Caplin RL Grey Areas in Restorative Dentistry – Don't Believe Everything You Think!.: J and R Publishing; 2015
Caplin RL Grey Areas in Restorative Dentistry – Don't Believe Everything You Think!.: J and R Publishing; 2015
Caplin RL Grey Areas in Restorative Dentistry – Don't Believe Everything You Think!.: J and R Publishing; 2015
Caplin RL ‘Is there anything wrong with my teeth and gums?’ The challenges of the dental examination and care planning. Br Dent J. 2022; 233:190-196 https://doi.org/10.1038/s41415-022-4553-7
Mamoun JS A rationale for the use of high-powered magnification or microscopes in general dentistry. Gen Dent. 2009; 57:18-26
Bud M, Jitaru S, Lucaciu O The advantages of the dental operative microscope in restorative dentistry. Med Pharm Rep. 2021; 94:22-27 https://doi.org/10.15386/mpr-1662
Sheets CG The periodontal-restorative interface: enhancement through magnification. Pract Periodontics Aesthet Dent. 1999; 11:925-931
Whitehead SA, Wilson NH Restorative decision-making behavior with magnification. Quintessence Int. 1992; 23:667-671
Grey Areas in Restorative Dentistry: Part 2. The Diagnosis: Dental Pain Robert L Caplin Dental Update 2025 51:11, 796-800.
Authors
Robert LCaplin
BDS, MSc, DGDP (RCS Eng), Dip Teach Ed (King's), Retired Senior Teaching Fellow, Faculty of Dentistry and Oral and Craniofacial Sciences, King's College London; General Dental Practitioner, London
In order to help those who seek our care with a problem, whether real or perceived, overt or covert, it is essential to make a diagnosis. Arriving at a diagnosis involves multiple steps, including taking a dental/medical history, performing a physical examination, undertaking diagnostic tests, and then examining the data to come to the best explanation for the situation presented. Only after this process can the options for management be properly considered
CPD/Clinical Relevance:
Pain management is an essential part of dental practice and requires an accurate diagnosis.
Article
When a patient attends a dental practice with an overt problem, it is essential that the practitioner makes a diagnosis so that effective measures can be put into place to address the issue. However, even at a routine check-up visit, the dentist may come across a covert situation that again, will require a diagnosis to be made.
What are we doing when we make a diagnosis? The ‘art or act of identifying a disease from its signs and symptoms’ or the ‘decision reached by diagnosis’.1 Arriving at a diagnosis involves multiple steps including taking a dental/medical history, performing a physical examination, undertaking diagnostic tests, and then examining the data to come to the best explanation for the illness, although there will be times when it is not possible to come to a definitive diagnosis and two or more possibilities will have to be considered, that is, it could be this, and/or this.
Taking a history is the first step in making a diagnosis and when a patient attends a practice, it is essential to have a sequential approach to managing their needs and wants, especially for someone who is in pain or discomfort. Such patients are likely to be stressed, fearful and anxious, and may have been without sleep or substantial food for a period before attending the practice. Creating a calm and relaxing atmosphere will reassure the patient as well as being more likely to elicit reliable information about the complaint. Wherever possible, the consultation should be away from the dental chair (Figure 1). Would you expect a surgeon to take a history of a complaint while the patient is lying on the table in the operating theatre?
Figure 1. Initial consultations should take place away from the dental chair.
Framing the problem
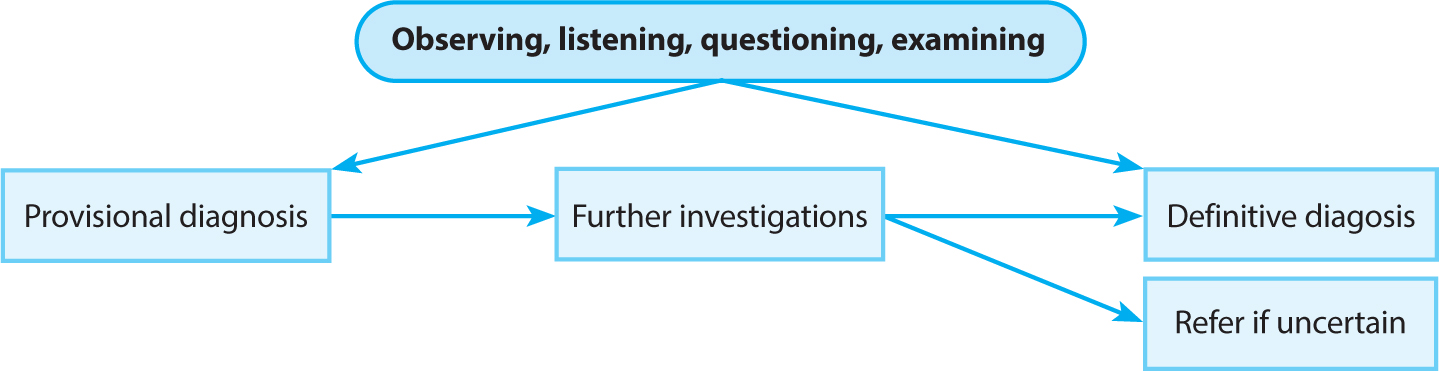
This process begins with the presenting condition of the patient. We can hear patients when we are told a history of the complaint, but if we listen carefully and ask appropriate questions, they will often give us a very good indication of what the problem is. It may be possible to arrive at a provisional diagnosis before even looking in the mouth (Figure 2). So, what is the difference between these two modalities? Hearing is ‘the process, function, or power of perceiving sound’2 whereas listening is ‘to hear something with thoughtful attention, to give consideration’.3 And then, the more experienced we become as dentists, the more easily and readily we will pick up important clues from the patient's narrative.
Figure 2. Stages in diagnosis. (Modified from Caplin.4)
There can be no doubt that the relief of a patient's pain or discomfort is one of the most rewarding aspects of dental practice.
Specific questioning regarding the pain, or the teeth, or the soft tissues can elicit more information leading to a provisional diagnosis.
Pain
Present now?
How long has it been present?
Any change?
Better or worse?
What type of pain? Aching, throbbing, sharp, boring?
Can you locate the pain accurately?
Is the pain affected by temperature changes?
Is the pain affected by sweet foods?
Is there pain with pressure to a tooth or an area?
What relieves the pain? Analgesics, thermal changes, pressure changes?
Are you kept awake at night?
Is the pain less since the swelling appeared?
Teeth
Have any broken recently?
Has there been any dental treatment recently in the area?
Are any teeth loose?
Swellings
When did the swelling appear?
Is it increasing in size?
Is the adjacent gum swollen?
Are there any areas of tingling or numbness? Lower lip, tongue, cheek?
Is there a bad taste in the mouth coming from a particular area?
Is there any limitation of opening?
The Socrates acronym is a useful way to structure the clinical questioning (Table 1). So, in a structured examination it is sensible to look at:
The patient
The mouth
The sextant in question (if symptoms are present) in static and dynamic position.
The tooth or teeth under suspicion
Site
Where is the pain or the maximal site of pain?
Onset
When did the pain start and was it sudden or gradual? Is it getting better or worse?
Character
What is the pain like? An ache, stabbing, boring, awareness?
Radiation
Does the pain radiate anywhere?
Associations
Any other signs or symptoms associated with the pain?
Time course
Does the pain follow any time pattern?
Exacerbating/relieving factors
Does anything change the pain? For example, temperature change/analgesics
Severity
How bad is the pain on a scale of 1–10 (10 being the worst)?
The patient
Look at how they care for themselves. How they are dressed and groomed. How they sit. Signs of nerves. Facial expressions. Listen to what they say and how they say it. How they respond to questioning. Assess their ability to explain their problems or to respond to further probing (Figure 3).
Figure 3. Pay attention to to the patient's demeanor and facial appearance.
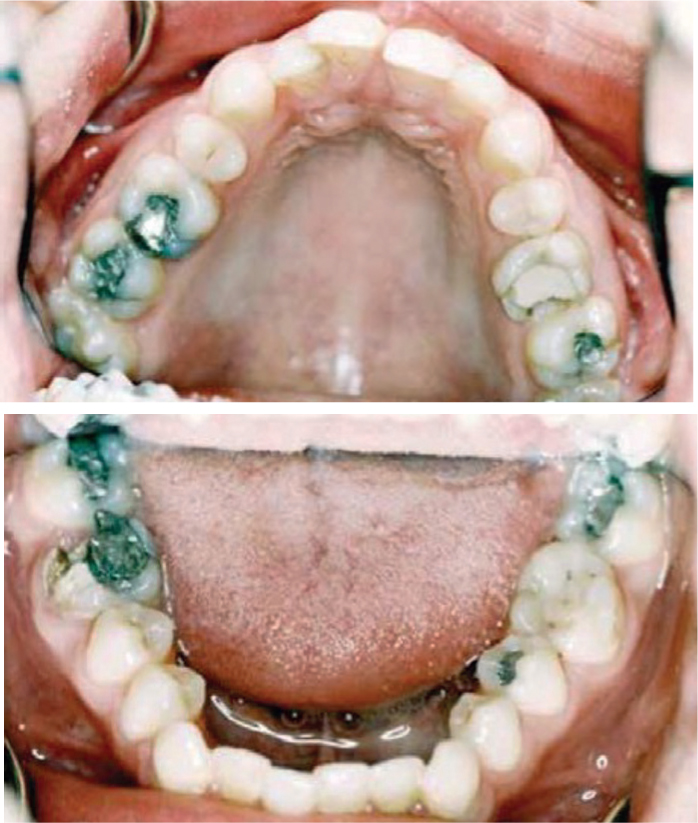
The mouth
Look at the state of the hard and soft tissues to get an overall impression of the patient's dental past and present. Lots of dentistry? What quality? Are there any missing teeth, appliances, bridges, crowns or caries? Look at the periodontal condition and any soft-tissue swellings (Figure 4).
Figure 4. Examine the mouth.
The sextant
Look at the area producing symptoms both in its static, intercuspal position and in its dynamic relationship with the opposing jaw in lateral excursions (Figure 5).
Figure 5. Look at the area producing the symptoms.
The tooth or teeth
Focus on the symptomatic tooth or teeth and make an assessment (Figure 6).
Figure 6. Focus on the symptomatic tooth or teeth an make an assessment.
Perhaps the most common presenting oral pain in the dental surgery is that arising from a tooth or teeth, so it becomes vitally important to be able to distinguish the presenting symptoms and signs of pulpal pain. Table 2 covers the range of pulpal conditions and their symptoms and signs.
Reversible pulpitis
Irreversible pulpitis
Pulpal necrosis
Apical periodontitis
Apical periodontitis with existing root filling
Peri-apical abscess
Pain
Sharp
Aching or throbbing
No
AchingAwareness
AchingAwareness
Boring, aching throbbing when acute Awareness when chronic
Localization
No
No
No
Yes
Yes
Yes
Onset
Thermal or tactile stimulus
Spontaneous or with thermal or tactile stimulus
None
Pressure from occlusal forces or chewing
Pressure from occlusal forces or chewing
Constant
Duration
ShortFew secondsSubsides with cessation of stimulus
Minutes to hours
None
Subsides when pressure is relieved
Subsides when pressure is relieved
Hours to days
Swelling
No
No
No
No
No
Yes, when acute; subsides when chronic
Periostitic
No
No
No
Yes
Yes
Yes, when acute; no when chronic
Buccal tenderness
No
No
No
Yes
Yes
Yes
Management
Deal with exposed dentine, e.g. repair or replace filling
Remove root canal contentsRoot canal treatment or extraction
Remove root canal contentsRoot treatment or extraction
Remove root canal contentsRoot treatment or extraction
Re-treat canal or apical surgery or extraction
Extraction if facial swellingRemove root canal contentsRoot treatment or root canal re-treatment or extraction
However, it is important to bear in mind that pain can arise from any of the tissues associated with the tooth. Periodontal tissue can give rise to acute or chronic pain, and investigation of the state of the periodontium in the region of the complaint should be undertaken with a periodontal probe. This would be to assess pocket depths as well as tooth mobility, which can be an indicator of localized excessive occlusal loading. Such overloading can also result in stress fractures in the tooth itself, which would lead to a pulpal reaction, and so it becomes important to identify the cause of the insult to the pulp (Figures 7 and 8). As indicated above, an occlusal examination is required to assess the stresses on the teeth in question. Where the symptoms are not consistent with pulpal or periodontal pain, other possibilities such as atypical facial pain or TMJ dysfunction should be considered.
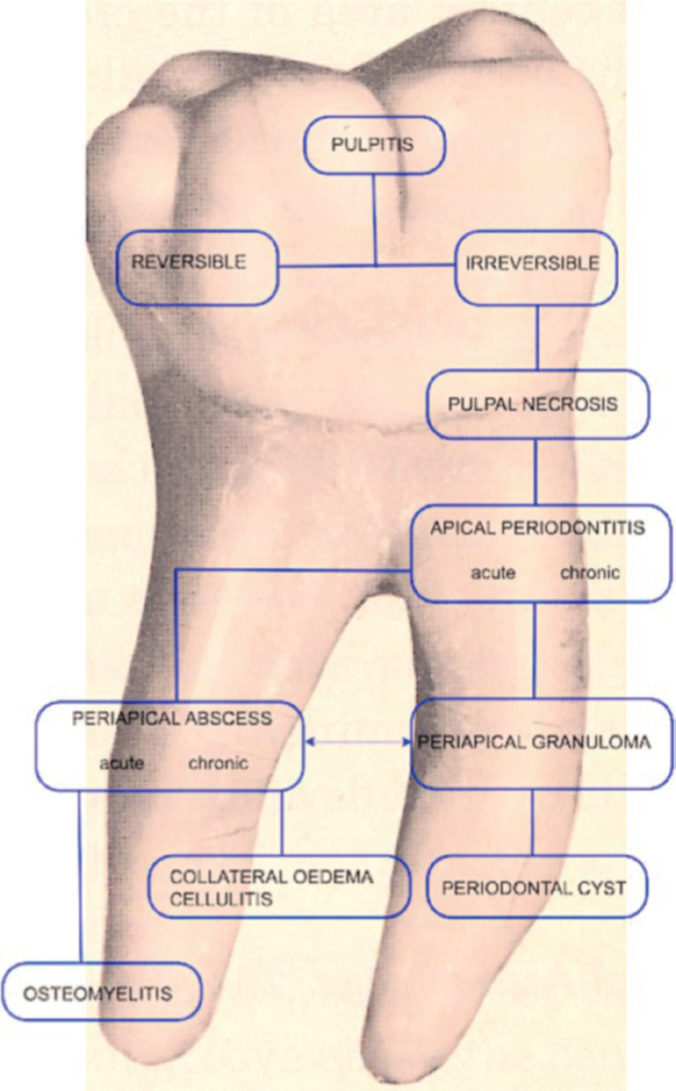
Figure 7. Sequelae of inflammation of pulpal tissues (from Caplin).6Figure 8. Fracture extending along root surface resulting from excessive occlusal loading and producing pulpal symptoms.
The challenge of accurate observation
Visual and tactile observations are only applicable to those structures that are readily accessible, whereas those structures that are beneath the surface can only be assessed by additional investigative procedures.7 It is essential to know what the normal appearance looks like to distinguish this from the abnormal, diseased appearance.
Further investigations
Having observed, listened to, questioned, and examined the patient, it may be that a provisional diagnosis can been made and that further investigations are required to give additional information, hopefully leading to a definitive diagnosis. These further tests may comprise sensibility tests, percussion, palpation, application of a dye, transillumination, radiographs, CBCT, temperature assessment and biopsy. However, if a definitive diagnosis can be made following clinical examination, then clearly further investigations are not warranted.
As mentioned, in practice there are two levels of observation: that of the superficial structures and surfaces which are directly visible (e.g. teeth, periodontal tissues, soft tissues) and the deeper tissues and structures. However, even within the visual assessment, there are two levels of observation: one with the naked eye and one with magnification. Experience shows that enhanced vision of carious lesions, restoration margins and tooth fractures aids diagnosis, and there is ample evidence that magnification improves operative procedures.8-12
Regarding the deeper structures, the practitioner should have a protocol for the taking of radiographs because this will be the most common way of assessing unseen areas. When there is an acute situation, clearly the area to be investigated will be determined by the suspected location of the problem. However, in a non-acute situation, such as a routine examination, consideration should be given to the investigation of teeth that are heavily filled or have indirect restorations in, or over, them. Only then can the status of the tooth or teeth be decided with some degree of certainty (Figure 9).
Figure 9. Asymptomatic upper right central incisor with a metal ceramic crown. Periapical radiograph taken as part of a new patient examination.
Re-framing leading to a diagnosis
Once the clinician is satisfied that enough information has been gathered, in most cases of dental pain a definitive diagnosis can be made. It is true to say that ‘there can only be one correct diagnosis but there may be several ways of dealing with the situation’. Should the practitioner be unsure of the diagnosis, it would be prudent to get a second opinion before embarking on irreversible procedures. Undoubtedly, there needs to be a full and frank discussion with the patient regarding the certainty or not of the diagnosis. There may be an incorrect assumption among dentists that to be worthwhile, one must be thoroughly competent and successful in his/her field, which might be taken to mean, practically, arriving at a diagnosis in all clinical situations. With experience comes the ability to be able to say, ‘I don't know’.
Conclusion
Arriving at a diagnosis can be very difficult and requires not only a sequential approach, but in addition, skill, and judgement from the practitioner. ‘Good judgement comes from experience and a lot of experience comes from bad judgement’. From a medico-legal perspective, it is extremely important that a record is kept of the interaction between the practitioner and the patient so that a third party perusing the notes can follow the flow of the complaint, the questioning, the investigations, the reporting of the investigations and the diagnosis. It may transpire that the diagnosis was incorrect but if it was made with as much information as possible, and the symptoms and signs are not clear, then it may be that the best guess is acceptable. As in a math's question, showing the working is as important, if not more so, than the answer!
Clinical conundrums
For these clinical scenarios, what would be the aims of treatment, the range of interventions to achieve these, and how would you choose? List the risks and benefits for each option.
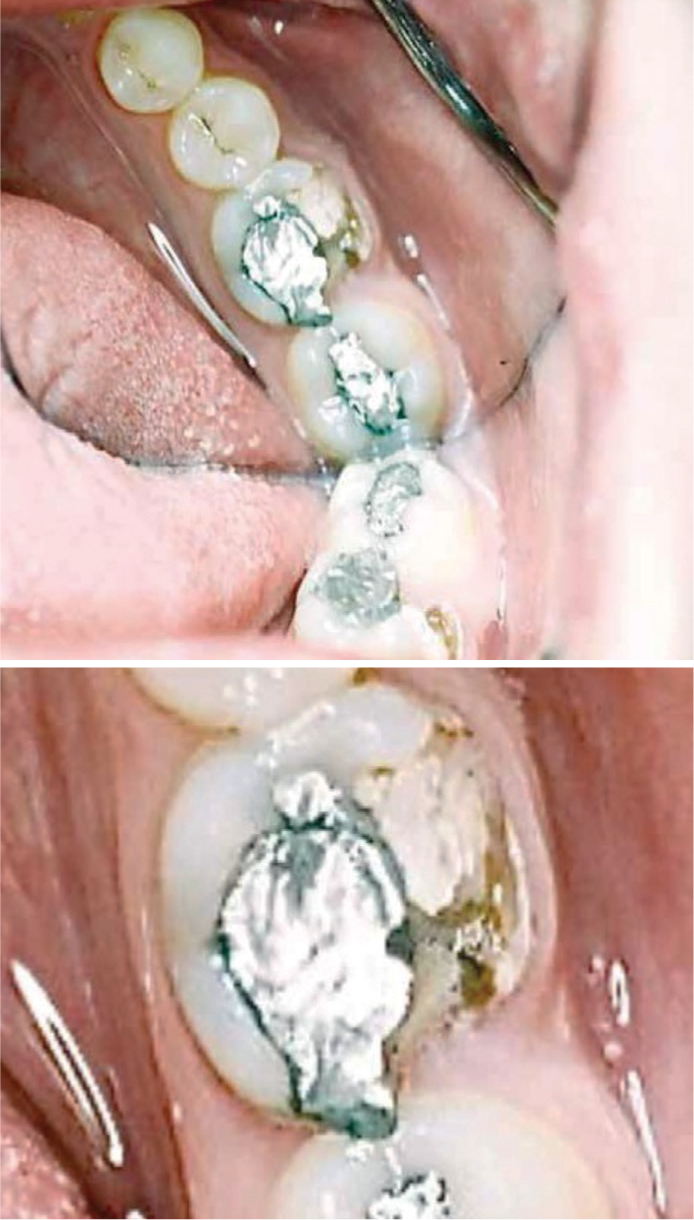
This patient complained of mild aching in the lower right quadrant and some discomfort on chewing. There was buccal tenderness at LR6.
What has happened here and what is the possible diagnosis?
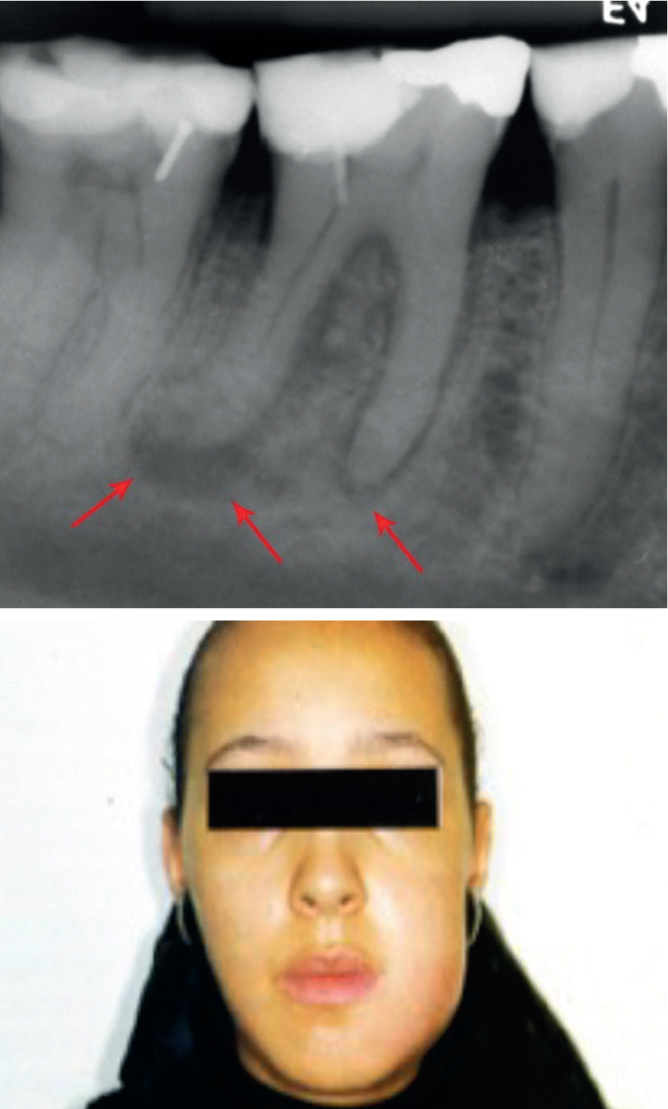
This patient presents in your practice. What history would you expect her to give and what provisional diagnosis would you make before inspecting the mouth?
What further investigations would be appropriate? What if the patient has limited opening?