Donatsky O. Osseointegrated dental implants with ball attachments supporting overdentures in patients with mandibular alveolar ridge atrophy. Int J Oral Maxillofac Implants. 1993; 8:(2)162-166
Doundoulakis JH, Eckert S, Lindquist CC, Jeffcoat MK. The implant supported overdenture as an alternative to the mandibular complete denture. J Am Dent Assoc. 2003; 134:(11)1455-1458
Sadowsky S. Treatment considerations for maxillary implant overdentures: a systematic review. J Prosthet Dent. 2007; 97:(6)340-348
McGill Consensus Statement on Overdentures. Int J Oral Maxillofac Implants. 2003; 8:601-602
Dudic A, Merickse-Stern R. Retention mechanisms and prosthetic complications of implant supported mandibular overdentures: long term results. Clin Imp Dent Related Res. 2002; 4:(4)212-219
Meijer HJA, Raghoebar GM, Batenburg RHK, Vissink A. Mandibular overdentures supported by two Brånemark, IMZ or ITI implants: a ten year prospective randomised study. J Clin Periodontol. 2009; 36:(9)799-806
Cochran D. The evidence for immediate loading of implants. J Evid Base Dent Pract. 2006; 6:(2)155-163
Galluci G, Morton D, Weber H-P. Loading protocols for dental implants in edentulous patients. Int J Oral Maxillofac Implants. 2009; 24:132-146
Kawai Y, Taylor JA. Effect of loading time on the success of complete mandibular titanium implant retained overdentures: a systematic review. Clin Oral Imp Res. 2007; 18:(4)399-408
Marzola R, Scotti R, Fazi R, Schincaglia GP. Immediate loading of two implants supporting a ball attachment-retained mandibular overdenture: a prospective clinical study. Clin Imp Dent Related Res. 2007; 9:(3)136-143
Liddelow GJ, Henry PJ. A prospective study of immediately loaded single implant-retained mandibular overdentures: preliminary one-year results. J Prosthet Dent. 2007; 97:126-137
Jivraj S, Chee W, Corrado P. Treatment planning of the edentulous maxilla. Br Dent J. 2006; 201:(5)261-279
Chee W, Jivraj S. Treatment planning of the edentulous mandible. Br Dent J. 2006; 201:(6)337-347
Chung K-H, Chung C-Y, Cagna DR, Cronin RJ. Retention characteristics of attachment systems for implant overdentures. J Prosthodont. 2004; 13:(4)221-226
Vere JW, Deans RF. Tooth-supported, magnet retained overdentures: a review. Dent Update. 2009; 36:(5)305-310
Fueki K, Kimoto K, Ogawa T Effect of implant-supported or retained dentures on masticatory performance: a systematic review. J Prosthet Dent. 2007; 98:(6)470-477
Salvi GE, Bragger U. Mechanical and technical risks in implant therapy. Int J Oral Maxillofac Implants. 2009; 24:(Suppl)69-85
Fitzpatrick B. Standard of care for the edentulous mandible: a systematic review. J Prosthet Dent. 2006; 95:(1)71-78
American Association of Oral and Maxillofacial Surgeons. 2009. www.aaoms.org
Moy P, Medina D, She2tty V Dental implant failure rates and associated risk factors. Int J Oral Maxillofac Implants. 2005; 20:(4)569-577
Nedir R, Bischof M, Szmukler-Moncler S, Belser UC, Samson J. Prosthetic complications with dental implants: from an up to 8 year experience in private practice. Int J Oral Maxillofac Implants. 2006; 21:(6)919-928
Chaffee N, Felton DA, Cooper LF, Palmqvist U, Smith R. Prosthetic complications in an implant retained mandibular overdenture population: initial analysis of a prospective study. J Prosthet Dent. 2002; 87:(1)40-44
Goodacre CJ, Kan JYK, Rungcharassaeng K. Clinical complications of osseointegrated implants. J Prosthet Dent. 1999; 81:(5)537-552
Fontijn-Tekamp FA, Slagter AP, Van Der Bilt A Biting and chewing on overdentures, full dentures and natural dentitions. J Dent Res. 2000; 79:(7)1519-1524
Implant-retained overdentures represent a treatment option for many patients unable to tolerate conventional dentures. They may be specifically indicated in patients with altered anatomy, neuromuscular disorders, a pronounced gag reflex or severe residual ridge resorption. This article discusses the different ways in which implant overdentures can be retained, outlines some of the clinical stages involved in planning and providing these prostheses, and highlights long-term maintenance requirements associated with implant-retained overdentures.
Clinical Relevance: Patients with implant-retained overdentures are likely to present in general dental practice. Practitioners should be aware of issues associated with the design, treatment planning and maintenance of these prostheses.
Article
An implant-retained overdenture is a removable dental prosthesis supported by the residual oral tissues and retained by dental implants. This concept has been successfully used for over 30 years.1 Implant-retained overdentures demonstrate improved retention and stability when compared to conventional dentures.2,3 Furthermore, implant-retained overdentures may reduce residual ridge resorption and improve chewing function, nutritional status, speech and patient confidence,2,4 This type of prosthesis should be considered in all patients unable to tolerate conventional dentures. They may be specifically indicated in patients with altered anatomy following surgery, neuromuscular disorders, a pronounced gag reflex or severe residual ridge resorption.
This review discusses the differing ways in which implant-retained overdentures can be retained, outlines some of the clinical stages involved in planning and providing these prostheses, and highlights the maintenance requirements associated with implant-retained overdentures.
Number of implants
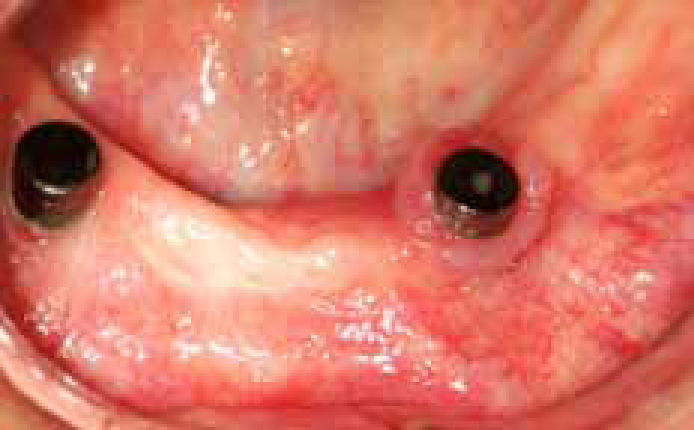
Overdentures may be retained by a varying number of implants, which may be splinted or freestanding.5 Studies investigating mandibular overdentures have reported high implant survival rates and treatment success rates when overdentures are retained by either two or four implants.1,5,6 Originally, implants retaining mandibular overdentures were splinted to distribute stresses and protect the bone-implant interface.7 However, later studies have suggested that this is unnecessary. A recent systematic review by Galluci et al reported that mandibular overdentures retained by two unsplinted implants in the canine regions were as successful as four splinted implants.8 This statement appears true regardless of whether the implants are conventionally or immediately loaded.9,10 It has even been reported that lower implant overdentures can be successfully retained by a single implant.11 However, this is not advocated as a mainline treatment strategy. Two freestanding implants in the canine regions, as the simplest option, would appear the treatment of choice to retain an overdenture in the edentulous mandible (Figure 1).
Figure 1. Two freestanding implants with ball abutments (Nobel Biocare, Göteborg, Sweden) to retain a lower overdenture.
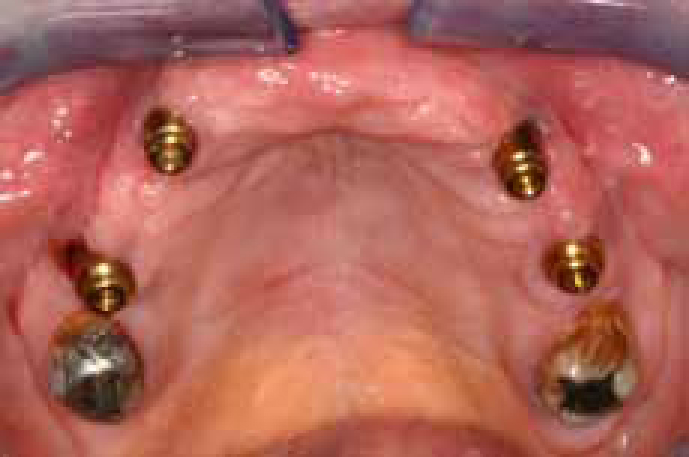
Traditionally, implant-retained overdentures have performed poorly in the maxilla.3 This has been attributed to relatively poor bone quality and quantity, increased implant to abutment ratios and non-axial loading.3 As a result, a greater number of implants are normally placed in the maxilla. Several reviews have concluded that there is little evidence to support any approach, other than the delayed loading of 4–6 splinted implants in the maxilla.3,8 When this approach is used, implant survival rates of 94.8–97.7% after 10 years have been reported.8 However, freestanding implants have also been successfully used to support implant-retained overdentures in the maxilla8 (Figure 2). Ideally, implants in the maxilla should be widely distributed, symmetrically about the arch. However, this may be complicated by pneumatization of the maxillary sinus, alveolar orientation and ridge morphology. Zygomatic implants can be useful where there is extensive pneumatization of the maxillary sinuses.12
Figure 2. Four implants with Locator® attachments (Zest Anchors LLC, California, USA) retaining a maxillary overdenture.
Attachments
Implant overdentures may be retained by rigid or resilient attachments.5 A rigid attachment can be provided by a milled bar. Resilient attachments include round bars (Figure 3), ball abutments (Nobel Biocare, Göteborg, Sweden) (Figure 1), Locators® (Zest Anchors LLC, California, USA) (Figure 2) and magnets (Figure 4).5 Milled bars do not allow movement of the denture base. They provide excellent retention and stability and can provide relief over painful areas such as superficial mental nerves.5 However, they are expensive, difficult to repair and derive limited mucosal support, which may overstress attachments and predispose to mechanical complications.13 Resilient bars, when appropriately designed, allow a single axis of rotation, utilize greater mucosal support, and offer greater protection to the retentive attachments.13 Both designs of bar may be used to align non-parallel implants.5,13 However, they require at least 10 mm of interocclusal clearance and should not be used where vertical space is limited.13 Both designs of bar may be associated with soft tissue hyperplasia.13
Figure 3. Round bar retaining a lower overdenture.Figure 4. Magnet abutments (Magnacap, Technovent, UK).
Freestanding abutments, such as balls, Locators® (Zest Anchors LLC, California, USA) and magnets, are generally simpler, cheaper and have smaller space requirements than bars.3,5 Freestanding abutments are screwed directly into the implant and come in varying heights to accommodate soft tissue contour. Ball attachments are commonly reported in the literature.1,3 However, Locators® (Zest Anchors LLC, California, USA) appear to be becoming increasingly fashionable, although there is limited evidence to support their use.8 Magnets appear to be the least retentive abutments.14 However, they are simple, hygienic, less sensitive to insertion direction than other attachments and self-locating.15 Modern magnets are less susceptible to corrosion than their predecessors. However, loss of magnetism can still be problematic with time. Magnets may be useful in patients with poor manual dexterity because they are relatively easy to insert and remove.15
Although several studies have attempted to compare different attachment mechanisms, results appear equivocal.5,16,17 A retrospective, cohort study, by Dudic and Merickse-Stern, involving 119 patients reported no difference in treatment outcome when rigid bars, resilient bars and freestanding ball abutments were compared.5 Fueki et al reported that the masticatory performance of overdentures was unaffected by the attachment mechanism.16 On the contrary, Salvi and Bragger reported that patient satisfaction and retention were greatest with bars and worst with magnets, with balls somewhere in between.17
We can conclude that overdentures can be successfully retained using a variety of attachment mechanisms, each having their own indications, advantages and disadvantages. In the maxilla the evidence base supports the use of 4–6 implants splinted with a bar, although freestanding abutments are increasing in popularity.3,8 In the mandible, two freestanding abutments appear to be the treatment of choice.8 All attachments have minimum space requirements and this should be considered during treatment planning.13
Treatment planning
Options available for the rehabilitation of edentulous patients are complete dentures, implant-retained overdentures or implant-supported fixed bridgework.13 Implant-retained overdentures with two implants in the intercanine region have been advocated as the standard of care in the edentulous mandible.4 However, this view is not universally held16,18 and implant overdenture treatment involves surgical procedures and is associated with long-term maintenance requirements.17 It is prudent to construct well-fitting, correctly extended conventional prostheses prior to considering implant treatment. This approach does not preclude future implant placement and permits assessment of vertical space requirements, tooth position and lip support. Furthermore, if future implant treatment is indicated, these dentures can be duplicated and used as both radiographic and surgical stents (Figure 5). When implants are placed without consideration of the final prosthesis, overdenture construction can be compromised, or even impossible, as some of the implants may be unusable (Figure 6). Maxillary dentures are generally well tolerated and a well designed, correctly extended, conventional prosthesis usually precludes the need for implant placement.
Figure 5. Denture duplicated in clear acrylic resin for use as surgical stent.Figure 6. Implants with magnet abutments (Magnacap, Technovent, UK), positioned too labially in maxilla with little regard for future tooth position.
When constructing an implant-retained prosthesis, the primary decision is between a removable and a fixed prosthesis. A full discussion of the merits of full arch fixed bridgework is beyond the scope of this article. However, several systematic reviews have suggested that patients are equally satisfied with both implant-retained overdentures and fixed bridges.16,18 Overdentures are simpler, more hygienic and cheaper to fabricate than fixed bridgework. Furthermore, overdentures can easily replace lost hard and soft tissue and provide lip support that may have been lost. Implant-supported fixed bridgework is often difficult in the upper arch because the pattern of bone resorption following tooth loss leads to ideal tooth position being much further forward than residual ridge position.12
A thorough assessment of the medical history is essential for all patients undergoing implant overdenture treatment. With the exception of intravenous bisphosphonates, there appear to be very few absolute contra-indications to implant placement.19,20 However, factors such as smoking, diabetes mellitus, corticosteroids, radiotherapy and osteoporosis represent relative contra-indications and should be considered in conjunction with other factors.20
Extra-oral examination should include assessment of the smile line, occlusal-vertical dimension and lip support with and without any prostheses in place. Where lip support is inadequate without the maxillary denture, a labial flange, and thus an overdenture, is likely to be the preferred treatment modality.12 Intra-orally, the quality and health of the mucosa overlying the denture-bearing area should be assessed. Visual examination should be supplemented by palpation to give an indication of alveolar ridge width and morphology. Particular consideration should be given to the presence of lingual undercuts in the lower jaw and tissue compressibility. Examination should always be supplemented by plain film radiographs and, where these provide insufficient information, cross-sectional imaging. The use of radiographic stents will result in the acquisition of maximum information.
Prosthodontic clinical stages
Following implant placement, the principles governing overdenture construction are similar to those for conventional denture construction. An accurate master impression is required to ensure that the denture bases are well adapted to the underlying tissues and fully extended.13 Implants are designed to supplement, not replace, the retention and stability derived from the denture base. Although underextended overdenture bases may have a role in the management of patients with a severe gag reflex, this is a compromised situation.
The determination of ideal tooth position, and thus assessment of space requirements, prior to selecting overdenture abutments is important. If the patient's existing prosthesis is satisfactory, and is to be copied, this information is readily available. Otherwise, it is necessary to proceed to a wax try-in with denture teeth. Following the try-in, the positions of the teeth and flanges can be related to a fixture head impression and appropriate abutments can be selected.
Attachments can be successfully added to the denture base indirectly at the processing stage or directly at the denture fit appointment using a cold cure acrylic resin such as Tokuyama® Rebase 2 (Tokuyama America Inc, CA, USA). A direct approach may be more accurate as it avoids processing errors and allows for compressibility of the soft tissues overlying the denture-bearing area. However, the direct approach must be used carefully because cold cure acrylic resin may lock into undercuts. The authors have found the direct approach to be highly successful when using freestanding abutments if undercuts are blocked out and appropriate vents are placed in the denture base (Figures 7 and 8).
Figure 7. Locator® attachments (Zest anchors, LLC, California, USA) prepared for intra-oral addition to denture base.Figure 8. Attachments cold cured into denture base.
Maintenance requirements
Regardless of attachment type, following insertion, implant-retained overdentures appear to be associated with a high incidence of prosthetic complications.5,6,17,21–23 Reported complications include:
Figure 9. Overdenture has fractured over freestanding abutment at LL3 site.Figure 10. Soft tissue hyperplasia associated with subgingival calculus around a magnet abutment (Magnacap, Technovent, UK).Figure 11. Soft tissue hyperplasia associated with a ball abutment (Nobel Biocare, Göteborg, Sweden) at LR3 site.Figure 12. Fistula and peri-implant bone loss associated with lower overdenture.
A prospective case series by Chaffee et al reported the prosthetic complications associated with ball-retained overdentures. Ninety percent of the patients included in this study required 327 return visits, 194 of which were unscheduled, over a three year period.22 These visits involved 115 practitioner hours and were estimated to cost $218 per patient. Meijer et al reported that 6–7.5 hours of aftercare was necessary for every patient with a bar-retained overdenture (n = 90) over a 10-year period.6
The most common complication associated with implant-retained overdentures is loss of retention. This may affect up to 75% of prostheses over a 2-year period.23 Loss of retention usually results from loosening or fracture of the retentive element.23 However, it may also be associated with wear of the implant abutment. It is usually straightforward to replace or retighten the retentive elements at the chairside, although it is sometimes necessary to replace the entire retentive housing. These housings can be replaced using a direct approach with a cold cure acrylic resin such as Tokuyama® Rebase 2 (Tokuyama America Inc, CA, USA), or indirectly following a reline impression (Figure 13). A localized reline is only appropriate where the denture base is well adapted to the underlying tissues. When the retentive housings of bar-retained overdentures are replaced directly, great care must be taken to block out undercuts beneath the bar (Figure 14). Undercuts can be blocked out with either carding wax or a caulking agent such as Oraseal (Ultradent Products Inc, USA). Although inconvenient for the patient, it is usually preferable to pick up the bar in a reline impression and replace the housings indirectly.
Figure 13. Localized reline impression, taken using a closed mouth technique, allowing indirect addition of retentive housings to denture base.Figure 14. Undercuts beneath a round bar blocked out with wax prior to a pick-up impression abutment.
Implant-retained overdentures appear more susceptible to fracture than conventional dentures. This may be attributed to increased masticatory forces.24 Overdentures should intimately contact the underlying mucosa to derive support and they should be constructed in sufficient bulk to provide fracture resistance, particularly around the retentive housings.23 Cobalt-chromium frameworks may reduce the incidence of some mechanical complications.17 However, they increase the cost of treatment.
Most of the complications associated with implant-retained overdentures are simple and easily remedied. However, they can occur on a regular basis and management of these complications can be expensive and time consuming for the patient, clinician and technician. Patients must be warned about maintenance requirements and future financial obligations prior to the commencement of implant overdenture treatment. This is an important part of the informed consent process.
Conclusions
Compared to conventional dentures, implant-retained overdentures have improved retention and stability, and they represent a valuable treatment option in those unable to tolerate conventional dentures.
Various attachments, with differing space requirements, advantages and disadvantages can be used to retain implant overdentures.
Implant-retained overdentures are associated with a high incidence of manageable prosthetic complications and clinicians should make patients aware of this before embarking upon treatment.