Ng YL, Mann V, Gulabivala K A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: peri-apical health. Int Endod J. 2011; 44:583-609 https://doi.org/10.1111/j.1365-2591.2011.01872.x
Nabil S, Samman N Incidence and prevention of osteoradionecrosis after dental extraction in irradiated patients: a systematic review. Int J Oral Maxillofac Surg. 2011; 40:229-243 https://doi.org/10.1016/j.ijom.2010.10.005
Kanatas AN, Rogers SN, Martin MV A practical guide for patients undergoing exodontia following radiotherapy to the oral cavity. Dent Update. 2002; 29:498-503 https://doi.org/10.12968/denu.2002.29.10.498
Eliyas S, Porter R, Briggs P, Patel RR Effects of radiotherapy to the jaws. I: The scale of the problem. Eur J Prosthodont Restor Dent. 2013; 21:161-169
Yamada RS, Armas A, Goldman M, Lin PS A scanning electron microscopic comparison of a high volume final flush with several irrigating solutions: part 3. J Endod. 1983; 9:137-142 https://doi.org/10.1016/S0099-2399(83)80032-6
Lea SC, Felver B, Landini G, Walmsley AD Ultrasonic scaler oscillations and tooth-surface defects. J Dent Res. 2009; 88:229-234 https://doi.org/10.1177/0022034508330267
Boutsioukis C, Lambrianidis T, Kastrinakis E, Bekiaroglou P Measurement of pressure and flow rates during irrigation of a root canal ex vivo with three endodontic needles. Int Endod J. 2007; 40:504-513 https://doi.org/10.1111/j.1365-2591.2007.01244.x
Tran XV, Gorin C, Willig C Effect of a calcium-silicate-based restorative cement on pulp repair. J Dent Res. 2012; 91:1166-1171 https://doi.org/10.1177/0022034512460833
Pandey P, Aggarwal H, Tikku AP Comparative evaluation of sealing ability of gutta percha and resilon as root canal filling materials – a systematic review. J Oral Biol Craniofac Res. 2020; 10:220-226 https://doi.org/10.1016/j.jobcr.2019.12.004
Mekhdieva E, Del Fabbro M, Alovisi M Postoperative pain following root canal filling with bioceramic vs. traditional filling techniques: a systematic review and meta-analysis of randomized controlled trials. J Clin Med. 2021; 10 https://doi.org/10.3390/jcm10194509
King PA, Foster LV, Yates RJ Survival characteristics of 771 resin-retained bridges provided at a UK dental teaching hospital. Br Dent J. 2015; 218:423-428 https://doi.org/10.1038/sj.bdj.2015.250
Neme AL, Evans DB, Maxson BB Evaluation of dental adhesive systems with amalgam and resin composite restorations: comparison of microleakage and bond strength results. Oper Dent. 2000; 25:512-519
This case report presents the endodontic and prosthodontic management of a rhinectomy patient who sustained iatrogenic damage to the apices of her anterior maxillary teeth during surgical resection of a nasal tumour. We discuss the issues with surgical and prosthodontic management of oncology patients who have undergone surgery and radiotherapy, in addition to the endodontic techniques employed to ensure success of treatment whilst noting important prognostic indicators. The case highlights the importance of routine radiographic review and post-surgical tooth assessment of patients who sustain trauma or have surgery in the midface, since clinicians may only radiograph anterior teeth when they are symptomatic and/or present with trauma.
CPD/Clinical Relevance: Close monitoring of traumatized teeth or teeth in close proximity to surgical sites should be provided.
Article
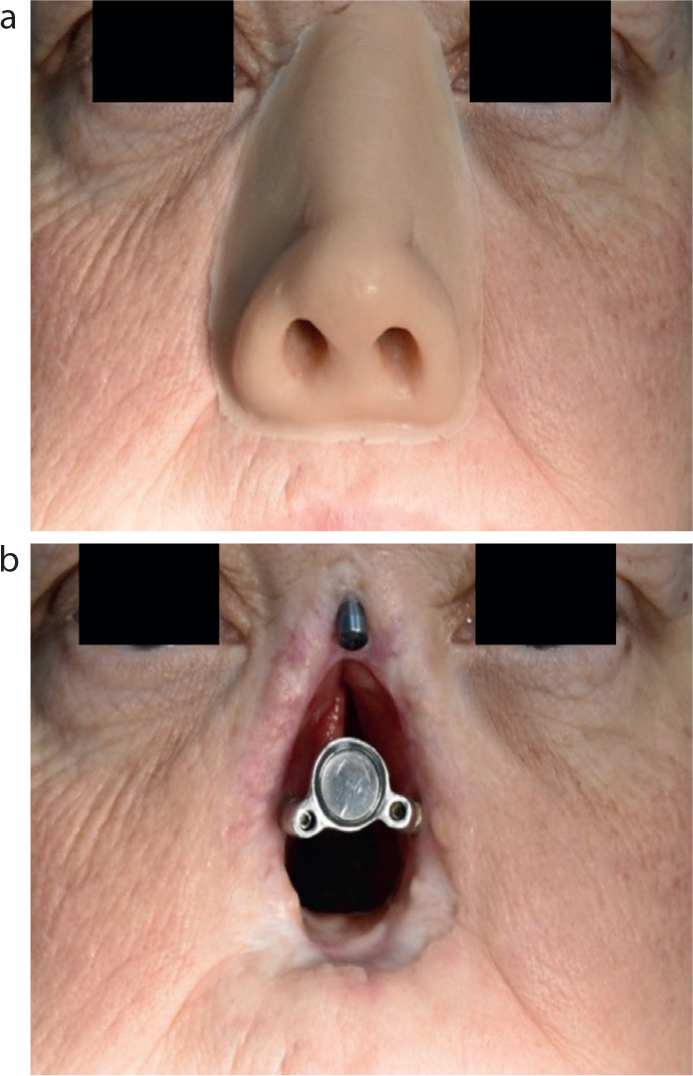
The present case report discusses a 46-year-old female who presented to the restorative department at Liverpool University Dental Hospital in July 2019, following referral from oral and maxillofacial surgery colleagues, for the management of her maxillary anterior teeth. Her complaints were of discomfort related to UR3. There was no history of swelling or infection related to the teeth. She had a history of squamous cell carcinoma of the nasal cavity, which was treated with total rhinectomy, primary horizontal zygomatic implant placement and post-operative radiotherapy, completed in July 2019. She had a zygomatic implant-retained nasal prosthesis that was functioning well (Figures 1 and 2). Her medical history was otherwise unremarkable. The patient experienced xerostomia as a result of radiotherapy to the head and neck region.
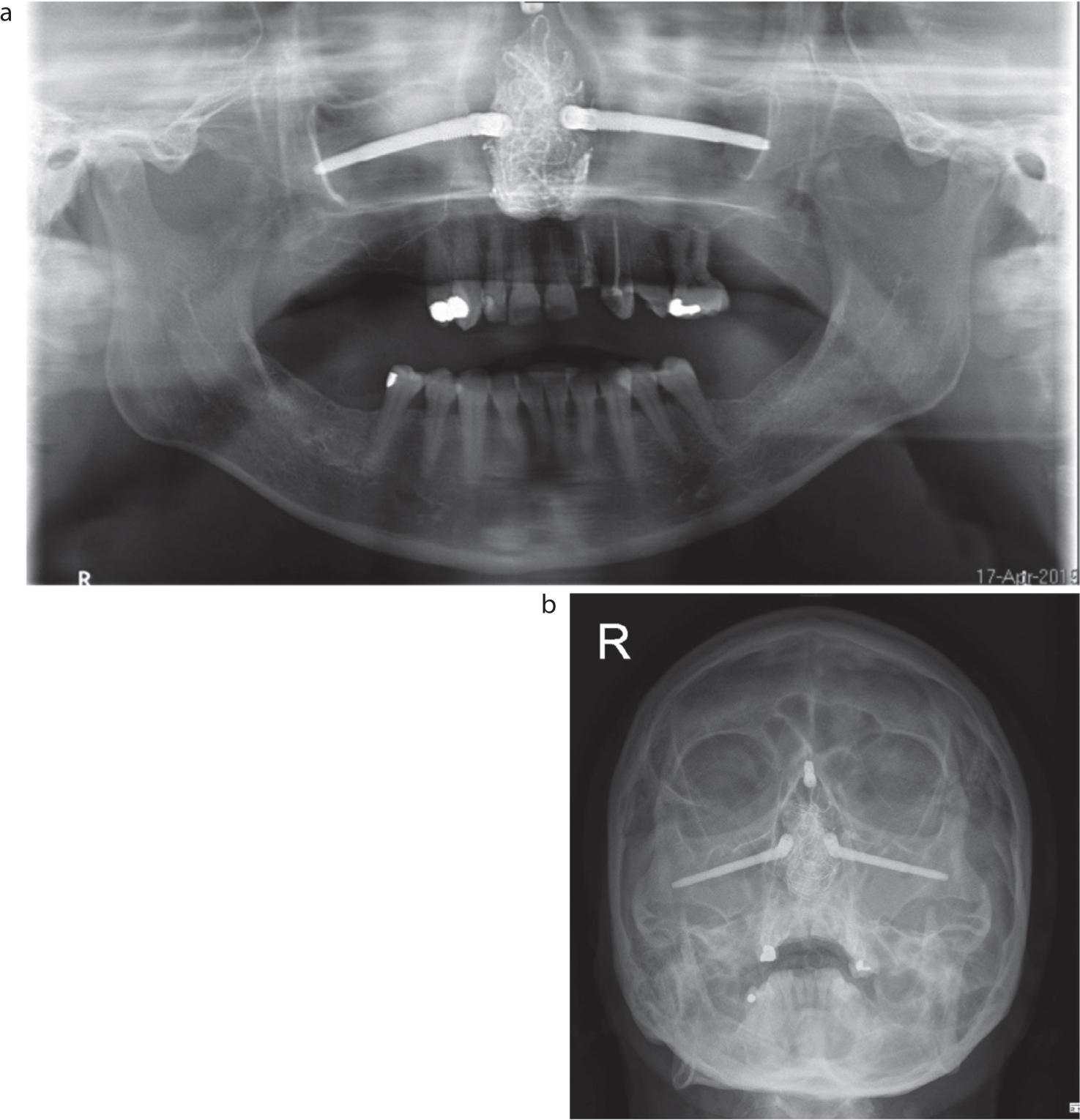
Figure 1. (a) Magnet-retained nasal prosthesis in situ and (b) removed. Two horizontal zygomatic implants at lateral margins of defect and a dental implant at superior margin.Figure 2. (a) Immediate post-operative rhinectomy dental panoramic tomogram (DPT) and (b) PA facial bone radiographs demonstrating the location of the zygomatic and dental implants. These radiographs were taken as standard to assess zygomatic implant position and proximity of local anatomy.
Intra-oral clinical examination revealed a partially dentate individual with loss of posterior support. The patient demonstrated periodontal disease resistance and good clinical attachment levels. No teeth were found to be tender to percussion or mobile beyond physiological tooth mobility; however, there was slight fremitus found associated with UR1, UR2 and UL1 and the patient had a feeling of numbness (suggesting the area ‘feels dead’) to palpation over the anterior gingivae. UL2 was fractured coronally and was found to be unrestorable.
Special investigations
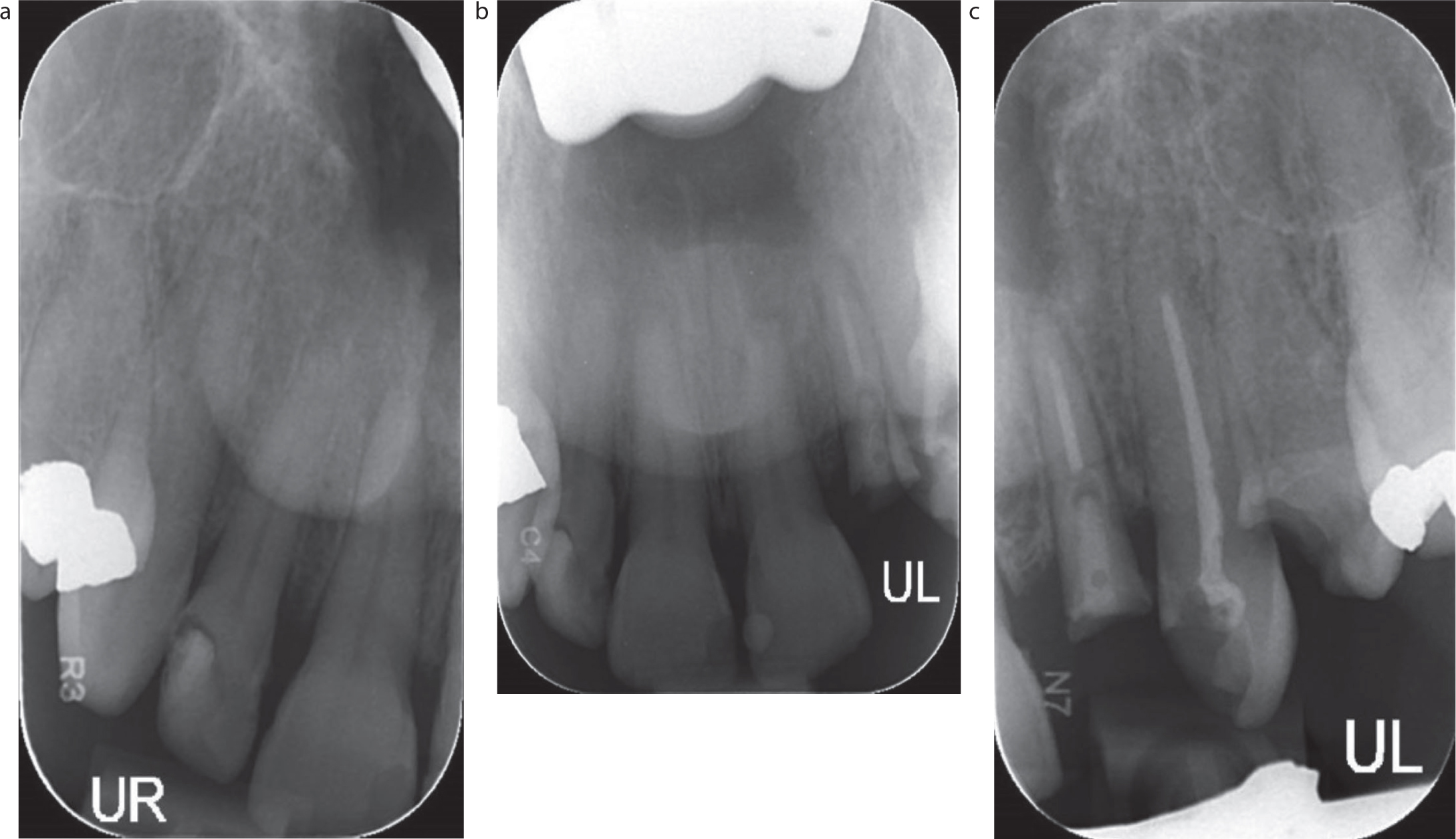
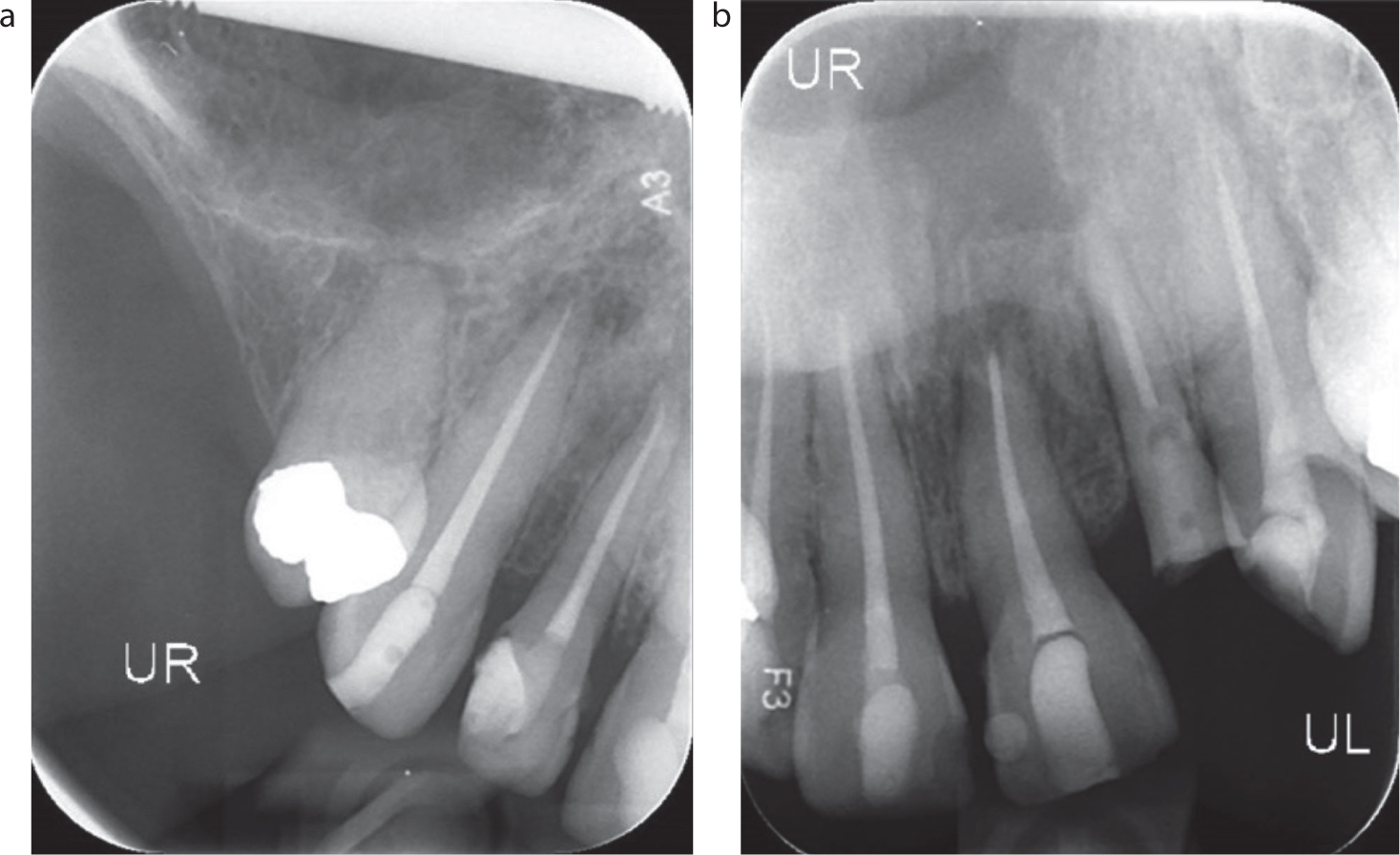
All teeth, UR3–UL4 were non-responsive to cold sensibility testing. Peri-apical radiological examination (Figure 3) revealed:
UR1, UL4 caries;
UR2 recurrent caries and failing restoration;
UL2, UL3 pre-existing endodontic treatment;
UL2 fractured to root level with fibre post in situ;
UL1 root tip blunting suggestive of either external inflammatory root resorption or iatrogenic damage;
UL1–UL4, UR1, 2 apical radiolucency and periodontal ligament widening.
Figure 3. Pre-operative peri-apical radiographs, showing blunting of the root apices of UR1 and UL1, and apical pathology related to UR2, UR3, UL2 and UL3. Existing root canal obturations UL3 and UL2 (with fractured fibre post in situ).
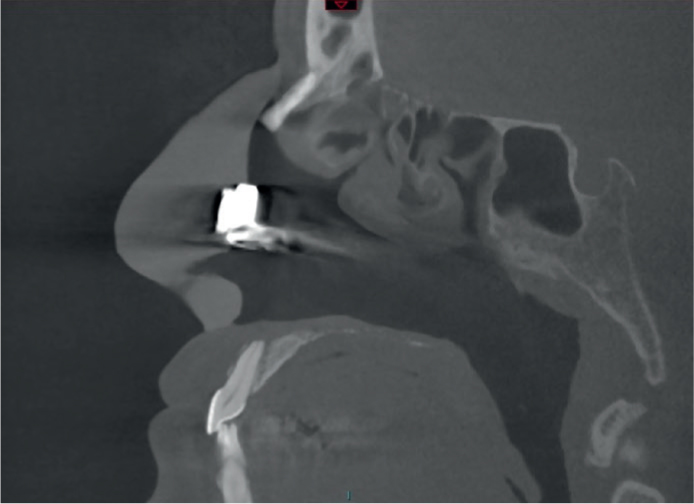
Further investigation of the maxillary anterior teeth was indicated to explain the clinical findings and suspected iatrogenic damage to the root surfaces. Cone beam computed tomography imaging of the maxilla revealed peri-apical pathology related to UR1–UR3 and UL1–UL4, and lack of adjacent floor of nose structure associated with UR1 and UL1. Figure 4 shows a sagittal slice of UL1 demonstrating horizontal iatrogenic damage to the root apex in alignment with the horizontal osteotomy cut of the nasal floor. This appearance was also seen on UR1.
Figure 4. Sagittal slice of CBCT demonstrating apical iatrogenic damage to UL1 root, in association with the inferior margin of the nasal defect.
Diagnosis
Retained unrestorable UL2 root;
Caries UR1, UR2, UL4;
Symptomatic apical periodontitis UR3;
Asymptomatic apical periodontitis UR1–UR2, UL1–UL4, associated with iatrogenic damage from nasal resection.
Prognosis
UL2 was deemed unrestorable and was planned for extraction. However, owing of the patient's radiation history to the anterior maxilla, there was significant risk of osteoradionecrosis following extraction of this tooth. UL3 required endodontic re-treatment and for this reason, had a reduced prognosis compared with the remaining anterior maxillary teeth, which required primary endodontic treatment.1
Issues identified
This case presented many challenges at the patient and clinical level. First, the patient's history of radiotherapy to the anterior maxilla necessitated retention of the teeth rather than extraction, where possible, except where teeth were unrestorable and symptomatic. Extractions were required to be performed as atraumatically as possible, along with antimicrobial prophylaxis.2,3 In addition, it was prudent to provide fixed rather than removable prostheses to replace missing teeth owing to the patient's radiation-induced xerostomia.
Since the teeth had become non-vital and infected because of the iatrogenic damage during rhinectomy surgery, the management of the resultant open apices required careful planning with the use of bioceramic materials during endodontic treatment to predictably achieve an apical seal and allow biological healing.
Treatment provided
The treatment was provided in the sequence shown Table 1.
Table 1. Phases of treatment provided for the rhinectomy patient. See Figures 5–8 for radiographs of the completed endodontic treatments and the restorations.
Treatment phase
Treatment provided
Details
1
UL3 root canal re-treatment
Traditional endodontic access, scouting and glide path acquisition. ProTaper Next rotary instrumentation preparation. Irrigation throughout instrumentation with sodium hypochlorite 1% and EDTA 17% penultimate irrigant rinse. Final irrigant rinse with sodium hypochlorite 1%, using passive sonic activation (EndoActivator, Dentsply Sirona) for 1 minute. Thermal vertical compaction of gutta percha with bioceramic sealer (TotalFill BC Sealer, FKG Dentaire, Switzerland) and warm gutta percha backfill. Treatment provided over two to three visits with non-setting 35% calcium hydroxide interappointment medicament (UltraCal XS, Ultradent, UT, USA)
Inability to gain four-point clamp contact and not possible to clamp UL6
6
Extraction UL2
3 g amoxicillin stat pre-operative prophylactic cover. The extraction was noted to be atraumatic and normal spontaneous bleeding and haemostasis were found. The sockets were allowed to heal by secondary intention without packing and suturing
7
Endodontic treatment UR3
ProTaper Gold, thermal vertical compaction of gutta percha with bioceramic sealer; over two visits
8
Emergency extraction UL4
Following evidence of successful healing UL2 socket
9
Resin-bonded bridge provision UR2, 3, UL5, 6
Constructed of non-precious alloy cobalt chrome framework and feldspathic porcelain veneering ceramic. Pre-cementation protocol included aluminium oxide 50 micron sandblast and steam cleaning. Cementation with Panavia F2.0 (Kuraray Medical Inc, Tokyo, Japan) system, with final light cure of margins
Following completion of treatment, the patient was reviewed clinically and radiographically, and was asymptomatic at 1 year, having been unable to attend her scheduled appointments at 3 and 6 months for clinical post-operative review. Following this, she was seen in our maxillofacial prosthodontics clinic for construction of a new nasal prosthesis.
The case report presented demonstrates the successful restorative management of surgically induced iatrogenic damage to multiple maxillary anterior teeth following a rhinectomy procedure, preserving the integrity of a number of restorable and functional teeth.
In the resection of mid-facial tumours, surgeons are guided to make their cuts by the extent of the tumours, which are guided by clinical presentation and by imaging. In order to gain clear margins and improve disease prognosis, this sometimes is at the expense of other anatomical structures, including teeth. The patient was fortunate to not experience too many adverse effects from the iatrogenic damage to the teeth, and was able to undergo a series of endodontic and extraction procedures to limit the risk of dental infection.
Radiotherapy is very effective as an adjuvant treatment in stage 3–4 disease of the head and neck, where there are involved margins (less than 1 mm from the surgical margin) and/or when one or more lymph nodes are involved because of metastatic spread or display extracapsular spread. The resultant effects of radiotherapy include mucositis, loss of taste, xerostomia, infection, trismus, muscle fibrosis and the risk of osteoradionecrosis (ORN). The majority of side effects often improve within 6–8 months after treatment; however, patients may report persistent symptoms of dry mouth and ORN for much longer. Extraction of teeth in the fields of previous radiotherapy carry a risk of ORN, particularly if the individual has received over 60 Gy of total radiation.2 The risk of ORN is higher in the posterior mandible and much lower in the maxilla, but it remains a profound complication. ORN can occur at any time following radiotherapy but 70–94% of cases occur in the first few years following completion of treatment.4
A systematic review has estimated the total incidence of ORN after tooth extraction in irradiated patients to be 7%, yet the pooled data incidence of ORN in the mandible was 3% compared to 1% in the maxilla.2 When extractions were performed in conjunction with antimicrobials, the total incidence was reduced to 6%. Specific clinical guidelines from the Royal College of Surgeons of England and the British Society for Disability and Oral Health state that although there is no conclusive evidence regarding pre-extraction antibiotic prophylaxis to prevent ORN, the general consensus would recommend antibiotic prophylaxis and continued antibiotics until completion of healing.5 Amoxicillin (or metronidazole in those allergic to penicillin) is generally the drug of choice for these patients. Any extractions completed should be performed with minimal trauma and, where possible, soft tissue primary closure obtained.2
It is necessary to evaluate the prognostic indicators for success before embarking on any endodontic therapy, regardless of the medical need to retain rather than extract teeth. This allows the patient to be consented appropriately by informing them of the anticipated outcomes of treatment. For example, a tooth requiring endodontic re-treatment has an overall lower success rate than a tooth requiring primary endodontic treatment (85% versus 76.7%) and the patient should understand this before treatment.1 The important prognostic indicators include presence and size of peri-apical lesions, sinus tracts, patency of root canal system, apical extent of the root canal preparation, root filling extrusion and adequacy of coronal restorations.1 With this knowledge, the clinician can adopt additional procedural techniques to optimise the outcomes. It is known that the use of EDTA or citric acid in endodontic re-treatments improves the overall tooth prognosis and should be used routinely in root canal treatment for removal of the smear layer.1
In the present case, the authors adopted different rotary instruments to root canal treat multiple anterior teeth. A knowledge of the type of nickel–titanium technology can help the clinician to select of the most appropriate system, in addition to selecting a system based on handling characteristics and clinician preference. Overall, multi-file systems can potentially encourage the clinician to have more contact time and exchange occasions of the irrigant in the root canal system while progressively instrumenting the canal system and moving between files, versus single file systems, which can reduce treatment time overall. Multi-file systems can therefore be advantageous for the preparation of canals with persistent or high-grade infection, while single file systems are advantageous when one has already spent a significant amount of time establishing a glide path, and once achieved, there is a requirement for the remaining canal preparation to be as fast as possible.
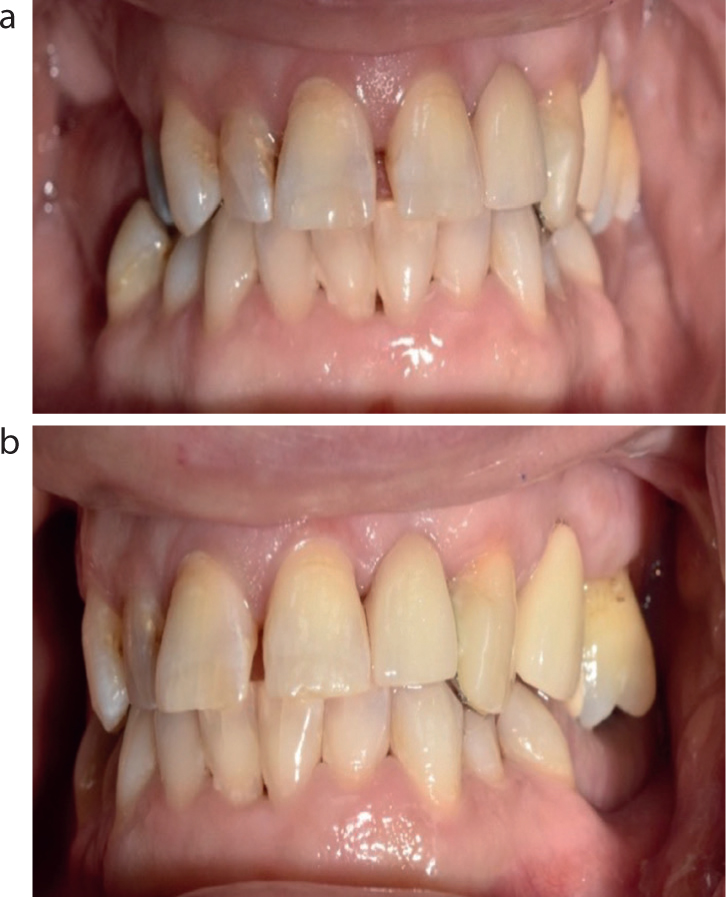
Figure 6. Mid treatment photographs demonstrating healed extraction sockets in UL2 and UL4 position.
Gold-coloured nickel-titanium files (such as ProTaper Gold, Dentsply Sirona, NC, USA) are known for being exceptionally flexible and therefore, good for curved canals. The martensitic wire is produced by being cut in to its final shape before heat treatment to gain its flexibility. In contrast, the austensitic M Wire found in files such as ProTaper Next (Dentsply Sirona), are cut in to shape after heat treatment and are stiffer than the gold files, but are highly resistant to cyclic fatigue. This case allowed the use of stiffer files, which have greater cutting effectiveness and improved torque resistance, in the straight canals for anterior teeth, although equally in this case, gold martensitic files could be used, but this is down to clinician preference.
A protocol of sodium hypochlorite irrigation throughout treatment of suppurating canals, followed by a final disinfection with 17% EDTA soak for 2 minutes and 1% sodium hypochlorite activated rinse was employed.6 This protocol has been shown to be effective in removal of the smear layer prior to obturation of the root canal system.7 The sodium hypochlorite irrigant was passively activated using sonic activation using the EndoActivator (Dentsply Sirona) with soft polymer tips. This assists in the chemomechanical debridement of root canals by enhancing tissue dissolution and removal of biofilm through creating vibrations in the irrigant, similar to ultrasonics, but at a lower frequency. Conventional irrigation with sodium hypochlorite in a side-vented syringe will cause laminar flow and remove the planktonic bacteria, but not necessarily the biofilm from the dentine surface. Sonic activation is theoretically safer to dentine wall structure than ultrasonic.8 Despite the latter being more powerful, it suffers from issues related to dampening of energy when in contact with dentine walls, and both are arguably equally effective.9
Figure 7. Resin-bonded bridges to replace UL2 and UL5. Locating lugs present on UL3 to allow seating of restoration to abutment tooth, prior to being removed off once cemented.Figure 8. Post-operative photograph of the completed restorations to replace UL2 and UL5.
All canals were obturated with warm vertical gutta percha compaction and the use of a bioceramic sealer (TotalFill BC Sealer, Schottlander, UK). Bioceramic sealers are tricalcium/dicalcium silicate-based, which not only provides a hermetic seal to the root canal obturation, but also aid in biological healing thanks to their antibacterial (pH12) and reparative and regenerative properties.10 The setting of TotalFill BC Sealer is triggered by the moisture present in the dentinal tubules, forming hydroxyapatite and a chemical adhesion between the dentine and the cement. The patient reported spontaneous return of sensation in the subnasal region following endodontic therapy, and while to the present authors' knowledge, there is no evidence in the literature of this being the case with bioceramic sealer use, the induction of apical healing in the area of previous surgery may have contributed to this effect. Although it would not have been wrong to use an epoxy resin-based sealer,11 in this case, the authors aimed to generate peri-apical healing in light of the iatrogenic trauma to the region during surgical tumour resection, which bioceramic sealers have advantageous biological responses to in contact with peri-apical tissues.
Mekhdieva et al have compared the outcome of patient-reported post-operative pain following the use of resin-based sealers versus bioceramic sealers in a systematic review and meta-analysis of randomized controlled trials.12 They found that, while no individual study reported a significant difference between the two types of sealer, when combining the outcomes in a meta-analysis, there was less post-operative pain at 24 and 48 hours post-operatively following the use of bioceramic sealer. Additionally, the use of post-operative analgesia was less in the bioceramic sealer group for the first 24 hours; however, this result did not reach statistical significance. Therefore, the use of bioceramic sealers in teeth with high risk of extrusion, in this case due to root-end damage, may not be as problematic as once thought in terms of patient-reported outcomes, and their use is superior in terms of biocompatibility.
For patients who have had significant radiotherapy to the head and neck and display signs of radiation-induced xerostomia, opting for fixed prostheses to replace missing teeth is preferred over removable prostheses as the latter can inadvertently traumatize dry, fragile mucosa. This would require bridgework to be cantilevered from teeth with reduced prognosis following root canal treatment and therefore, careful planning of the prostheses was required. Such a flexible approach in this specific situation is supported by studies such as Sorenson and Martinoff.13 Additionally, this patient required short appointments due to the difficulties with maintaining an open mouth because of the surgical and radiation scarring.
Alternatively, implant replacement of the missing teeth was an option, but is not without significant risk of osteoradionecrosis in the field of previous radiotherapy. The strategic abutment teeth (maxillary left first molar and maxillary left canine) were in situ and of good condition for the use as bridge abutments, despite the canine having undergone root canal treatment. The old amalgam intracoronal restorations were replaced for new composite immediately prior to bridge provision, to ensure optimal bonding of the indirect restoration to the new direct resin. King et al found that restoration replacement prior to resin-bonded bridge provision facilitated a three-fold risk reduction of failure compared to resin-bonded bridge placement over old restorations.14 This is further explained by existing composite restorations known to absorb moisture over time and therefore have poorer bonding capability. In addition, resin-based adhesive cements are known to bond better to composite than amalgam.15
To aid location of resin-bonded bridges to anterior teeth, the authors prefer the use of incorporating ‘locating lugs’ on the incisal edge of the metal retainer (Figure 7). These can be simply removed at the fit appointment following cementation. Other options for enabling accurate fit of the retainer to the abutment tooth include pattern resin jigs, which should be designed to leave the entire restoration margin free for excess cement clear-up. The use of locating lugs is not necessary on posterior teeth, especially when an onlay-type retainer design is used owing to a single obvious insertion position. The onlay retainer is beneficial for use when there is no opposing tooth, or when interocclusal space allows. It benefits from maximizing the bonding surface area of enamel.
Conclusions
The present case report highlights the need for routine radiographic assessment of maxillary anterior teeth following trauma and midfacial surgery, in order to diagnose and treat any asymptomatic pathology. This should be provided in addition to the routine bitewing or similar radiographs taken for the investigation of periodontal disease and caries. A question is now raised. Should we be asking our surgical colleagues to consent the patient for loss of dental vitality as part of the surgical resection? While pre-cancer treatment dental assessments are routinely provided in the UK, should patients also be reviewed by a dental team in the early post-operative phase? It is the authors' view that when teeth are retained in close proximity to the surgical site, a dentist should review the teeth clinically and radiographically as soon as feasibly possible after surgery when the patient is fit enough and ideally prior to radiotherapy. Should endodontic treatment be required, this should ideally be completed before radiotherapy, but not to delay the start of radiation treatment.
The patient, who underwent a rhinectomy procedure and sustained iatrogenic damage to the apices of all maxillary anterior teeth, was successfully treated with endodontic treatment, extractions of unrestorable teeth and replacement with resin-bonded bridges. We have discussed the strategies for endodontic success in similar cases, the surgical management of hopeless prognosis teeth in the irradiated patient, and prosthodontic management of spaces in head and neck cancer patients.