Loomans B. European statement of consensus regarding the treatment of severe tooth wear. Nederlands Tijdschrift voor Tandheelkunde. 2018; 125:223-231
Van't Spijker A, Rodriguez J, Kreulen C, Bronkhorst E, Bartlett D, Creugers N. Prevalence of tooth wear in adults. Int J Prosthodont. 2009; 22:35-42
Office for National Statistics. Living longer – how our population is changing and why it matters. 2020. https://tinyurl.com/2p984dsa (accessed January 2022)
Shellis R, Addy M. The interactions between attrition, abrasion and erosion in tooth wear. Monogr Oral Sci. 2014; 25:32-45
Lussi A, Carvalho T. Erosive tooth wear: a multifactorial condition of growing concern and increasing knowledge. Monogr Oral Sci. 2014; 25:1-15
The glossary of prosthodontic terms. J Prosthet Dent. 2017; 117:e1-e105
Falcon H, Richardson P, Shaw M Developing an index of restorative dental treatment need. Br Dent J. 2001; 190:479-486
Malkoc M, Sevimay M, Yaprak E. The use of zirconium and feldspathic porcelain in the management of the severely worn dentition: a case report. Euro J Dent. 2009; 3:75-78
Robinson S, Nixon P, Gahan M, Chan M. Techniques for restoring worn anterior teeth with direct composite resin. Dent Update. 2008; 35:551-558
Mehta S, Banerji S, Millar B, Suarez-Feito J. Current concepts on the management of tooth wear: part 4. An overview of the restorative techniques and dental materials commonly applied for the management of tooth wear. Br Dent J. 2012; 212:169-177
Ahmed K, Murbay S. Survival rates of anterior composites in managing tooth wear: systematic review. J Oral Rehab. 2015; 43:145-153
Milosevic A, Burnside G. The survival of direct composite restorations in the management of severe tooth wear including attrition and erosion: a prospective 8-year study. J Dent. 2016; 44:13-19
Magne P, Schlichting L, Maia H, Baratieri L. In vitro fatigue resistance of CAD/CAM composite resin and ceramic posterior occlusal veneers. J Prosthet Dent. 2010; 104:149-157
Gulamali A, Hemmings K, Tredwin C, Petrie A. Survival analysis of composite Dahl restorations provided to manage localised anterior tooth wear (ten year follow-up). Br Dent J. 2011; 211
Al-Khayatt A, Ray-Chaudhuri A, Poyser N Direct composite restorations for the worn mandibular anterior dentition: a 7-year follow-up of a prospective randomised controlled split-mouth clinical trial. J Oral Rehab. 2013; 40:389-401
Maroulakos G, Nagy W, Stathopoulou P Restoration of the worn dentition: basic prosthodontic principles and current rehabilitation techniques. Curr Oral Health Rep. 2017; 4:124-130
Vailati F, Belser U. Full-mouth adhesive rehabilitation of a severely eroded dentition: the three-step technique. Part 3. Eur J Esthet Dent. 2008; 3:236-257
Vailati F, Belser U. Full mouth adhesive rehabilitation of a severely eroded dentition: the three step technique. Part 1. Eur J Esthet Dent. 2008; 3:30-44
Loomans B, Opdam N. A guide to managing tooth wear: the Radboud philosophy. Br Dent J. 2018; 224:348-356
Smales R, Etemadi S. Survival of ceramic onlays placed with and without metal reinforcement. J Prosthet Dent. 2004; 91:548-553
Van Dijken J, Hasselrot L. A prospective 15-year evaluation of extensive dentin–enamel-bonded pressed ceramic coverages. Dent Mater. 2010; 26:929-939
Lu T, Peng L, Xiong F A 3-year clinical evaluation of endodontically treated posterior teeth restored with two different materials using the CEREC AC chair-side system. J Prosthet Dent. 2018; 119:363-368
Kaytan B, Onal B, Pamir T, Tezel H. Clinical evaluation of indirect resin composite and ceramic onlays over a 24 month period. Gen Dent. 2005; 53:329-34
Mehta S, Banerji S, Millar B, Suarez-Feito J. Current concepts on the management of tooth wear: part 1. Assessment, treatment planning and strategies for the prevention and the passive management of tooth wear. Br Dent J. 2012; 212:17-27
Hemmings K, Truman A, Shah S, Chauhan R. Tooth wear guidelines for the BSRD part 2: fixed management of tooth wear. Dent Update. 2018; 45:590-600
Maroulakos G, Nagy W, Stathopoulou P Restoration of the worn dentition: basic prosthodontic principles and current rehabilitation techniques. Curr Oral Health Rep. 2017; 4:124-130
El Wazani B, Dodd MN, Milosevic A. The signs and symptoms of tooth wear in a referred group of patients. Br Dent J. 2012; 213
Direct versus indirect restorations in the treatment of tooth wear: a report of two cases Farima Mehrabi Shihab Romeed Dental Update 2025 49:2, 133-138.
The process of tooth wear is multifactorial in aetiology, and when the progression has been considered excessive enough to be associated with aesthetic and functional concerns, appropriate assessment of each case and its treatment selection must be made, using evidence-based practice to treat such patients. Composite and ceramics are dental materials that have long been used for the restoration of patients with tooth wear. This article will explore the comparisons and rationale between direct and indirect methods and materials, using two rehabilitation cases as examples to show the impact of management of such patients. Although some cases may require a removable treatment option, this article will focus on non-removable options only.
CPD/Clinical Relevance: This article provides readers with an understanding of the selection criteria and utility values when deciding whether to restore a patient's dentition with indirect or direct materials.
Article
Tooth wear has increasingly posed challenges within the realms of primary care dentistry. Pathological tooth wear is defined as one ‘which is atypical for the age of the patient, causing pain or discomfort, functional problems, or deterioration of aesthetic appearance, which, if it progresses, may give rise to undesirable complications of increasing complexity’.1 The results of Van't Spijker's review indicate that the predicted percentage of adults presenting with severe tooth wear increased significantly from 3% at the age of 20 years to 17% at the age of 70 years.2 Increasing levels of tooth wear are directly associated with age, and as the percentage rise in the number of elderly people is estimated to increase by 16.4% by 2030,3 there will inevitably be an upsurge of such cases within the primary dental care sector.
The aetiology of tooth wear is multifactorial and comprises erosion, attrition and abrasion.4,5 Patients who present to both primary and secondary care with moderate to severe wear often require complex restorative care that may consist of full or partial mouth rehabilitation, quite often at an increased occlusal vertical dimension (OVD).6 Therefore, careful and thorough care planning and phased treatment might be both challenging and time consuming, and also at a high financial cost.
The current approach to management of tooth wear is to err on the side of minimum intervention approaches with some cases progressing to more conventional forms of treatment.1
There are several factors to consider when determining whether a treatment is suitable for primary or secondary care.7 For example, in the presence of significant parafunction, whereby a reorganization of occlusion or alteration in the occlusal vertical dimension is required due to severe tooth wear, referral should be considered.7 Within primary care every effort should be made to determine:
The diagnosis and classification of tooth wear (attrition, abrasion or erosion);
The number of affected surfaces (generalized or localized);
The severity of the tooth wear (BEWE/ACE/TWI);
The progression (speed) of tooth surface loss using intra-oral photographs, cast study models and/or CAD/CAM scanning;
Whether the tooth wear is pathological or physiological (depending on the patient's age);
Aetiological factors and the quality of the remaining tooth structures;
Presence of symptoms.
In the absence of functional and aesthetic issues, counselling and monitoring the patient may suffice as a preferred management option. Preventive advice is crucial, including medical referral, when eating disorders or reflux disease is suspected. Oral hygiene and diet advice is important, especially emphasizing a reduction in the quantity and frequency of acidic food and drinks. Appropriate tooth brushing advice should be provided and must include explaining the harmful effects of overzealous brushing and the risks of using abrasive toothpastes. Furthermore, fluoride application should be encouraged especially in those with symptoms of sensitivity. Finally, those who have bruxist habits may benefit from stress management techniques.
In all cases of tooth wear, whether the decision is made to treat or not, it is advisable to monitor the progression of the wear process. This can be done with either a series of casts or digital 3D datasets. They may help, over time, to explain the nature and severity of the condition to the patient.1 Visual aides are a good way to reinforce agreed care plans to patients, whether the decision is taken to prevent, preserve or restore.
Restorative management protocol
The European consensus statement on management guidelines1 advises the following considerations when treating tooth wear patients:
Initial restorative interventions should be postponed, and counselling and monitoring patients by using preventive measures should take precedent;
Informed consent must be gained. Ensure that the patient has been provided with all the risks and benefits of possible restorative treatment options to acquire realistic expectations of the clinical outcomes. This should be carefully documented in the clinical notes;
Restorative treatment should aim to be additive rather than subtractive to avoid further removal of tooth tissue. Minimal intervention approaches should be considered, and are favoured over invasive and extensive preparations.
Restorative treatment options include both direct and indirect techniques. Traditionally, patients who attended with severe tooth wear would be treated with interventional full and partial coverage restorations, which carry higher risk and potentially compromise the prognosis of the tooth structures and vitality.8 Although in some instances they still have a part to play in cases where direct composite restorations have failed. In such cases careful clinical judgement must be exercised.
There are, therefore, two groups of materials and techniques that can be used to restore worn dentition: direct and indirect.
This article focuses on the use of composite versus ceramic material in the rehabilitation of two tooth wear cases.
Planning and selection criteria
Careful pre-operative assessment is essential for restoring the worn dentition regardless of the technique or material used. A thorough clinical examination and history should be taken to determine the pattern and severity of the tooth wear in order for an accurate diagnosis to be made. Preventive measures must be undertaken, and any active disease should be controlled prior to commencement of treatment.9
There are several factors that should be considered when deciding whether treatment is appropriate.9 These factors include:
Aetiology of tooth wear;
Quantity and quality of tooth tissue remaining;
Occlusal relationship and loss of OVD.
If tooth wear appears to be minimal and confined to single surfaces, for example, palatal, as in many intrinsic erosion cases, then composite is an appropriate material of choice and can be used with a high degree of predictability.9 Where there is sufficient enamel remaining along the periphery, then the likelihood of improved bond strength will ensue.9
Treatment techniques
With regard to preparation of the worn dentition for restoration, there is great advantage in carrying out minimally invasive procedures first. This way, the rehabilitation of the teeth focuses more on the preservation of an already compromised tooth structure, and therefore, should that then fail, there is opportunity to re-treat with more invasive techniques.10
Composite
Using direct composite as a restorative material in the provision of treatment for tooth wear has a number of advantages over the use of indirect materials:9
Minimally invasive additive procedure;
Restoration of aesthetics and function;
Chairside control over final treatment outcome;
Reduced cost and treatment time;
Fewer perceived complications by patient in comparison to crown-lengthening surgery and indirect laboratory work, such as crowns.
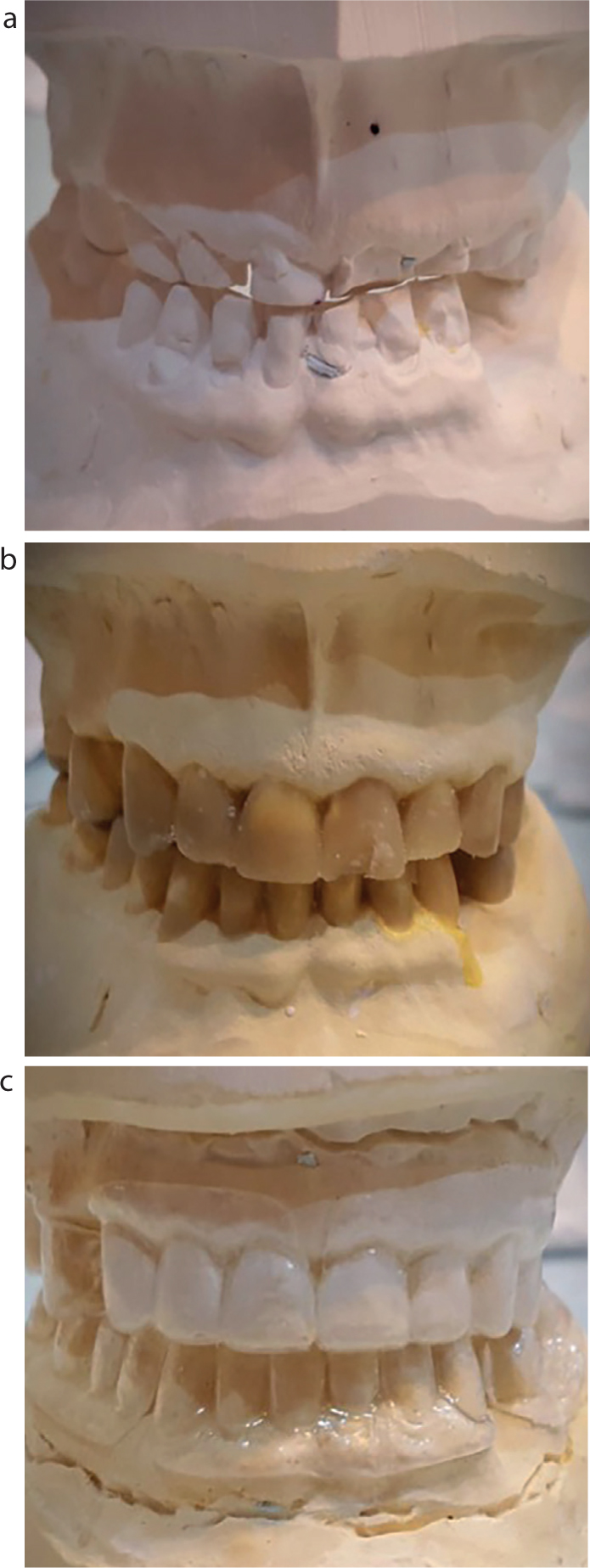
There is a variety of direct composite techniques that can be used for rehabilitation. In all cases of severe tooth wear, articulated study casts must be mounted in the retruded axis position, in order to assess the proposed increase in occlusal vertical dimension.9 Diagnostic wax-ups on articulated study casts are a useful aid for allowing the clinician to make more accurate assessments of the final outcome (Figure 1). Here, we will discuss two techniques for the rehabilitation of tooth wear specifically for anterior teeth: free-hand and matrix techniques.
Figure 1.
(a) Articulated study casts depicting evidence of tooth wear. (b) Wax-up of upper and lower teeth carried out. (c) Vacuum-formed stent created from the wax-up for use during the chairside mock-up appointment for consent.
Freehand techniques
In the majority of cases, patients present with tooth wear that has been localized to the anterior segment. A useful guide is to add composite onto the cingulum region of both upper canine teeth while manipulating the mandible into the retruded axis position, until the desired anterior space is achieved. Once cured, the contact should provide the new occlusal vertical dimension.9
From here on, the teeth can be individually built up taking into consideration the average width:height ratio and rebuilding teeth to their original contours. The patient should be warned at the consent stage that the posterior teeth will be out of occlusion, and it may be months before posterior occlusal contacts are re-established (Dahl concept).
Matrix technique
Alternatively, a silicone matrix can be used to assist in the build-up of the teeth. Impressions, an inter-occlusal record, as well as a face bow record should be taken to allow study casts to be mounted onto a semi-adjustable articulator in the retruded axis position. The clinician and technician work together to establish the required increase in vertical dimension and a diagnostic wax-up is carried out.9 It is important to ensure that cingulum occlusal stops are produced to ensure axial loading of restored teeth. A palatal silicone matrix is then made that should extend beyond the incisal edges (Figure 2).9 A thin increment (0.5–1 mm) of composite can then be placed on the matrix to build up the palatal-incisal aspect of the tooth. This will ensure that the palatal contour and incisal length are determined. Once this has been carried out the matrix can be removed, and the composite further layered to build up the worn teeth.9
Figure 2.
(a) Initial frontal view of upper and lower teeth with tooth wear evident. (b) Silicone putty matrix in place against the palatal aspect of the maxillary teeth. (c) Direct composite build-up of the UR1 palatal aspect using the silicone putty matrix. (d) UR1 and UL1 midway through composite build-up with the putty matrix in place. (e) Frontal view immediately after initial placement of the composite. (f) Frontal view without retractors in place immediately after direct composite build-up prior to polishing being undertaken.
As it currently stands, the level of evidence for long-term survival of composite restorations is relatively limited. However, results from two retrospective studies and three prospective studies have shown that composites are a favourable management modality for the treatment of tooth wear in the short to medium term, with survival rates over 90% at 2.5 years, and over 50% at 5 years.11
A further study supporting the use of composite as an appropriate restorative material for the severely worn dentition demonstrated a failure rate of 5.4% over 8 years in 164 patients for whom 1010 restorations were placed. Failure was shown to be greater in older patients who lacked posterior support, those with a Class 3 or edge-to-edge incisal relationship and more often in the lower arch (9.6%) when compared to the upper arch (6%).12
Composite restorations are cost-effective alternatives to indirect ceramic restorations for the treatment of tooth wear cases. Despite having inferior long-term aesthetics in comparison to ceramics, indirect composite resin restorations have been shown to have higher fatigue resistance and compressive strength compared to ceramics under conditions of higher occlusal load.13 They offer a minimally invasive approach, which can be easily maintained through either repair or replacement, at a supplementary cost to the patient. They present a viable treatment option for the short-to medium-term rehabilitation of cases.11 There is evidence to support an increase in patient's satisfaction and quality of life after treatment.14,15
Cermic
When direct techniques are not suitable, in cases where they have either failed or more predictable treatment is required, it may be suitable to consider indirect techniques, especially in restoring severely worn dentitions.
One technique that can be undertaken is the minimally invasive prosthetic procedure (MIPP), which comprises:16
Increasing the occlusal vertical dimension;
Minimally invasive tooth preparations;
Posterior restorations made from monolithic zirconia or lithium disilicate;
Adhesive bonding of restorations.
An anterior intra-oral trial prosthesis based on a diagnostic wax-up (Figure 1) is first undertaken to establish the amount of increase in the OVD necessary to accomplish both aesthetic and functional goals. Preparation is then carried out: for ceramic (monolithic zirconia or lithium disilicate) because this can be as thin as 0.8–1 mm, which would result in minimal reductions of tooth tissue. However, most of the tooth preparation will be axial wall reductions, and the OVD is usually increased to create inter-occlusal spaces for the indirect posterior restorations.
A second approach for generalized tooth wear is a three-step technique:17,18
Diagnostic casts are articulated and a diagnostic wax-up (Figure 1) is carried out at an increased OVD with the posterior occlusal plane evaluated with a mock-up;
The posterior teeth are then temporarily restored using direct composite restorations using silicone matrices constructed from the diagnostic wax-up. This will create an anterior open bite;
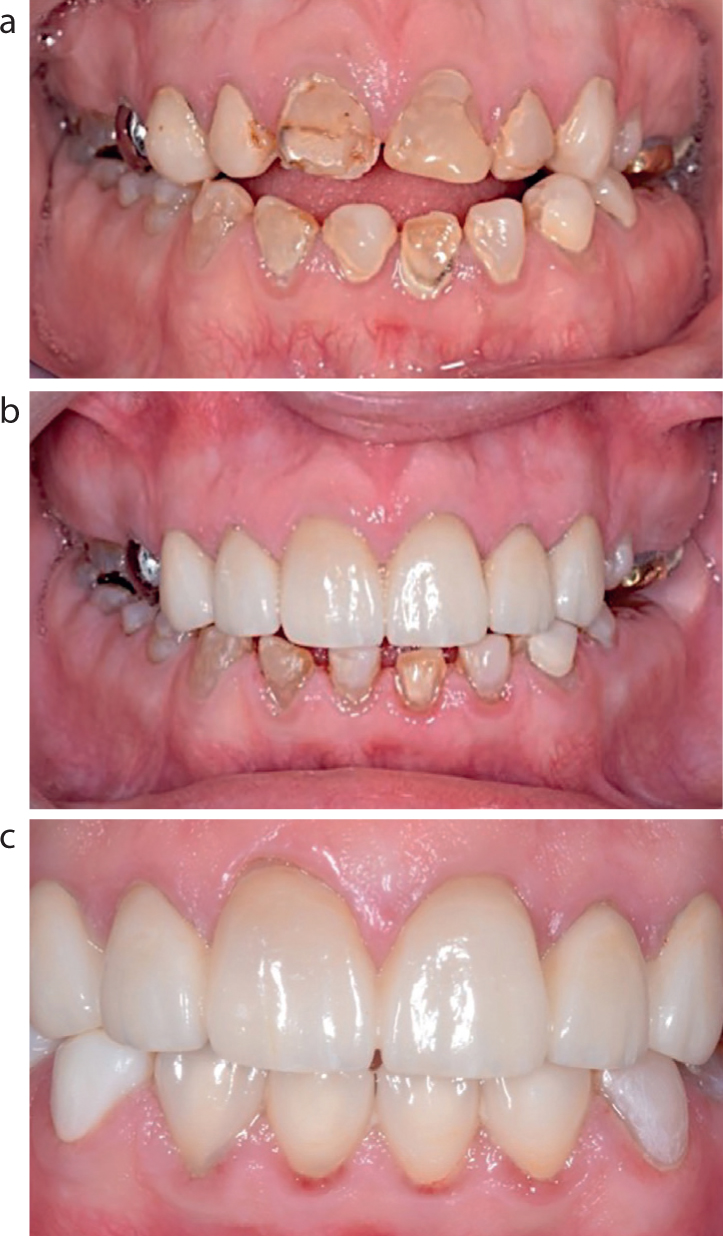
Restoration of anterior guidance can then commence with direct or indirect palatal composite resin veneers. The posterior interim composite resin restorations can then be replaced with indirect composite resin onlays or, alternatively, monolithic zirconia or lithium disilicate or CAD/CAM ceramic–polymer hybrid onlays (Figure 3).
Figure 3.
(a) Tooth wear as a result of amelogenesis. (b) Six lithium disilicate crowns in place. (c) Mandibular teeth with six composite restorations in place, and maxillary teeth restored with six lithium disilicate crowns. Image taken immediately after ultrasonic scaling with residual redness still present.
According to the Radboud tooth wear project, indirect restorations can play an additive role in the rehabilitation of severe tooth wear cases.19 This is known as the ‘hybrid technique’ and ensues when indirect material is used on selected teeth only, for example in Figure 3, in the upper anterior 3-3 segment, and the remaining teeth are restored with direct composite restorations.19
Presently, there have been no clear influences noted on the effect of preparation thickness (2.1–3.2-mm floor depth reduction, and 1.6–2.6-mm working cusp reduction) and taper on the likelihood of failure or fracture of feldspathic onlays in posterior molar teeth.20 A study carried out by van Dijken and Hasselrot demonstrated that teeth that had been endodontically treated with no retention (no post or core) had the greatest failure rate, while teeth with preparations that incorporated retentive features within the preparation had a reduced chance of failure.21
When considering the fabrication method and materials, there have been no studies to date that have suggested that one performs better over another, and the methods used do not appear to affect performance. In comparison to traditional cast, pressed, milled and sintered ceramics, chairside CAD/CAM feldspathic and polymer infiltrated ceramics have shown a similar clinical outcome.22 With regard to comparing ceramic with other materials, Kaytan et al demonstrated that pressed-leucite-reinforced ceramic showed a superior colour match to composite resin onlays over a 2-year period.23
With patients who demonstrate bruxist habits, it is important to take into consideration the long-term effects this may have on the restorations placed. Felden et al showed that parafunctional habits had a negative effect on the longevity of indirect restorations and that there is in fact an overall higher failure rate of restorations displayed in such patients.24
Longevity of restorations
It is important that during the consenting stage a comprehensive discussion is undertaken with the patient in order to manage their expectations. Carrying out any restorative work on teeth that have already been compromised by extensive wear will carry some risks, limitations and, moreover, potential clinical, as well as financial, implications with regard to possible failure. The patient needs to be motivated and aware of all clinical consequences prior to the start of treatment.25
In order to maintain such restorations, it is important to protect them. Occlusal removable appliances (Michigan or Tanner splints) have been recommended for the protection of these definitive restorations from parafunctional forces in patients with bruxist tendencies or who have other parafunctional habits.16 This is because they act to reduce direct occlusal contact between the opposing restored teeth and provide mutually protected occlusion (the magnitude of bite forces is significantly higher in such patients), therefore provision of such an appliance is beneficial for all rehabilitated patients with a history of tooth wear.16
It is essential to examine the vitality of severely worn teeth prior to the direct or indirect rehabilitation of worn dentition to rule out the need for endodontic treatments. It was indicated that the proportion of subjects with undiagnosed apical pathology might be up to 13% on worn teeth.27
Conclusion
First and foremost, accurate diagnosis and prevention is key when it comes to the management of tooth wear. From there on, minimal intervention procedures should be undertaken first including provision with direct composite restorations in the short to medium term to establish the patient's new OVD, to act as an aesthetic guide and as a maintainable way of making adjustments if necessary. Rehabilitation with indirect ceramic restorations can then be considered to replace composites for long-term provision, to increase aesthetic outcomes and durability.