Chaturvedula BB, Muthukrishnan A, Bhuvaraghan A Dens invaginatus: a review and orthodontic implications. Br Dent J. 2021; 230:345-350 https://doi.org/10.1038/s41415-021-2721-9
Thakur S, Thakur NS, Bramta M, Gupta M Dens invagination: a review of literature and report of two cases. J Nat Sci Biol Med. 2014; 5:218-221 https://doi.org/10.4103/0976-9668.127341
White SC, Pharoah M Oral Radiology: Principles and Interpretation. 2000;
Gündüz K, Çelenk P, Canger EM A retrospective study of the prevalence and characteristics of dens invaginatus in a sample of the Turkish population. Med Oral Patol Oral Cir Bucal. 2013; 18:e27-32 https://doi.org/10.4317/medoral.18285
Colak H, Tan E, Aylıkçı BU Radiographic study of the prevalence of dens invaginatus in a sample set of Turkish dental patients. J Clin Imaging Sci. 2012; 2 https://doi.org/10.4103/2156-7514.97755
Zhu J, Wang X, Fang Y An update on the diagnosis and treatment of dens invaginatus. Aust Dent J. 2017; 62:261-275 https://doi.org/10.1111/adj.12513
Oehlers FA Dens invaginatus (dilated composite odontome). I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol. 1957; 10:1204-1218 https://doi.org/10.1016/0030-4220(57)90077-4
Ridell K, Mejàre I, Matsson L Dens invaginatus: a retrospective study of prophylactic invagination treatment. Int J Paediatr Dent. 2001; 11:92-97 https://doi.org/10.1046/j.1365-263x.2001.00234.x
Alkadi M, Almohareb R, Mansour S Assessment of dens invaginatus and its characteristics in maxillary anterior teeth using cone-beam computed tomography. Sci Rep. 2021; 11 https://doi.org/10.1038/s41598-021-99258-0
Kfir A, Flaisher Salem N, Natour L Prevalence of dens invaginatus in young Israeli population and its association with clinical morphological features of maxillary incisors. Sci Rep. 2020; 10 https://doi.org/10.1038/s41598-020-74396-z
Bonsor DJ, Camilleri J Hydraulic cements for various applications in endodontics: part 2. Dent Update. 2023; 48:707-709
Kjaer I Morphological characteristics of dentitions developing excessive root resorption during orthodontic treatment. Eur J Orthod. 1995; 17:25-34 https://doi.org/10.1093/ejo/17.1.25
Mavragani M, Apisariyakul J, Brudvik P, Selvig KA Is mild dental invagination a risk factor for apical root resorption in orthodontic patients?. Eur J Orthod. 2006; 28:307-312 https://doi.org/10.1093/ejo/cjl006
Kronfeld R Dens in dente. J Dent Res. 1934; 14:49-66
Fischer CH To the question of the dens in dente. Dtsch tooth mouth Kieferheilkd. 1936; 3:621-634
Sprawson EC Odontomes. Br Dent J. 1937; 62:177-201
Rushton MA A collection of dilated composite odontomas. Br Dent J. 1937; 63:65-85
Euler HMünchen, Germany: Lehmann; 1939
Atkinson SR The permanent maxillary lateral incisor. Am J Orthod. 1943; 29:685-698
Bruszt P Etiology of dens in dente. SSO Schweiz Monatsschr Zahnheilkd. 1950; 60:534-542
Gustafson G, Sundberg S Dens in dente. Br Dent J. 1950; 88:83-88
Oehlers FA Dens invaginatus. II. Associated posterior crownforms and pathogenesis. Oral Surg Oral Med Oral Pathol. 1957; 10:1302-1316
Dens invaginatus is a developmental anomaly predominantly occurring in maxillary lateral incisors, resulting in the invagination of the enamel into the dentine. This infolded area creates a void enabling the stagnation of bacteria and development of dental caries. If left untreated the caries may progress and ultimately result in pulpal necrosis. The treatment of these teeth can be challenging due to the potential complexity of the lesion. It is essential that teeth with dens invaginatus are diagnosed early allowing prophylactic treatment and prevention of pulpal necrosis. This article aims to review the aetiology, prevalence, classification, diagnosis, treatment and orthodontic considerations of teeth affected by dens invaginatus.
CPD/Clinical Relevance: Knowledge of dens invaginatus enables early diagnosis, effective management and, therefore, the best treatment outcomes.
Article
Dens invaginatus (DI) is a developmental anomaly occurring during the formation of a tooth. It is the result of an invagination of the enamel organ into the dental papilla prior to calcification of the dental tissues.1
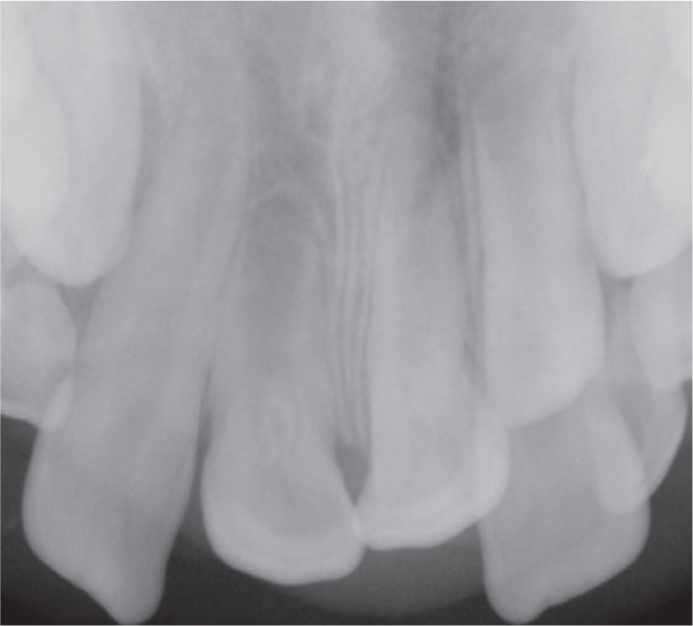
It has also been described as ‘dens in dente’, which translates as a ‘tooth within a tooth’ owing to its radiographic appearance.2 The name DI reflects the infolding of the enamel into the dentine, resulting in a pocket that may extend deep into the pulp chamber and, in certain cases, to the root apex. The invagination creates an area of dead space, separated from the pulpal tissues by only a thin layer of enamel and dentine.3 This stagnant area enables entry for bacteria and other potential irritants, presenting a predisposition for the development of dental caries and consequently pulpal necrosis. In certain cases, the enamel lining is incomplete, and some lesions may have channels existing between the invagination and the pulp.4 Pulp necrosis often occurs within a few years of tooth eruption, occasionally before complete closure of the apex. Immature teeth that have undergone pulpal necrosis may exhibit wide open or ‘blunderbuss’ apices radiographically (Figure 1). Abscess formation, cysts, displacement of teeth and internal root resorption have also been reported as sequelae of teeth with undiagnosed and untreated DI.1
Figure 1. Maxillary occlusal radiograph showing a transposed upper right lateral incisor with DI type II and a ‘blunderbuss’ apex.
Aetiology
Theories pertaining to the development of DI include growth pressures, discrepancies in cellular hyperplasia, genetic factors, trauma, infection, or alterations in tissue pressure. Despite the various theories that have been proposed (Table 1), the aetiology of DI remains unclear.
Table 1. List of theories surrounding the aetiology of DI.4
Distortion of the enamel organ during tooth development Protrusion of part of the enamel organ leads to the formation of an enamel-lined canal terminating at the cingulum or occasionally the incisal tip
Prevalence
Maxillary permanent lateral incisors are the teeth most affected by DI, with lesions typically seen under the palatal pit. DI has also been described in maxillary central incisors, maxillary canines, premolars and molars; however, this is less common.5,6 The occurrence of bilateral DI is not unusual, and DI lesions may also occur concomitantly with other dental conditions, such as macrodontia, hyperdontia, hypodontia, taurodontism and amelogenesis imperfecta.7,8 The prevalence of DI has been reported to be between 0.3% and 10%, with problems observed in 0.25–26.1% of individuals.2
Classification
DI has a broad spectrum of morphological variations, the most widely used classification is that described in 1957 by Oehlers, in which the anomaly is separated into three different forms: type I, type II and type III (Table 2).9 The determination of the type of DI is based on the radiographic appearance of how far the invagination extends from the crown into the root. Type III is separated into a and b depending on the positioning of the invagination's foramen. Based on Oehlers classification, the prevalence of each type of invagination was reported to be 79% for type I, 15% for type II and 5% for type III.2,6,10,11
Table 2. Oehlers classification of types of DI.9
Type
Properties
I
Minimal invaginationEnamel linedOccurs within the crown of the toothDoes not extend beyond the level of the cemento-enamel junction
II
Enamel linedExtends into the rootMay communicate with the pulp chamberNo communication with the periodontal ligament
IIIa
Invagination extends through the root, communicating laterally with the periodontal ligament through a pseudo-foramenThe pulp is compressed in the root, usually no communication with the pulp
IIIb
Invagination extends through the root, communicating with the periodontal ligament at the apical foramenUsually no communication with the pulp
Clinical assessment
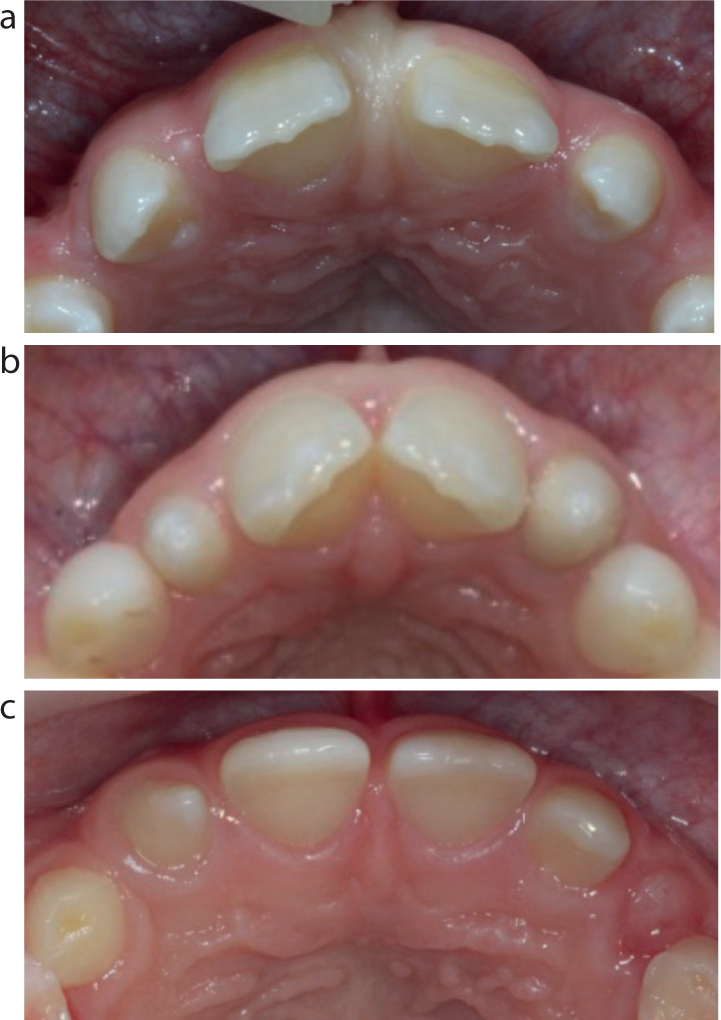
Clinically, most DI cases are asymptomatic and affected teeth may not show any apparent external deformity (Figure 2).12 The entrance to the invagination may be difficult to locate clinically and therefore, identification can require the use of methods such as the application of methylene blue dye applied to the palatal portion of the tooth.13 A 2020 study found 88% of teeth affected by DI to have unique clinical morphological characteristics.14 The following changes in the morphology of a tooth affected by DI have been described:
Increased width mesio-distally or labio-lingually;15
A deep palatal pit associated with an over-development of the cervico-lingual ridge;13
A labial groove with associated incisal notching.15
Figure 2. Clinical presentation of DI lesions based on Oehlers classification. (a) UL2: type I; UR2: type II. (b) Type IIIa. (c) Type IIIb.
Owing to the spectrum of morphological variations in the clinical presentation, radiographic examination provides a more reliable way to diagnose DI, and is the gold standard.
Radiographic assessment
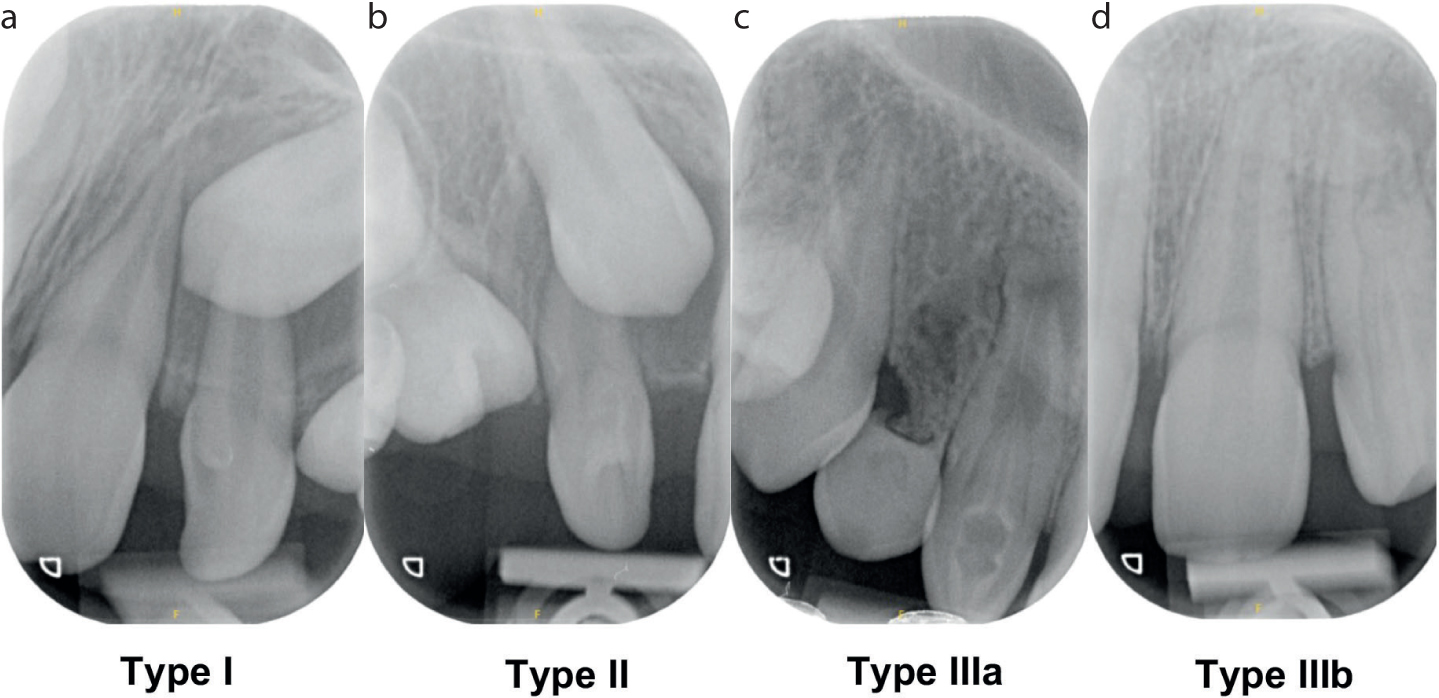
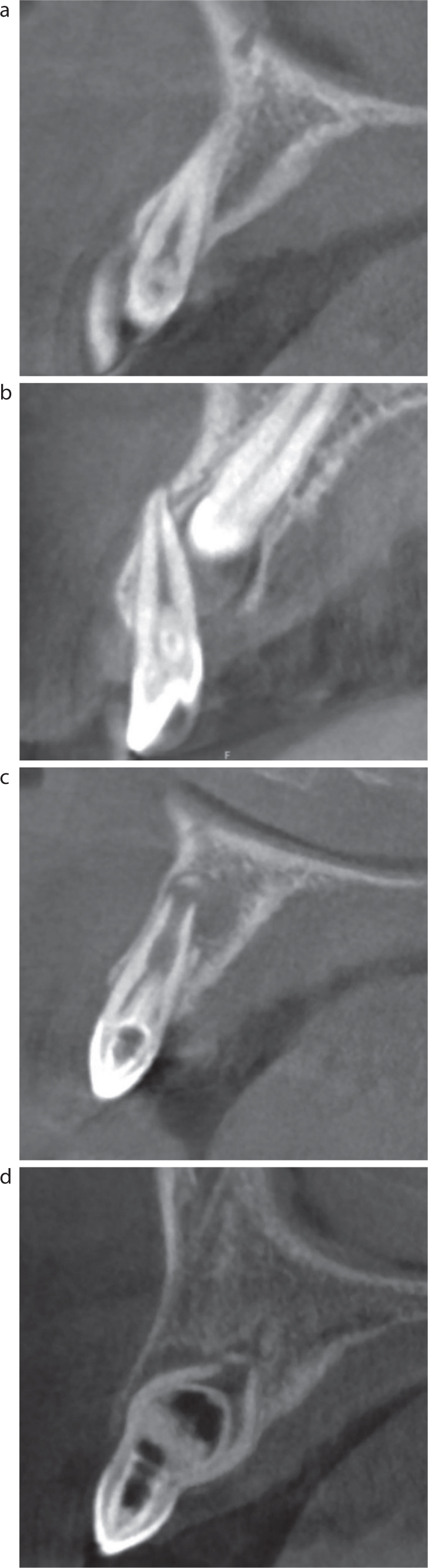
The radiographic presentation of teeth with DI varies depending on the lesion type (Figure 3). Radiographically, teeth with type I and II DI usually display a radiopaque projection (comparable in density to the enamel) varying in shape and depth, extending towards or into the pulp space.8 At the centre of the lesion is a radiolucent core.7 The cemento-enamel junction (CEJ) is used as a boundary to differentiate type I and type II lesions. Type II lesions cross the CEJ and extend as a pocket into the root, varying in depth, but not reaching the apical portion or connecting with the periodontal ligament (PDL).8 Type III lesions also display a radiolucent core with a radiopaque border; however, the invagination results in communication with the PDL, with type IIIa lesions communicating laterally via a pseudo-foramen and type IIIb lesions communicating through the apical foramen. Cone beam computed tomography (CBCT) scans provide detailed information on the internal morphology of the root canal system of affected teeth and can prove extremely beneficial if root canal treatment is to be undertaken (Figure 4).
Figure 3. Radiographic presentation of DI lesions based on Oehlers classification. (a) Type I; (b) type II; (c) type IIIa; (d) type IIIb.Figure 4. Cone beam computed tomography presentation of DI lesions based on Oehlers classification. (a) Type I; (b) type II; (c) type IIIa; (d) type IIIb.
Treatment options:
Owing to the complex anatomy of certain DI lesions, endodontic chemo-mechanical debridement and obturation can be extremely difficult.12 Other treatment complications arise with the tendency for the affected tooth to develop pulpal necrosis prior to completion of root formation. The lack of apical constriction in teeth with open ‘blunderbuss’ apices (Figure 1) is challenging to obturate. Previously, teeth affected by DI would have been considered poor prognosis and routinely extracted. While this may still be the preferred treatment option for teeth with severe invaginations, other treatment options are now advocated.13
Improvements in modern endodontics have enabled teeth affected by DI to be successfully treated with a combination of non-surgical and surgical techniques.12 However, despite these improvements, the treatment of these lesions should not be underestimated because they are still very challenging. Therefore, most cases are treated in secondary care or specialist practice.
Treatment of cases according to Oehler's classification
Oehlers' type I
Following the detection of a type I lesion with no evidence of pulpal disease, treatment should be carried out as soon as possible in order to prevent the development of caries. This is of particular importance for immature teeth with open apices owing to the difficulties encountered with root treating these teeth.13
Type I DI lesions can mostly be managed by sealing the invagination with a flowable composite resin to prevent the development of caries.1 In teeth where the entrance is not clinically visible however, and radiographically, there is evidence of a minimal invagination, these teeth should still be sealed to prevent bacterial contamination via a microscopic defect.
If there are signs of pulp necrosis, root canal treatment should be initiated. The root canal morphology of teeth with type I lesions is not usually grossly deformed and therefore, it is possible to complete a root canal treatment. The access cavity should incorporate the entire invagination to ensure adequate debridement and improve success of treatment.12 Techniques to achieve sufficient instrumentation of the invagination include the use of ultrasonic tips and Gates–Glidden burs under magnification.13
Oehlers' type II
Owing to the more extensive defect present in type II lesions, and difficulties with direct visualization, caries may develop within the invagination and remain clinically undetectable. The use of flowable composite resin to seal the defect, as with type I lesions, may result in the creation of a void and is not advisable. Therefore, creating a coronal entrance to enable inspection, preparation and aid debridement is more appropriate and will allow the invagination to then be fully sealed.
In the absence of signs of pulpal pathology, the tooth may be restored without involvement of the root canal systems. Tungsten carbide burs can be used under magnification to access the invagination. If caries is identified, it can be removed with ultrasonic tips or round long-neck burs. The invagination should then be further debrided with ultrasonic tips and either 1% sodium hypochlorite or chlorhexidine.13 If there are no signs of pulpal pathology, the invagination can then be dressed with a material to promote hard tissue formation (such as hydraulic cement),16 and then sealed with a composite resin.
If there is evidence of extensive caries or a communication with the pulp, then a pulpotomy or extirpation should be considered. This should be performed as with type I lesions; however, the invagination will extend further apically and is usually wider, therefore care should be taken to ensure the lesion is fully incorporated into the preparation.13
Oehlers' type III
Owing to the complexity and extent of type III lesions, the management is more difficult. If the tooth is asymptomatic and there is no evidence of pulp necrosis, a prophylactic approach should be adopted as for type I lesions.13 The affected tooth/teeth should then be closely observed clinically and radiographically to monitor the health of the pulp. It is recommended that a more conservative approach is adopted owing to the close proximity of the root canal system to the invagination. A more aggressive approach to treatment could result in iatrogenic pulpal involvement or inadequate debridement and restoration of the lesion.1
In some cases, patients may experience peri-invagination periodontitis, a condition in which the invagination becomes necrotic, leading to an inflammatory response within the periodontal tissues; however, the main pulp remains healthy and vital.3 In these cases, all efforts should be aimed at preserving the health of the pulp while treating the invagination in isolation. This may only be possible with type IIIa lesions because of the morphology and apical proximity of type IIIb lesions.13 Referral to an endodontic specialist is indicated for the treatment of type III lesions owing to their complexity.12
Orthodontic implications
Dental anomalies such as DI can impact planned orthodontic treatment, therefore early diagnosis is essential. The long-term prognosis of teeth with complex DI lesions, or those exhibiting pulpal symptoms should be considered along with the type of orthodontic treatment required to enable the formulation of a comprehensive treatment plan. Teeth with complex DI invaginations may be planned for extraction. Orthodontic consideration should be given to whether the remaining space is then closed (to avoid a prosthesis) or optimised for prosthetic replacement.12 It has been suggested that DI is a predisposing factor for root resorption during orthodontic treatment.17 However, a retrospective study by Mavragani et al found no statistically significant difference in the severity of root resorption of non-invaginated and invaginated teeth following orthodontics. Furthermore, the extent of the invagination did not relate to the amount of the root resorption.18
Conclusion
Teeth affected by DI have a wide variation in their clinical and radiographic presentation; however, they may also be asymptomatic and identified as an incidental finding. There are several approaches to the management of this dental anomaly, these are largely based on the type of lesion (Oehlers type I, II and III) and the health of the pulp. The most important objective for teeth affected by DI is the preservation of a healthy pulp. This can be achieved through the early diagnosis and prophylactic treatment of DI lesions, regardless of their type. This is essential in preventing the development of pupal pathology and therefore avoiding the need for complex specialist endodontic treatment.12,13 Orthodontic consideration should be given to teeth with complex lesions or pulpal pathology, and necessary interventions can be planned accordingly to help achieve the best result.