Lee AHC, Neelakantan P, Dummer PMH, Zhang C. Cemental tear: literature review, proposed classification and recommendations for treatment. Int Endod J. 2021; 54:2044-2073 https://doi.org/10.1111/iej.13611
Jepsen S, Caton JG, Albandar JM Periodontal manifestations of systemic diseases and developmental and acquired conditions: consensus report of workgroup 3 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Clin Periodontol. 2018; 45 https://doi.org/10.1111/jcpe.12951
Jeng PY, Luzi AL, Pitarch RM Cemental tear: to know what we have neglected in dental practice. J Formos Med Assoc. 2018; 117:261-267 https://doi.org/10.1016/j.jfma.2017.09.001
Lin HJ, Chang SH, Chang MC Clinical fracture site, morphologic and histopathologic characteristics of cemental tear: role in endodontic lesions. J Endod. 2012; 38:1058-1062 https://doi.org/10.1016/j.joen.2012.04.011
Marquam BJ. Atypical localized deep pocket due to a cemental tear: case report. J Contemp Dent Pract. 2003; 4:52-64
Chou J, Rawal YB, O'Neil JR, Tatakis DN. Cementodentinal tear: a case report with 7-year follow-up. J Periodontol. 2004; 75:1708-7013 https://doi.org/10.1902/jop.2004.75.12.1708
Ishikawa I, Oda S, Hayashi J, Arakawa S. Cervical cemental tears in older patients with adult periodontitis. Case reports. J Periodontol. 1996; 67:15-20 https://doi.org/10.1902/jop.1996.67.1.15
Nagata M, Kanie T, Shima K. Cemental tear in an autotransplanted tooth that had been functioning for 15 years. Clin Adv Periodontics. 2016; 6:111-117 https://doi.org/10.1902/cap.2015.150047
Keskin C, Güler DH. A retrospective study of the prevalence of cemental tear in a sample of the adult population Applied Ondokuz Mayis University Faculty of Dentistry. Meandros Medical and Dental Journal. 2017; 18
Özkan G, Özkan HD. Evaluation of cemental tear frequency using cone-beam computed tomography: a retrospective study. Meandros Medical and Dental Journal. 2020; 21
Yamamoto T, Hasegawa T, Yamamoto T Histology of human cementum: its structure, function, and development. Jpn Dent Sci Rev. 2016; 52:63-74 https://doi.org/10.1016/j.jdsr.2016.04.002
Ong TK, Harun N, Lim TW. Cemental tear on maxillary anterior incisors: a description of clinical, radiographic, and histopathological features of two clinical cases. Eur Endod J. 2019; 4:90-95 https://doi.org/10.14744/eej.2019.13007
Pedercini A, Weitz DF, Heyse JD Cemental tear: an overlooked finding associated with rapid periodontal destruction. A case series. Aust Dent J. 2021; 66:S82-S87 https://doi.org/10.1111/adj.12844
Xie C, Wang L, Yang P, Ge S. Cemental Tears: a report of four cases and literature review. Oral Health Prev Dent. 2017; 15:337-345 https://doi.org/10.3290/j.ohpd.a38745
Haney JM, Leknes KN, Lie T Cemental tear related to rapid periodontal breakdown: a case report. J Periodontol. 1992; 63:220-224 https://doi.org/10.1902/jop.1992.63.3.220
Harrel SK, Wright JM. Treatment of periodontal destruction associated with a cemental tear using minimally invasive surgery. J Periodontol. 2000; 71:1761-176 https://doi.org/10.1902/jop.2000.71.11.1761
Tamse A. Vertical root fractures in endodontically treated teeth: diagnostic signs and clinical management. Endod Topics. 2006; 13:84-94
Liao WC, Tsai YL, Wang CY Clinical and radiographic characteristics of vertical root fractures in endodontically and nonendodontically treated teeth. J Endod. 2017; 43:687-693 https://doi.org/10.1016/j.joen.2016.12.009
Fuss Z, Lustig J, Katz A, Tamse A. An evaluation of endodontically treated vertical root fractured teeth: impact of operative procedures. J Endod. 2001; 27:46-48 https://doi.org/10.1097/00004770-200101000-00017
Stewart GG. The detection and treatment of vertical root fractures. J Endod. 1988; 14:47-53
Endodontics: colleagues for excellence-Cracking the cracked tooth code. 1997;
Rivera EM, Walton RE. Cracking the cracked tooth code: detection and treatment of various longitudinal tooth fractures. Am Assoc Endodontists Colleagues for Excellence News Lett. 2008; 2:1-9
Papapanou PN, Sanz M, Buduneli N Periodontitis: consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J Periodontol. 2018; 89:S173-S182 https://doi.org/10.1002/JPER.17-0721
Herrera D, Retamal-Valdes B, Alonso B, Feres M. Acute periodontal lesions (periodontal abscesses and necrotizing periodontal diseases) and endo-periodontal lesions. J Periodontol. 2018; 89:S85-S102 https://doi.org/10.1002/JPER.16-0642
Park Y-S, Lee J-H, Jeong S-N. Treatment of the cemental tear. Oral Biol Res. 2018; 42:248-253
Damasceno LS, Dutra WO, Melgaço EG Cemental tear: a case report with nonsurgical periodontal therapy. Revista Odonto Ciência. 2012; 27:74-77
Tibbetts LS, Shanelec D. Periodontal microsurgery. Dent Clin North Am. 1998; 42:339-359
Caton JG, Zander HA. The attachment between tooth and gingival tissues after periodic root planing and soft tissue curettage. J Periodontol. 1979; 50:462-426 https://doi.org/10.1902/jop.1979.50.9.462
Schmidlin PR. Regenerative treatment of a cemental tear using enamel matrix derivatives: a ten-year follow-up. Open Dent J. 2012; 6:148-152 https://doi.org/10.2174/1874210601206010148
Rojas MA, Marini L, Pilloni A, Sahrmann P. Early wound healing outcomes after regenerative periodontal surgery with enamel matrix derivatives or guided tissue regeneration: a systematic review. BMC Oral Health. 2019; 19 https://doi.org/10.1186/s12903-019-0766-9
Rosenberg ES, Torosian J. Esthetics and periodontics. Chapter 14, 3rd edn. In: Aschheim KW (ed). St Louis, MO, USA: Mosby; 2015
Pilloni A, Nardo F, Rojas MA. Surgical treatment of a cemental tear-associated bony defect using hyaluronic acid and a resorbable collagen membrane: a 2-year follow-up. Clin Adv Periodontics. 2019; 9:64-69 https://doi.org/10.1002/cap.10053
Hsin Y, Wu C, Lin S, Chen C. Treatment of cemental tear using intentional replantation. J Endod Sci. 2011; 2:49-54
Rouhani A, Javidi B, Habibi M, Jafarzadeh H. Intentional replantation: a procedure as a last resort. J Contemp Dent Pract. 2011; 12:486-492 https://doi.org/10.5005/jp-journals-10024-1081
Tai TF, Chiang CP, Lin CP Persistent endodontic lesion due to complex cementodentinal tears in a maxillary central incisor – a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103:e55-60 https://doi.org/10.1016/j.tripleo.2006.12.011
Cemental tears: challenges in the diagnosis and management of an unusual finding associated with rapid localized periodontal and peri-radicular bone loss
Cemental tears: challenges in the diagnosis and management of an unusual finding associated with rapid localized periodontal and peri-radicular bone loss Siew Leng Tan Kajal B Patel Julie K Kilgariff Dental Update 2025 49:11, 895-903.
Authors
Siew LengTan
BDS, AKC, MJDF RCSEng, PGCert MedEd
Orthodontic Registrar, Eastman Dental Hospital, University College London Hospitals NHS Foundation Trust
A cemental tear is a rare form of root surface fracture whereby a fragment of cementum partially or completely detaches from the root surface at the cemento-dentinal junction or within the body of cementum. Tears are most prevalent in incisors and lead to the breakdown of periodontal issues. Owing to challenges involved in diagnosis, cemental tears may be misdiagnosed because associated clinical and radiographic features closely resemble those seen in vertical root fractures, periodontal abscesses and endo-periodontal lesions. If incorrectly diagnosed, inappropriate and delayed management may result in treatment failure and tooth loss.
CPD/Clinical Relevance: Correct diagnosis and timely management of cemental tears can prevent further destruction of periodontal tissues, improve treatment outcomes and increase tooth survival.
Article
A cemental tear is a fragment of cementum partially or completely detached from the root surface at the cemento-dentinal junction or within the body of cementum along the incremental lines.1,2 Although rare, cemental tears can also involve part of the root dentine adjacent to the cementum.2 If the tear is not detected and removed in a timely manner, severe bone loss in the location of the tear can occur. This is because it is a localized tooth-related factor predisposing to plaque-induced gingival diseases or periodontitis.3 Correct diagnosis is paramount to avoid treatment delays, inappropriate treatment, treatment failure and potentially tooth loss.
However, cemental tears are rare and, therefore, clinicians may be unfamiliar with them. Misdiagnosis and mistreatment can occur; lesions being erroneously thought associated primarily with periodontal or endodontic disease aetiologies, such as vertical root fractures.4
Vertical root fractures (VRF) are challenging to diagnose because of the varied presentations.5 A tooth diagnosed with a VRF often requires extraction. However, a root-treated tooth with periodontal breakdown may have similar clinical and radiographic features to a VRF, but be amenable to treatment.6 It is therefore important that clinicians can distinguish between a tooth with a hopeless condition, such as a VRF, and conditions that are treatable. This article discusses a lesser-known condition, cemental tear, the presentation of which can resemble VRF, but in contrast, cemental tears can often be successfully treated and the tooth retained, if the tear is identified early. The prognosis of cemental tears is therefore more favourable than VRF.2 In addition, similar clinical and radiographic presentations may be seen with periodontal abscesses and endo-periodontal lesions.1 This article aims to assist clinicians in reaching the correct diagnosis when faced with four conditions of different aetiology and prognosis, but similar presentations: cemental tears, VRF, periodontal abscesses and endo-periodontal lesions. Correct diagnosis dictates the most appropriate treatment options, including referral to specialist services, if indicated.
Tear location and features
Single or multiple tears can occur at any point on the root; however, the mid-third is the most frequent site reported, with the majority occurring on proximal surfaces (79.6%) (Figure 1).2,7 Cemental tears located in the apical third may be more difficult to identify and therefore less frequently reported in the literature. Furthermore, torn fragments present on the buccal or lingual aspects of teeth are not easily identifiable on peri-apical radiographs, resulting in tears being unidentified and missed by clinicians.2
Figure 1. Diagram showing potential locations of cemental tears. The majority are identified as occurring in the mid-third of the root length.
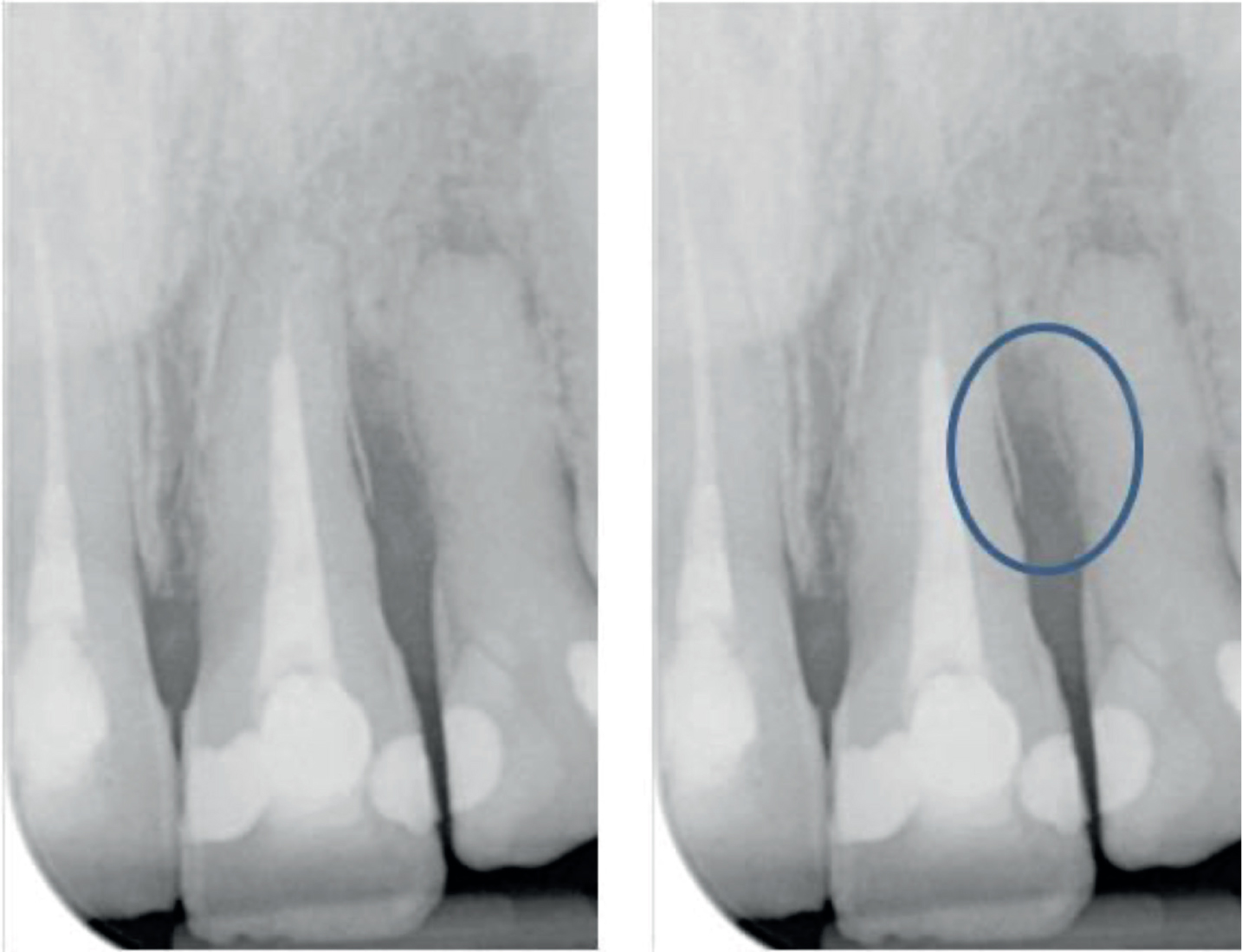
The cemental fragment can be totally detached from the root surface or remain partially attached (Figure 2).8 These thin, radiopaque, sheet/piece-shaped4 or ledge-like8 fragments projecting from the root surface are usually located on one aspect of the root surface, but can be U-shaped, extending around more of the root circumference.1 Extensive U-shaped defects are more often associated with the apical third.4,7,9
Figure 2. A partially attached cemental tear in the mid-third of UL1. Severe infrabony alveolar bone loss is seen. This tooth was previously diagnosed with an endo-periodontal lesion and treated as such, but no resolution in symptoms occurred.
Prevalence and predisposing factors
The prevalence of cemental tears
In teeth identified as having cemental tears:
The highest prevalence is reported in incisors (in 74.1% of cases),2,7,10 possibly caused by protrusive and lateral occlusal forces on single-rooted teeth;7
Less commonly affected are second premolars,11 molars,12,13 and in one case, an autotransplanted tooth.14
General prevalence in population
A retrospective study investigating cemental tear prevalence via peri-apical radiographs of 4629 permanent teeth, identified cemental tear prevalence in the sample of 1461 patients as 0.89%.15 A different study reported the prevalence of tears as 1.9% based on evaluation of 813 cone beam computed tomography (CBCT) images.16 The use of CBCT three-dimensional images is likely to provide a more accurate estimation of tear prevalence because tears present on the buccal or lingual root surfaces are more likely to be detected. The prevalence of cemental tears may be lower than VRF, which has a reported prevalence of 10.9% in 147 extracted root-treated teeth examined using a magnifying glass.17 However, it is noteworthy that this study examined only root-filled teeth, potentially more likely to develop VRF, and therefore a prevalence of 10.9% may be an overestimation of that seen in the general population, including root-filled and non-root-filled teeth.
Predisposing factors
There are various predisposing factors for cemental tears:
Age: patients over the age of 60 years (in 72.3% of cases);2,4,7
Tooth type: majority of reported cases are of incisors;2,7,10,12
Tooth wear: moderate to severe attrition.2,7Attrition has been identified as a predisposing factor in two studies;2,7 however, no index appears to have been used to quantify the extent of attrition at which cemental tears are more likely to occur;
Occlusal factors: occlusal trauma4 describes injury causing tissue changes within the periodontal ligament, supporting alveolar bone and cementum owing to occlusal forces.18 The association of tooth wear and occlusal trauma as predisposing factors suggests tears may occur from excessive loading or traumatic forces from parafunctional habits, such as bruxism.4 In recent years, cemental tears have been identified as a clinical and radiographic indicator of occlusal trauma, along with fremitus, progressive tooth mobility, occlusal discrepancies, wear facets, fractured tooth or teeth, etc.18
However, although investigated, no significant associations with cemental tear development have been identified as yet with:
Prior endodontic treatment and presence of post or cores;2
External and internal factors have been suggested in the development of cemental tears.1,19 External factors include repeated stress induced by occlusal trauma, resulting in a fracture line that propagates at the cemento-dentinal junction (CDJ) or within the body of cementum, causing a fragment of cementum to be partially or completely detached from the root surface at the CDJ or within the cementum.1 It has been suggested that cemental tears develop at the pressure side of the tooth subjected to occlusal trauma.18
Internal factors are associated with an intrinsic structural deficiency in cementum, such as:
Weak interconnecting connective tissue and adhesion at the CDJ between the cementum and dentine;19
Physical changes associated with thickened secondary or tertiary cementum;19,20
Iatrogenically induced structural cementum weakness from periodontal mechanical instrumentation.1,10
Clinical and radiographic findings
Generally, findings closely resemble those seen in VRF, periodontal abscesses and endo-periodontal lesions.1,7 The reported clinical (Figure 3) and radiographic (Figures 2, 4 and 5) findings associated with cemental tears are outlined in Table 1.21–23
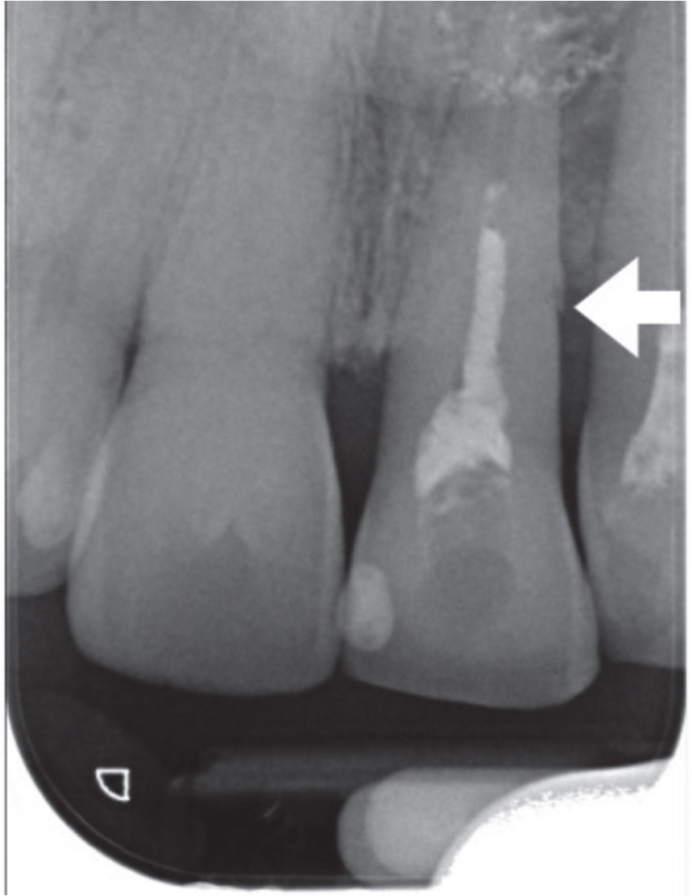
Figure 3. Clinical photographs of the cemental tear case shown in Figure 2 demonstrating (a) buccal swelling and (b, c) isolated deep periodontal pocket in the UL1 of a 39-year-old female patient with no known history of trauma. The tooth mobility at the time of presentation resulted in short-term composite splinting being used while root canal re-treatment, internal tooth whitening (b,c) taken following tooth whitening) and non-surgical periodontal therapy were carried out. The isolated deep periodontal pocket persists on UL1. GTR procedures were therefore carried out. (See also Figures 8 and 9 for photographs and radiographs of GTR procedures.)Figure 4. A 61-year-old male presented with a buccal abscess and sinus, deep mesial pocket of 10 mm and increased mobility in UR1. There was no known history of trauma. The cemental tear (arrow) is seen in the mid-third of UR1 root surface and significant bone loss mesially. Note the more subtle appearance of the cemental tear in comparison to Figure 2, and, as with the case in Figures 2 and 3, this case was initially misdiagnosed as an endodontic problem. The tooth was unresponsive to root canal treatment and the patient was referred to a specialist-led clinic.Figure 5. Cemental tear in UL1 (arrow) noted in the mid-third of root surface of a 43-year-old male presenting with dull pain from the tooth, a deep distal pocket of 5 mm and increased tooth mobility. Occlusal trauma (fremitus) of UL1 was noted in intercuspal position and during lateral excursion. Note: as with the cases in Figures 2–4, prior to referral, this case was misdiagnosed and treated as an endodontic problem.
If not already root canal treated (RCT), the pulp is likely to be vital
To prevent unnecessary endodontic treatment, it is recommended that clinicians carry out sensibility tests on teeth suspected of cemental tears to determine the pulpal status and exclude endo-periodontal lesion as a possible diagnosis.2
Periodontal and/or peri-radicular bone destruction (radiolucency)
Bone destruction is progressive if the tear is left untreated
A thin, radiopaque fracture-like fragment seen parallel to the proximal root surface
Figures 2, 4 and 5 Peri-apical radiographs taken at different angles can aid identification of cemental tears located on the mesial or distal root surfaces. However, tears can also be present on the buccal or lingual root surfaces and therefore not easily identifiable on radiographs2
CBCT
May be of more use (compared to a peri-apical radiograph) in detecting the presence and pattern of a cemental tear, but evidence is currently lacking.
Depending on the extent and site of defect, this may aid surgical planning
If a cemental tear is present and exposed to the oral microflora, via periodontal pocketing, signs and symptoms (eg acute swelling, suppuration, pain) can persist.24 The torn fragment serving as a retentive site for plaque and calculus results in rapid localized periodontal breakdown, progression of pocket and increasing mobility, in patients with or without pre-existing periodontitis.1,8,25,26 Some authors suggest that cemental tears located in the apical region result in peri-radicular inflammation caused by mechanical irritation of the torn fragments, but this, theoretically, is sterile inflammation, a form of pathogen-free inflammation caused by mechanical trauma because there is no communication to the oral environment.1 However, if there is sufficient periodontal breakdown and communication with the tear, the root canal system could become infected in these cases.1
Provisional diagnosis
As cemental tears are not commonly reported in the literature, they may be overlooked. When patients present with cases of isolated deep pockets and rapid periodontal destruction located to a single tooth, cemental tears should be considered as a potential cause, along with more common diagnoses. Provisional diagnoses will include: VRF (Figure 6), periodontal abscesses and endo-periodontal lesions (Figure 7).1,4,8,10Table 2 summarizes the key findings and treatment associated with each provisional diagnosis for teeth with isolated deep pockets.27–35 However, if a definitive diagnosis is unclear, referral for specialist input is recommended, for example to a restorative, endodontic or periodontal specialist.
Figure 6. Clinically, two sinuses are present adjacent to LR6, one on the buccal and one on the lingual surface. A ‘tear-drop shaped radiolucency, which is seen on both the distal and mesial of the distal root (blue) and a ‘J shaped’ radioluency (orange) are shown. Both of these features, when seen radiographically, suggest a vertical root fracture may be present.Figure 7.
(a) LL6 has advanced chronic periodontitis that has extended to the apex of the distal root. This has resulted in pulpal necrosis. (b) An endodontic-periodontal lesion is present and, owing to the extent of bone loss and pocketing, the tooth has a hopeless prognosis (circled). Evidence of bone loss around adjacent teeth indicates pre-existing periodontitis (arrows).
Cemental tear
Vertical root fracture (VRF)
Periodontal abscess
Endo-periodontal lesion
Definition
A fragment of cementum partially or completely detached from the root surface at cemento-dentinal junction or within the body of cementum along the incremental lines
A fracture that extends through the enamel, dentine and pulp, down the long axis of the tooth27
A localized accumulation of pus within the gingival wall of the periodontal pocket34
Involvement of the pulp and periodontal disease in the same tooth
Teeth most likely to be affected
Incisors
Functional premolars and mesial roots of mandibular molars28,29 with lost marginal ridges +/-loss of a pulp chamber roof are most vulnerable to fracture30Presence of tapered cast metal or screw-type posts associated with higher risk31
Any tooth with pre-existing pockets in periodontitis casesCan also occur in non-periodontitis cases due to impaction of foreign bodies or alteration of root surface35
Any tooth. May or may not have had pre-existing periodontitis34Root damage, such as fractures and perforations, may be associated and have a reported reduced prognosis35
Pulpal status
Vital (unless previously extirpated and/or periodontal bone loss has extended sufficiently close to the tooth apex to cause pulpal necrosis
Tooth may have been root canal treated previously or have signs/symptoms of pulpal degeneration or necrosis
One isolated deep pocket, narrow or wide +/- suppuration
One or two (on opposite sides of tooth root) isolated deep, narrow pockets4
A deep pocket, suppuration, bleeding on probing with ovoid elevation of the gingiva35
Wide, deep pocket extending to, or very close to root end35
Radiographic findings
Majority of tears located on proximal root surfaces, in mid-third, along cementodentinal junctionThin radiopaque fragment along the root surface (Figures 2, 4, 5). Bone loss to the level of the tear is common
Vertical root fractures can occur in the bucco-lingual or mesio-distal direction. Unless tooth root has split, fractures are rarely identified radiographicallyIndirect suggestions: ‘Tear-drop’ or ‘J-shaped’ radiolucencies wrapping around root (Figure 6)
Periodontal abscesses often occur in patients with periodontitis. Bone loss around the tooth in question is often observed, including furcal bone loss in molars
Periradicular radiolucencies, including furcal bone loss in multirooted teeth, is common35Localized bony defect such as absence of alveolar bone over the entire root length can occur (Figure 7)
Treatment
Requires complete removal of torn fragment, either non-surgically or surgicallyRegenerative procedures may be useful to restore defect
Extraction: If fracture extends subgingivally or into pulp chamber/root canals32Cracks limited to the clinical crown may be possible to remove and a cuspal coverage restoration placed33
Acute management: Drainage, mechanical debridement +/- topical or systemic adjuncts. Alternatively tooth extraction, if appropriateDefinitive management: non-surgical or surgical periodontal treatment or tooth extraction
In teeth considered restorable, root canal treatment (RCT) should be performed prior to periodontal interventionFollowing RCT, spontaneous resolution of the periodontal defect may occur. If not, surgical regenerative procedures may be considered
Treatment aims
If the overall aim is to retain the tooth as a functional and aesthetic unit, treatment must remove the pathological source and restore structure and function.4 Complete removal of the fractured cemental fragment is necessary for a successful outcome. Torn fragments may be removed during non-surgical or surgical periodontal or endodontic procedures.1,4,36
Treatment options
To remove the cemental tear, the treatment approach is dependent on the location of the tear and the severity of periodontal disease.4
Large-scale studies and evidence-based publications on appropriate treatment options are limited. A range of procedures including root surface debridement, root canal treatment, periodontal microsurgery, peri-radicular microsurgery, guided-tissue regeneration (GTR), bone grafting and intentional replantation have all been reported as being used to manage cemental tears.4,36,37 These options are summarized below.
Watchful waiting/treatment delay
Although an option, this is not a recommended approach because of the ongoing periodontal and/or peri-radicular bony destruction that may culminate in tooth loss.
Active treatment to retain tooth in a functional and aesthetic state: non-surgical procedures
For cemental tears present in, or adjacent to, the cervical third of the root, a non-surgical approach, such as root surface debridement may be sufficient to completely remove the fractured cemental fragment.38
Active treatment to retain tooth in a functional and aesthetic state: surgical procedures
Periodontal microsurgery
If a non-surgical approach fails, or the tear is located in the mid-third of the root length, periodontal microsurgery is likely to be required to remove the fragment.1,8,36 Microsurgery is a minimally invasive technique that aims to improve visual acuity and surgical outcomes. It is carried out with a surgical microscope and smaller adapted instruments and suture materials.39 A dental microscope is considered essential for better visualization, improved access and to facilitate complete removal of cemental tears during the procedure.2
Endodontic microsurgery
If the cemental tear is in the apical third of the root length, the periodontal bone loss and pocketing is likely to have challenged the pulpal health. Sensibility testing is recommended. If pulpal necrosis is confirmed through evidence of radiographic peri-radicular changes, together with negative sensibility test results, root canal treatment may be commenced if the tooth is to be retained and considered restorable and of satisfactory prognosis. Following this, peri-radicular microsurgery is carried out for complete removal of the cemental tear in the apical region.1,4
Regenerative procedures
While conventional periodontal surgery aims to result in reparative healing, guided-tissue regeneration (GTR) stimulates regeneration of lost tissues. Reparative healing is repair by scar-tissue formation, that is healing with connective tissue and long junctional epithelium, which does not fully restore the lost tissue to its original form. Regeneration is favoured over repair because it is healing of tissues to their original form (ie no scar tissue).40,41 GTR prevents migration of epithelial cells into the wound and therefore also prevents formation of scar tissue. Regeneration is considered preferable because lost tooth-supporting structures are rebuilt, such as cementum, periodontal ligament and alveolar bone.42
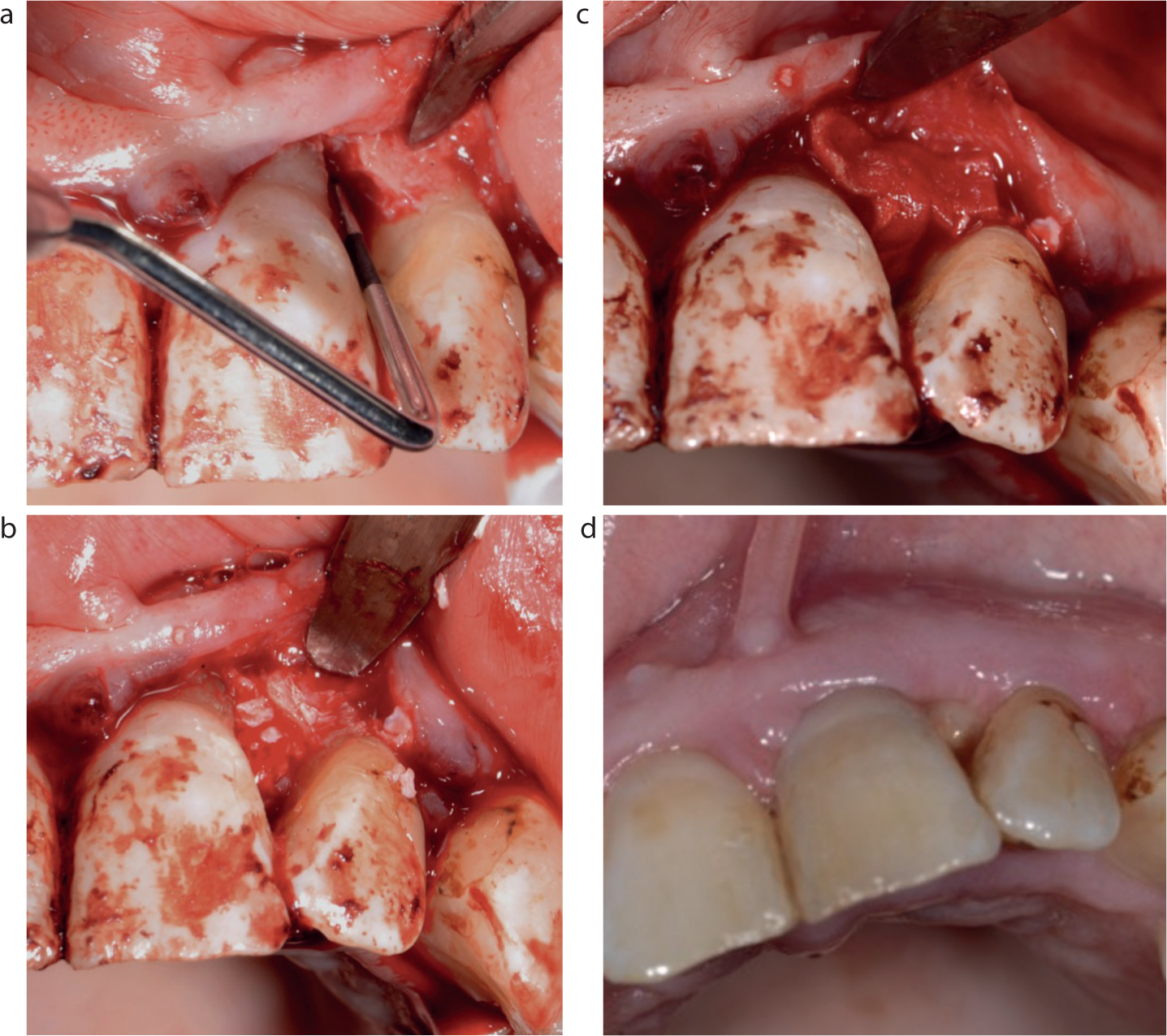
Following surgical removal of the cemental tear, GTR, with or without bone grafting, can be considered to restore the structure and function of the defect. Figure 8 illustrates this procedure being carried out.
Figure 8. GTR procedures carried out for the same patient as shown in Figures 2 and 3. (a) A three-walled vertical bone defect was seen during surgical exploration, with loss of half of the buccal wall. (b,c) The cemental tear was removed and the defect was packed with Bio-Oss and Bio-Gide (Switzerland). (d) The appearance of UL1 at 1 week review post GTR. Images courtesy of Dr Andrew Pye.
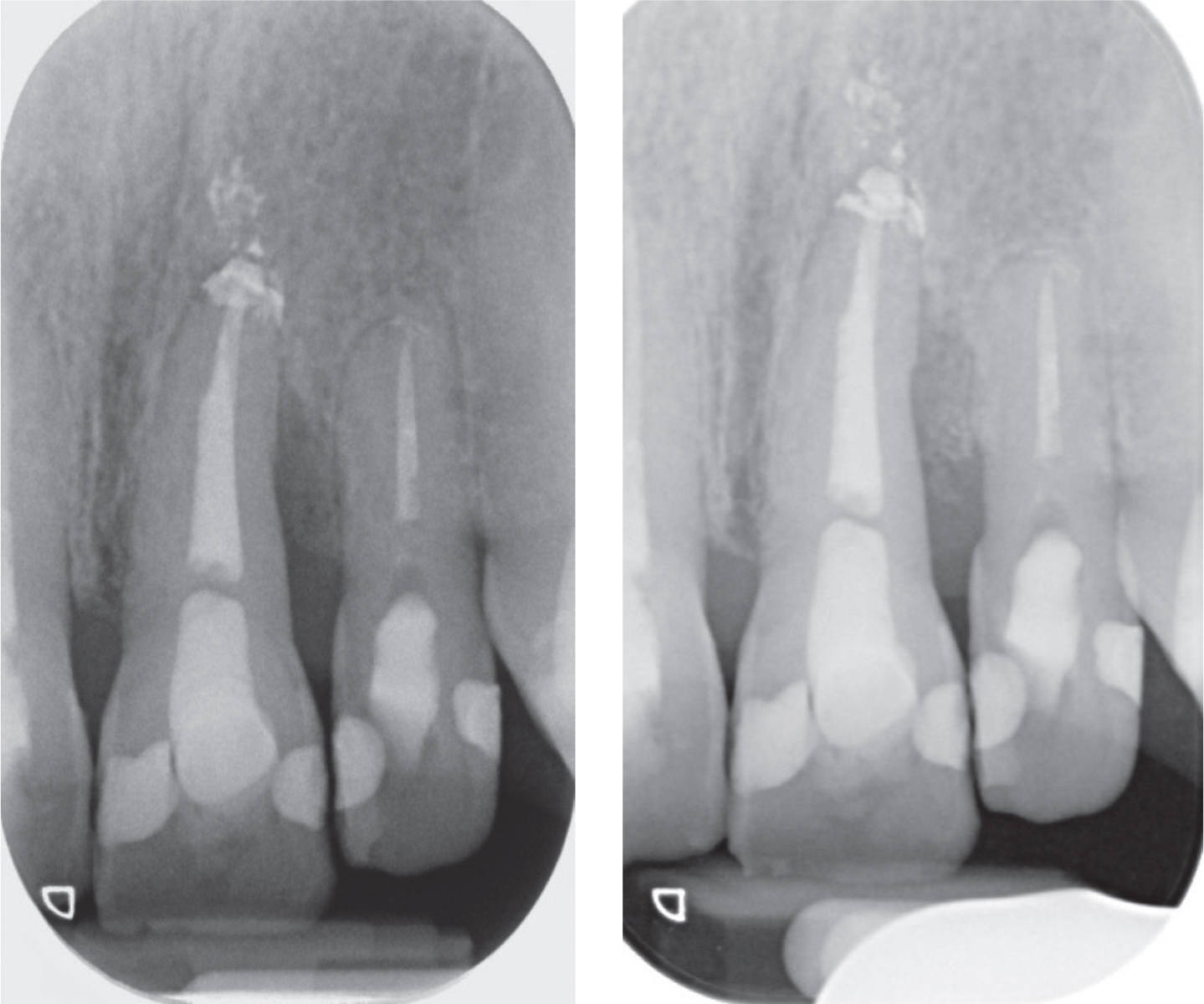
Follow-up is necessary to ensure resolution of periodontal pocketing clinically. Radiographically, evidence of bony infill and increased radiodensity in the periodontal defect is sought. An example is shown in Figure 9.
Figure 9. Further images of the case seen in Figures 2, 3 and 8. (a) Pre GTR, root canal re-treatment was carried out and a distal infrabony defect persists on UL1. (b) 1-year review after GTR. Evidence of bony infill and increased radiodensity in the vertical periodontal defect on the distal surface of UL1.
Enamel matrix derivative (EMD) is porcine tooth-germ extract used to stimulate the regeneration of both soft and hard tissue.43 EMD has been reported as having been used successfully in the management of a cemental tear in a 10-year follow-up study41, as has hyaluronic acid used with a resorbable collagen membrane.44 However, both studies are case reports and more evidence is needed to draw clear conclusions on the advantages, disadvantages and long-term outcomes of these techniques.
Intentional replantation
If it is not thought possible to completely remove the cemental tear using conventional or ideally, microsurgical approaches, intentional replantation has been reported as a possible last resort to salvage a tooth.45 This is performed by extracting the tooth, removing the pathological source and re-implanting the extracted tooth. Although an option, it is an uncommon procedure and in the authors' opinion, not a recommended approach. The risks of this procedure include root fracture during extraction, external resorption of the replanted tooth or ankylosis, which may occur due to periodontal ligament damage.46
Tooth extraction
In some cases, particularly those of late diagnosis, the amount of bone loss and extent of pocketing around a tooth (+/- tooth mobility), may render the tooth unsalvageable and extraction is recommended.
Prognosis
Teeth with cemental tears have an unpredictable prognosis.47 The success rate, generally reported as no signs or symptoms, is higher for cemental tears managed surgically because cemental tears are better identified and removed during surgical procedures.1,36,37 The best outcomes are reported for tears located in the mid-third and cervical third of roots.36 Tears located in these regions may be completely removed more easily during treatment, whereas tears in the apical third have the lowest success.36 It is suspected that persistent micro-organisms and tear fragments at the apical third (usually U-shaped) are more difficult to remove.9,33,36
Given the limited number of studies available in the literature, the criteria used to define ‘success’ and ‘failure’, as well as the follow-up times vary between studies. It is difficult to determine the prognosis of cemental tears because there are currently no randomized control trials investigating the effectiveness of different treatment methods for cemental tears. To gain an accurate insight into the prognosis of cemental tears, there is a need for high-quality and prospective studies on the treatment outcomes of the various management strategies, ideally under controlled conditions, with larger sample sizes and long-term follow up.
Delayed diagnosis or misdiagnosis is likely to reduce the treatment outcome considerably; however, there is a paucity of high-quality research available in the literature to confirm this, understandably, owing to the rarity of the condition.
Conclusion
Cemental tears predispose to plaque-induced rapid periodontal tissue loss. Diagnosis can be challenging. Knowledge of cemental tears, together with thorough clinical and radiograph examinations are important in distinguishing between tears and other possible diagnoses presenting with similar findings.
Positive outcomes for teeth with cemental tears can be achieved if clinicians accurately diagnose the condition early. This allows the appropriate treatment approach to be embarked on, with the aim of completely removing the tear/fractured cemental fragments, while the tooth is salvageable.
Managing such cases is complex, and the benefits afforded by the operating microscope and the use of microsurgical and regenerative techniques is likely to impact favourably on the treatment outcome. Clinicians are encouraged to expedite exclusion of other provisional diagnoses discussed in this article, before considering referral to a specialist for management of the cemental tear, when appropriate.