Mannocci F, Machmouridou E, Watson TF, Sauro S, Sherriff M, Pilecki P, Pitt Ford TP Microtensile bond strength of resin-post interfaces created with interpenetrating polymer network posts or cross-linked posts. Med Oral Patol Oral Cir Bucal. 2008; 13:(11)E745-E752
Mosedale RF Current indications and methods of periodontal splinting. Dent Update. 2007; 168-180
Sewon LA, Ampula L, Vallittu K Rehabilitation of a periodontal patient with rapidly progressing marginal alveolar bone loss: 1 year follow-up. J Clin Periodontol. 2000; 27:615-619
Pollack RP Non-crown and bridge stabilization of severely mobile, periodontally involved teeth. A 25-year perspective. Dent Clin North Am. 1999; 43:(1)77-103
Martelli H, Pellizzer EP, Rosa BT, Lopes MB, Gonini A Fracture resistance of structurally compromised root filled bovine teeth restored with accessory glass fibre posts. Int Endodont. 2008; 41:685-692
Sfondrini M-F, Fraticelli D, Castellazzi L, Scribante A, Gandini P Clinical evaluation of bond failures and survival between mandibular canine-to-canine retainers made of flexible spiral wire and fiber-reinforced composite. J Clin Exp Dent. 2014; 6:(2)e145-149
Özcan M, Valandro LF, Amaral R, Leite F, Bottino MA Bond strength durability of a resin composite on a reinforced ceramic using various repair systems. Dent Mats. 2009; 25:1477-1483
Özcan M, Breuklander MH, Vallittu PK The effect of box preparation on the strength of glass fiber-reinforced composite inlay-retained fixed partial dentures. J Prosthet Dent. 2005; 93:(3)337-345
Briggs PFA, Bishop K, Djemal S The clinical evolution of the “Dahl Principle”. Br Dent J. 1997; 183:171-176
Bjorn L, Krogstad D, Krogstad O The effect of a partial bite raising splint on the occlusal face height. Acta Odont Scand. 1982; 40:17-24
Yokoyama D, Shinya A, Lippo VJ, Lassila LVJ, Gomi H, Vallittu PK, Shinya A Framework design of an anterior fiber-reinforced hybrid composite fixed partial denture: a 3D finite element study. Quintessence. 2009; 22:(4)405-412
Hussey DL, Linden GJ The clinical performance of cantilevered resin-bonded bridgework. J Dent. 1996; 24:(4)251-256
Shinya A, Yokoyama D, Lassila LVJ, Shinya A, Vallittu PK Three-dimensional finite element analysis of metal and FRC adhesive fixed dental prostheses. J Adhes Dent. 2008; 10:365-371
Visser HJ, van Rensburg JJJ Fibre-reinforced composites – alternative for lost teeth replacement. SADJ. 2005; 60:(1)20-22
Replacing missing teeth is an integral part of the clinical services of the dental practitioner. The fibre-reinforced composite (FRC) bridge is a relatively new method for replacing missing teeth. This article will explain and discuss this alternative treatment option. Practical instructions on how to construct a FRC bridge will be given, by means of a clinical case. Different technique options will be illustrated to provide the reader with a good understanding of the most practical way to use the FRC strips. The fibre-reinforced composite provides a non-destructive, aesthetically pleasing and cost-effective way to restore missing teeth.
Clinical Relevance: Minimally invasive options should always be considered and destruction of healthy enamel and dentine during the preparation phase of a replacement treatment should be avoided as much as possible.
Article
Providing a fixed replacement for a missing tooth is an important part of the work of a dentist and, today, we have a range of options to offer patients in order to achieve this. In some instances, an implant might be the treatment option of choice, but this may be declined for a variety of reasons, such as poor bone quality, the patient's medical history, lack of adequate bone, unfavourable position of anatomical structures and adjacent roots, periodontal susceptibility, social habits like smoking, and cost.
Conventional bridgework may also be offered but this can be relatively expensive, not to mention how destructive this can be to the abutment teeth. Another option that may be considered is a resin-retained porcelain fused to metal bridge, a treatment that, although conservative, can leave a lot to be desired when it comes to aesthetics and reliability.1 Dentures, even the chrome cobalt or flexible Valplast options, may not be the patient's preferred option. With all of these treatment options there is a delay between the initial preparation and impression and the placement of the final restoration, because laboratory work takes time. The fibre-reinforced composite (FRC) bridge is not the ultimate solution for tooth replacement but it is a treatment option available to patients which is highly conservative, aesthetically pleasing, relatively inexpensive and can be placed in one session, offering the ‘quick-fix’ required by many patients. As little or no preparation is carried out to the abutment teeth, this option can make the treatment reversible and, because the bridge is constructed in resin composite material, it can be readily repaired in the event of breakage. The FRC bridge is especially useful as an option for elderly patients where the treatment options should preferably be simple and quick.
There are a number of fibre-reinforced materials on the market today including Fiberkor (Jeneric/Pentron), Vectris (Ivoclar), EG Fibres (Kuraray/Japan) and everStick (GC) and others.
The everStick range of fibres (GC Corporation) has proven to be popular in the UK as their use is backed up by more than 300 scientific papers with many years of clinical follow-up data.2 The everStick products have the interpenetrating polymer network (IPN),3 which provides excellent properties for bonding with composite materials, adhesives and resin cements. The fibre bundles consist of silanated glass fibres impregnated with a PMMA (polymethylmethacrylate) polymer and BisGMA matrix.4,5,6 This results in each fibre bundle being surrounded by a PMMA outer layer. Otherwise, the ‘ingredients’ of the fibre-reinforced composite are the same as that of a composite. In essence, it is only the shape and the size of the glass filling particles that differ. In the fibre-reinforced composites the filling particles are unidirectional glass strands instead of small glass particles. The FRC bridge technique uses these fibre bundles, which may be bonded to or embedded in abutment teeth, to create a scaffolding within which a pontic may be constructed using composite restorative materials. Even when clinicians are familiar with the concept of FRC bridges, many fail to develop their skills in this area because of misconceptions about the difficulty of the technique. Admittedly, FRC bridges may be technique sensitive and can have something of a learning curve, but this type of treatment should be well within the capabilities of any practising dentist.
FRC bridges may also be constructed by an indirect technique, with the bridge being manufactured in an accredited dental laboratory. Although good aesthetic results may be obtained, the direct method still has the advantage that the end result could be achieved in a single session. That being said, the indirect technique has the attraction of requiring less chair time, less patient co-operation and less clinical skill.
FRC bridges may not be suitable for all clinical situations. Case selection and treatment planning are therefore crucial to ensure the best results. Factors such as the span of the space to be bridged, the condition of the potential abutment teeth, the occlusion and any parafunctional habits of the patient should be taken into account. To place FRC bridges with consistent success one must understand fully the limitations as well as the advantages of this technique and all aspects should be discussed with the patient.
FRC bridges can be used for temporary, medium-term and long-term solutions. The FRC restorations (splints, bridges and posts) perform well and results recorded and presented by Mutlu Özcan of the University of Zurich reported a 95.2% success rate after 6 years.2 Similar results were also found in a recent article from Germany and the conclusion of this article stated: ‘Fibre reinforced composite fixed partial dental prostheses provide sufficient stability and very good aesthetic, biological and functional performance in cases of specific clinical indications’.7 The ability to reinforce dental composites opens up a new world of treatment options available to the dental clinician. Besides FRC bridges discussed here, fibre-reinforced composite has diverse other applications in dentistry, including periodontal splinting,8,9,10 the anatomical post construction,3,11 orthodontic permanent retention,12 and more.
General principles when considering providing a FRC bridge
The oral hygiene of the patient
Patients with poor oral hygiene should be evaluated carefully. If the patient proves not to respond to good oral hygiene instructions, he/she might be better off without the bridge.
A dry operating field
A dry operating field is crucial for adhesive dentistry and rubber dam isolation is mandatory.
Bonding the fibres
Bonding the fibres to porcelain will be less successful than bonding to natural enamel. The bond between composite and etched enamel is considered as the gold standard. If bonding the fibres to porcelain is the only option, the patient should be informed of the possibility of debonding due to weaker bond strength.13 When bonding to porcelain and metal, porcelain and metal primers should be used according to the manufacturer's instructions.
The position in the dental arch
Anterior replacements are preferable, as compared to replacement of molar teeth using a direct FRC bridge, as posterior bridges are more demanding. The occlusal forces are much greater on posterior teeth14 and a stronger frame (more fibres) will be required. The molar pontic is also bulkier and will take longer to construct. Access is more difficult and isolation for a dry operating field may be less effective than in the anterior area. An indirect option might be a better choice for replacement of molar teeth. However, the FRC bridge may be reliable for posterior bridges if sufficient fibres are used and the design of the fibre frame is correct.14
The occlusion
During the planning phase of the treatment, the clinician should study the occlusion. Occlusal contact points should be checked with articulating paper prior to placing the fibres in order to plan the best possible design and attachment positions of the fibre to the retainer teeth. Adequate clearance for the fibre wings attached to the abutment teeth may present a problem with upper anterior bridges where there is little intra-occlusal space, such as is found in some Class 2 occlusions with an increased overbite. In these cases, the fibre wings on the palatal aspects of the upper anterior teeth can interfere with the occlusion of the lower anterior teeth. In these problematic cases, the clinician can consider making a preparation on the palatal aspect of abutment teeth, in order to create space for the fibres. Removing existing restorations may provide the necessary room for these fibre wings. In cases with perfectly sound teeth where preparation is not ideal, the construction can be deliberately left, ‘high’ in occlusion,15 relying on the modified Dahl principle.16 The patient should be informed that it will feel strange at the outset but the posterior occlusion should re-establish itself within 4–6 months.16 Placing the fibres on the labial side of the retainer teeth could also be considered. Direct composite veneers will then have to be constructed in order to cover the fibres and to achieve an acceptable aesthetic result. Lateral excursive movements should always be checked and sound prosthodontic principles applied when creating these bridges.
Para-function
FRC or pure composite restorations might have an advantage over the porcelain and other tooth-coloured laboratory manufactured restorations as they are more easily repairable in mouths with greater load on the restorations and where fractures of the restorations may be more common. Communication with these patients is very important and they should be informed of their bruxist habits and the consequences that this will have on their dentition.
The span of the bridge
The span of the bridge should also be taken into account. Single tooth replacement is the ideal application, but if the fibre frame is designed and constructed correctly, it can be employed to replace two or even up to four anterior teeth. The everStick fibre bridges are sufficiently strong to replace posterior teeth.14 The method of attachment and the number of retainer teeth will play a significant role in the longevity of these posterior bridges. The most reliable method of attachment to the retainer teeth will be achieved by bonding the fibres into MO or DO cavities14(for example, after removal of existing restorations), combined with labial or lingual fibres bonded to the lingual or labial surfaces of the retainer teeth. As with any other material, the shorter the bridge span the better the durability will be.
The fibre frame design for an anterior FRC bridge17
The conventional design for an anterior bridge will consist of an everStick C&B (GC) (or other) fibre bonded from the palatal side of the first retainer tooth bridging the space of the missing tooth then bonded onto the palatal side of the second abutment tooth (fixed/fixed). Cantilever designs can also be considered in the case of a missing lateral where the canine tooth can act as the retainer.6 A vertical piece of fibre could be added to the horizontal fibre for pontic reinforcement. An everStick C&B (GC) fibre can be used for the vertical reinforcement or a thinner everStick Perio (GC) could also be considered to prevent a ‘too bulky’ fibre frame as the perio fibre is much thinner than the C&B fibre. Cantilever resin-bonded bridges constructed with a metal frame prove to be very successful, especially when replacing missing laterals.18 According to Yokoyama, the fibre frame can still be successfully bonded to both adjacent retainer teeth (fixed/fixed),18 as well as the less invasive, cantilever options (especially when replacing missing lateral incisor teeth).6 As the force distribution is different in the fibre frame than in the metal frame, the double retainer technique is also successful in the fibre frame, resin-retained bridges.19
The ‘U-shaped’ fibre technique
When constructing the pontic directly in the mouth, clinicians may be concerned about the fitting area of the pontic on the gingivae. The pontic should be created so that it will be smooth and easy to clean. Over the years, the author has used many different ways to construct the pontics directly in the mouth but the ‘U-shaped technique’, which was developed by the author, is a means of ensuring a well-fitting pontic. Chairside construction of a part of the fibre frame and pontic, outside the mouth, will simplify the procedure and will ensure a well-fitting and an aesthetically pleasing final result. This method can also save valuable ‘chairtime’. This technique is also useful when constructing a posterior bridge where the pontic is bigger and also further back in the mouth. A short description of this technique follows:
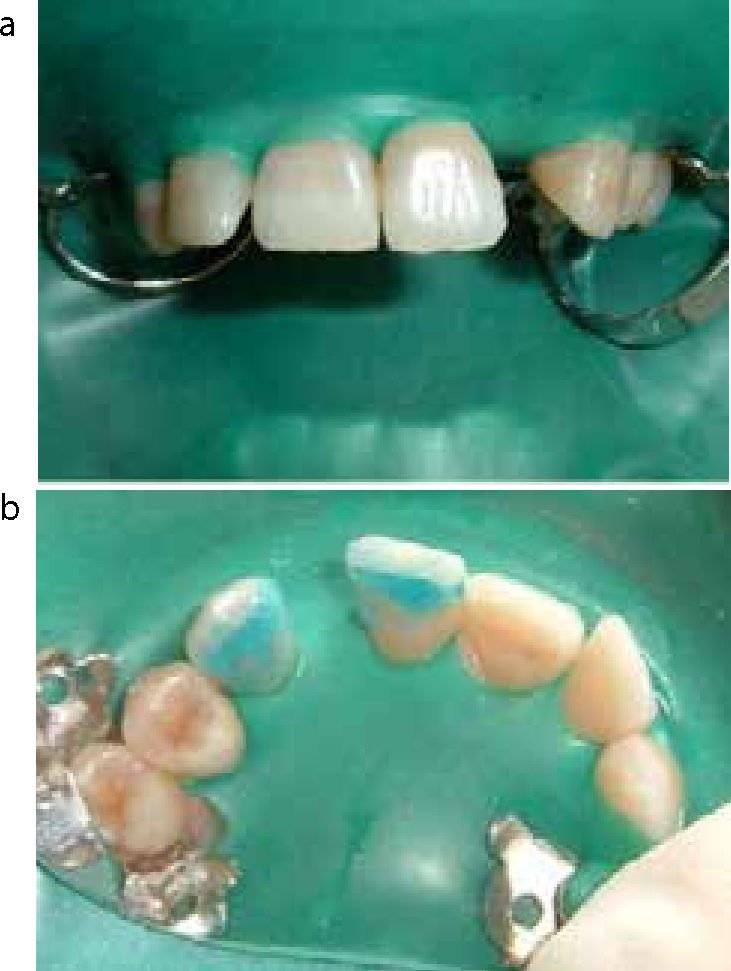
A silicone model is created by carefully injecting bite registration material into an alginate impression of the patient's dentition. On this silicone model the pontic is partially constructed with composite and a ‘U-shaped’ fibre between the retainer teeth (Figure 1).
The thinner perio fibre is normally used to create the ‘U-shape’. The fitting surface of the partially constructed pontic can now be polished before bonding it into the mouth (Figure 2).
The partially constructed pontic and the conventional everStick C&B fibre (on the palatal of the retainer teeth) can then be bonded (Figure 3).
The pontic can then be completed by layering the different layers of composite for the end result (Figure 4).
Figure 1. On this silicone model the pontic is partially constructed with composite and a ‘U-shaped’ fibre between the retainer teeth.Figure 2. The fitting surface of the partially constructed pontic can now be polished before bonding it into the mouth.Figure 3. The partially constructed pontic and the conventional everStick C&B fibre (on the palatal of the retainer teeth) can then be bonded.Figure 4. The pontic can then be completed by layering the different layers of composite for the end result.
The conventional fibre-reinforced composite bridge
In cases where the ‘U-shape’ is not used, the pontic may be built up directly in the mouth by forming the pontic ‘free hand’ against the rubber dam. This technique works well in the case of an anterior tooth and will be described by means of a clinical case.
Clinical case
In this case, a missing upper left lateral incisor tooth was replaced with a FRC bridge. During the consultation appointment all treatment options were explained, as mentioned previously.
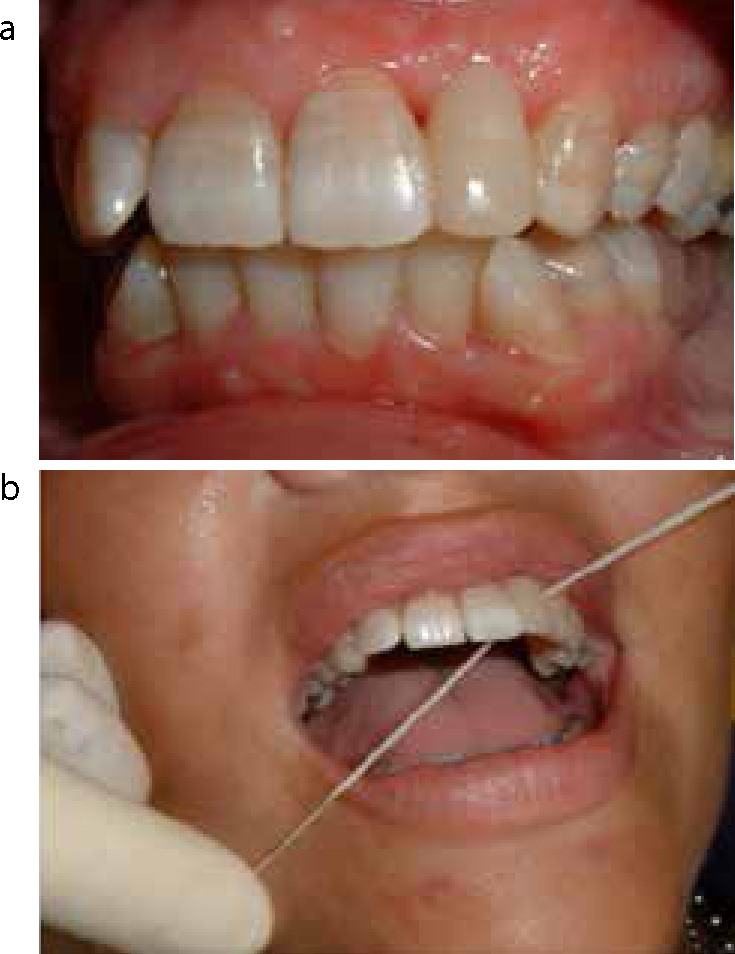
Figure 5 presents the pre-operative view of the missing upper left lateral.
Rubber dam isolation was achieved and shallow groove preparations were made on the palatal aspect of the UL1 and UL3 in order to accommodate the fibres (Figure 6).
The surface retained option (with no preparation) may also be followed but a shallow groove within the enamel will provide a good surface for etching of the enamel and bonding of the fibres. The length of the fibre is normally measured in the mouth with a piece of ligature wire.
Phosphoric acid (37%) was used to etch the enamel. Bonding agent was applied according to the manufacturer's instructions. Flowable composite was used as luting cement for the fibres.
The uncured fibre is positioned in the uncured flowable composite and then cured simultaneously with the fibre in the correct position.
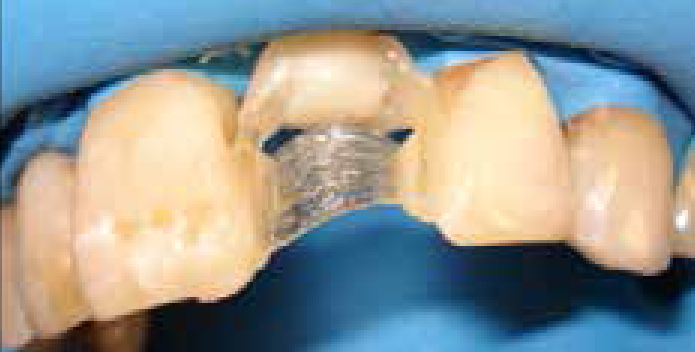
The position of the fibre is very important. As can be seen in Figure 7, the fibre is curved in a labial direction and, from an incisal direction, the fibre should be in the centre of the two retainer teeth.17 The well positioned fibre-wings on the palatal aspect of the UL1 and UL3 are then covered with a layer of composite (G-aenial A3) (GC).
It is strongly recommended to add a vertical fibre for pontic reinforcement (Figure 8), with the best position for the vertical fibre being on the palatal side of the horizontal fibre. The vertical fibre is attached to the horizontal fibre by placing a small amount of flowable composite onto the horizontal fibre, positioning the uncured vertical fibre into the uncured flowable composite and then securing it in position by curing the vertical fibre and flowable composite simultaneously. The different layers of composite can now be bonded onto this frame during the pontic construction.
In most cases, where an anterior tooth is missing, the pontic may be directly built up in the mouth (there are other ways to construct the pontics as mentioned earlier). It is recommended to use a flowable composite directly on the fibre as the first layer of composite. Once this is cured, the different layers of composite are added to construct the pontic. A good aesthetic result can be achieved when building up a complete pontic in layers of composite with different translucencies. In this case the G-aenial (GC) range of composites was used to build up the pontic.
The rubber dam is stretched tight over the gingiva and the inside layer (G-aenial AO3) (GC) is pushed in under the fibre frame with a flat plastic composite instrument (Figure 9). This layer is in direct contact with the rubber dam (which is stretched over the gingivae) and the pontic is shaped against the rubber dam.
The composite brush together with Composite primer (GC) are handy to shape the different layers and to control their volumes (Figure 10). Care is taken not to trap any air bubbles inbetween the composite and the rubber dam. This layer is then covered by the next layer of standard shade (G-aenial A3) (GC).
The pontic is then completed by placing the final layer of enamel shade (G-aenial AE) (GC) (Figure 11). The occlusion is checked and adjusted.
Figures 9-12 illustrate a basic layering technique which is not time consuming. It is also possible to include more detail to the inside layers of the pontic by, for example, adding the mamelon structure and thinning out the edges of the layers to prevent definite lines between the different layers. As the clinician gets more experienced with the technique, these finer details, together with the use of composites stains, can be applied to reach the ultimate aesthetic result.
This procedure took approximately 2 hours to complete.
In some cases it may be useful to use pink gingivae shade composites to make the pontic look shorter (Figure 13). This is an extra advantage of working with the fibres and composite.
Figure 5. The pre-operative view of the missing upper left lateral.Figure 6.
(a, b) Rubber dam isolation was achieved and shallow groove preparations were made on the palatal aspect of the UL1 and UL3 in order to accommodate the fibres.Figure 7.
(a, b) The fibre is curved in a labial direction and should be in the centre of the two retainer teeth.Figure 8. Vertical fibre added for pontic reinforcement.Figure 9. The rubber dam is stretched tight over the gingiva and the inside layer (G-aenial AO3) (GC) is pushed in under the fibre frame with a flat plastic composite instrument.Figure 10. The composite brush together with composite primer (GC) come in handy for shaping the different layers and to control their volumes. The handle is autoclavable and the tips are disposable.Figure 11.
(a, b) The pontic is then completed by placing the final layer of enamel shade (G-aenial AE) (GC).Figures 12.
(a, b) The bridge was completed and oral hygiene instructions were given.Figure 13. In some cases, it may be useful to use pink gingivae shade composites to make the pontic look shorter.
Conclusion
Fibre-reinforced composite bridges offer a good alternative and minimally invasive treatment option to replace missing teeth. They are useful for temporary and medium-term solutions. Both the direct and indirect options could be employed. The direct option requires the learning of a new clinical skill but is a useful technique, especially for emergency cases and when treating the elderly patient. FRC bridges are a reversible, cost-effective treatment option and provide a fixed solution for the replacement of one or more teeth, instead of providing the patient with a removable prosthesis which is, in many cases, not easy to manage.20