, it is recommended that, when the transfer of radiographs between practitioners is required, the image is transmitted digitally to ensure no loss of diagnostically useful information. There are technical and data protection hurdles that may need to be overcome in order to achieve smooth transfer of high quality images. Where this digital transfer is not possible, it is recommended that images are printed onto a high quality medium such as radiographic film or photographic paper.