Norton WE, Funkhouser E, Makhija SK Concordance between clinical practice and published evidence: findings from The National Dental Practice-Based Research Network. J Am Dent Assoc. 2014; 145:22-31 https://doi.org/10.14219/jada.2013.21
Zitzmann NU, Krastl G, Hecker H Strategic considerations in treatment planning: deciding when to treat, extract, or replace a questionable tooth. J Prosthet Dent. 2010; 104:80-91 https://doi.org/10.1016/S0022-3913(10)60096-0
Avila G, Galindo-Moreno P, Soehren S A novel decision-making process for tooth retention or extraction. J Periodontol. 2009; 80:476-491 https://doi.org/10.1902/jop.2009.080454
Manola M, Hussain F, Millar BJ Is the shortened dental arch still a satisfactory option?. Br Dent J. 2017; 223:108-112 https://doi.org/10.1038/sj.bdj.2017.625
Report of a WHO Expert Committee. World Health Organ Tech Rep Ser. 1992; 826:1-37
Caplin R Grey Areas in Restorative Dentistry: Part 1. What are the Aims of treatment?. Dent Update. 2024; 51:730-734
Grey areas in restorative dentistry: Part 3. clinical decision making and care planning Robert L Caplin Dental Update 2025 52:1, 67-72.
Authors
Robert LCaplin
BDS, MSc, DGDP (RCS Eng), Dip Teach Ed (King's), Retired Senior Teaching Fellow, Faculty of Dentistry and Oral and Craniofacial Sciences, King's College London; General Dental Practitioner, London
Much of clinical dentistry is subjective rather than objective, and every dental practitioner must make decisions about how to manage the various clinical and ethical challenges that patients present. These clinical decisions are ultimately idiosyncratic and are, therefore, the reason that there can be wide variation between dentists as to how each would manage a particular situation. There is a need to balance the demands of the patient with the ethical requirements of the profession and the moral position of the practitioner.
CPD/Clinical Relevance: Whereas some aspects of dentistry are supported by science and the evidence base, many are not, especially in the realm of clinical decision making.
Article
When a patient attends either for a routine examination or as an emergency, it is essential to have a standard protocol so that an effective and appropriate care plan can be drawn up. This will involve listening, observing, questioning, examining, making a provisional diagnosis, testing, reviewing the test results, revisiting the provisional diagnosis and then, with all of the gathered information, producing a care plan that meets the needs and wants of the person that has come for care.
The care plan will be based on what outcome is agreed between the patient and the practitioner. Sometimes it will be just the management of a single issue, whereas at other times, it may be bringing the mouth to a state of good oral health. It is time well spent in discussing with the patient their hopes and aspirations for their dental care because it can avoid misunderstandings, disappointment, and perhaps legal redress, later on in the treatment and post-treatment phase: ‘disappointment lives in the gap between expectation and reality’.
A written plan will certainly aid this process. At the time of the examination, it should be realized that the clinical situation presented is part of an ongoing, vital process and it is essential to understand what has gone before to bring the patient to this state and in the light of this knowledge to plan for the future (Figure 1).
Figure 1. When we see a patient, it is like looking at a single frame of a video.
Clinical decision making
It is important to remember that dentistry is ‘the art or profession of a dentist’1 and that much of clinical dentistry is subjective rather than objective. Indeed, Fish and Coles2 consider clinical decision making as professional artistry. There isn't a probe that we can put onto a tooth that will tell us what to do. Fill this one. Watch this one. Repair this filling. Replace this filling. Put a post in this tooth. Extract this tooth. These clinical decisions are ultimately subjective and, therefore, are the reason that there can be wide variation between dentists as to how they would manage a particular situation, and even a wide variation by the same dentist on different days and at different times. As Kahneman3 pointed out, ‘the extent of the inconsistency is often a matter of real concern. Experienced radiologists who evaluate chest x-rays as “normal” or “abnormal” contradict themselves 20% of the time when they see the same picture on separate occasions. A study of 101 independent auditors who were asked to evaluate the reliability of internal corporate audits revealed a similar degree of inconsistency. A review of 41 separate studies of the reliability of judgments made by auditors, pathologists, psychologists, organizational managers, and other professionals suggests that this level of inconsistency is typical, even when a case is re-evaluated within a few minutes. Unreliable judgments cannot be valid predictors’.
Dentists are not immune to this lack of consistency. Like it or not, our decisions are going to vary.4 From a professional development point of view, we should think about them, reflect on them, and learn from the outcomes of the treatments.
The stages in the production of decisions are:
Framing of the problem that is to be solved.
The collection of relevant information leading to a decision.
Reflection and review.
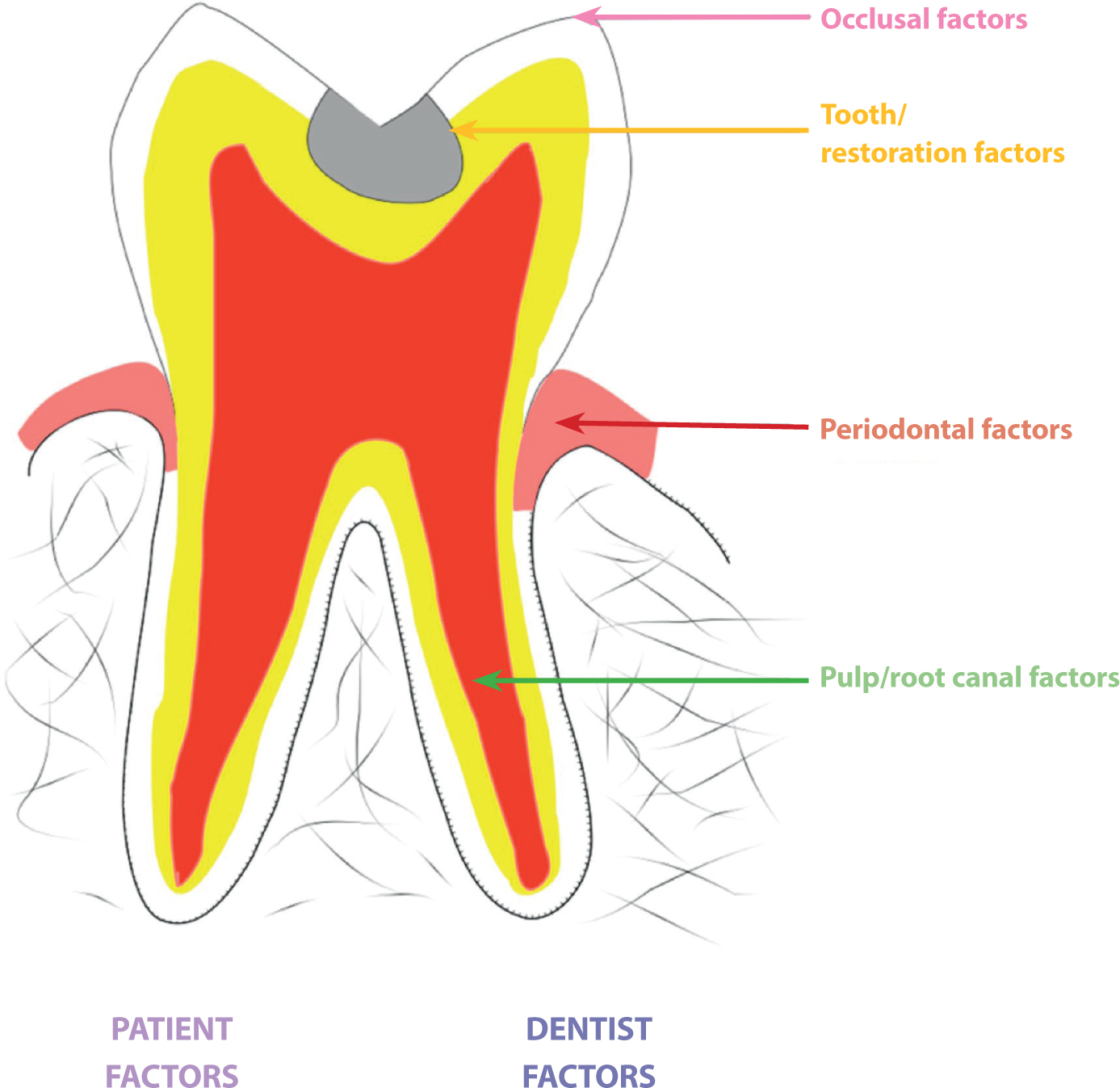
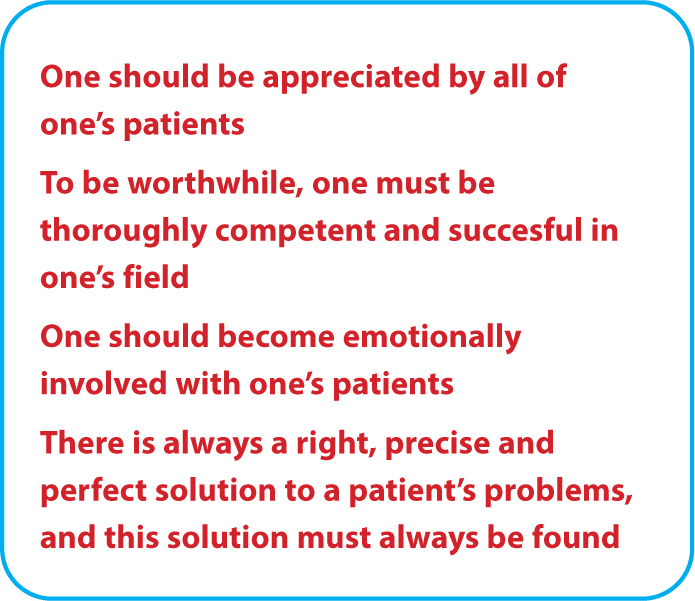
For any given tooth, there will be several aspects that should be considered when deciding on a care plan (Figure 2, Table 1). These patient factors can be the cause of much stress often based on incorrect assumptions by the practitioner, as indicated in Figure 3.
Figure 2. Factors that affect treatment options.
Table 1. Factors that affect treatment options.
Area
Factors
Example
Occlusal
Loading from opposing tooth or teeth in maximum intercuspation and lateral and protrusive excursions
Excessive force resulting in tooth wear and possible fracture of cusp
Lost mesiolingual cusp at lower left first molar and subgingival margin
Importance of tooth in the mouth for function/aesthetics
Depth of boxes in relation to the gingival margins and bone levels
Extent of caries
Extent of fracture/fracture lines
Marginal integrity
Periodontal
Plaque associated with the tooth and generally in the mouth
Periodontal condition beneath a bridge
Pocketing associated with the tooth and generally in the mouth
Bone levels associated with the tooth and generally in the mouth
Gingival margin level/s associated with the tooth and generally in the mouth
Mobility associated with the tooth and generally in the mouth
Pulp/root canal
Vital/non-vital
Sub-optimal root filling and post placement
Root canal morphology
Number of root canals
Existing root filling:optimal/sub-optimal
Apical status
Root fractures
Presence of post/posts
Dentist
Skill level
Know your limitations
Confidence to carry out procedures
Competence to carry out procedures
Rapport with patient
Adequate facilities/support
Available time for the treatment – now/future
Patient
Patient expectations
Emergency situations can be very stressful
Ability to cope with treatment
Time: availability/distance from practice
Cost: willing/able to pay
Attitude/response to preventive advice
General health/medications
Rapport with dentist
Figure 3. Incorrect assumptions about professionalism and caring.
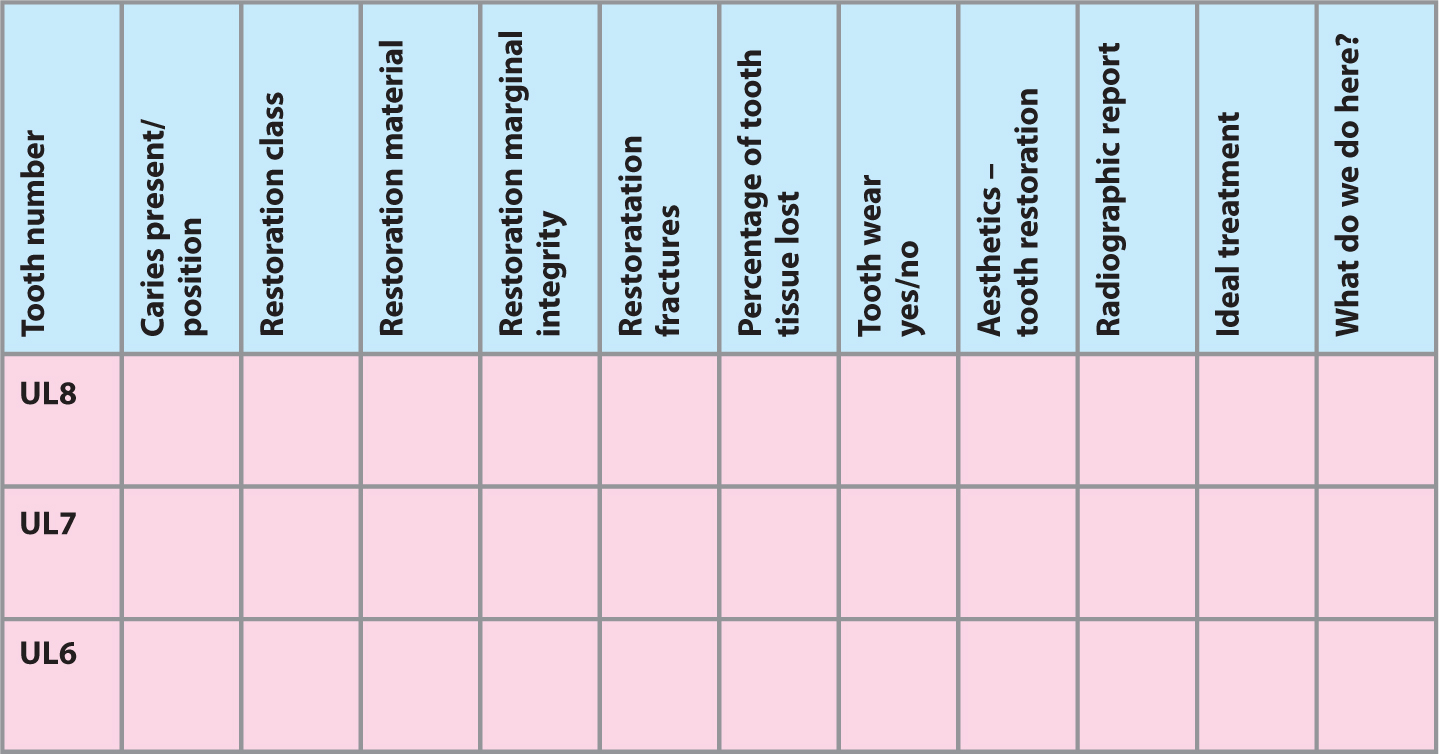
Bearing in mind these various factors, decisions have to be made, ranging from individual teeth to the whole mouth, and a chart such as shown in Figure 4 is very useful for recording the status of all teeth present in the mouth
Figure 4. Section of chart to record clinical observations for individual teeth and possible treatment.
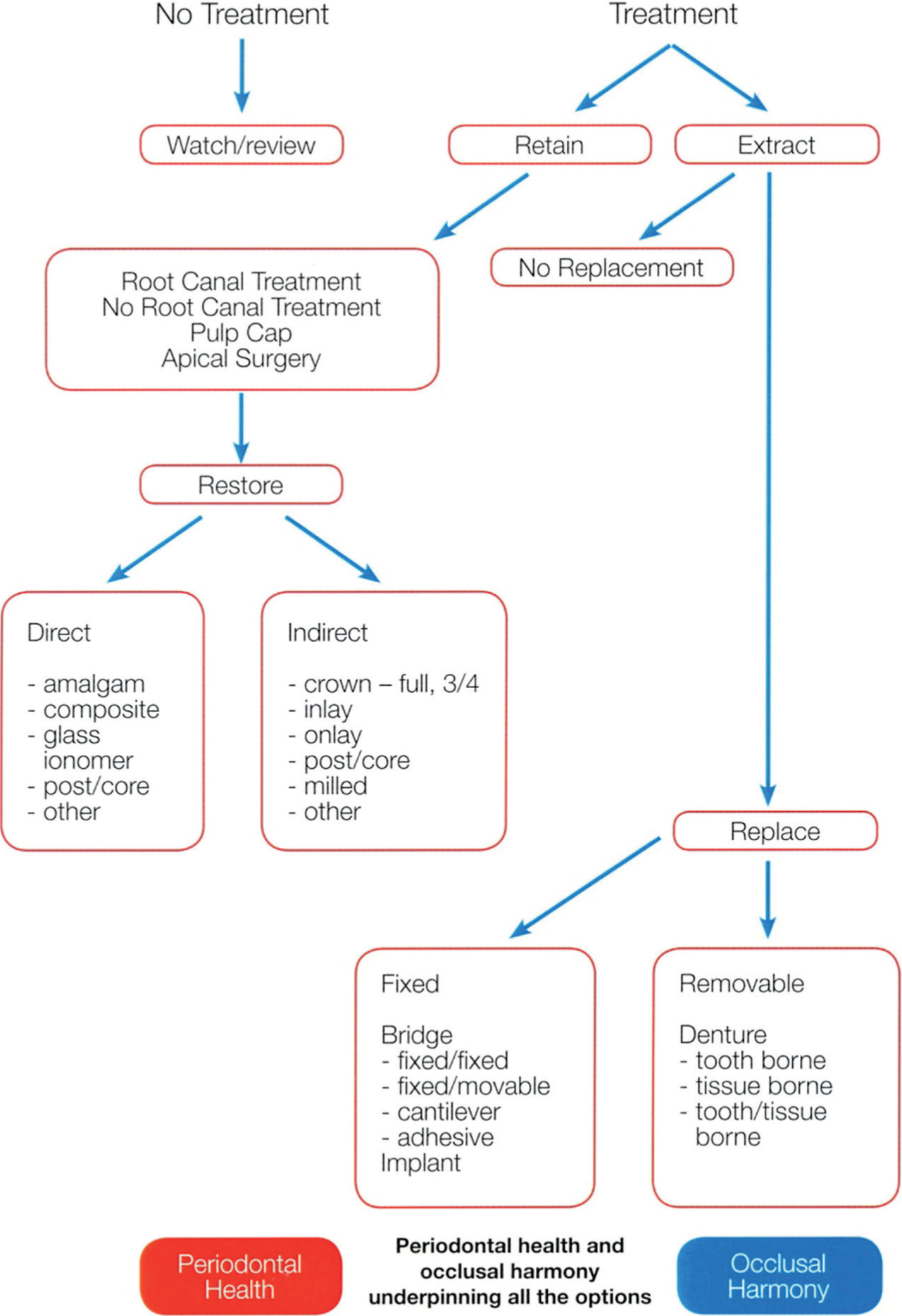
Context is an essential part of the care plan for either an individual tooth or the whole mouth. If it was possible to take the distressed tooth out of the mouth and the question asked ‘what would have to be done to restore this tooth to health and function’, the answer may be very different to the same question if that distressed tooth was placed back in the mouth because the factors mentioned above are critical components in the decision-making process. The care plan should enshrine the concept of ‘best guessing’ what treatment would be the most appropriate for ensuring longevity. We cannot know what will work best as there as so many factors that contribute to the success or failure of treatments, some of which can be predicted but many of which cannot be known.6 This needs to be discussed with the patient. There have been attempts to reduce the subjectivity in dental clinical decision making,7,8,9,10 but each situation and each practitioner is unique and so will give rise to the variations that are seen (Figure 5).
Figure 5. Flow chart for decision making in restorative dentistry.
The shortened dental arch
There also needs to be consideration as to the replacement of missing teeth. In the absence of aesthetic considerations, the concept of the shortened dental arch should be considered because patients can function well without the full complement of teeth and where attempts to replace them exposes the patient to greater risks than benefits.11,12,13 In 1992, the World Health Organization stated that a functional and aesthetic dentition requires no less than 20 well-distributed teeth.14
Varying the care plan
Where there is extensive dental and periodontal disease and/or occlusal disharmony, the care plan may have to be broken down into phases, each subsequent phase dependent on the success or not of the previous treatment and advice.
Immediate phase
This is to relieve pain, restore aesthetics, and comfort and is generally completed over a relatively short space of time.15
Intermediate phase
This is to deal with the factors that have led to the current state of poor oral health:
Diet analysis;
Temporary improvement of any restorations preventing good periodontal health;
Oral health advice alongside periodontal treatment;
Occlusal adjustment.
Definitive treatment should not be undertaken until the practitioner is satisfied that the patient can maintain a good level of oral health, otherwise there will be the continuing cycle of drill, fill and bill!
The aim should be to have the patient reduce their plaque score to 10%, the reduction of pockets, and to eliminate any sites of periodontal bleeding. This phase can last several months, even a year or more, working with the patient to eliminate those factors that have brought them to their current state of poor oral health. That is why it is prudent not to provide definitive restorations, such as indirect restorations, if they are going to be inserted into a disease-producing environment (Figure 6).
No plaque = No caries or periodontal disease
Figure 6. Stable and maintainable periodontium achieved over 1 year.
Final phase
The care plan will now be dependent on how well the toxic environment has changed. With good oral health and hygiene practices, the patient can be offered all the options in Figure 5 with a degree of confidence that there will be longevity for any restorative treatment undertaken. Should there be anything less than this, the practitioner should think carefully about prescribing indirect restorations that are expensive in terms of both tooth tissue loss and cost, because if nothing changes, nothing will change. That is, it is necessary to break the cycle that has brought the patient to their current state (Figure 7).
Figure 7. We must study the present in the light of the past for the purposes of the future (unknown).
Conclusion
Each clinical situation is unique. Each dental practitioner is unique. Using knowledge, judgement, and experience in the clinical decision-making process a care plan can be drawn up that meets the needs and wants of the patient and at the same time does not conflict with the ethical, moral, and professional responsibility of the practitioner (Figure 8). The various options should be weighed carefully for their risks and benefits and a full discussion held with the patient. Full notes should be made. Although this takes time, there is no substitute for good contemporaneous records. The final agreed course of action should be based on rational thinking and not what seems like a good idea at the time. It should be justifiable to a third party should the need arise.