Lussi A, Jaeggi T, Zero D. The role of diet in the aetiology of dental erosion. Caries Res. 2004; 38:34-44
Järvinen VK, Rytömaa Heinonen OP. Risk factors in dental erosion. J Dent Res. 1991; 70:942-947
Steele J, O'Sullivan ILeeds: NHS Information Centre for Health and Social Care; 2011
Chadwick B, Pendry L.London: Office for National Statistics; 2004
Tahmassebi JF, Duggal MS, Malik-Kotru G, Curzon MEJ. Soft drinks and dental health: a review of the current literature. J Dent. 2006; 34:2-11
Lussi A, Megert B, Shellis RP, Wang X. Analysis of the erosive effect of different dietary substances and medications. Br J Nutr. 2011; 30:1-11
Okunseri C, Okunseri E, Gonzalez C, Visotcky A, Szabo A. Erosive tooth wear and consumption of beverages among children in the United States. Caries Res. 2011; 45:130-135
Touyz LZ. The acidity (pH) and buffering capacity of Canadian fruit juice and dental implications. J Canad Dent Assoc. 1994; 60:454-458
Creanor SL, Creanor S, Alharthy N. A comparison of in vitro-like mineral loss between continuous and intermittent acidic exposure with and without human saliva. Arch Oral Biol. 2011; 56:703-708
Cleveland, Ohio: The Chemical Rubber Company; 2005
, 2nd edn. In: Patty F (ed). New York: Interscience Publishers; 1963
Klofutar C, Šegatin N. Electrical conductivity studies of quinic acid and its sodium salt in aqueous solutions. J Sol Chem. 2007; 36:879-889
Hughes JA, West NX, Parker DM, Van Den Braak MH, Addy M. Effects of pH and concentration of citric, malic and lactic acids on enamel, in vitro. J Dent. 2000; 28:147-155
Rees JS. The role of drinks in tooth surface loss. Dent Update. 2004; 31:318-326
Edwards M, Creanor SL, Foye RH, Gilmour WH. Buffering capacities of soft drinks: the potential influence on dental erosion. J Oral Rehab. 1999; 26:923-927
Eisenburger M, Addy M. Influence of liquid temperature and flow rate on enamel erosion and surface softening. J Oral Rehab. 2003; 30:1076-1080
Amaechi BT, Higham SM, Edgar WM. Factors influencing the development of dental erosion in vitro: enamel type, temperature and exposure time. J Oral Rehab. 1999; 26:624-630
Gandara BK, Truelove EL. Diagnosis and management of dental erosion. J Contemp Dent Prac. 1999; 1:28-44
West NX, Hughes JA, Addy M. Erosion of dentine and enamel in vitro by dietary acids: the effect of temperature, acid character, concentration and exposure time. J Oral Rehab. 2000; 27:875-880
Amaechi BT, Higham SM. Dental erosion: possible approaches to prevention and control. J Dent. 2005; 33:(Spec Iss)243-252
An in vitro investigation of the initial ph and titratable acidity of a selection of fruit smoothies Suzanne M Blacker Stephen L Creanor Siobhan Creanor Dental Update 2025 38:9, 604-609.
Authors
Suzanne MBlacker
BDS, PhD, MFDS, RCSEd, AHEA, MDSci
Clinical Lecturer/Honorary Specialist Registrar in Restorative Dentistry, Level 9, Dundee Dental Hospital and School, Park Place, Dundee DD1 4SY
Professor of Oral Sciences and Director of Undergraduate Dental Studies, Peninsula Dental School, Peninsula College of Medicine and Dentistry, The University of Plymouth, Room C407, Portland Square, Plymouth PL4 8AA
Four commercially-available fruit smoothie drinks were assessed for both initial/baseline pH and titratable acidity. A commercially-available smooth orange juice drink was used as a positive control. Baseline pH and titratable acidity were measured by titrating each fruit smoothie with 0.5 mL increments of 1M sodium hydroxide (NaOH), and measuring the pH following the addition of each increment, until pH 7 and pH 10 were reached. Each of the fruit smoothies investigated demonstrated a low baseline pH and had relatively high titratable acidity. Owing to both their low pH and high titratable acidity, it would be advisable to limit the consumption of such fruit smoothies to meal times.
Clinical Relevance: Fruit smoothies, which are made from pure fruit blended with 100% fruit juice, are a relatively new addition to the soft drinks market. It is recommended that they be consumed through a straw, similar to the advice given for other acidic soft drinks.
Article
It has been claimed that fruit smoothies ‘are set to be the high street success story for the UK soft drinks industry over the next few years’.1
In the UK, consumption of shop-purchased fruit smoothies has risen dramatically, from 6 million litres in 20011 to 51 million litres in 2010, having peaked at 79 million litres in 20072 and in 2010 UK smoothie sales were worth £141 million.2 The true level of smoothie consumption is not known, however, as these figures exclude consumption of homemade drinks, as well as those bought from cafés, coffee shops and juice bars.
The increase in smoothie consumption has been in line with the UK Government's ‘five-a-day’ campaign which encourages the public to consume at least five portions of fruit and vegetables every day.3 Many individuals see the consumption of fruit smoothies as one means of achieving this target. One serving of fruit smoothie can be counted as up to two of the recommended ‘five-a-day’.3 Despite this campaign, the majority of adults and children are still not achieving this daily target. In 2007, fruit in the form of pure fruit juice accounted for an 11.6% share of the ‘5-a-day’ consumption in children, an 8% increase on the previous year.4 Of the 1180 million litres of fruit juice consumed in the UK in 2010, smoothie consumption accounted for around 5%.2
Historically, fruit smoothies appear to have originated in Brazil from juicing fruit.5 Smoothies first appeared in the UK in 1994 and have steadily increased their share of the soft drink market.5 Legally, there is no definition of a fruit smoothie, but it is well accepted in the soft drinks industry that fruit smoothies are made only from pure fruit blended with 100% fruit juice, not from concentrate, and with no added ingredients, such as dairy, sugar, sweeteners or water.5,6
There are many varieties of fruit smoothies which use different combinations of a range of fruits, which contain various combinations of organic fruit acids such as citric, malic, phosphoric, oxalic and tartaric acids. Because of the acidic contribution to their composition, fruit smoothies, therefore, may have the potential to cause dental erosion.
Dental erosion is an increasingly common problem in dentistry which can affect both adults and children. Dental erosion has been defined as ‘the loss of tooth tissue by a chemical process not involving bacteria’.7 Acids of either intrinsic or extrinsic origin are thought to be the main aetiologic factors for dental erosion.8 Järvinen et al ranked various risk factors in developing dental erosion and identified eating citrus fruit more than twice daily, along with a history of vomiting, as high risk factors in developing dental erosion.9
The most recent Adult Dental Health Survey (2009) has reported that:
Over three-quarters (77%) of dentate adults had some wear of their anterior teeth that involved at least some dentine; and
15% had moderate wear (ie extensive involvement of dentine), with only 2% demonstrating severe wear.10
The UK Children's Dental Health Survey (2003) has reported tooth surface loss (TSL) affecting the lingual surfaces of the permanent incisors to be 14%, 30% and 33% in the 8, 12 and 15-year-old groups, respectively. There has been a 6% increase in the proportion of 15-year-olds affected by TSL since the last survey in 1993, although very little TSL was reported to involve either dentine or pulp.11
There has been a paucity of research, to date, investigating the erosive potential of fruit smoothies. Research has focused on carbonated soft drinks, carbonated diet drinks, carbonated fruit-based drinks, pure fruit juices, fruit teas, wine, ciders and alcopops.12–14 Fruit smoothies are seen as an ever increasingly popular ‘healthy’ alternative to carbonated soft drinks.
The aim of this study, therefore, was to attempt to answer two questions:
What is the range of initial/baseline pH values measured for fruit smoothies; and
What is their titratable acidity, as a measure of their erosive potential? Titratable acidity is an assessment of the total acid content of a drink.
Material and methods
Four commonly available fruit smoothies were investigated in this study:
Innocent® Strawberry and Banana;
Innocent® Mango and Passion Fruit;
Innocent® Blueberry and Blackberry; and
Innocent® Cranberry and Raspberry.
Tropicana® Smooth Orange Juice was used as a positive control. Measurements of the pH of each drink were made using a calibrated pH electrode (Microelectrodes Inc MI-410, NH, USA) connected to an Orion EA940 IonAnalyser (Orion Research, Cambridge, UK). Calibration of the pH electrode was carried out at the start of each laboratory session using standard buffers of pH 4.0 and pH 7.0.
Baseline acidity
100 mL of freshly opened fruit smoothie, which had been stored at room temperature, were placed in a plastic beaker and stirred continuously using a non-heating magnetic stirrer and a pH reading taken after 5 min. Tropicana® Smooth Orange Juice was used as a positive control. Each drink had measurements made on two further occasions to permit a mean value to be calculated.
Titratable acidity
100 mL of freshly opened fruit smoothie, which had been stored at room temperature, were placed in a plastic beaker and stirred continuously using a non-heating magnetic stirrer. All pH measurements were made after 5 min. The initial pH was noted and was followed by the addition of 0.5 mL increments of 1 M sodium hydroxide (NaOH) with the pH being noted after the addition of each increment. This procedure was continued until a pH of 7 and a pH of 10 was reached.15 Each fruit smoothie was titrated on three separate occasions to assess repeatability and to allow a mean value to be calculated. The volume of NaOH added was subsequently plotted against the pH to determine the titratable acidity of each fruit smoothie. Once again, Tropicana® Smooth Orange Juice was used as a positive control and the orange juice drink's titratable acidity was measured using the same technique.
Statistical analysis
The average initial pH levels of the five drinks and the total volume of NaOH required to reach (i) pH 7 and (ii) pH 10 for each of the drinks were compared using one-way analysis of variance with Bonferroni-corrected pair-wise follow-up comparisons. These analyses were undertaken after checking that the data were approximately normally distributed using the Kolmogorov-Smirnov normality test (all p-values>0.05).
Results
Four Innocent® fruit smoothies and Tropicana® Smooth Orange Juice (positive control) were investigated for baseline acidity and titratable acidity.
Baseline acidity
The mean pH values of the Strawberry and Banana, Cranberry and Raspberry, Blueberry and Blackberry and Mango and Passion Fruit smoothies were 3.50, 3.38, 3.49 and 3.35, respectively. The positive control of orange juice had a mean pH of 3.73. These data are displayed in Table 1, which shows that all the fruit smoothies investigated demonstrated a lower mean initial pH value than the orange juice control.
Drink
Mean pH
SD
Orange Juice
3.73
0.000
Strawberry/Banana
3.50
0.015
Cranberry/Raspberry
3.38
0.021
Blueberry/Blackberry
3.49
0.020
Mango/Passion Fruit
3.35
0.015
The analysis of variance confirmed that there were statistically significant differences between the drinks (p<0.001). The follow-up multiple comparisons identified statistically significant differences between each fruit smoothie and the orange juice control (all pair-wise p-values<0.0001). There were also significant differences between Strawberry and Banana and Cranberry and Raspberry (p=0.0001); Strawberry and Banana and Mango and Passion Fruit (p<0.0001); Blueberry and Blackberry and Cranberry and Raspberry (p=0.0001); and Blueberry and Blackberry and Mango and Passion Fruit (p<0.0001). There was no evidence of a significant difference between Strawberry and Banana and Blueberry and Blackberry (p=1.000) or Cranberry and Raspberry and Mango and Passion Fruit (p=0.4589).
Titratable acidity
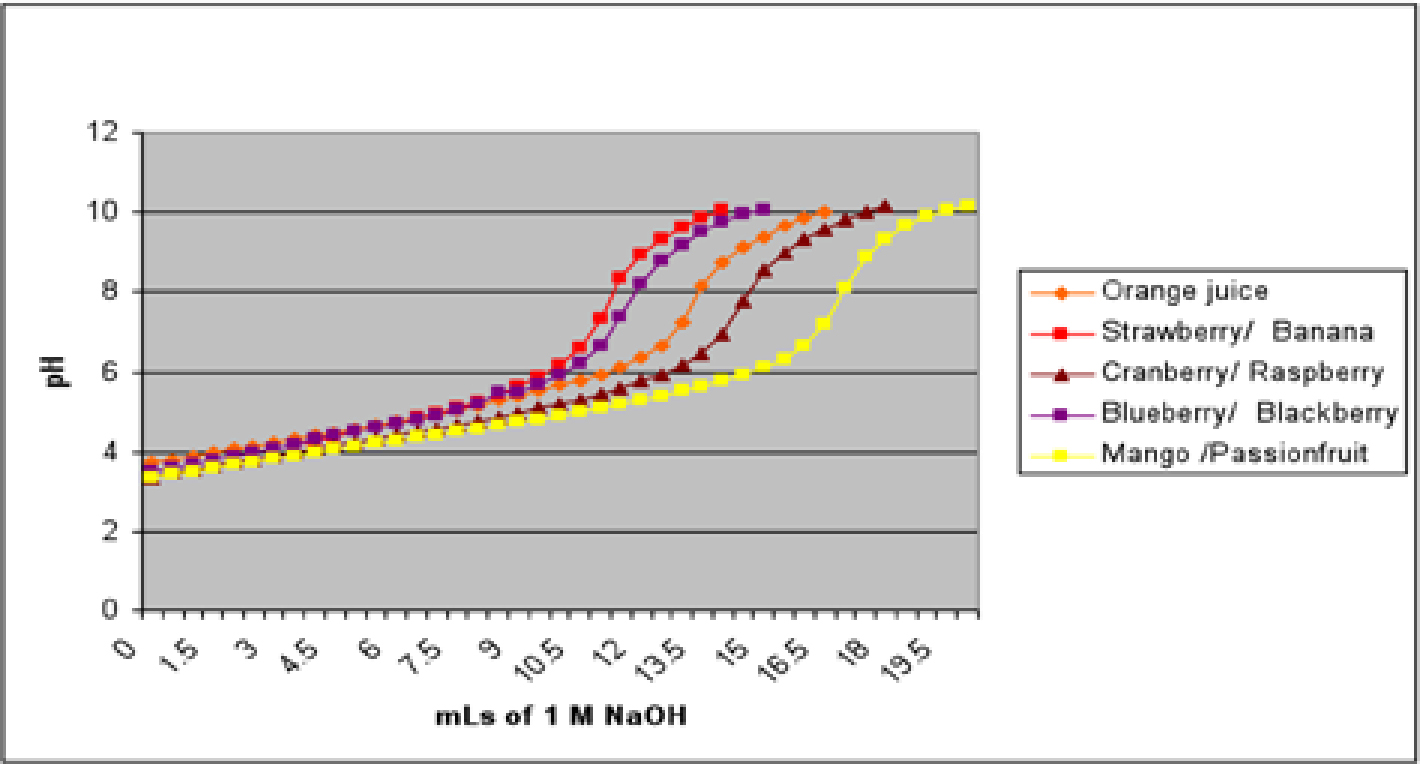
Figure 1 illustrates the titration curves for each of the four smoothie drinks, along with the orange juice control. For a drink to be considered ‘safe’ as far as dental erosion is concerned, the initial pH should be near neutral (which none of the drinks has in this test) and the titratable acidity should be ‘low’ – that is, even if the drink has a low initial pH value, the rise in pH, with the addition of alkali, should be rapid.
Figure 1. Titration curves of four fruit smoothie drinks with 1M NaOH and control.
All of the drinks, including the orange juice, start off with a pH between 3.30 and 3.80. With the addition of increments of the alkali (NaOH), all five drinks then demonstrate an extremely slow rise in pH, with the Strawberry and Banana being the earliest to demonstrate a quickened rise in pH (at the addition of approximately 11.0 mL of alkali) and the Mango and Passion Fruit being the slowest (at the addition of approximately 15.5 mL of alkali) with the orange juice control demonstrating a more rapid rise in pH at the addition of 12.5 mL of NaOH. Of all the fruit smoothies, the Mango and Passion Fruit drink required the largest volume of 1M sodium hydroxide (mean of 19.5 mL) to raise the pH to a value of 10. The Cranberry and Raspberry smoothie drink exhibited the same tendency as the Mango and Passion Fruit smoothie, starting with a low baseline pH and demonstrating a high titratable acidity, with 17.7 mL of 1 M NaOH being necessary to raise the pH to a value of 10. The Strawberry and Banana smoothie drink required the least volume of 1M NaOH (14.0 mL) to raise the pH to a value of 10. The orange juice control, despite having the highest baseline pH of all the drinks investigated, required a mean volume of 16.5 mL to raise the pH to 10 (Figure 1, Table 2). For comparability with previous work, the mean volume of NaOH necessary to raise the pH to a value of 7 for each drink is also listed in Table 2.
pH 7 (mL of NaOH)
pH 10 (mL of NaOH)
Drink
Mean
SD
Mean
SD
Orange juice
13.0
0.00
16.5
0.00
Strawberry/Banana
11.0
0.00
14.0
0.00
Cranberry/Raspberry
14.2
0.29
17.7
0.29
Blueberry/Blackberry
12.0
0.00
15.3
0.29
Mango/Passion Fruit
16.7
0.29
19.5
0.50
Analysis of variance confirmed that there were statistically significant differences between the drinks in terms of the total volume of NaOH needed to reach both pH 7 and pH 10 (both p<0.001). The follow-up pair-wise comparisons showed that there were significant differences between all pairs of drinks, for both pH 7 and pH 10 (all pair-wise p-values<0.01; Table 3).
Orange Juice
Strawberry/Banana
Cranberry/Raspberry
Blueberry/Blackberry
(i) pH 7
Strawberry/Banana
< 0.0001
Cranberry/Raspberry
0.0001
< 0.0001
Blueberry/Blackberry
0.0005
0.0005
< 0.0001
Mango/Passion Fruit
< 0.0001
< 0.0001
< 0.0001
< 0.0001
(ii) pH 10
Strawberry/Banana
< 0.0001
Cranberry/Raspberry
0.0058
< 0.0001
Blueberry/Blackberry
0.0058
0.0021
< 0.0001
Mango/Passion Fruit
< 0.0001
< 0.0001
0.0002
< 0.0001
Discussion
In 2010, 51 million litres of fruit smoothies were consumed in the United Kingdom.2 This yields an average of 0.8 litres per person and an 8.5% increase on the previous year.2 In 2007, fruit juice consumption in children is known to have accounted for 20% of all UK children's choice of soft drink.4 The additional contribution to this figure from smoothies could, therefore, be substantial. A fruit smoothie is a ‘blend of crushed and freshly squeezed fruit’. It should be 100% pure fruit with no added sugar or water and, very importantly, be made with fresh rather than concentrated juices.16 The actual current level of fruit smoothie consumption by children is unknown.
The success of fruit smoothies seems, at least in part, to be attributed to the public's perception of these drinks being considered ‘healthy’, ‘natural’ and convenient.17 The public is currently being encouraged to eat more healthily by consuming more fruit and vegetables and less saturated fat. The consumption of fruit smoothies is viewed by some as a means of fulfilling this requirement.3,17 Various ‘boosters’, such as vitamin C (ascorbic acid), aloe vera, ginseng, ginger, wheatgrass juice and bee pollen, are also offered in many smoothie bars as additional ‘shots’.1 Some smoothies are being made with so-called ‘superfruits’, such as Goji and Açai berries which, the manufacturers claim, have superior anti-oxidant properties compared to other fruit.
Erosion appears to be the major cause of TSL in childhood and adolescents.11 Some of the fruit smoothies on the market are aimed specifically for consumption by children, with ‘child friendly’ recipes and lunchbox-sized cartons of fruit smoothies. These are readily available from supermarkets, newsagents and are even sold from vending machines in some schools in the United Kingdom. Drinks consumed during school hours are either brought in lunchboxes (71%) or purchased at school (26%). Recent research would suggest that the frequency of acidic exposure may be an important factor in dental erosion.18 It is reassuring, however, to note in this regard that 77% of fruit smoothies are reported to be consumed at mealtimes.4
The investigation of the baseline pH of the fruit smoothies showed that all the drinks tested demonstrated a pH value of between 3.0 and 4.0. The differences in the mean baseline pH and titratable acidity of the various fruit smoothies could be due to the different types of acids and their concentrations in the fruit from which the fruit smoothies are prepared. The main organic acids in Mango and Passion Fruit and Raspberry and Cranberry fruit smoothies are ascorbic acid, and ascorbic, gallic, quinic acids, respectively. The term pKa is a measure of the amount of dissociation (or strength) of an acid solution. An acid molecule is made up of the conjugate base and a single proton, or hydrogen ion. When there is only one single proton available per molecule, these are known as monoprotic acids. An acid with a low pKa indicates a relatively high amount of dissociation and indicates, therefore, a relatively ‘strong’ acid. In contrast, an acid with a high pKa value indicates low dissociation and, therefore, a relatively ‘weak’ acid. Ascorbic and citric acids, however, have two (diprotic) and three (triproic) protons, respectively, available per single molecule, each of which will be released at differing pKa values. L-Ascorbic acid has a pKa1 and pKa2 of 4.04 and 11.7, respectively, whereas citric acid has a pKa1, pKa2, pKa3 of 3.13, 4.76 and 6.40, respectively.19 Gallic acid has a pKa of 4.40.20 Quinic acid has a pKa of 3.572 +/- 0.006 at 25°C.21
One reason for the high titratable acidity in the Mango and Passion Fruit and Raspberry and Cranberry smoothies could be the different ‘acid systems’, the concentrations and combinations of the fruit acids and how they compete with each other when titrated with sodium hydroxide. The way an acid behaves depends on the pH of the solution. For example, Hughes et al found that lactic acid (which is usually viewed as a ‘weak’ acid) at low pH was more erosive than either citric or malic acids, while malic acid was less erosive than either citric or lactic acids at a high pH.22 In comparison with other fruit-based drinks, eg fruit teas, flavoured mineral waters, ciders and alcopops/designer drinks, the mean baseline pH and titratable acidity of fruit smoothies were comparable.23 The fruit-based smoothies tested here had both a low pH and a high titratable acidity, which makes their erosive potential greater than orange juice. Edwards et al demonstrated that, whilst the orange juice had the highest titratable acidity of the drinks they tested, the pH of that drink was the highest, but was still deemed to be the most potentially erosive drink in that study.24 In complete contrast, the orange juice in the study reported here (which was employed as the control) demonstrated the highest pH and lowest intractable acidity when compared with all of the fruit smoothies. Thus, quite surprisingly, the fruit-based smoothies may be estimated as demonstrating far greater potential for damage to the mineralized tissues of the tooth than the orange juice.
Another factor which may have a bearing on the quantity of potential erosion that fruit smoothies could produce is the temperature at which they are consumed. Eisenburger and Addy found that, in an in vitro study, tooth erosion depth increased significantly with increasing temperature.25 The fruit smoothies investigated in this study were investigated at room temperature (approximately 25°C). Amaechi et al found, also, that the erosiveness of orange juice was less pronounced at a lower temperature although, interestingly, they found no statistical difference in pH over different temperatures.26 In any case, the temperature employed here probably simulates the highest temperature that a fruit smoothie would be consumed at and would, therefore, simulate the maximum erosiveness of the fruit smoothie.
Drinks made with fruits containing high concentrations of citric acid and vitamin C (ascorbic acid) showed, in general, a higher titratable acidity and have been linked with greater levels of dental erosion.23 Investigations of the effect of different acids on enamel have shown that more erosion was found when there was a low pH and a high acid concentration than at a high pH and low acid concentration.22 Since the fruit smoothies investigated had a high titratable acidity, it seems reasonable to assume such drinks could be potentially erosive to the human dentition.
Patients and parents should be made aware of the potential risk of dental erosion in consuming ‘healthy’ fast food such as fruit smoothies. Prevention of dental erosion is by far the preferred choice rather than restorative intervention. Treatment can be complicated and prolonged and varies from monitoring the dentition, placement of simple composite restorations, to restoration with complex extra-coronal restorations, in the case of more advanced conditions, which can be both time-consuming and expensive.27,28
Conclusions
Further research is required to determine the effect of fruit smoothie drinks on the human dentition. From the data presented here, such drinks exhibit both low baseline pH values and high titratable acidity and, therefore, may pose a potential risk of dental erosion in susceptible individuals.
Fruit consumption should still be encouraged, since it is part of a healthy diet.5 Consumption of fruit smoothie drinks, as with many other acidic beverages, should be limited to mealtimes and consumed through a straw.29,30