In: Bailey M : United States Environmental Protection Agency; 2013
Walker BLSeattle; London: University of Washington Press; 2010
Wilson NHF, Gelbier S: British Dental Association; 2014
Lynch CD, Wilson NHF Managing the phase-down of amalgam: part I. Educational and training issues. Br Dent J. 2013; 215:109-113
Combe EC, Burke FJT, Douglas WHChicago: Kluwer Academic Publishers; 1999
Burke FJT Dental materials – what goes where? The current status of glass inomer as a material for loadbearing situations in posterior teeth. Dent Update. 2013; 40:840-844
Gurgan S, Kutuk ZB, Ergin E, Oztas SS, Cakir FY Four year randomised controlled clinical trial to evaluate the clinical performance of a glass ionomer restorative system. Oper Dent. 2015; 40:134-143
Gavic L, Gorseta K, Glavina D, Czarnecka B, Nicholson JW Heat transfer properties and thermal cure of glass-ionomer dental cements. J Mater Sci Mater Med. 2015; 26
Opdam NJM, Bronkhorst EM, Loomans BAC, Huysmans MC 12 year survival of composite vs amalgam restorations. J Dent Res. 2010; 89:1063-1067
Rodolpho PADR, Donassollo TA, Cenci MS, Loguércio AD, Moraes RR, Bronkhorst EM, Opdam NJ, Demarco FF 22-Year clinical evaluation of the performance of two posterior composites with different filler characteristics. Dent Mater. 2011; 27:955-963
Pallesen U, van Dijken JW, Halken J, Hallonsten A-L, Höigaard R Longevity of posterior resin composite restorations in permanent teeth in Public Dental Health Service: a prospective 8 years follow up. J Dent. 2013; 41:297-306
Opdam N, van de Sande F, Bronkhorst E, Cenci M, Bottenberg P, Pallesen U Longevity of posterior composite restorations: a systematic review and meta-analysis. J Dent Res. 2014; 93:943-949
Astvaldsdottir A, Daerhamn J, van Dijken JWV, Naimi-Akbar A, Sandborgh-Englund G, Tranieus S, Nilsson M Longevity of posterior resin composite restorations in adults – a systematic review. J Dent. 2015; 43:934-954
Audience response systems in higher education: applications and cases. In: Banks DA Hershey Pa: Information Science Publishing; 2006
Shon H, Smith L A review of Poll Everywhere audience response system. J Technol Hum Serv. 2011; 29:236-245
Brunton PA, Burke FJT, Sharif MO, Creanor S, Hosey MT, Mannocci F, Wilson NHF Contemporary dental practice in the UK in 2008: aspects of direct restorations, endodontics and bleaching. Br Dent J. 2012; 212:63-67
Soderholm KJ, Mariotti A BIS-GMA – based resins in dentistry: are they safe?. J Am Dent Assoc. 1999; 130:201-209
Rasines Alcaraz MG, Veitz-Keenan A, Sahrmann P, Schmidlin PR, Davis D, Iheozor-Ejiofor Z Direct composite resin fillings versus amalgam fillings for permanent or adult posterior teeth. Cochrane Database Syst Rev. 2014; 3
Kwang S, Aminoshariae A, Harding J, Montagnese TA, Mickel A The critical time-lapse between various restoration placements and subsequent endodontic intervention. J Endod. 2014; 40:1922-1926
Hunter A, Treasure E, Hunter A Increases in cavity volume associated with the removal of class 2 amalgam and composite restorations. Oper Dent. 1994; 20:2-6
Purk JH, Dusevich V, Glaros A, Spencer P, Eick JD In vivo versus in vitro microtensile bond strength of axial versus gingival cavity preparation walls in Class II resin-based composite restorations. J Am Dent Assoc. 2004; 135:185-193
Hashimoto M A review – micromorphological evidence of degradation in resin-dentin bonds and potential preventional solutions. J Biomed Mater Res. 2010; 92:268-280
Beazoglou T, Eklund S, Heffley D, Meiers J, Brown LJ, Bailit H Economic impact of regulating the use of amalgam restorations. Public Hlth Reps. 2007; 122
Lynch CD, Wilson NHF Managing the phase-down of amalgam: part II. Implications for practising arrangements and lessons from Norway. Br Dent J. 2013; 215:159-162
Fleming GJP, Hall DP, Shortall ACC, Burke FJT Cuspal movement and microleakage in premolar teeth restored with posterior filling materials of different reported volumetric shrinkage values. J Dent. 2005; 33:139-146
British society of prosthodontics debate on the implications of the minamata convention on mercury to dental amalgam – should our patients be worried? Rupert Austin Shiyana Eliyas FJ Trevor Burke Phil Taylor James Toner Peter Briggs Dental Update 2025 43:1, 8-18.
In 2013, the Minamata Convention on Mercury called for a global phase-down of amalgam use, with a view to reduce environmental mercury pollution. This will significantly impact UK dentistry, given the still extensive use of amalgam in UK general dental practice. However, until now there has been little national discussion or debate. In Spring 2015, The British Society of Prosthodontics dedicated a significant part of its Annual Conference to debating the implications of this issue. Clinical case examples were discussed with audience interaction and voting facilitated using innovative Audience Response System Technology. A remarkable range of concerns and opinions were given. The debate elicited specific concerns amongst clinicians regarding the suitability of mercury-free alternatives to amalgam; particularly where cavities are large and extend beneath the gingival anatomy. There are also anecdotal reports of Dental Foundation (DF) dentists not being adequately taught the use of dental amalgam in undergraduate dental schools.
CPD/Clinical Relevance: Many clinicians, especially those treating patients for whom moisture control is challenging, feel that amalgam should remain available for clinicians to choose in certain clinical circumstances for the restoration of posterior teeth, even in the event of a complete phase-down.
Article
The phase-down of amalgam
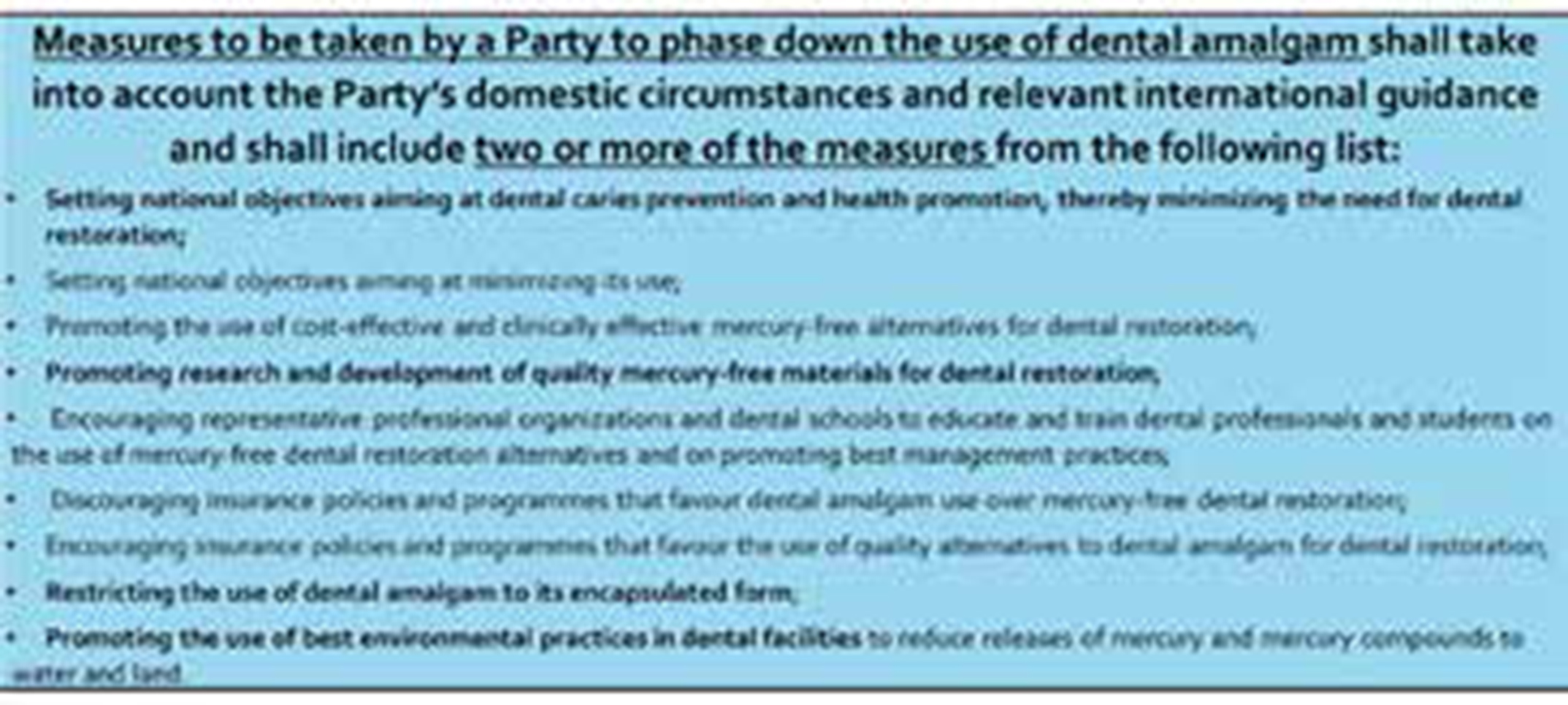
The Minamata Convention on Mercury, a United Nations treaty signed on the 10 October 2013 by 128 signatory nations, including the UK, was designed to protect human health and the environment from anthropogenic emissions and releases of mercury and mercury compound.1 Minamata Bay in Japan was heavily polluted from the 1930s by wastewater, mixed with mercury, dumped into Hyakken Harbour from the Chisso Corporation's factory in Minamata, particularly by methylmercury. The highly toxic compound bio-accumulated in fish and shellfish in the bay which, when eaten by the people living around the bay, gave rise to Minamata disease (mercury intoxication) affecting more than 10,000 people.2 Article 4 on the Convention addresses the question of mercury-added products and includes specific requirements for signatory nations regarding the use of dental amalgam. The requirements are shown in Figure 1.
Figure 1. MINAMATA Convention on Mercury 2013 – ANNEX A Part II: Products subject to Article 4, paragraph 3.
The aim is to reduce mercury pollution over the next few decades with targeted activities. The Convention prohibited a number of mercury-containing products, including vaccines containing mercury, thermometers, a variety of light bulbs, blood pressure devices and dental fillings using mercury amalgam. By 2020, their production and trade will be prohibited.
However, dental amalgam is the only mercury-added product that is subject to a phase-down, whereas all products will be banned or phased out. Countries such as Norway had previously undertaken significant national debate in the 1980s and 1990s and began phasing out dental amalgam in 1991, mainly due to environmental concerns. From 2008 onwards, a ban on the import, export and use of most mercury-based products came into place in Norway. However, dental offices in Norway may apply for exemptions to use amalgam on a case-by-case basis. Therefore, dental professionals living in countries that have ratified the Convention (of which UK is one) will need to amend their practice accordingly, which is likely to affect the global dental profession and public. This has resulted in a spectrum of clinical opinion on the use of dental amalgam, with views being expressed in the dental literature regarding the use of mercury-free direct restorative materials, which are perhaps not fully representative of the wider dental community, especially that of the general dental practitioner.3,4
Dental amalgam and its current alternatives
Amalgam is a cost-effective and clinical proven restorative material, the use of which has been widespread in the UK for over a century. Amalgam contains silver (40–70%), tin (12–30%), copper (12–30%), zinc (1%) and 44–48% mercury by weight.5 The process of mixing amalgam has changed significantly over the years, as has the handling and disposal within a dental surgery. It is advocated that amalgam is placed under rubber dam with high volume suction, within a room with good ventilation. The removal of amalgam should also be carried out under rubber dam with high-speed suction, water spray and sectioning and scooping of the fragments of the restoration.
The principal alternatives to dental amalgam for restoration of posterior teeth today are resin composite and glass ionomer. The latter, in a review of the literature, has been shown to perform suboptimally under certain conditions,6 although results of a recent clinical evaluation in Turkey indicate 100% survival of reinforced glass ionomer restorations at four years.7 Recent work on the thermocuring of glass ionomer restorations indicates that this substantially improves the early physical properties of these materials8 and appears to hold promise for the future development of these materials in load-bearing situations. The use of resin composite restorations in posterior teeth has been the subject of a number of extensive clinical evaluations,9,10,11 with positive findings, and two recently published systematic reviews, also publishing positive findings, by Opdam and colleagues,12 and by Astvaldsdottir et al,13 who concluded ‘that the overall survival proportions of posterior resin composite restorations is high’, reporting that the overall failure incidence rate for all reasons of failure was 1.55 restorations per 100 restoration years. Major reasons for failure were secondary caries and restoration fracture.
However, there are continuing concerns amongst dental professionals regarding the management of large cavities in posterior teeth with direct restorations, which suggests that there is a need for wider debate amongst the UK dental profession as to whether an effective ban of the use of amalgam may result in poorer clinical outcomes for patients. This may be especially concerning for some patients (namely those patients with special needs) for whom long clinical appointments and increasingly complex alternative treatments, such as posterior composite resin restorations or indirect restorations, are not possible.
Against this background, members of the British Society of Prosthodontics expressed concern regarding the phase-down of dental amalgam, as it is still a clinically useful material without an ideal successor in the event that it is no longer available. Therefore, the programme of the 2015 British Society of Prosthodontics (BSSPD) Annual Conference, which was held in London, included a live interactive debate regarding the ‘Implications of the Minamata Convention on Mercury to Use of Dental Amalgam’ entitled ‘Should our patients be worried?’. The goal of the debate was two-fold. First, to gauge the views of two eminent speakers on the subject and, secondly, to ask the large group of dentists (that consisted of specialists, generalists and foundation trainees) who had listened to this debate, to input their views on the management of several clinical examples.
The audience response system (ARS)
This debate used novel audience response system technology in order to survey the audience regarding their opinions and feelings on the potential ramifications for clinical practice, education and policy of phasing-down dental amalgam in the UK. There has been increasing awareness of the use of technology-enhanced ARSs in order to enhance the quality and quantity of audience participation during higher education lectures and debates.14 Initially, this technology operated using clicker-based devices requiring dedicated battery-powered handsets distributed to the audience and collected at the end of the session. However, this could only accommodate simple yes/no, true/false or multiple-choice questions and therefore limited the uptake of this technology. Recently, the technology has become sufficiently advanced allowing the use of smartphones, tablets and laptops to respond to text or image-based responses, as well as closed or open-ended questions in real time via Powerpoint.15 This widens the potential for interaction and discussion with a potentially unlimited worldwide audience via a web URL, as well as providing beneficial qualitative information regarding the audience's responses in order to increase the interaction between speakers and their audience, whether they share the same physical location or not.
To our knowledge, this is the first time that a smartphone-based audience response system has been used during a live debate within a dental educational context. This article describes the debate and the resulting views of the audience; captured using this novel information technology enhanced learning technique.
Method: the debate
A personal device-based ARS (Polleverwhere, San Francisco, CA) was used to live poll the audience at The British Society of Prosthodontics national debate on the global phase-down in the use of dental amalgam as a direct restorative material in March 2015. The ARS was operated via PowerPoint (Microsoft Office 2010) using a free add-in (available from www.polleverywhere.com/app) and the audience was asked to use their personal device internet browsers to navigate to the website (www.pollev.com/bsspd), in order to display and interact with the question which was being simultaneously displayed via the projected PowerPoint slide. A series of image-based, closed- and open-ended questions were displayed and the audience was invited to respond via their personal devices.
Two of the authors (PB and RA) developed the questions regarding amalgam for this debate. Using the PollEv and PowerPoint integration, the questions were then entered into the slides of the two main presenters representing the two sides of the debate (PT spoke in favour of the continued use of amalgam and TB spoke in favour of the complete phase-down of amalgam). The two speakers had a two-week window prior to the event to provide their responses to the questions. Therefore, once the audience had been live-polled, the speakers' positions could be revealed and the chairman (PB) could challenge the speakers to defend their statements in light of the audience responses.
Before the debate commenced the audience was asked to access, via their browsers, a unique PollEv URL, which displayed a waiting screen until the first poll was displayed. During the live debate, following the opening statements by the two main speakers, the chairman ran the PowerPoint with the PollEv Add-In installed and the pre-selected polls embedded within to enable a seamless experience.
As a result, the PowerPoint ran as normal and the polls were automatically opened and instantly ‘pushed’ to the audience's personal devices whilst also simultaneously displaying the polls using the lecture theatre projector in the normal way. The respondents' answers were then displayed in real-time on the projected PowerPoint screen. Participants were allowed to send in their answers as long as the chairman kept the poll open. The responses were tallied and displayed as a horizontal bar chart, with a total count for the multiple-choice questions and as a word cloud for the free text responses. For the free text responses, two of the authors present (RA and JT) acted as moderators to remove any inappropriate responses prior to display of the results of each poll.
The debate
The chairman ‘flipped’ a coin and TB chose to speak first in support of the phasing-down of amalgam. He began by summarizing the history of amalgam and citing the evidence suggesting that amalgam restorations release small amounts of mercury, below the threshold levels considered dangerous for occupational exposure for patients. The use of amalgam has steadily decreased in the United States and the United Kingdom, from 86% in 2002 to 59% in 2008.16 The alternatives to amalgam were presented. Myths associated with composite restorations were challenged. It was stated that polymerization shrinkage of the restoration would be reduced to 1% by the use of, for example, Filtek Silorane (3M ESPE, Seefeld, Germany). Recently introduced bulk fill composites were recommended to reduce the technique sensitivity and the time required to place and polish the restorations, with most recent materials not requiring a conventional composite top layer. Supermat (Kerr-Hawe) matrix bands and sectional matrices were advocated to achieve a good contact point, a problem noted when using resin composites in Class II cavities prior to the introduction of dedicated composite matrices. Proximal box elevation using resin modified glass ionomer cements were endorsed for deep proximal boxes with limited or no enamel for bonding, with the caveat that the patient must be warned that this is a compromised situation. It was suggested that new graduates in some schools have received more training and experience in the placement of composite restorations than in placing amalgam restorations. At five years the annual failure rate of posterior composite restorations has been cited at 1.8% and that at 10 years as 2.4%.11 Other studies have suggested the overall failure of posterior composite restorations to be 2% per annum.10.12
The second speaker (PT) spoke against the phasing-down of amalgam, citing evidence that there was no significant risk to neuropsychological function from amalgam restorations in children. Numerous governments (United States, Canada, Australia and a number of countries in Europe) had issued statements to the effect of maintaining amalgam as a dental restorative material as the current evidence suggests that it is a safe and effective material. The Norwegian Board of Health stressed that its decision to phase out amalgam was not related to safety of dental amalgam but due to long-term goals in reducing the release of mercury into the environment. Both Norway and Sweden have stated that they will issue exemptions to the ban on amalgam on a case-by-case basis. Potential health risks associated with composite monomers were discussed.17 Composite restorations were said to have a significantly higher risk of failure than amalgam (RR 1.89, 95% CI 1.52–2.35), with an increased risk of secondary caries under composite restorations.18 Composite restorations were said to lead to 1.9 times more need for endodontic intervention than amalgam.19 Removal of composite restorations was said to produce significantly greater increases in cavity volume compared to the removal of amalgam.20 The micro-tensile bond strength of adhesive/resin-based composite bonded to the gingival wall was shown to be significantly weaker than the bond to axial walls, with in vivo bond strengths significantly weaker than in vitro conditions.21 The degradation of the resin-dentine bonds and destruction of the composite itself with time was highlighted.22 The economic impact for banning dental amalgam was considered to lead to a significant short- and long-term increase in expenditure on dental care, leading to a decrease in the utilization of dental treatment and an increase in untreated disease in the United States23 and a significant potential increase in cost to the National Health Service in the UK.
The Interactive Clinical Case Discussion included four cases and a series of open- and closed-ended questions. Table 1 shows the clinical case photographs and the questions posed to the audience regarding the clinical management of the tooth. Table 2 shows the open-ended and closed-ended questions put to the audience regarding the potential ramifications to the phase-down of dental amalgam.
Case 1:
How would you manage the pulp in this case? You have chosen to restore with composite - which would be your preferred cavity modification prior to applying the dentine-bonding agent? Which type of dentine-bonding agent would you use?What type of composite would you use?
Case 2:
Which matrix band system would you use to restore the proximal cavity?
Case 3:
What would be your preferred material choice for restoring these teeth?
Case 4:
What would be your preferred material choice for restoring this tooth? What would be your tooth-coloured restoration of choice for this tooth? If using amalgam restoration, what design would you choose?
1. Assuming that there will phase-down of dental amalgam use, should we be fighting for continued use of dental amalgam in selected clinical situations?
2. If amalgam is no longer allowed to be used, do you think that more indirect restorations will be prescribed for broken down posterior teeth?
3. Those who said yes - please state clinical situations for which amalgam should continue to be used
4. For those who answered no - state clinical situations when you consider composite resin contra-indicated in posterior teeth
5. Having listened to the debate, do you believe that the clinical performance of amalgam and composite are equal for approximal posterior restorations?
6. Do you believe that amalgam should still be taught in UK dental schools?
7. Do London DFs feel that they were adequately trained to use amalgam at dental school?
8. Having worked for 6 months as a DF trainee, do you think composite is the solution for all clinical situations when restoring posterior teeth?
9. Those who have said no - state examples of clinical situations for which composite has not been the solution
10. Do you believe that the view of the UK GDP is being appropriately heard in this debate?
11. Those that have said no - how can it be heard better?
The main screen allowed the audience to view, in real time, the results of ‘yes’/‘no’ and free text votes. The technology allowed comparison of the views of the two specialist speakers and the audience. It was possible to ask specific questions of the Dental Foundation trainees enrolled with Health Education London (London Dental Education and Training) as many would have had limited undergraduate experience with dental amalgam.
Poll results
The total sample size was 323 and the audience was composed of 134 Dental Foundation Trainees (Postgraduate Dentists who qualified less than 12 months prior) and 189 dentists who had a special interest in Prosthodontics. An average response rate of 48% was received.
Case 1
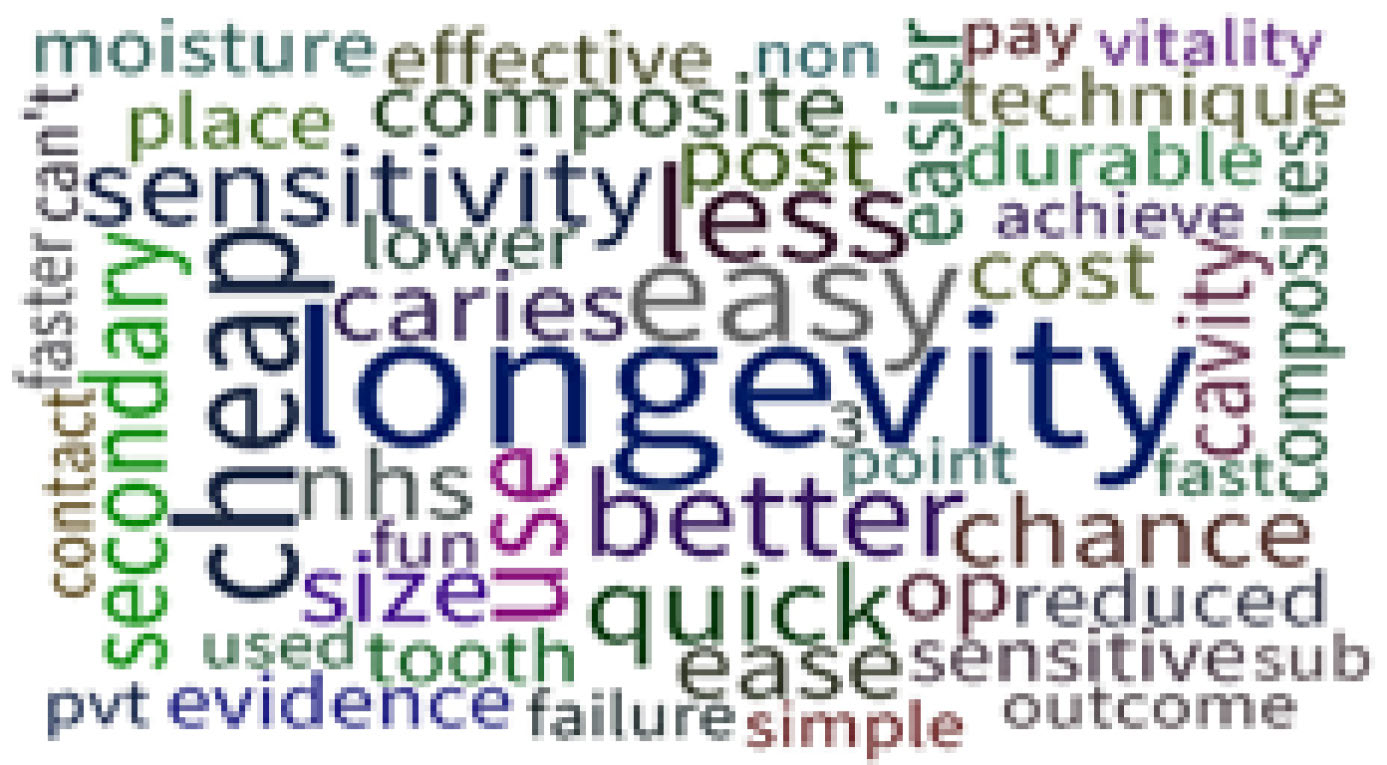
The majority of respondents (34%) would indirectly pulp cap using a dentine-bonding agent. TB stated that he would use a dentine-bonding agent to seal the dentinal tubules and an incremental composite. PT would use direct amalgam and avoid a dentine-bonding agent as bonding agents can hydrolyse leaving a space between the restoration and the tooth. Fifty six percent of respondents would use a total etch technique using 37% orthophosphoric acid prior to the bonding agent, as would both speakers. Seventy percent of respondents preferred a two-bottle or two-stage ‘total etch’ or ‘total rinse’ system. TB stated that he would use a new Universal Bonding System and PT stated that he would use a three-step system every time. The majority (30%) of respondents stated that they would use a microhybrid composite and 20% would restore this cavity with amalgam. The main reason given for restoring with amalgam was longevity (Figure 2).
Figure 2. Audience response results to the question ‘Why would you choose to restore Case 1 with amalgam?’ (n = 93).
Case 2
Forty nine percent of respondents would use a sectional matrix with ring retainer for restoring the proximal cavity, as would TB. PT stated that he would use a Siqveland (Dentsply, Addlestone, UK) or Automatrix (Dentsply, Addlestone, UK), which were the second and third choices of respondents.
Case 3
The majority of respondents would restore these teeth with direct composite (61%), as would TB. Twenty one percent, and PT, stated that they would restore using amalgam.
Case 4
Forty percent of respondents would restore this tooth with an indirect metal restoration, 18% stated that they would restore with amalgam, 15% would restore with indirect composite. Twelve percent would restore the tooth with ceramic and 12% with direct composite.
TB stated that he would use direct resin composite and PT stated that he would use amalgam. If using a tooth-coloured restoration, 27% percent (the majority) of respondents stated that they would restore this tooth with an indirect resin composite onlay. TB stated that he would use direct composite and PT an amalgam core and a milled partial coverage crown. If using amalgam, 50% would place an amalgam core restoration with a view to placing a cuspal coverage indirect restoration.
Having listened to the debate, 66.7% of the participating audience stated that amalgam and composite were not equal in their clinical performance as approximal posterior restorations and that amalgam performs better than composite.
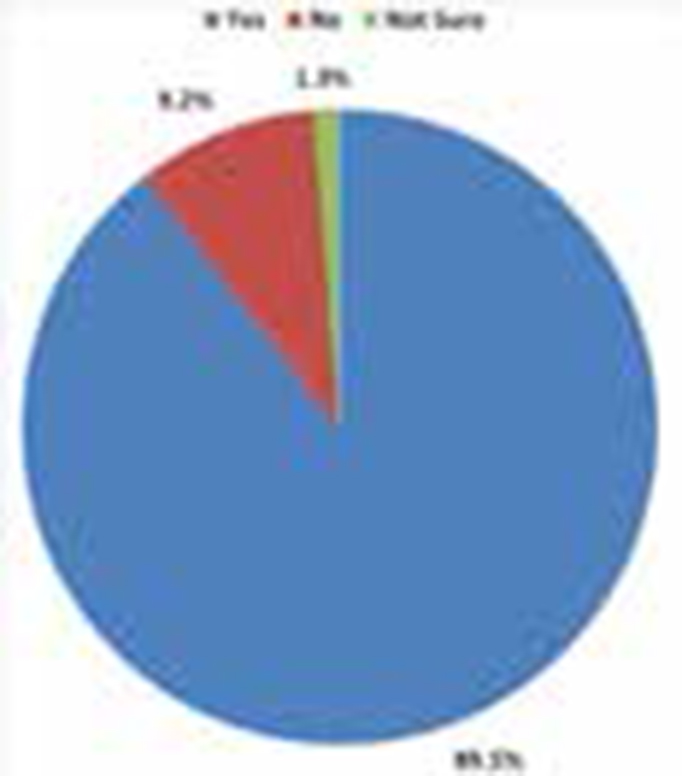
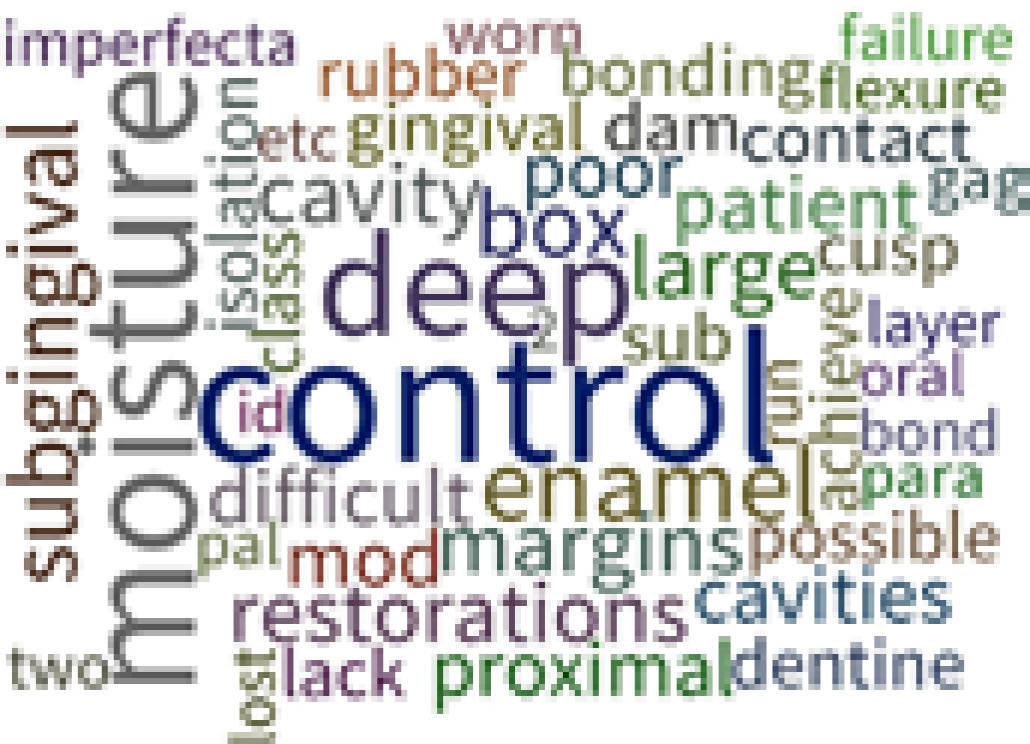
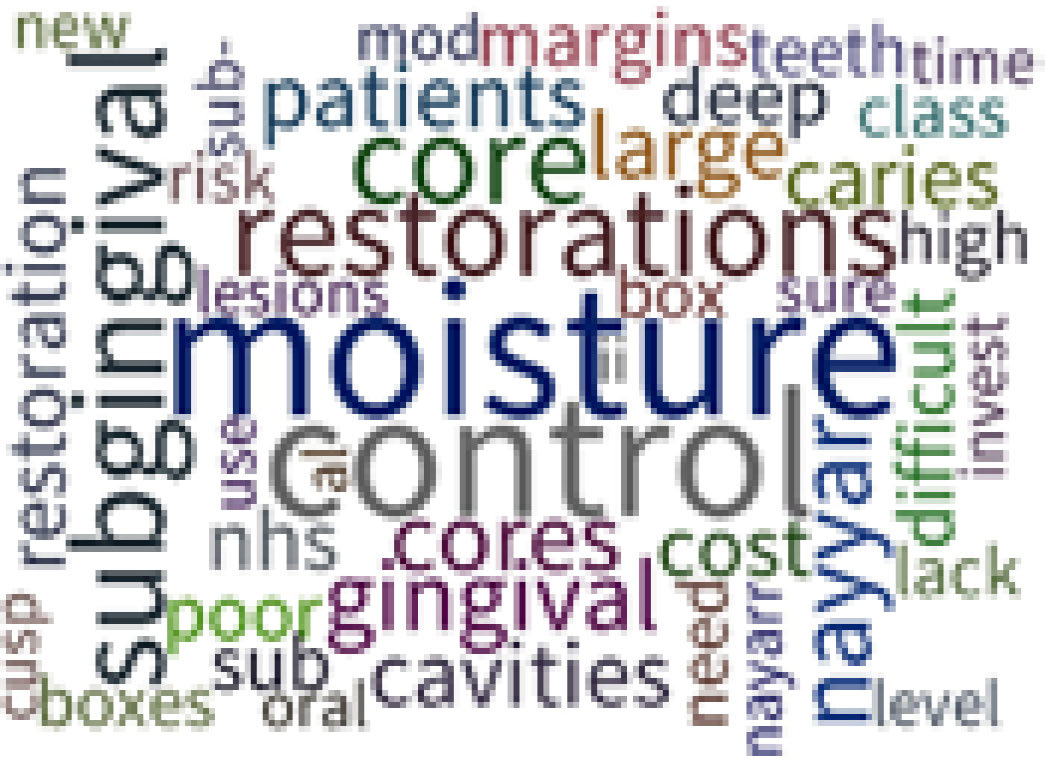
When asked if we should be fighting for the continued use of dental amalgams in selected clinical situations, 89.5% of the participating audience stated that we should (Figure 3). The free text responses stated moisture control as the main reason for not using composite and for using amalgam in posterior teeth (Figure 4 and Figure 5). The two questions, which effectively asked the same open-ended question in two different ways, resulted in two word clouds with very similar appearances, providing internal validity to this question.
Figure 3. Audience response results to the question ‘Assuming that there will be a phase-down of dental amalgam use, should we be fighting for continued use of dental amalgam in selected clinical situations?’ (n = 153).Figure 4. Audience response results to the question ‘State clinical situations for which you consider composite resin contra-indicated for posterior teeth?’ (n = 63).Figure 5. Audience response results to the question ‘State clinical situations for which amalgam should continue to be used?’ (n = 106).
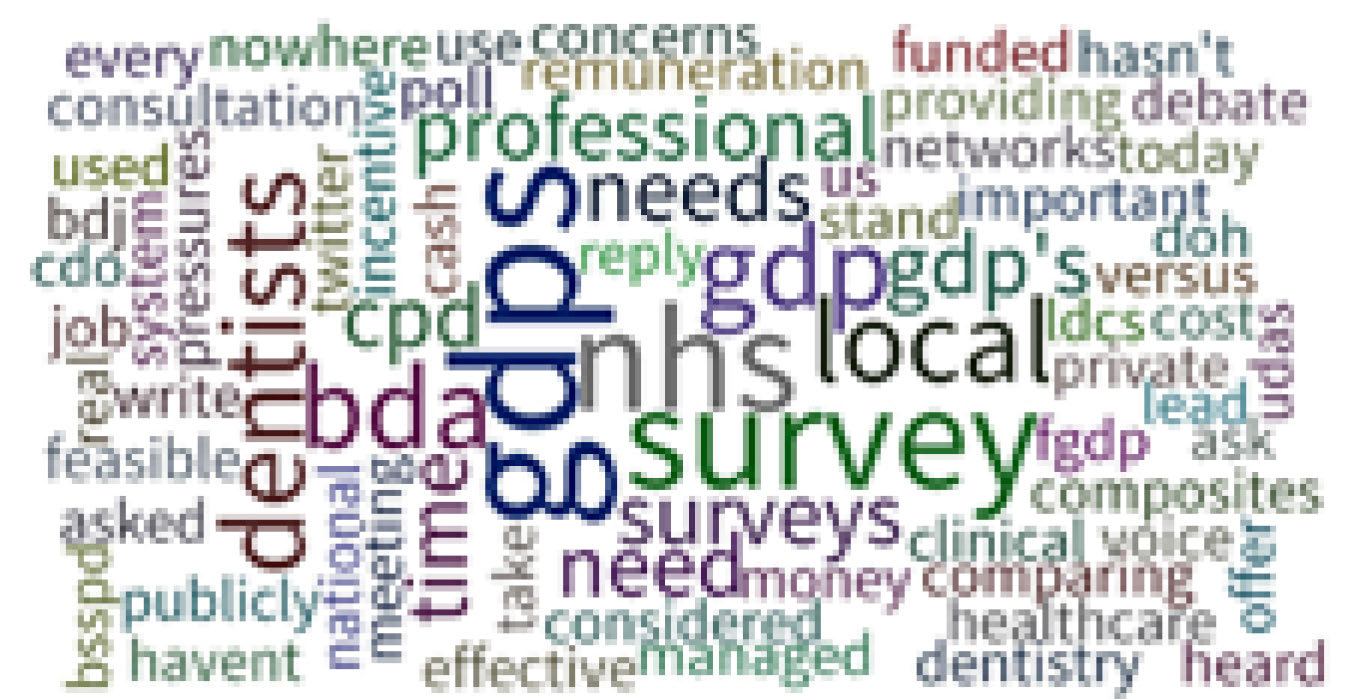
If amalgam were no longer available, 80.5% of the participating audience thought that more indirect restorations would be prescribed for broken-down posterior teeth. Fifty-three percent said that they believed more teeth would be extracted if amalgam was unavailable and 93.8% said that they believed that amalgam should still be taught in dental schools in the UK. When asked if the voice of the general dental practitioner is being appropriately heard in this debate, only a third felt that it was being heard (Figure 6).
Figure 6. Audience response results to the question ‘How can the voice of the GDP be heard in the amalgam debate?’ (n = 99).
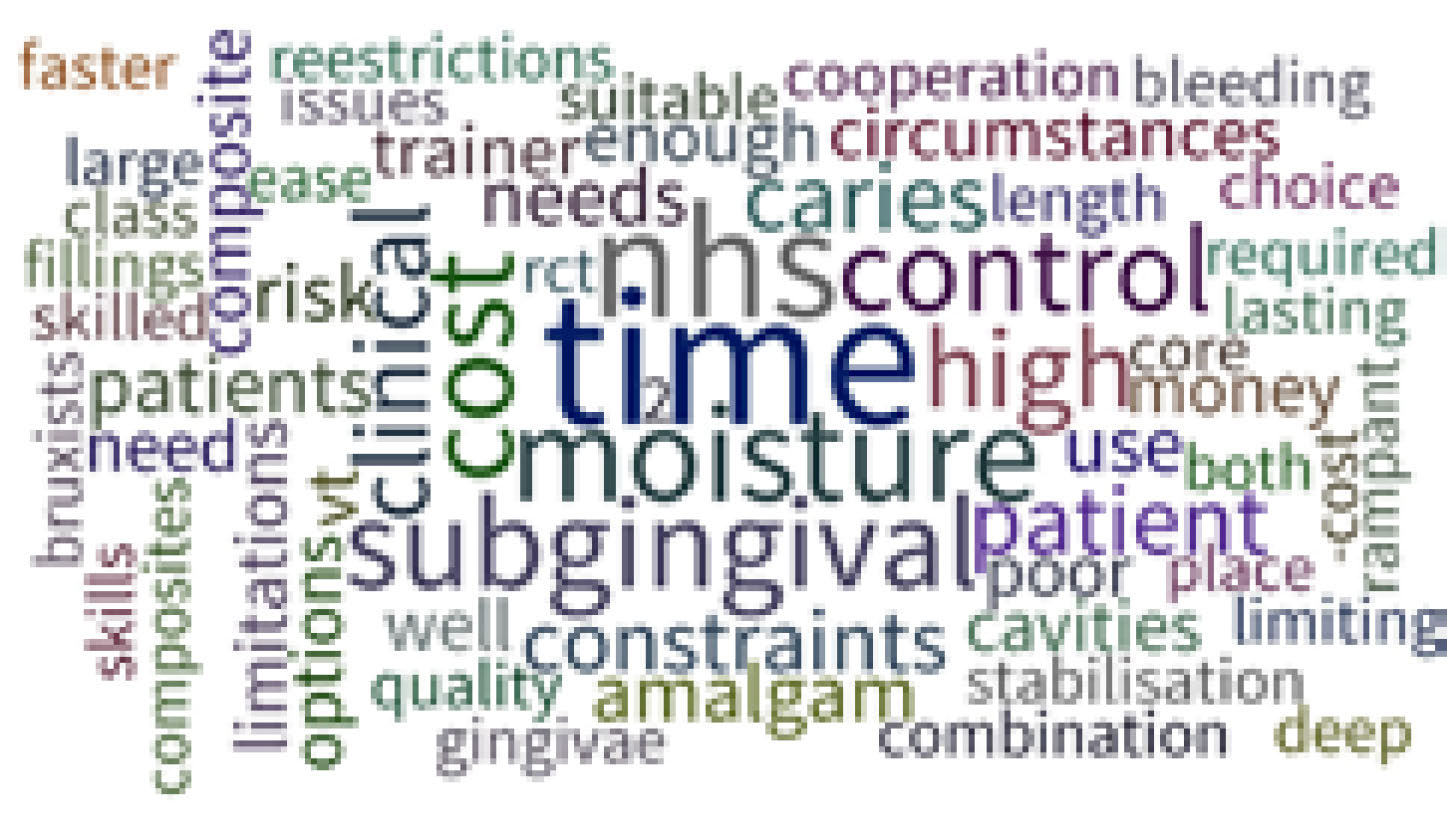
When the Dental Foundation trainees were asked if they felt that they were adequately trained to use amalgam at dental school, 34.7% stated that they were not adequately trained. Having worked as a DF trainee for 6 months, 93.9% stated that they did not think that composite was the solution for all clinical situations when restoring posterior teeth; the main reason given being ‘time’, followed by ‘NHS’ and ‘subgingival’ (Figure 7).
Figure 7. Audience response results to the question ‘State examples of clinical situations for which composite has not been the solution?’ (n = 70)
Discussion
The results of this poll make interesting reading and, while not a representative sample of all UK dentists, may be considered to give a snapshot of dentists whose main occupation is the restoration of teeth. As indicated by the responses to Cases 1, 2 and 3, a majority of the respondents were content to use resin composite as the restorative material, these cases being cavities of moderate proportions, although the interproximal box in Case 3 was wide. It is also of interest to note a respondent's preference for a two-stage etch and rinse system in Case 1. It is also interesting to note the popularity of the relatively recently introduced bulk fill composites, which were chosen by 22% of the respondents. Twenty per cent of respondents decided that they would restore the cavity with amalgam, the principal reason for this (Figure 2) being longevity (although, as stated by TB, the literature no longer supports amalgam being of greater longevity,9 despite respondents' opinions not appearing to support this) along with ease-of-use and cost, which favour amalgam in comparison to resin composite, with clinician time costs being the principal factor in any restoration. It was for more challenging clinical situations, such as that in Case 4, that the respondents would generally not choose resin composite, in this case an indirect restoration being favoured. This is reflected by the response which indicated that 89% of respondents considered that amalgam should continue to be used in selected clinical situations. This is further reflected by the response to the statement that ‘if amalgam were no longer available’, more indirect restorations would be prescribed for broken down posterior teeth and an increased number of teeth would be extracted. Perhaps the respondents perceived a concept similar to the situation in Norway, where amalgam is effectively banned,24 but in which dentists may apply to use amalgam for certain clinical situations.
This is the first publication to present results from the use of smartphoneand tablet-based audience response system (ARS) technology to live-survey the views of a large dental audience. This technology provided an ideal method for collecting quantitative and qualitative information regarding a sensitive and impassioned topic such as the continued use of dental amalgam.
The use of audience response systems operating using personal devices can be an inexpensive and environmentally friendly alternative to clicker-based ARS and has the added advantage that the communication medium is familiar to nearly all audience members, thus allowing live surveying of a potentially unlimited audience size. Although those without an internet-enabled device or with difficulty using their device are not able to participate, in this present study only one audience member reported that they felt excluded by the process as they did not have a smartphone. As the market presence of smartphones, tablets and laptops widens to almost universal adoption, such issues will become ever rarer due to increasing familiarity with their features and usages.
The results of this survey appear to indicate that there is still not an actual replacement/substitute for amalgam. Indeed, it may be surmised that, if the ideal amalgam replacement had been developed, it would have taken over the market and amalgam would no longer be used. This ideal material might have the following properties:
Be non-toxic;
Be self adhesive, providing an ideal seal as well as obviating the need for producing or removing undercuts;
Set fully in its entirety over a clinically acceptable time span;
Have good physical properties once set such as being dimensionally stable and wear resistant;
Be quick and easy to place and usable in all shapes and sizes of cavities;
Be aesthetically acceptable;
Perform well even when planed during suboptimal conditions.
While resin composite fulfils some of these properties, with some of its variants being self-adhesive (for example, self-adhesive resin luting materials), some having 5 mm depth of cure (bulk fill resin composites), some having low shrinkage stress (for example, Filtek Silorane25 and Filtek Bulk Fill Restorative [Palin WM, unpublished data]) and all having suitable physical properties, there remains concern in respect of the increased time required for placement as compared with amalgam and technique sensitivity. If and when these concerns are addressed and an ideal material becomes available (as listed above), the phase-down of amalgam will not be an issue. The authors, and indeed all the respondents of this BSSPD survey, keenly await the development of this material. Moreover, given industry awareness of the vast global demand for a mercury-free alternative to dental amalgam, all major dental materials manufacturers are investing significant resources and revenue to develop exactly such a solution.
Currently, however, over 90% of respondents stated that they believed the use of dental amalgam should continue to be taught in UK dental schools, with only 62% of the younger dentists in the audience saying that they felt adequately trained to use amalgam at undergraduate dental school. On the other hand, it may be salutary to note that, when the phase-down of amalgam takes effect, many senior practitioners may not necessarily have the skills to provide posterior composite restorations to an optimal standard. In the present study, the responding dentists cited time as the most important limiting factor for use of composite in general dental practice (Figure 7) and, moreover, subgingival margins were mentioned as the most important factor favouring use of amalgam for all posterior restorations (Figure 5).
Altogether, the results of this survey suggest significant workforce impacts to the phase-down, for example, when practitioners undergo a new learning curve there can be variability in the speed at which new techniques are adopted. The responsibility for training the workforce appropriately will fall to Health Education England, National Societies and the individual practitioner, with a financial impact to the NHS. This present paper therefore clearly highlights the need for strong leadership amongst the dental profession, in terms of raising awareness of the potential issues of the phase-down of amalgam. The results from this study suggest that only a third of respondents considered that the general dental practitioner's (GDP's) voice was being heard in this debate and there was a concerning lack of consensus as to how the voice of the GDP can best be heard as the debate continues (Figure 6). Therefore, there remains a clear and present need to engage and involve as broad a spectrum of the dental profession as possible. Professional societies and representative bodies should bear this in mind as the global picture increasingly trends towards the complete phase-down of dental amalgam use.
Conclusions
This debate has confirmed that dental amalgam is still considered a useful and important material for the restoration of posterior teeth. Over 90% of those that voted wished to see the choice of dental amalgam continue into the future within the UK for certain indications. The majority of conference attendees participating in the amalgam debate also felt that more posterior teeth will be extracted if amalgam is no longer available.