Defective dental restorations: to repair or not to repair? part 2: all–ceramics and porcelain fused to metal systems Igor R Blum Daryll C Jagger Nairn H F Wilson Dental Update 2025 38:3, 150-158.
Clinical Lecturer/Hon Specialist Registrar in Restorative Dentistry, University of Bristol Dental Hospital & School at Guy's, King's College and St Thomas' Hospitals, London, UK
Professor of Restorative Dentistry and Dean and Head of King's College London Dental Institute at Guy's, King's College and St Thomas' Hospitals, London, UK
With the increasing use of ceramics in restorative dentistry, and trends to extend restoration longevity through the use of minimal interventive techniques, dental practitioners should be familiar with the factors that may influence the decision either to repair or replace fractured metal-ceramic and all-ceramic restorations and, also, the materials and techniques available to repair these restorations. This second of two papers addresses the possible modes of failure of ceramic restorations and outlines indications and techniques in this developing aspect of restoration repair in clinical practice.
Clinical Relevance: The repair of metal-ceramic and all-ceramic restorations is a reliable low-cost, low-risk technique that may be of value for the management of loss or fracture of porcelain from a crown or bridge in clinical practice.
Article
Ceramics are widely used in dentistry given their favourable aesthetic properties, excellent biocompatibility and chemical durability. The diversity of colour and translucency enable ceramics to ‘mimic the optical properties of enamel and dentine’.1 Not surprisingly, the popularity of all-ceramic restorations and the number of all-ceramic materials and systems commercially available for clinical use, including in stress-bearing areas, have been reported to be increasing.2–4
Despite the clear trends towards the use of minimally interventive, direct restorative techniques, the use of all-ceramic restorations, including ceramic inlays, onlays, veneers, all-ceramic crowns and all-ceramic bridges, is anticipated to continue to expand. The reasons for this anticipated growth may be attributed to patients' increasing aesthetic expectations, advancements in ceramic technologies, developments in computer-aided design and computer-aided manufacturing (CAD/CAM) and the further development of all-ceramic adhesive systems.
Failure of ceramic restorations
Ceramic restorations may fail in clinical service and, in common with all other types of restorations, should not normally be considered to be permanent. Next to secondary caries, as diagnosed clinically, porcelain fracture and chipping have been reported to be the major cause for the replacement of both all-ceramic and ceramic fused to metal restorations.5–7 The literature, however, includes conflicting data on the incidence of failure as a consequence of fracture or chipping. A retrospective study6 on the longevity of porcelain fused to metal bridges reported the five-year failure as a result of fracture of the porcelain facing to be 8%. Other studies that have investigated longevity of metal–ceramic restorations have reported failure rates resulting from fracture of the porcelain facing to be in the range of 2.3–18%, over a seven-year period.5,8 Recent systematic reviews reported the five-year failure as a result of chipping of the porcelain facing to be 3.7% and 5.7% for all-ceramic and metal-ceramic single crowns, respectively, and 13.6% and 2.9% for all-ceramic and metal-ceramic fixed-fixed bridges, respectively.9,10
It has been suggested that possible reasons for porcelain fractures in both metal-ceramic and all-ceramic restorations include:
Contamination and other errors in fabrication;
Incorrect treatment planning with inappropriate use of the material, notably in relation to the occlusion, and failure to create sufficient space for the restoration.11,12
Furthermore, given the inherent brittle characteristics and relatively low tensile strength of ceramics, both all-ceramic and metal-ceramic restorations are prone to fracture in clinical service when subjected to impact loading and other high extrinsic stresses.13 A longitudinal study which evaluated the clinical performance of 96 leucite-reinforced glass ceramic inlays and onlays (IPS Empress, Ivoclar Vivadent, Liechtenstein) over a six-year period, reported bulk fracture as the most common cause of failure in 9% of 67 restorations reviewed at recall.7 Similarly, in another clinical study which looked at the performance of 33 leucite-reinforced glass ceramic inlays, over an eight-year period, the single failure observed related to fracture of the ceramic material.14 These clinical findings are in agreement with the view of other investigators who reported that bulk fracture of the ceramic material is the main reason for failure in all-ceramic restorations.11
Porcelain fracture in metal-ceramic restorations
The cause of fracture of veneering porcelain in metal-ceramic restorations has been reported to be multi-factorial.15 Such fractures may be classified as:
Simple: involving only the porcelain, eg intra-ceramic defects, trauma and parafunctional habits.16,17
Complex: associated with the exposure of metal substructure, eg failures at the metal-ceramic interface, improper design, inadequate framework support for the porcelain, flexural fatigue of the metal substructure and internal stresses resulting from incompatibilities of coefficients of thermal expansion between the porcelain and the metal.
Porcelain fracture in all-ceramic restorations
Most all-ceramic systems have a two-layer structure, comprising a high strength ceramic substructure core and a relatively weak veneering ceramic layer.18 The most frequent mode of fracture for all-ceramic restorations occurs in the form of internal surface crack formation, owing to high stress concentration areas. This results in fracture initiation and propagation from the inner, unglazed fitting surface outwards towards the veneering ceramic material; thus leading to fracture and exposure of the substructure core.19 Variations in fracture toughness have been reported to exist among the various high strength ceramic cores.4,20 The most common causes of fracture of all-ceramic restorations have been reported to include intra-ceramic defects, trauma and parafunctional habits.11,21
Managing porcelain fractures
A replacement approach to the management of all-ceramic and metal-ceramic restorations that suffer fractures, which could be repaired, is based on a flawed mechanistic style of restorative dentistry.22 The result, notwithstanding cost and time considerations for the patient, is the unnecessary removal of sound tooth tissue, iatrogenic weakening of the remaining tooth structure and an increased risk of loss of tooth vitality.13 In contrast, the repair of defective ceramic restorations, ie partial replacement of a ceramic restoration allowing preservation of that portion of the restoration which presents no clinical or radiographic evidence of failure, is a conservative approach, preserving tooth-structure and extending the life of the tooth.
It cannot be overemphasized, however, that when a patient presents with a fracture of a ceramic restoration, in particular, soon after provision of the restoration, it is important to diagnose and eliminate the reason for the fracture, for example excess occlusal loading. Otherwise, the repaired restoration may be subjected to the same, possibly unrecognized, limitations of the original restoration.
Given the benefits of the minimally interventive approach of repair rather than replacement, several dental material manufacturers have developed products for performing chairside aesthetic and functional composite resin repairs of ceramic restorations.23 Reasons for performing an intra-oral repair of a ceramic restoration, other than those considered already, include the opportunity to avoid lengthy clinical appointments, the provision of a temporary restoration, the avoidance of laboratory costs and the elimination of the risk of iatrogenic damage to periodontal tissues in the process of providing a new indirect restoration.11
The development of porcelain repair systems
The growing use of metal-ceramic and all-ceramic restorations during the 1970s and 1980s resulted in an increased incidence of ceramic fractures and growing interest in porcelain repair systems and techniques. The material of choice for the repair of all forms of ceramic restorations is composite resin, given the favourable aesthetic properties, handling and cost benefits of this material.24 The first ceramic repair systems, including silane primers, to mediate chemical bonds between composite resins and organic and inorganic surfaces were developed in the late 1970s.25,26 Subsequently, systems were introduced using refined techniques and the development of successive generations of resin-based adhesives.27,28 Since the late 1990s, developments in ceramic repair systems have continued, employing various repair protocols and the use of state-of-the-art composite resins.13
Findings from laboratory-based ceramic repair studies recommend a combination of mechanical and chemical surface procedures to promote satisfactory adhesion between a repair with composite resin and the ceramic substrate.28,29 It is not surprising, therefore, that current generations of porcelain-repair systems rely on micromechanical retention, mediated through acid etching with hydrofluoric acid or acidulated phosphate fluoride and/or airborne-particle abrasion and chemical retention, facilitated by means of the application of a silane coupling agent.
It has been suggested that the removal of the glazed ceramic layer, if still present, can contribute to a stronger composite resin-ceramic bonding.30 Removal of the glazed layer may be performed mechanically, chemically or by a combination of these methods.12 It has been reported that roughening of porcelain surfaces prior to bonding is best performed by airborne particle abrasion.12 However, if particle abrasion is not available to the practitioner then roughening may be performed using a diamond bur. This should be done under light operating pressures at high speed to avoid the vibration associated with the use of low-speed handpieces, which could produce cracks and fissures at the ceramic margins.12
Surface treatment
Acid etching, grit-blasting with aluminium oxide or sandblasting with silica-coated particles are the most common methods of surface treatment described in the literature.12,13
Acid etching
Acid etching provides a clean surface with enhanced capacity for micromechanical retention and, as a consequence, increased bond strength potential. Three types of acid etchant have been reported in the literature for the surface preparation of dental ceramics: hydrofluoric acid,31 acidulated phosphate fluoride32,33 and phosphoric acid.34
Hydrofluoric acid
Hydrofluoric acid (HF) acts on the silicon dioxide (SiO2) of the glass phase of ceramics, creating surface microporosity, which allows the formation of a mechanical interlock with the composite resin.35 HF is, however, poisonous and caustic and poses a health hazard owing to its toxicity and volatility.36 During intra-oral ceramic repair procedures involving the use of HF, both dental personnel and the patient may be exposed to a substantial risk of acid damage to, in particular, the soft tissues. Consequently, rubber dam isolation, careful use of the triple air water syringe, removal of any acid excess and the use of a high volume aspirator are of paramount importance to maximize safety precautions.
The recommended etching time for HF has been reported to range from 20 seconds to 20 minutes, depending on the concentration of the acid and the type of ceramic substrate.29,37 The concentration of HF used for ceramic repair varies between 5% and 10%.12 The clinical use of this acid requires meticulous attention to detail with great respect for the potential for significant iatrogenic damage and harm to the dentist, dental nurse and patient.
Although numerous authors29,31,37 have demonstrated that etching porcelain with HF significantly contributes to enhanced bond strength of the repair composite resin, Filho and co-workers24 have suggested that the risks posed by the use of HF outweigh the benefits. This view is supported by others12 who stated that a consensus had not yet been reached regarding the justification for the use of HF, as similar outcomes had been reported with other surface treatments. Examples of commercially available porcelain repair systems using HF are the Ultradent® Porcelain Repair Kit (Ultradent, Utah, USA) and Ceram-Etch (Gresco Products Inc Stafford, Texas, USA).
Acidulated phosphate fluoride
Acidulated phosphate fluoride (APF) gel is commonly used for topical fluoride applications.38 Unlike HF, APF in low concentration has been reported to be safe for intra-oral use with little, if any, risk of damage to, in particular, soft tissue.33 Consequently, 1.23% APF gel has been used for ceramic surface etching prior to bonding with composite resin.39
Laboratory studies have failed to reveal any significant differences in adhesive bond strength between composite resin and feldspathic porcelain treated with either 9.5% HF for four to five minutes, or 1.23% APF gel for 10 minutes.32,33 A similar study found no significant difference in the adhesive bond strength between composite resin and all-ceramic specimens treated with 9.6% HF for four minutes or 1.23% APF gel treated for seven to ten minutes.24 It has been suggested, however, that an APF gel application time of less than seven minutes produces lower bond strengths, but this difference has not been found to be of statistical significance.12
Interestingly, surface analyses of HF-etched and APF gel-etched ceramics have revealed different etching patterns.40 HF interacts with silica in the glass matrix in feldspathic porcelain, resulting in the selective removal of the glassy matrix, exposure of crystalline structures and an increase in surface roughness.2,41,42 In contrast, APF attacks the glass phase of ceramics, probably due to the selective release of sodium ions, interrupting the silica network and creating small pits around the leucite crystals in the ceramics, producing surface microporosity.33,41 It has been reported, however, that APF gel produces minimal surface topography change in ceramics, with differences in etching patterns being found to be related to the etching time and concentration of the etching agent.43
Whereas existing literature indicates an etching time of 4 to 15 minutes with APF gel, depending on the type of ceramic, Bertolotti and co-workers44 recommend a 10-minute etch, irrespective of variation in the substrate. Whatever etching time is selected, it would be beneficial to the patient and clinician if etching times with APF could be shortened. At present, APF is not available as a component of a commercial porcelain repair system. It is commercially available, however, as a separate product. An example of a product containing 1.23% APF gel is Protect® (John O Butler Co, Chicago, USA).
Phosphoric acid
While phosphoric acid etching fails to effect any change in the morphology of ceramic substrates, it may be used to good advantage for surface cleaning, following mechanical roughening.45 It has been suggested that etching with 35–40% phosphoric acid is indicated where a fracture is associated with exposed enamel and dentine, in particular, in situations where there is no risk of iatrogenic damage to soft tissues.12,34
Commercially available porcelain repair kits containing phosphoric acid include Clearfil Repair® (Kuraray, Japan) and Ceramic Repair® (Ivoclar Vivadent, Liechtenstein).
Grit-blasting with aluminium oxide
Several authors have reported that grit-blasting with particulate aluminium oxide cleans ceramic surfaces and forms surface irregularities which increase the surface area available for bonding.29,46 The grit-blasting of fractured ceramic surfaces is usually performed using purified aluminium oxide particles of 30–250 μm diameter, delivered in a 2–3 bar airstream applied for approximately 15 seconds. The nozzle of the grit-blasting handpiece should be held perpendicular to and 10 mm from the ceramic surface.46 Care is required to avoid injuries to soft tissues and to control the spread of aluminium oxide particles in the operative area. This may be accomplished using rubber dam isolation and a high-volume aspiration system.12,47
Sandblasting with silica-coated particles
An air-abrasion technique, based on tribochemical silica-coating (silicatization) and chemico-physical bonding, was developed in the 1980s for laboratory conditioning of ceramic substrate surfaces.48 This technique (Rocatec; 3M, Seefeld, Germany) increases the ceramic–composite bond through an increase in the silica content of the substrate surface.23,46 Initially, the ceramic substrate surface is sandblasted with a compressed airstream of 30 μm diameter size silica-coated alumina particles. The particles hit the surface, causing locally high temperature increases (up to 1200 °C) developed by the transfer of the kinetic energy of the particles. The blasting results in silica particles being embedded in the substrate surface to a depth of 10–15 μm, making the surface more reactive chemically, and thereby enhancing silane-mediated bonding. Metal surfaces exposed in the fracture of metal-ceramic restorations may be sandblasted in a similar manner to ceramic surfaces, with a similar outcome in terms of an enhanced silane-mediated bonding capacity.
The substrate surface, be it ceramic or metal alloy, is left, after sandblasting, covered in a layer of small silica particles which provide both micromechanical retention and sites for chemical adhesion.49,50 The silicacoated substrate surface is subsequently silanized by the application of a silane coupling agent to allow covalent bonding between the silica-coated ceramic layer and an applied adhesive resin-based system, such as a composite resin. This bonding mechanism is not dissimilar to the chemical binding of silanized filler particles in resin-based composites.51 An example of a commercially available silica-coating system for dental use is the CoJet system (3M ESPE, Seefeld, Germany).
It is important to note that the terms ‘surface etching’, ‘surface conditioning’, airborne particle abrasion’, ‘grit-blasting’, ‘roughening’, ‘sandblasting’, ‘silica-coating’ all appear in the literature, often used as synonyms. This variation in terms often leads to misunderstanding and, in certain situations, confusion in respect of methods and techniques.
The application of a silane coupling agent is the most common chemical surface treatment procedure described in the literature pertaining to the intra-oral repair of dental ceramics. Silane coupling agents (silanes) have been extensively utilized in the development of porcelain repair systems and are included in virtually all porcelain repair kits: Cimara® (Voco, Germany), Ceramic Repair® (Ivoclar Vivadent, Liechtenstein), Clearfil Repair® (Kuraray, Japan), Bistite II DC® (Tokuyama, Japan), Ultradent® Porcelain Repair (Ultradent, USA), Ceram–Etch® (Gresco Products, USA) and the CoJet® repair system (3M ESPE, Germany).
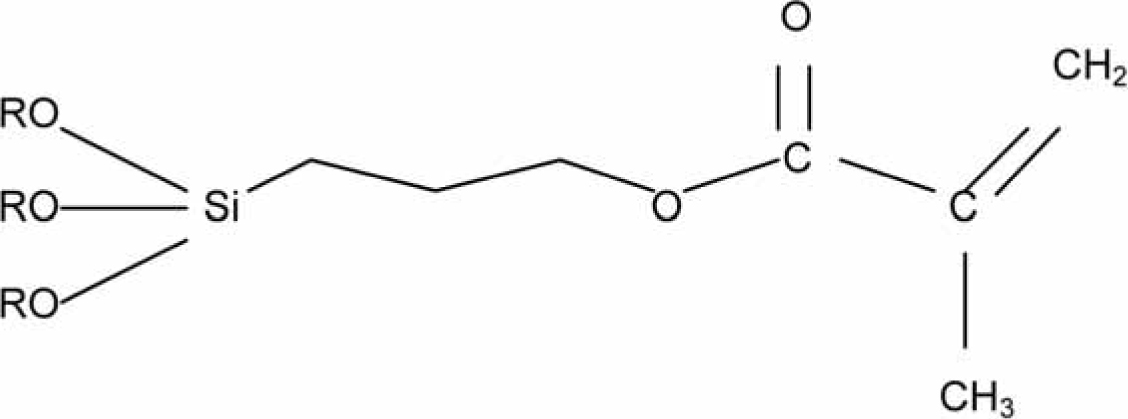
Silane coupling agents are mediators that promote adhesion between inorganic and organic substances.51 They are characterized as molecules with two ends of different polarity; they are bifunctional and have dual reactivity: the hydrolyzable alkoxy groups of the silanol unit, (RO)3Si group on the left side in Figure 1, form a chemical bond with the silicatized surface. The methacrylate groups on the right side in Figure 1 copolymerize with the monomers of adhesive resins. This allows a chemical bond to be achieved between a ceramic surface and an applied resin. Silanes may also be viewed as materials that increase the surface energy of an acid-etched ceramic so that a hydrophobic composite resin can more easily penetrate into it.46
Figure 1. Chemical formula of a typical silane coupling agent (3-methacryloxypropyltrimethoxysilane).
Review of repair approaches for dental ceramics
Various ceramic repair techniques have been described in the literature.12,52,53 Numerous studies have demonstrated that, irrespective of the surface treatment selected, the application of silane significantly increases the bond strength of the composite resin repair to the fractured ceramic, enhancing the clinical success of the repair procedure.24,29,30,54 Whenever a metal surface is also exposed, the use of an opaquer is indicated to mask the grey colour of the metal.
While silica coating of both ceramic and metal-ceramic substrates, followed by the application of a silane, yields significantly higher repair bond strengths than other techniques,7,15 a more recent study17 has failed to demonstrate significant differences between the silica-coating approach and other commercially available porcelain repair systems. Most studies are, however, in agreement that commercially available porcelain repair systems exhibit bond strengths in excess of the 10 MPa required to effect a clinically viable bond between a ceramic substrate and a composite resin system.55
Clinical case 1
A 35-year-old woman was referred because of loss of ceramic from two metal-ceramic crowns following trauma. Examination showed a complex fracture where porcelain had fractured from the labial surfaces of the patient's maxillary right lateral incisor and canine teeth (Figure 2). Clinical and radiographical examination indicated that the crown margins were sound, although some gingival recession was present. The patient stated that she was satisfied with the appearance of the crown margins as they were not visible on smiling and it was therefore decided to repair the crowns. The shade of the crowns was noted. The defective crowns were then isolated using rubber dam and the patient was provided with protective eyewear. The exposed metal was sandblasted using an intra-oral sandblaster (Microetcher: Danville Engineering) filled with CoJet sand at 40psi for 15 seconds, which had resulted in a matt appearance of the exposed metal surface (Figure 3). Silane (ESPE-SIL) was then applied to the treated metal surface and allowed to dry for 30 seconds. The powder and liquid of the opaquer (Visio Gem, 3M ESPE) were mixed and applied in a thin layer to the exposed metal and light cured for 10 seconds. A layer of unfilled resin (Visio Bond, 3M ESPE) was then applied to the opaquer and light cured for 20 seconds, following which the defect was repaired using a composite resin restorative material (Figure 4).
Figure 2. The loss of ceramic from the metal-ceramic crowns following trauma is evident (presented with kind permission of George Warman Publications).Figure 3. After treatment with CoJet powder from an intra-oral sandblaster the exposed metal has a matt appearance.Figure 4. The repair was completed with the CoJet system and a composite resin restorative material (Filtek Z250; 3M ESPE).
Clinical case 2
The patient, a 35-year-old female, attended following trauma to UL2, a metal-ceramic bridge pontic. The bridge was of adequate fit and appearance: it had not been loosened during the trauma. The ceramic at the incisal edge of the pontic had been fractured off (Figure 5), with a small amount of metal exposed (complex fracture). Although it was considered that a replacement bridge could be constructed with improved aesthetics, the patient requested that an attempt be made to repair the existing bridge and this was duly carried out under rubber dam isolation using the stages of the CoJet system (3M ESPE, Seefeld, Germany) and a composite resin restorative material; a substantially more minimally invasive option than a replacement bridge (Figure 6).
Figure 5. Ceramic had been lost from the metal-ceramic bridge pontic following trauma.Figure 6. Completed repair of the bridge pontic in Figure 5 using the CoJet system and composite resin material (Filtek Z250; 3M ESPE).
Both repairs have functioned satisfactorily for over one year and will be kept under review. Further clinical studies are required to determine the performance and longevity of the technique described. Such work should be part of a programme of work to provide the evidence base necessary to advance minimally interventive dentistry further.
Conclusion
Given the ever–increasing application of dental ceramics in restorative dentistry, dental practitioners are increasingly likely to undertake the repair of fractured ceramic restorations. As with all repair procedures, careful diagnosis and treatment planning, meticulous technique and subsequent monitoring is important in achieving favourable clinical outcomes.