Reichert I, Figel P, Winchester L. Orthodontic treatment of anterior open bite: a review article – is surgery always necessary?. Oral Maxillofac Surg. 2014; 18:271-277 https://doi.org/10.1007/s10006-013-0430-5
Greenlee GM, Huang GJ, Chen SS Stability of treatment for anterior open-bite malocclusion: a meta-analysis. Am J Orthod Dentofacial Orthop. 2011; 139:154-169 https://doi.org/10.1016/j.ajodo.2010.10.019
Huang G, Baltuck C, Funkhouser E The National Dental Practice-Based Research Network Adult Anterior Open Bite Study: Treatment recommendations and their association with patient and practitioner characteristics. Am J Orthod Dentofacial Orthop. 2019; 156:312-325 https://doi.org/10.1016/j.ajodo.2019.05.005
Manfredini D, Lombardo L, Siciliani G. Temporomandibular disorders and dental occlusion. A systematic review of association studies: end of an era?. J Oral Rehabil. 2017; 44:908-923 https://doi.org/10.1111/joor.12531
Kelleher M. The ‘Uberization of orthodontics’–or how low can you go?. Orthod Update. 2017; 10:6-7
Ruparelia R, Kelleher MGD, Dhanda LS. Darwinian dentistry? Social media, smartphones and selfie sticks. Prim Dent J. 2022; 11:75-80 https://doi.org/10.1177/20501684221088434
Anterior open bites: the additive direct resin composite solution Martin Kelleher Khawer Ayub Dental Update 2025 50:1, 9-17.
Authors
MartinKelleher
MSc, FDSRCS, FDSRCPS, FCGDent
MSc, FDSRCS, FDSRCPS, FDSRCS, FCGDent, Specialist in Restorative Dentistry and Prosthodontics, Consultant in Restorative Dentistry, King's College Dental Hospital, London
This article describes a clinically proven, pragmatic approach to managing anterior open bites (AOBs) by using additive, non-destructive, freehand direct resin composite bonding. Direct composite has been used by many clinicians to solve a multitude of clinical problems. The use of these techniques and the procedural aspects have been published extensively. However, in relationship to managing AOBs there appears to be an under-appreciation by some practitioners, as well as by some in the orthodontic and maxillofacial communities, of its pragmatic use for managing many AOBs, or about what additive direct resin composite bonding could offer those patients who enquire about their realistic options to deal with their perceived concerns.
CPD/Clinical Relevance: This article seeks to raise awareness about different ways of using direct resin composite bonding (‘bondodontics’) to manage many AOBs pragmatically, at very low risk and at reasonable costs.
Article
The available options for anterior open bites (AOBs) range from doing nothing, through to doing extensive, expensive and speculative treatments.
Variations of bonding direct composite have been devised by various clinicians to solve many clinical problems, using different techniques and processes, and these have been published widely.1 Using direct resin composite bonding to manage many anterior open bites is a useful and pragmatic clinical technique.
Orthodontics, on its own, or combined with facial surgery, are recognized approaches to managing AOB problems.2,3 However, Greenlee et al4 reported on the problems of relapse with different approaches. Huang et al5 described wide variations in the treatments offered for AOBs in different centres in the USA with many subjective, institutional, or commercial factors seemingly involved in the different orthodontic/orthognathic treatment decisions about managing AOBs. The many difficult issues associated with long-term retention, including when treating AOBs, have been reported extensively.6 The uncertainties and the possibilities of unsatisfactory long-term outcomes with orthodontics, as described by Talic in 2015,7 with or without jaw surgery, ought to be described candidly to any AOB patients, and/or their guardians, as part of good ‘Montgomery consent’ processes.
This article suggests the use of some variations in the use of the additive, non-destructive, direct resin composite bonding as a pragmatic, modifiable approach. The main benefits include that it is biologically safe, time efficient, reparable and renewable, and it avoids the well-known problems of relapse and indefinite retention, mainly because the teeth and/or jaws do not get moved in the first place.
Sadly, half-truths and blatant lies about anterior open bites abound on the moronosphere of the internet, which now delivers an all-you-can-eat buffet of ill-informed opinions and some nonsensical claims. Highly dubious statements appear on some orthodontic websites (eg https://diamondbraces.com/conditions/open-bite). For instance, the Spear Education website (www.speareducation.com) contains this statement: ‘Although many cases of open bite don't require medical intervention, even a mild case can cause some dental issues later on. Having an open bite places excessive stress on the teeth that are touching properly, which erodes the enamel more quickly and puts you at higher risk of tooth decay and gum disease down the road.’
There are three fallacies in that statement alone, and the purpose appears to get people to seek extensive treatment, or to worry them unnecessarily for no good long-term health reason. The present authors challenge many of the assertions made on the internet on various platforms and on many websites. In our view, there are no robust, scientifically valid reasons to treat anterior open bites for the prevention of caries or tooth wear, or preventing future periodontitis. Similarly, there are no scientifically valid reasons for undertaking orthodontics or orthognathic surgery to prevent, or to treat, temporomandibular dysfunction (TMD) symptoms in patients with an AOB.8
Doing very little orthodontically, or surgically, avoids the risks of relapse, resorption or surgical complications.7 Most people with an anterior open bite manage chewing reasonably well. The main reasons for many seeking unbiased, neutral information, or compassionate help, are concerns about their future, or that of their child, if the AOB is not treated. However, many have understandable concerns about their appearance issues in a selfie-obsessed Instagram society.9
‘Montgomery’ and validity of consent issues
‘Montgomery consent’ means that any potential patient needs to understand the material risks and benefits of the viable options available to them in order to make their consent valid.
As is the case in many areas of healthcare, a useful acronym for patients to use is ‘BRAN’. That acronym is made up from the first letters of Benefits, Risks And Nothing. The realistic possibilities, including doing nothing, very much ought to be presented in a fair and unbiased way. If some relevant information is concealed from a patient, whether deliberately or subconsciously, in order to treat someone orthodontically, or orthognathically, or in some other way, if there are complications of relapse, resorption or some other problems during, or afterwards, then any patient might well complain later on.
A claim could be based on the validity of their consent, possibly alleging that they would not have had such extensive or speculative treatments, which resulted in some later unsatisfactory or unstable outcomes, if they had known in advance that there were viable and safer alternatives that were (in theory at least) available to them.
Aggressive advertising of aligners and direct-to-consumer orthodontics is likely to lead to longer-term problems of relapse and resorption with serious complaints, or claims, likely at some stage.10 Sadly, many cases are only treated by ‘additive bondodontics’ after there have been failures or serious complications, such as resorption and/or relapse, as is shown in the first case.
Case 1
History and presentation
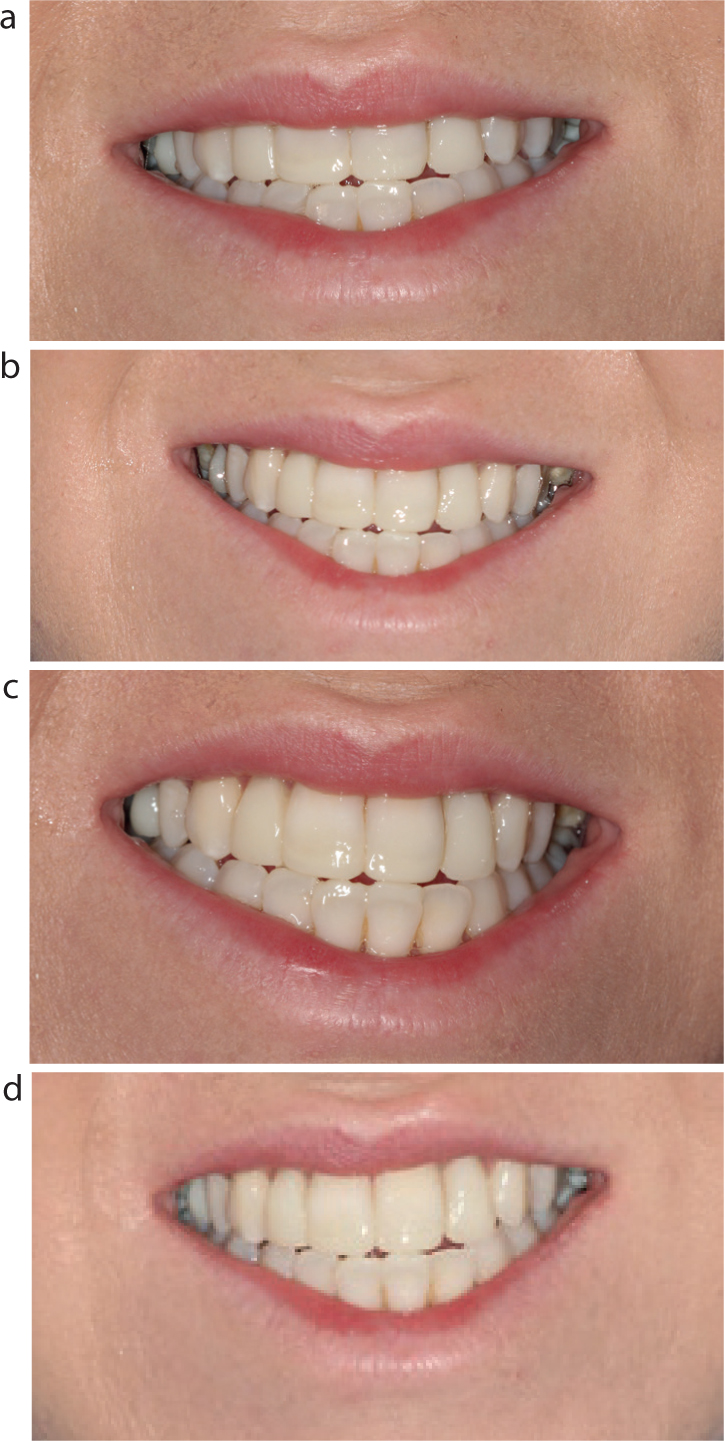
A 23-year-old female presented on a restorative clinic because she was unhappy with her dental appearance (Figure 1). She did not like the gaps between her upper and lower teeth, or her crooked upper right lateral incisor, which was in crossbite.
Figure 1.
(a–c) The initial clinical presentation, showing the AOB between the maxillary and mandibular incisors in ICP, but with (b,c) a crossbite between the palatally instanding and crowded upper right lateral incisor and the lower right canine.
She reported that her dental appearance problem was present despite two courses of fixed orthodontics and further treatment with aligners. The patient stated that, after each course of orthodontics, ‘the teeth just went back towards their original positions in spite of her trying to wear her retainers.’
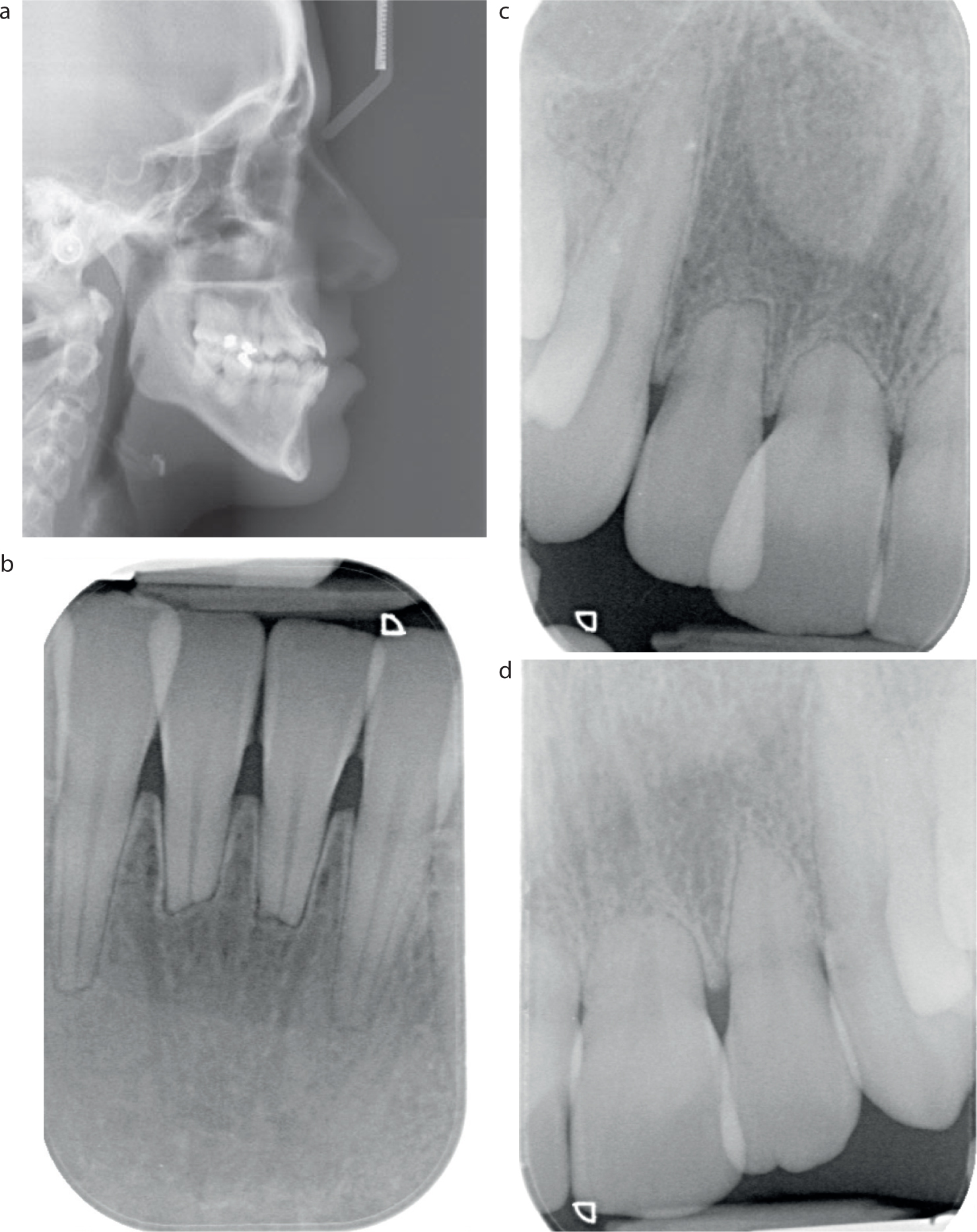
Apparently, someone in an orthodontic department elsewhere took the radiographs shown in Figure 2, but declined to get involved, probably on the grounds of the obvious root resorption that was present on the upper and lower anterior teeth, and therefore referred her back to her dentist with that refusal. Subsequently, her dentist referred her to the Department of Restorative Dentistry at King's College Hospital for another assessment.
Figure 2. Radiographs confirmed the (a) skeletal AOB issues as well as (b–d) the extensive root resorption following previous orthodontic treatments.
Assessment
There was an obvious AOB present, with a crossbite between the crowded upper right lateral incisor and the lower right canine. All the central incisors were proclined, and there was marked gingivitis present. Clinically, the anterior teeth appeared to be surprisingly firm in spite of their short, resorbed roots (Figure 2b–d).
Discussions, diagnostic, readily reversible composite mock-up and consent
After some initial discussions, verbal consent was given to evaluate some temporary appearance changes. The front teeth were just dried (not etched) and a readily reversible direct composite mock-up, using shade A1 chilled hybrid composite, was done to show the patient some possible changes for her assessment and for her comments.
That temporary ‘walking diagnostic composite bond-up’ (similar to Figure 3a) was photographed for clinical record reasons, but it was also photographed on the patient's mobile phone as a ‘selfie’.
Figure 3.
(a) A temporary, readily reversible, diagnostic composite bond-up similar to this was performed on the unetched teeth for the patient's evaluation and her comments. (b–d) Following discussions and written consent being received, then, at one subsequent long appointment, the teeth were bonded using chilled direct composite to replicate the previously agreed visual outcome.
It was left in position for a few days for the patient, and any others to evaluate that possible option prior to the patient flicking it off with a metal nail file. The appearance (ie without the direct resin composite mock-up), was then photographed on her smartphone from different angles, thereby allowing her, and any interested others, to make direct comparison between her existing dental appearance situation and one possible option.
It was made very clear in the early discussions that the possible deal on offer was ‘limited self-improvement with self-preservation, but no self-destruction.’ Because the diagnostic bond-up was not polished or finished initially, it allowed for some ‘under-promising and over-delivering’.
Other options discussed included doing nothing, doing some pragmatic bonding, similar to the demonstrated mock-up (Figure 3a), possibly extracting the instanding upper right lateral incisor to be followed by its immediate replacement with a fibre-reinforced composite bridge from the upper right canine, to be performed along with other direct composite bonding at that visit, or re-treatment with orthodontics, up to and including undertaking multiple extractions prior to some prosthodontic replacement of different types of varying aggressiveness or predictability.
It was stated, both verbally and in writing, that that if pragmatic direct bonding was going to be done for real, that the outcome was not going to be either ‘perfect’ or ‘permanent’ and that the oral hygiene needed to be much better before, and after, any possible treatment.
The patient declined extractions, even though it was emphasized that the instanding upper right lateral incisor position was always going to be problematic.
Sometime after those extensive discussions, written acceptance was received in which the patient accepted her oral hygiene responsibilities and that the composite would need polishing and eventual re-surfacing, which could be done by any dentist, but that this aspect would be her own long-term responsibility.
Discussions, pragmatic treatment planning and rationale
The main objectives of the additive direct bonding were to make the tips of the upper and lower incisor teeth appear to be parallel to the interpupillary line, while eliminating most of the irregular dark spaces around, and between, the visible anterior teeth. The incisal tips would be made to follow the outline of the lower lip and to be only in light contact.
Treatment details
The patient had some local anaesthetic (LA) prior to one session of direct, freehand, additive composite bonding, using a total etch approach, a three-bottle bonding system and chilled hybrid composite. The LA was provided for patient and operator comfort, so that the finishing at the gingival margins caused no discomfort.
The chilled hybrid composite was applied freehand to both sides of the etched and bonded upper anterior teeth and light cured to provide a rough matrix. Doing that first reduced the irregular and asymmetric dark spaces, which highlighted the negative anterior occlusal plane problems.
The tips of the top teeth were then brought downwards, and the tips of the lower teeth were brought upwards, to be in light contact and made to follow roughly the outline of the lower lip.
Because the teeth were not moved from their present positions, and the newly bonded shapes had wider and tighter contact areas, that combination stopped later unfavourable tooth movements.
Follow-up
Apart from a quick annual polish, no other treatment was required or performed during the next 4 years.
Discussion of technical and consent aspects
Freehand pragmatic additive hybrid resin composite was used after it had been chilled to stop it from slumping, without any articulated models, or a laboratory-made diagnostic wax-up, or any fiddly matrix being used.
Those traditional laboratory and clinical processes contribute little in achieving a reasonable result, which is based largely on the patient's realistic visual assessment of the initial reversible composite mock-up, which had been done directly in her mouth at the first visit and modified slightly after her initial comments. That original clinical appearance, and the diagnostic direct composite mock-up had both been photographed to manage her expectations as representing ‘the deal that was on offer’ – no more and no less.
In most anterior open bite cases, there is plenty of etchable enamel available for predictable bonding purposes. In such situations, the physical properties of bulk of direct resin composite are optimised, because in AOB cases it is being used in thick section, and it is not being subjected to massive shearing or tensile forces.
A suggested simple ‘formula’ for managing anterior open bites using pragmatic additive composite bonding
It is the appearance of the irregularities of the multiple dark spaces around the teeth that most patients do not like. Adding direct resin composite eliminates those visibly dark areas by stopping light transmission through there. Just doing those simple changes addresses most patients' main concerns.
The tips of the upper and lower teeth should be made parallel to the interpupillary line – an imaginary line joining the pupils of the patient' eyes, and should be made to follow the outline of the lower lip.
The dark spaces, which highlight the negative anterior occlusal plane problems, can be reduced pragmatically by bringing the tips of the upper teeth downwards, and bringing the tips of the lower teeth upwards, mainly on the insides of the teeth, as deemed to be appropriate following a bit of initial ‘eyeballing’ by both the clinician and the patient.
The individual teeth should be ‘anonymised’ by minimizing the length differences between all four incisors and the adjacent, usually pointy, canines, which can be bleached selectively and bonded as required.
It is wise to make the incisal tips slightly longer than is expected to be needed. It is very easy to adjust the incisal tip lengths or shapes, as requested by the patient, by using a fine felt-tipped black permanent ink pen (Staedtler) to draw on the incisal tips to simulate what that particular patient thinks the desired incisal lengths and shapes of their teeth should be.
If that initial simulation of the lengths made by drawing on the cured composite with the black permanent ink is not what that patient finds attractive, then one can use surgical spirit to clean off that dried ink quickly. One can then use the fine felt tip black permanent ink pen to try again and do that as often as necessary until the patient expresses their approval.
Once those incisor tip lengths have been approved by the patient, one simply grinds off just the areas of composite covered by that black ink to provide that patient's preferred shapes and lengths.
Application of minor variations of those ideas is all that is required in most AOB cases. However, it is important in managing patient expectations realistically, that the patient's non-verbal and verbal reactions (and those of any relevant others) to those possible, but reversible, changes are assessed quickly and carefully, immediately by the experienced clinical team after doing that direct composite mock-up on their dried (not etched) enamel.
If the patient appears negative or largely unimpressed, then sit the patient back in the chair and gently flick off the reversible composite. It is advisable to walk away, or to gently excuse yourself at that point, preferably without charging the patient anything.
In extricating oneself from what has not impressed that patient, or perhaps when something in the patient's reactions has worried any one of your clinical nursing team, it is sometimes wise to use words such as: ‘I do not think that I am the person who can help you as much as you deserve. You might be wise to get the opinion of someone else who might be able to help you more than I can.’
If you do not accept any payment, you may well have saved yourself a lot of grief in the long term, because their expectations are unlikely to be met by the proposed direct bonding treatment approach. Instead, to maintain a cordial relationship, you can suggest that they should see some other specialist, or other colleague for their opinion instead of yours, and that you would be happy to help to arrange that, but only if requested by them to do so.
Even if the patient appears enthusiastic and very positive about those possible elective changes with the readily reversible diagnostic composite mock-up, it is also important to emphasize that this option has limitations, and that ‘it is not going to be either permanent or perfect, but it will probably look a bit better than the current anterior open bite.’
Attention needs to be drawn to the facts that having it done for real will keep the residual sound structure of their teeth, but that it will have associated costs, including those involved with the initial treatment, polishing, maintenance and probably re-surfacing or re-doing at some time in the future. Those aspects need to be discussed candidly, in a neutral way, as being just one possible option among others.
No commitment should be made, by either side, until everyone involved has had enough time to reflect carefully on what might be involved and any issues arising. It is important that any queries have been dealt with honestly and fairly and, obviously, only when a mutually acceptable fair fee has been agreed, all depending on what is expected to be involved.
Case 2
History
A 36-year-old male patient presented in practice with an AOB, a fractured maxillary incisor and a crossbite on the right side (Figure 4). At three previous consultations he had had elsewhere, he had been told that his only real option to ‘cure his anterior open bite’ was to have prolonged fixed orthodontics and extensive jaw surgery to be followed by a ‘full mouth rehabilitation.’
Figure 4.
(a–d) The problematic anterior open bite, with an obviously fractured upper right central incisor. (a,c,d) Note the crossbites in the premolar regions.
He did not like his smile, but he did not really fancy the prolonged orthodontics, let alone the proposed jaw surgery and multiple crowns to address his appearance issues. On direct questioning, he reported no problems with chewing or with TMD.
Assessment and discussions
The root lengths, bone levels and pulp tests were all normal.
Following some preliminary discussions, a readily reversible temporary direct resin composite mock-up was performed at that first appointment on the dried, but not etched, teeth by applying the formula outlined above, using just some chilled hybrid resin composite.
That temporary appearance change looked roughly similar to what appears in Figure 5c and was carried out in approximately 45 minutes to show to the patient what might be achieved without orthodontics or surgery.
Figure 5. Unfortunately, the patient had a less than ideal gingival condition, which showed inflammation and erythema. He was counselled about this, and, by the end of treatment, the gingivitis had successfully resolved with more focused oral hygiene. (a) Chilled direct composite was added lingually and palatally and cured to provide a matrix against which to drag and sculpt the incisal lengthening composite. (a,b) The lower incisal tips were raised pragmatically by about half the height of the dark gap. (c) The dark gaps were eliminated to ‘anonymise the smile’ and made the upper teeth incisal tips parallel to the interpupillary line. (c,d) The same length teeth followed roughly the outline of the lower lip. Addition of direct buccal composite concealed the premolar crossbites.
The patient expressed immediate enthusiasm for those possible changes in his smile, particularly as it would mean avoiding the considerable future travel and time commitments, as well as the risks and costs involved in the previously proposed orthodontics, jaw surgery and some destructive conventional crowns for a supposed ‘occlusal rehabilitation’.
He photographed those possible changes in his dental appearance on his smartphone and some clinical images were taken for records/consent reasons. The reversible composite bond-up was then flicked off with a standard sickle scaler.
More ‘selfie ‘photographs of the existing appearance were then taken from different angles, again on his own mobile phone to allow him, and any interested others, to assess that possible option in his own time.
Consent issues
The patient already knew a lot about the risks and time involved in the other more aggressive options from his three previous consultations elsewhere. It was explained that the ‘material risks’ here were of slow surface deterioration of the composite, which could be managed easily with polishing or re-surfacing, by any dentist. However, the existing teeth and their roots would remain stable and still structurally sound. There would be no risks incurred of possible resorption, relapse or problems from a general anaesthetic, or of serious pain or other risks, such as nerve damage, or the potential problems of removal of his existing sound tooth structure for full crowns – unlike the potential plans that had been previously proposed.
Following receipt of the patient's written confirmation of his understanding of the proposed risks, benefits, limitations, costs, fall-back positions and confirmation of his full awareness of his other options, the patient was scheduled for one open-ended all-afternoon appointment.
Technical treatment details
Under LA, small sections (roughly 5-mm long) of non-cutting ends of Komet serration strips (West One, Croyden) were inserted between the adjacent teeth to prevent etching of their long adjacent enamel surfaces.
Following check-etching with viscous phosphoric acid gel to ensure that all target surfaces of all target teeth went frosty after washing and drying, the small sections of the non-cutting ends of Komet serration strips were removed, washed, dried and then re-inserted between the teeth.
The hydrophilic resins from a three-bottle bonding system (All-Bond 2, BISCO, Schaumburg, IL, USA) were prepared by mixing one drop from bottle A, mixed with one drop from bottle B, in a plastic disposable dappen dish.
That mixture of hydrophilic resins was applied with disposable fine brush, left in position for 20 seconds and then blown dry so that the etched surfaces went from being visibly frosty to being visibly shiny.
The small sections of the non-cutting Komet metal strips were then removed, re-dried and reinserted between the teeth before the hydrophobic resin was applied with a brush and air thinned to stop the hydrophobic resin from pooling against the ultra-thin small metal strips.
The small sections of the thin metal strips were then removed, and the hydrophobic resin was cured without those metal strips being present. The metal strips were not now reinserted.
That meant that one could now sculpt the chilled resin composite material from any angle, without any interference from the metal strips, and make the teeth to be any pragmatic shape or height that was deemed to be desirable quite quickly.
Some chilled hybrid resin composite (Charisma, Kulzer Shade A1; Kulzer, Basingstoke) was applied freehand on to the lingual surfaces of the lower front teeth and cured in position (Figure 5a,b).
Doing that first created a pragmatic matrix against which it was very easy to sculpt more composite to lengthen the relevant lower teeth in order to eliminate some of the visibly dark areas between the lower and upper teeth
Something similar was done to the palatal aspects of the top front teeth, and more composite was added to that initial pragmatic matrix of cured composite to produce a roughly correct estimated length to eliminate the dark shapes between the upper and lower front teeth and then, all that was bonded in position.
Once the chilled composite had been cured on all the relevant teeth some initial shaping was carried out using a Komet H 48 LQ bur and a Jet FG 7901 (West One), so that the newly added composite followed roughly the outline of the lower lip.
Further adjustments were made until the articulating paper marks showed that the composite was not being subjected to excessive shear or tensile forces (please see suggested formula above).
Also, 20-mm sections of Komet serration strips were used to cut through the residual inter-proximal resin, leaving flat tight contacts.
Follow up
The teeth and composite remained stable and were polished on an annual basis, as had been agreed, but no other treatment was carried out or required for 4 years. There were no TMD issues, or any other problems reported.
Case 3: closure of an anterior open bite caused by acromegaly
History
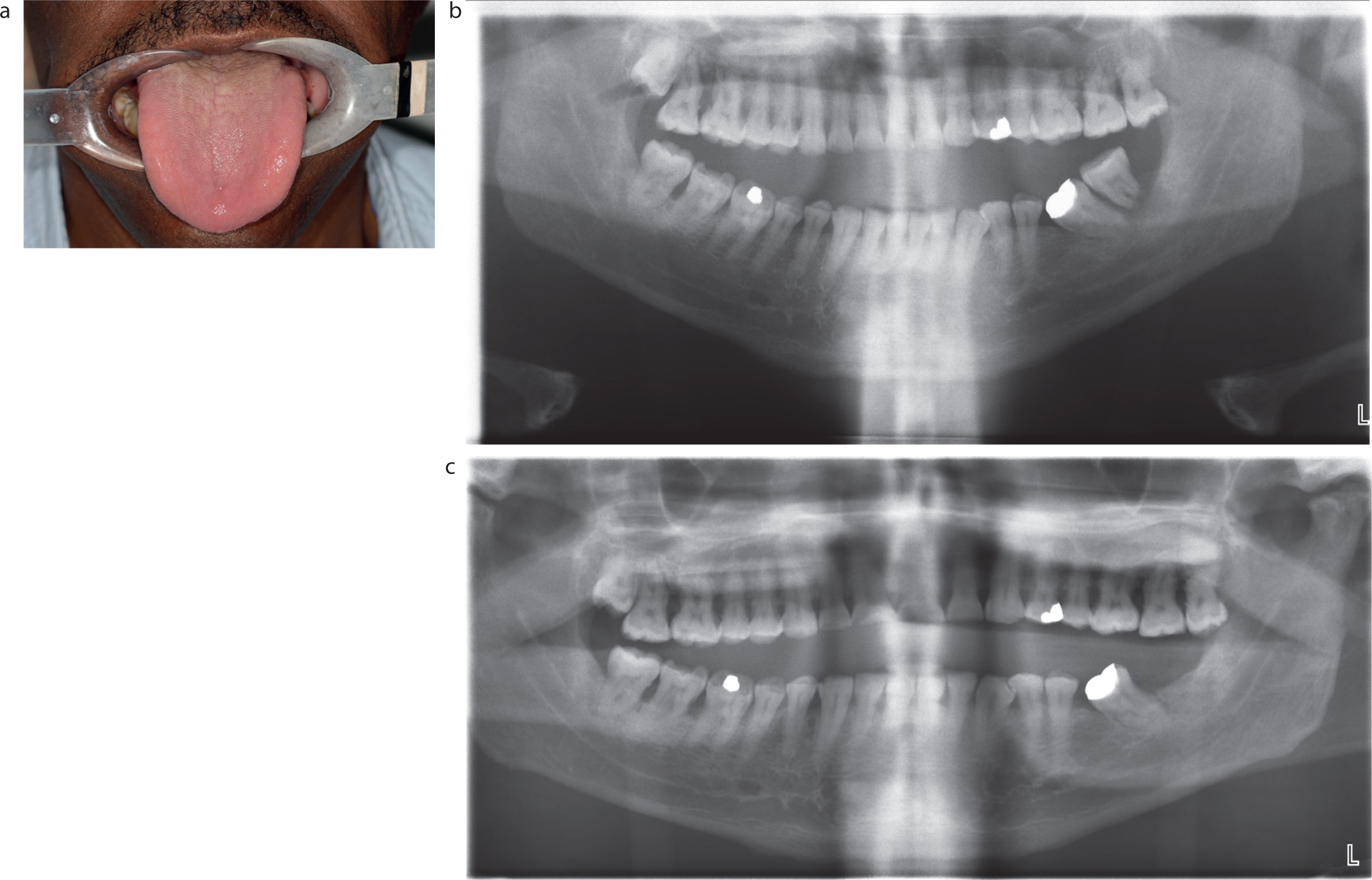
A 54-year-old male of African origin presented with a diagnosis of acromegaly, which was being investigated by the neurosurgeons. The problems with the changes in his hands, feet and jaws had started 1 year previously, but now his main complaint was that the front teeth did not meet. He was not in any pain.
Clinical and radiographic examination
There was an anterior open bite of 11 mm in the central incisor region. He had a bimaxillary proclination and the classic very large tongue seen in acromegaly (Figure 6a). The only contacts were on the last molars. Examination of the teeth showed average occlusal wear, signifying that those worn teeth must have been in contact for much of his life. Localized periodontitis (stage 4, grade C) was noted in the molar sextants (Figure 6b,c).
Figure 6.
(a) Macroglossia was noted. (b) An OPT showed, among other things, the AOB and gross overeruption of the lower left and right third molars with advanced periodontitis and terminal bone loss at LL8. (c) A later OPT, taken after the neurosurgical removal of his 15-mm diameter pituitary adenoma, showed the ongoing AOB, bone loss associated with the established periodontitis and the now missing lower left last molar.
Occlusal examination and initial discussions
Study casts were taken and mounted on a Denar Mk 2 articulator (Prestige Dental, Bradford) in the retruded contact position (RCP)(Figure 7). Lengthy discussions of some options and their limitations were undertaken, most of which were similar in content to those outlined in the previous two cases.
Figure 7.
(a) The mounted study casts confirmed the extent of the AOB and that the only occlusal contact were at the right last molars. (b–d) There was the obvious tooth surface loss visible both occlusally and buccally on the mounted study casts. It had been suggested initially that the last molar in both lower quadrants and the one in upper left quadrant should be removed reasonably soon to see what effect that might have had on his being able to bite better, but this was declined by the patient who decided to wait until after removal of his large pituitary adenoma before having any teeth extracted. Unsurprisingly, the lower left last molar exfoliated.
Discussions and option planning
After the neurosurgical removal of the15-mm diameter pituitary adenoma, some months were allowed to elapse before further discussions about various options and their limitations and risks were undertaken, with the help of the mounted study casts, photographs and radiographs to help the patient to visualize his problems. Emphasis was placed on the patient's resposibiities in terms of daily use of various sizes of long-handled tapering interdental brushes from both sides of all his teeth, as well as the use of a single-tufted brush to be used vertically.
A video was made on his own smart phone of him using these cleaning devices correctly to act as a reminder for him when doing this required more effective interdental and intracrevicular cleaning, which would be a prerequisite and ongoing requirement before, and after, any bonding might be performed to help with the anterior open bite.
Following written confirmation of his understanding of the risks and benefits and doing nothing (‘BRAN’ analysis), and answering some queries openly and honestly, he was scheduled for one open-ended session for additive direct resin bonding.
Basically, that involved applying the previously mentioned formula and technique using chilled direct resin composite to close the anterior open bite and establish pragmatic occlusal contacts on many more teeth (Figure 8).
Figure 8.
(a,b) The post-bonding position. (c) The 2-year post-operative OPT shows the variations in thickness of the pragmatic, non-destructive, direct composite additions that were bonded to the different teeth to bring them in to functional contact. There was little further bone loss at the compromised upper molars because the patient was using different diameter long-handled tapering interdental brushes every day from both sides. (d) Additive pragmatic bonding established functional occlusal contacts on many teeth without damaging the important load-bearing ring structures of the teeth. (a–d) The tips of the anterior teeth were made parallel to the interpupillary line and made to follow the outline of the lower lip, while reducing the visibly dark anterior gap. That pragmatic direct resin composite bonding, which was added without damaging the sound structure of his teeth, could, and can, be modified in any way required at any stage
Follow-up
The patient was followed up for 3 years and reported ‘having no problem chewing anything he liked’.
Discussion
Anterior open bites: the additive direct resin composite bonding option to help solve perceived problems of open bites. Who cares and so what?
Regardless of the aetiology, direct resin composite additions can offer a biologically sensible, affordable, quick and stable treatment for managing anterior open bites.
Most orthodontists focus on genetic, skeletal and soft tissue issues primarily, which is entirely understandable, because they account for many cases that they see routinely.2
However, for consent reasons, patients with perceived problems from their anterior open bite, or their parent, or their guardians, need to be made very aware, early on in any discussions, that such traditional approaches of orthodontics, with or without jaw surgery, involve considerable time, costs, and risks. For instance, such traditional approaches often carry risks of significant instability afterwards, and the probable need for effective long-term retention indefinitely, without which high rates of relapse have been reported.4,6
In contrast to these approaches, viable direct and other pragmatic bonding options were, and are, in theory at least, available.
Condylar fractures, rheumatoid arthritis, or conditions such as acromegaly (qv) are among various causes of anterior open bites, most of which can be managed effectively with additive direct bonding of (usually) just the relevant teeth. In theory at least, that can be carried out by any dentist of average skill, if given enough time and resources, often in a matter of hours.
Similarly, lateral and posterior open bites have been, and can often be, managed reasonably predictably by different bonding techniques.
Summary
In most anterior open bite cases, chilled composite can be used directly in the mouth as a readily reversible ‘temporary mock-up’ material to assess whether direct bonding might offer an acceptable approach for that particular patient. Chilling hybrid composite reduces its slumping and makes it very easy to apply freehand from any chosen angle.
The important things to do are to apply some of the direct composite to the inside of the target teeth and cure that first to provide a pragmatic matrix.
One can then sculpt more composite so that it eliminates most of the irregular dark visible spaces anteriorly, while also making the tips of the upper and lower incisor front teeth parallel to the interpupillary line.
All the upper and lower incisal tips should be ‘anonymised’ by reducing the length and shape differences between them, while making the incisal tips follow roughly the outline of the lower lip (as described in the suggested formula above).
The lengths and shapes of the incisal tips of the bonding can be modified quickly by using a black permanent ink pen to draw on them to simulate whatever shapes that a patient would like, before subsequently grinding that ink-covered area to produce the patient's desired incisal lengths or shapes.
The validity of ‘Montgomery’ consent is based on a direct composite mock-up having been done on the existing teeth and photographed. Doing that first allows for two-way discussions, without commitments from either side, based on a realistic, but readily reversible simulation of what is being proposed because nothing has been etched at that point.
In any detailed discussions, it is often helpful to explain to patients that the proposed ‘additive bonding’ result involves ‘some self-improvement’ which can be achieved with ‘self-preservation’ but does not involve ‘self-destruction’. However, the result will not be perfect or permanent, and will require maintenance and probable resurfacing – at the patient's expense – in the longer term. The readily reversible composite resin bond-up, can be photographed on the patient's smartphone as a record of what is really on offer, no more and no less, as an important part of the candid and neutral discussions of it being just one of their viable options for consideration.
Following the easy removal of the trial bond up with a sickle scaler, further ‘selfies’11 of the existing appearance should be taken on that patient's smartphone, from different angles immediately, so that they can be present beside the pictures of the trial composite mock up for comparison for as long as that patient wishes.
The patient can discuss matters with anyone of significance in their lives and they should be encouraged to take as much time as they like time to process, in their own mind, what the limitations are in the promised result with it being neither perfect nor permanent, nor likely to look any better than what has been shown to them. However, as clinicians, one can hope to improve on that initial reversible mock-up with some re-shaping and detailed polishing, but it is very wise not to mention that to the patient at that stage to ensure that they have limited expectations. In other words, aim to ‘under-promise and hope to over-deliver.’
Direct resin composite additions do not damage the teeth, unlike aggressive ceramic veneers or full crowns and, because the teeth have not been moved recently, the result should be stable.
Direct resin composite can be bonded pragmatically in various shapes to different teeth (please see the radiograph shown in Figure 8c).
In the case of a significant AOB, the direct resin composite is being bonded mainly to very predictable enamel and is bonded in very thick section and will be loaded in compression. Under those circumstances direct resin composite is a great material. Composite is only a poor material when it is placed in thin sections and when subjected to massive shear or tensile stresses. None of those things apply when it is being used for managing anterior (or indeed lateral or posterior) open bites. A total etch and a three-bottle bonding system remain the gold standard and that system was used in all the cases shown.
The formula for dealing with anterior open bites that was suggested above and those materials and techniques have been used over many years to succesfully treat very many other open bite cases of different types. It is very easy to add, subtract or modify the direct composite material if that becomes indicated at any stage.
The material is available in a wide variety of colours, filler sizes and viscosity, usually at very modest cost. Finally, although direct composite additions do not last indefinitely, and they do not supply the ridiculous, mythical ‘perfect smile’, they can provide rapid and usually acceptable improvements for many people with an anterior open bite.
It involves using a non-destructive additive, reasonably durable, proven material that is capable of being sculpted, shaped, finished, re-polished or re-surfaced, or replaced, by any competent dentist anywhere in the future – if that dentist happens to have any interest in doing such pragmatic treatments and they are given enough time and resources to make it a viable proposition to do so.
Finally, perhaps before advocating prolonged orthodontics and risky, unpleasant and possibly unstable facial surgery for anterior open bites, experienced and compassionate dental professionals, orthodontists, or maxillofacial surgeons, might wish to consider ‘the daughter test’, which is - ‘knowing what I know about all the things that might be involved, both now and later on, would I do this proposed orthodontic or orthognathic treatment on my own daughter?’12 (For which please read any other very close family member.12)
Not quite sure? Possibly consider asking a colleague with the requisite skills to do a quick, readily reversible, direct diagnostic composite mock-up on the dried teeth first for full and frank discussion with the patient, possibly to be followed by one long session of non-destructive additive direct composite bonding?