Brånemark PI, Hansson BO, Adell R Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand J Plast Reconstr Surg Suppl. 1977; 16:1-132
Hämmerle CH, Araújo MG, Simion M Osteology Consensus Group 2011. Evidence-based knowledge on the biology and treatment of extraction sockets. Clin Oral Implants Res. 2012; 23:(Suppl 5)80-82 https://doi.org/10.1111/j.1600-0501.2011.02370.x
Schulte W, Kleineikenscheidt H, Lindner K, Schareyka R Das Tübinger Sofortimplantat in der klinischen Prüfung [The Tübingen immediate implant in clinical studies]. Dtsch Zahnarztl Z. 1978; 33:348-359
Cosyn J, Eghbali A, De Bruyn H Immediate single-tooth implants in the anterior maxilla: 3-year results of a case series on hard and soft tissue response and aesthetics. J Clin Periodontol. 2011; 38:746-753 https://doi.org/10.1111/j.1600-051x.2011.01748.x
Raes F, Cosyn J, Crommelinck E Immediate and conventional single implant treatment in the anterior maxilla: 1-year results of a case series on hard and soft tissue response and aesthetics. J Clin Periodontol. 2011; 38:385-394 https://doi.org/10.1111/j.1600-051x.2010.01687.x
Cosyn J, Eghbali A, Hermans A A 5-year prospective study on single immediate implants in the aesthetic zone. J Clin Periodontol. 2016; 43:702-709 https://doi.org/10.1111/jcpe.12571
Kan JY, Rungcharassaeng K, Lozada JL, Zimmerman G Facial gingival tissue stability following immediate placement and provisionalization of maxillary anterior single implants: a 2- to 8-year follow-up. Int J Oral Maxillofac Implants. 2011; 26:179-187
Chen ST, Buser D Esthetic outcomes following immediate and early implant placement in the anterior maxilla—a systematic review. Int J Oral Maxillofac Implants. 2014; 29:(Suppl)186-215 https://doi.org/10.11607/jomi.2014suppl.g3.3
Tonetti MS, Cortellini P, Graziani F Immediate versus delayed implant placement after anterior single tooth extraction: the timing randomized controlled clinical trial. J Clin Periodontol. 2017; 44:215-224 https://doi.org/10.1111/jcpe.12666
Quirynen M, Vogels R, Alsaadi G Predisposing conditions for retrograde periimplantitis, and treatment suggestions. Clin Oral Implants Res. 2005; 16:599-608 https://doi.org/10.1111/j.1600-0501.2005.01147.x
Chappuis V, Engel O, Reyes M Ridge alterations post-extraction in the esthetic zone: a 3D analysis with CBCT. J Dent Res. 2013; 92:195S-201S https://doi.org/10.1177/0022034513506713
Kan JY, Rungcharassaeng K, Sclar A, Lozada JL Effects of the facial osseous defect morphology on gingival dynamics after immediate tooth replacement and guided bone regeneration: 1-year results. J Oral Maxillofac Surg. 2007; 65:13-19 https://doi.org/10.1016/j.joms.2007.04.006
Morton D, Chen ST, Martin WC Consensus statements and recommended clinical procedures regarding optimizing esthetic outcomes in implant dentistry. Int J Oral Maxillofac Implants. 2014; 29:(Suppl)216-220 https://doi.org/10.11607/jomi.2013.g3
Chen ST, Darby I The relationship between facial bone wall defects and dimensional alterations of the ridge following flapless tooth extraction in the anterior maxilla. Clin Oral Implants Res. 2017; 28:931-937 https://doi.org/10.1111/clr.12899
Cooper LF, Raes F, Reside G Comparison of radiographic and clinical outcomes following immediate provisionalization of single-tooth dental implants placed in healed alveolar ridges and extraction sockets. Int J Oral Maxillofac Implants. 2010; 25:1222-1232
Kohal RJ, Hürzeler MB, Mota LF Custom-made root analogue titanium implants placed into extraction sockets. An experimental study in monkeys. Clin Oral Implants Res. 1997; 8:386-392 https://doi.org/10.1034/j.1600-0501.1997.080505.x
Paolantonio M, Dolci M, Scarano A Immediate implantation in fresh extraction sockets. A controlled clinical and histological study in man. J Periodontol. 2001; 72:1560-1571 https://doi.org/10.1902/jop.2001.72.11.1560
Kan JY, Rungcharassaeng K, Morimoto T, Lozada J Facial gingival tissue stability after connective tissue graft with single immediate tooth replacement in the esthetic zone: consecutive case report. J Oral Maxillofac Surg. 2009; 67:40-48 https://doi.org/10.1016/j.joms.2009.07.004
Tarnow DP, Chu SJ, Salama MA Flapless postextraction socket implant placement in the esthetic zone: part 1. The effect of bone grafting and/or provisional restoration on facial-palatal ridge dimensional change-a retrospective cohort study. Int J Periodontics Restorative Dent. 2014; 34:323-331 https://doi.org/10.11607/prd.1821
Chu SJ, Hochman MN, Tan-Chu JH A novel prosthetic device and method for guided tissue preservation of immediate postextraction socket implants. Int J Periodontics Restorative Dent. 2014; 34:(Suppl 3)S9-S17 https://doi.org/10.11607/prd.1749
Szmukler-Moncler S, Piattelli A, Favero GA, Dubruille JH Considerations preliminary to the application of early and immediate loading protocols in dental implantology. Clin Oral Implants Res. 2000; 11:12-25 https://doi.org/10.1034/j.1600-0501.2000.011001012.x
Takeshita K, Vandeweghe S, Vervack V Immediate implant placement and loading of single implants in the esthetic zone: clinical outcome and esthetic evaluation in a japanese population. Int J Periodontics Restorative Dent. 2015; 35:715-723 https://doi.org/10.11607/prd.2494
Chen ST, Buser D Esthetic outcomes following immediate and early implant placement in the anterior maxilla – a systematic review. Int J Oral Maxillofac Implants. 2014; 29:(Suppl)186-215 https://doi.org/10.11607/jomi.2014suppl.g3.3
Gallucci GO, Hamilton A, Zhou W Implant placement and loading protocols in partially edentulous patients: A systematic review. Clin Oral Implants Res. 2018; 29:(Suppl 16)106-134 https://doi.org/10.1111/clr.1327
There are a number of protocols that the clinician has to consider when providing implant treatment. Immediate implant placement has its place in implant dentistry and should be considered following a strict case selection. This article discusses the factors that should be taken into account when planning and providing immediate implant placements, with an emphasis on achieving a good outcome. The evidence base is discussed with a description of the surgical stages involved and subsequent restoration. Cases to illustrate this technique and its limitations are presented.
CPD/Clinical Relevance:
Principles for single tooth implant replacement in the anterior maxilla, where aesthetic expectations are high are relevant to clinicians.
Article
Clinicians often encounter situations where dental extraction of a single tooth in the aesthetic zone is required. The objective in these cases is obtaining a successful aesthetic and functional outcome. The purpose of this article is to discuss the important aspects that need to be considered when selecting patients to undergo immediate implant placement. The indications and contraindications of immediate implant placement will be explored in detail to guide the dental practitioner on selecting appropriate cases. Moreover, this article describes the steps involved in adopting this technique from clinical examination, tooth extraction, immediate implant placement, temporization and definitive restoration.
Classifications
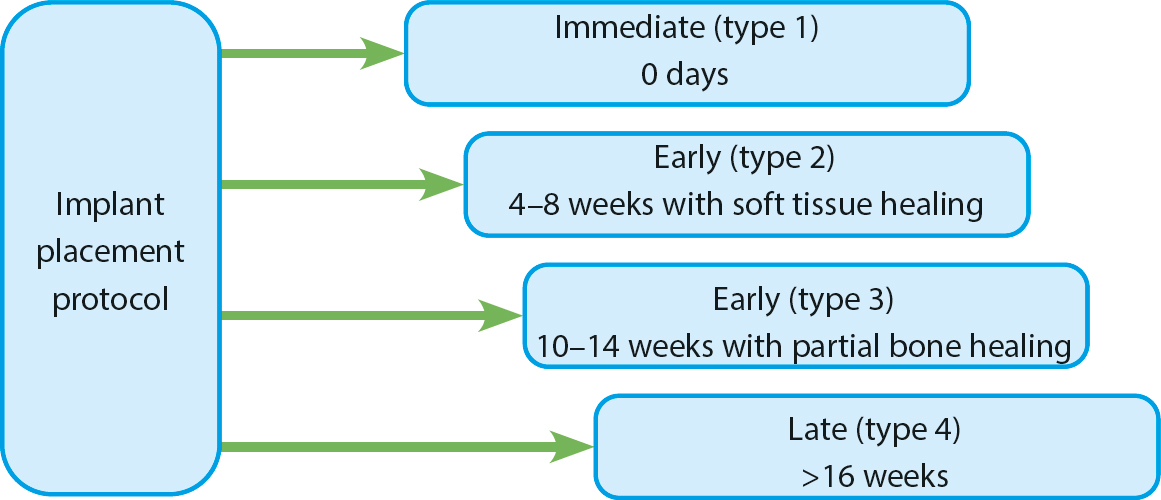
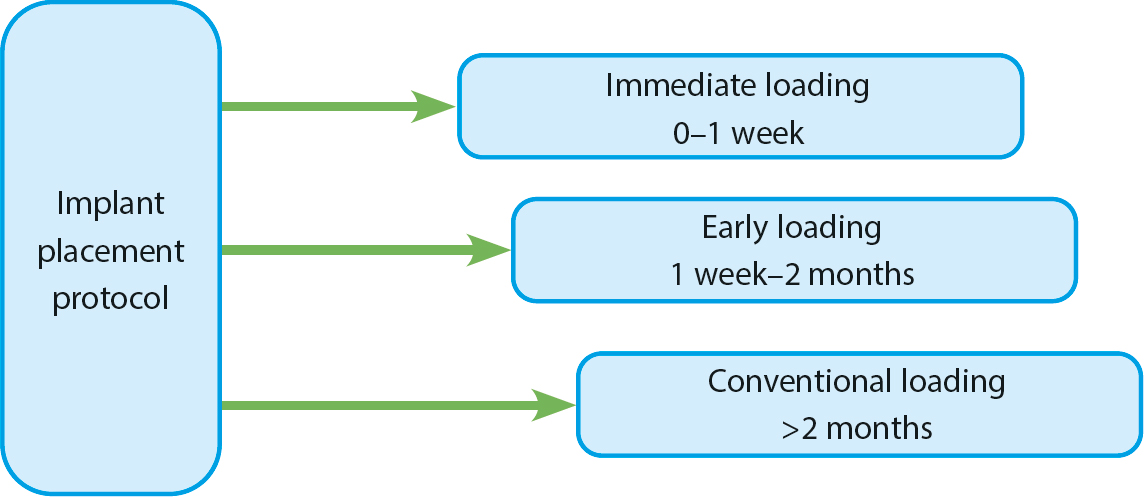
Four implant placement protocols have been introduced by the International Team of Implantology (ITI) outlining the timing of implant placement and loading protocols. ITI classifications are detailed in Figures 1 and 2 and Table 1.
All four implant protocols can be used in appropriate situations and they are favoured by different clinicians in varying circumstances. The early placement techniques (type 2 and 3) have been gaining popularity. The benefits of adopting these protocols are:
Soft tissue coverage of the socket occurs, resulting in additional keratinized mucosa and soft tissue thickening with normal healing. This is helpful in areas where buccal bone defects or a thin tissue biotype is present. The need for soft tissue grafting is reduced.
Easier osteotomy at the implant site owing to the formation of new bone, especially in the apical portion. This has to be balanced against a more difficult flap elevation.
The risk of post-surgical infection is reduced in cases where acute infection or fistula is present at the extraction site.
Historically, implants were mainly placed using a late placement approach (type 4) in healed sites, commonly with placement 6 months after extraction.1 It has been demonstrated that the average horizontal and vertical alveolar bone loss in the extraction socket is 3.8 mm and 1.24 mm, respectively, during a 6-month post-extraction period.2 This can significantly reduce bone volume in the implant site when prolonged healing times are considered. However, should a late placement protocol be indicated, ridge preservation could be considered to prevent the anticipated bone resorption. Two of the authors have carried out implant placement for over 35 years and have favoured immediate placement or delayed placement at about 4 months post-extraction to provide good outcomes. In some delayed placements, localized bone augmentation may be required. The authors prefer to place implants in normal alveolar bone rather than a grafted site, or one with a mix of healing soft tissue and bone.
History of immediate implant technique
Immediate implant placement procedures have been practised since 1978. Professor Wilfried Schutle from Germany was the first to document immediate implant placement.3 Nowadays, this treatment modality is frequently considered in cases where a single tooth in the aesthetic zone requires extraction, or replacement of primary teeth is planned. The technique is more challenging when used to replace a multi-rooted tooth, especially when the alignment of roots is unfavourable. Indications and contraindications of placing immediate dental implants are listed in Table 2. The advantages of placing immediate implants include:
Fewer surgical interventions;
Reduction in treatment time;
Lower pain and morbidity;
Psychological benefits to the patients, who might find it difficult to accept being ‘toothless’ following the extraction of a natural tooth;
Good cost-effectiveness;
Preserves papilla; however, possible mid-facial recession can occur.
Indications
Contraindications
Single-rooted tooth (multi-rooted teeth more difficult)
Severe recession
Primary canines and molars
Acute infection
Thick buccal bone morphotype
Thin buccal bone morphotype
Thick gingival phenotype
Thin gingival phenotype
Availability of apical and palatal bone to obtain primary stability
Severe periodontal disease
Intact socket walls
Tooth ankylosis/difficult extraction
Risks associated with immediate implant placement
The aim of the implant treatment provided to patients should be focused on the provision of predictable and successful long-term outcomes, while minimizing the risks to which patients are subjected. Some studies showed promising positive aesthetic soft and hard tissue outcomes associated with immediate implant placement in the anterior maxilla of carefully selected cases.4,5 Others, however, showed negative aesthetic outcomes.6,7
Some studies have observed an increased risk of soft tissue recession with immediate implants.8 Tonetti et al9 highlighted that pink aesthetics can be inferior compared to a delayed implant placement approach. These potential adverse aesthetic outcomes can be minimized by following the strict selection criteria outlined below.
Operator experience may be a key factor in the success of immediate implants. All dentists should feel confident in straightforward implant placement before attempting immediate placements. If dentists have not been trained in this technique, they will benefit from mentoring in their first few cases.
Selection criteria
It is important for the clinician to assess the patient's risk profile as a whole and for the tooth. Therefore, besides the medical and social risk factors, a detailed examination of the tooth to be extracted is considered a fundamental step in the planning process. The key factors to consider during the decision-making process are as follows.
Endodontic status
Ideally, there would be no endodontic pathology to complicate implant planning. However, teeth with limited endodontic involvement, such as chronic apical periodontitis, root resorptive defects, root perforation or fractures, may still be suitable for immediate implants. Nonetheless, it is important to appreciate that chronic infection might result in the loss of labial plate bone. Root fracture, tooth ankylosis and post crowns might lead to difficult dental extraction, resulting in excessive bone removal.
Acute infections should be cleared before surgery. The endodontic status of adjacent teeth is important to consider prior to implant placement.10
Periodontal status
The tooth should have good periodontal support. The following factors are to be considered for successful outcomes.
Thick gingival phenotype
Patients with thick gingival phenotype will be at reduced risk of marginal soft tissue recession. It is important to appreciate that the majority of the soft tissue in the anterior maxilla is found to be thin.11
Thick buccal bone plate (thick bone morphotype)
This is difficult to assess, even with a cone beam CT scan (CBCT). The presence of a thick (>1 mm) buccal bone plate reduces the risk of resorption.12 Thin buccal bone a tends to resorb in a corono-apical direction three times more than thick bone.13 In situations where a graft material is used with a thin buccal plate, the graft material will no longer be contained once the buccal bone plate resorbs post-extraction. This can result in loss of graft and soft tissue volume.
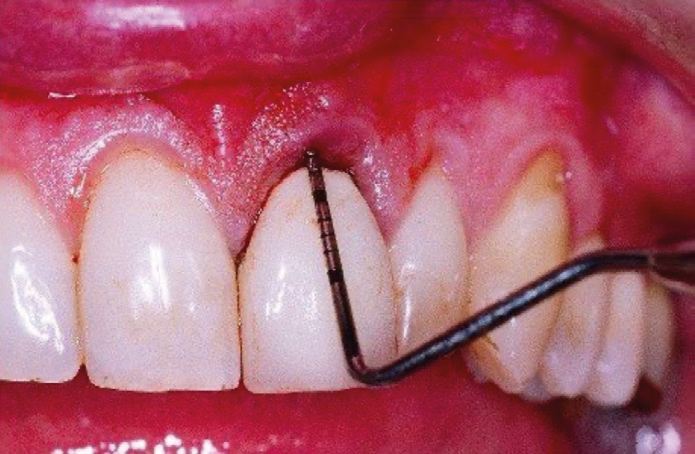
Intact buccal bone and absence of recession
There is a general consensus that severe buccal bony defects in the extraction site preclude using an immediate implant technique (Figure 3). The lack of a buccal bone wall is often associated with increased gingival recession.14 The greater the bone dehiscence, the greater the soft tissue recession will be. The labial plate can be palpated with a probe after an extraction.
Figure 3. Deep probing depth indicating labial bone defect.
Availability of adequate palatal and apical bone to acquire good primary stability of the implant
Anatomical structures, such as the nasal/sinus floor and inferior dental neuromuscular bundle, reduce available apical bone for primary stability. Approximately 5 mm of the osteotomy site should be intact to allow for good stability. This is usually bone apical to the tooth socket, but can involve the socket if the root was tapered.
When these key factors are absent, the clinician should consider a delayed approach.15 It is important to note that in some cases, the buccal bone plate will not be intact.16 Cooper and colleagues17 reported that 21% of sites planned to receive immediate implant placement were abandoned owing to the significant bone loss when teeth were extracted. This possibility should be explained to the patients at the outset.
Technique
Standard implant treatment planning is required, in common with standard implant placement. The aesthetic demands of the patient need to be assessed with attention to smile design, and possibly an aesthetic try-in. In most cases, CBCT scans are considered helpful in assessment. They can be used to measure the presence and volume of apical bone, plan implant angulation and sometimes assessment of thickness and quality of buccal bone of the extraction site. It is important to note that CBCT scans can suggest the buccal plate to be thin or absent, which can sometimes be misleading.
Surgical steps associated with dental extraction and immediate implant placement
Step 1: Flapless surgery
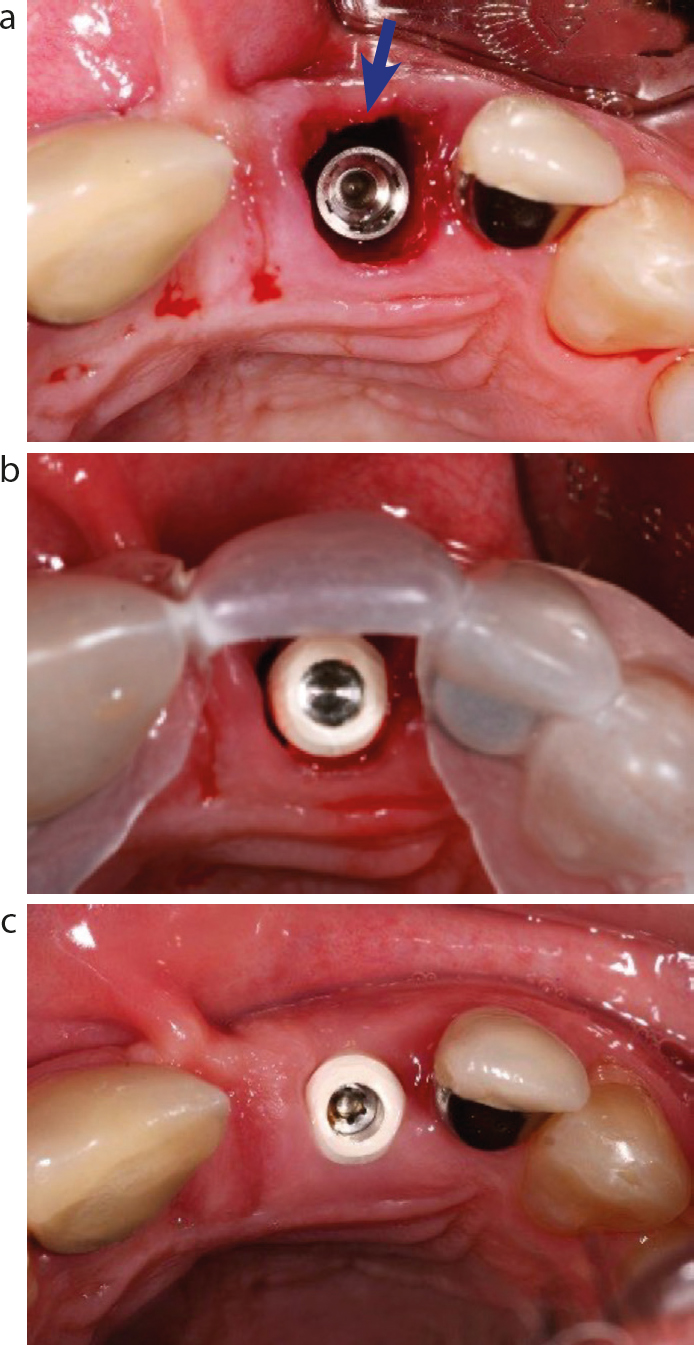
This approach has more predictable outcomes when compared with the open-flap technique (Figures 4,5,8–10). Flapless surgery is associated with less risk of buccal soft tissue recession5 owing to the maintenance of the blood supply that would otherwise be disrupted during periosteal elevation when a flap is raised. The authors advocate a flapless approach, when possible.
Figure 4.
(a) Immediate implant placement UL1 site using the flapless approach. The blue arrow highlights the 2-mm marginal gap. (b) A surgical guide used for implant placement UL1. Healing abutment in situ. (c) Healing around UL1 healing abutment 1 week after surgery. Temporary replacement was provided using a maxillary acrylic partial denture.Figure 5.
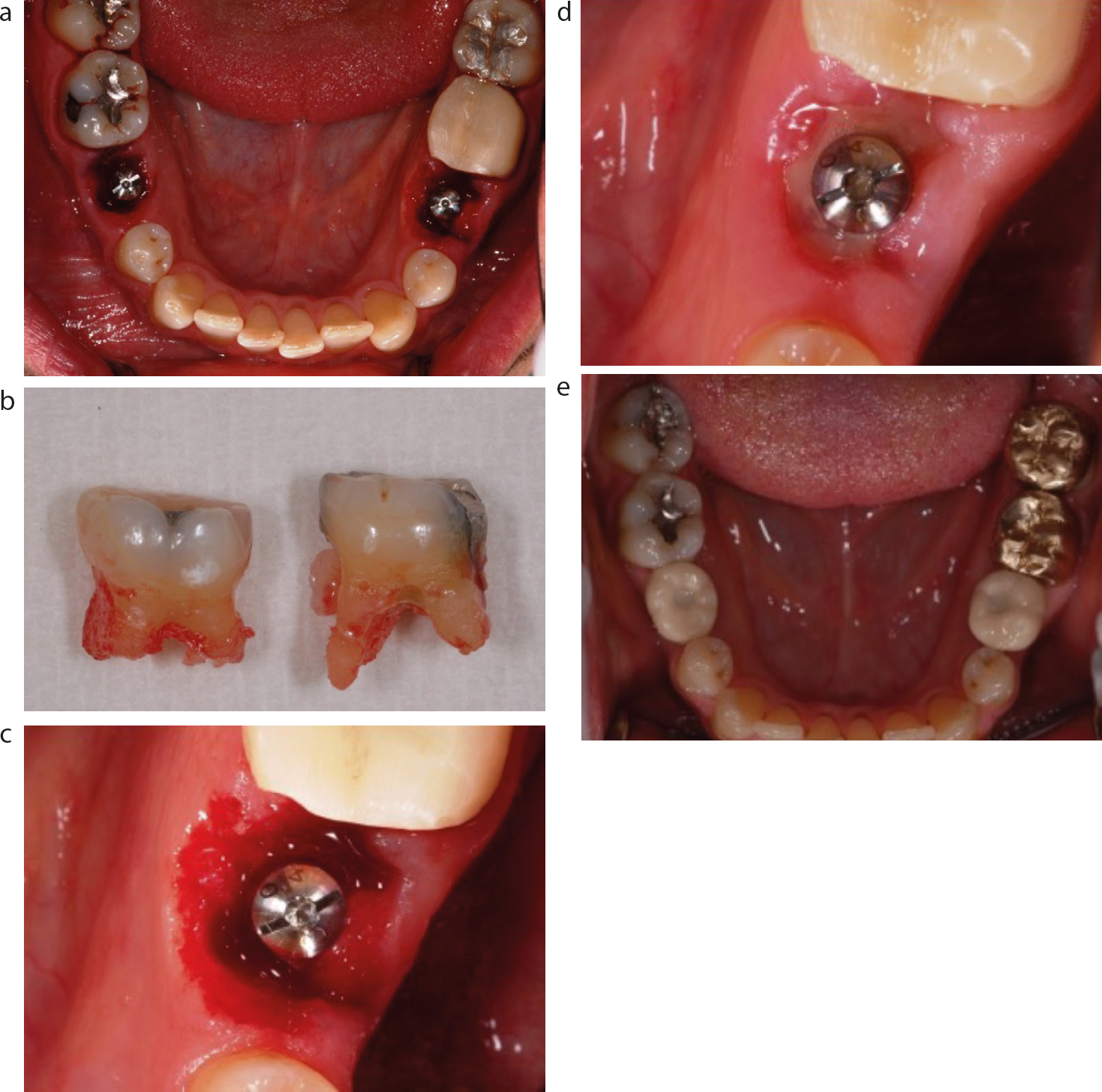
(a) Immediate implant placement LR5 and LL5 following extraction of LRE and LLE. (b) Extracted LRE and LLE. (c) Immediate implant placement LL5 in the middle of the extraction socket. (d) Soft tissue healing around LL5 immediate implant 1 week following treatment with healing abutment in situ. (e) Occlusal view of definitive implant-supported screw-retained porcelain-fused-to-metal crowns replacing the LR5 and LL5 (E size).Figure 6.
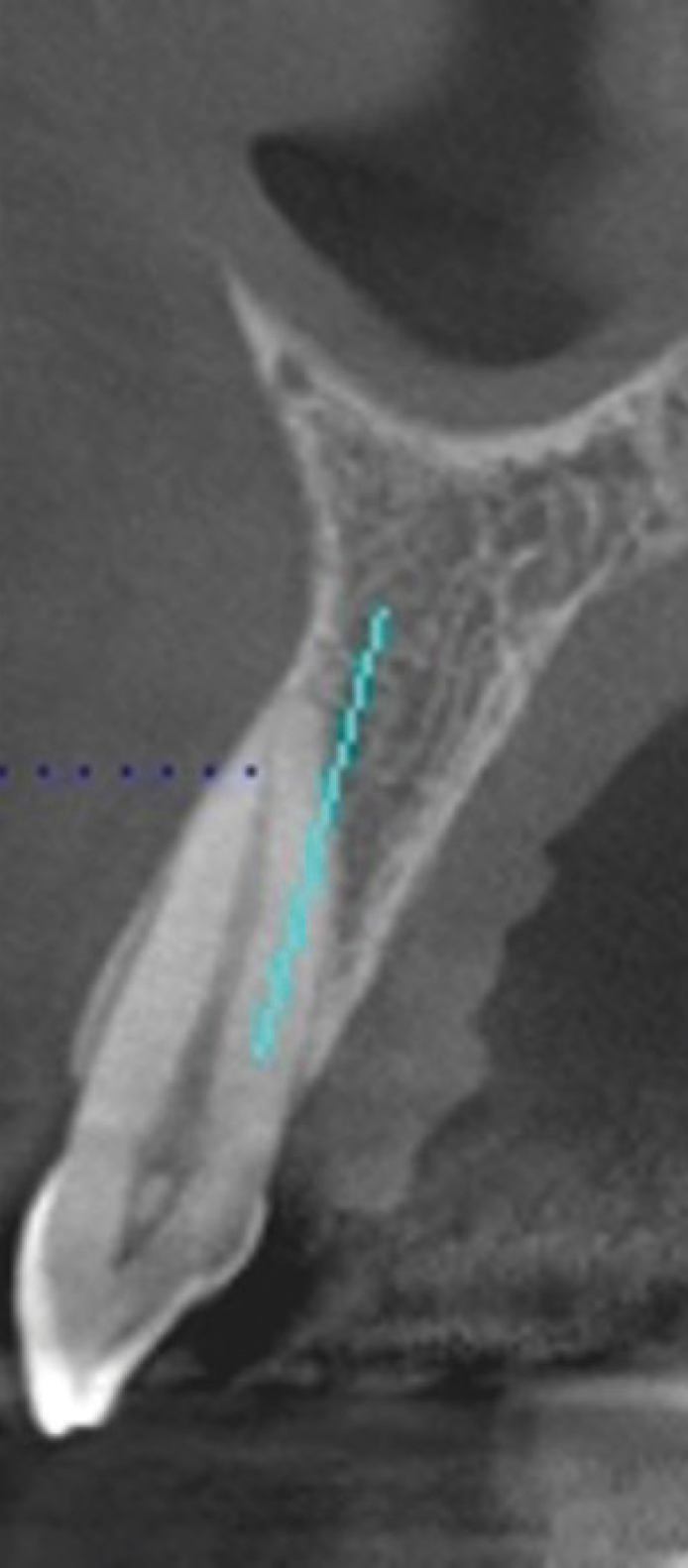
(a) Periotome used to sever the periodontal ligament of UL2. (b) Luxators can be used for the extraction of UL2. (c) Socket of the extracted UL2 and dismantled UL3 crown. (d) Full muco-periosteal flap raised and immediate implant placement UL2 site. A flapless surgical approach is preferred. (e) Provisional conventional bridge cantilevered from UL3 tooth. Forces on the UL2 implant should be controlled and eliminated. (f) Radiographic image of the implant with abutment for a cemented crown UL2. A screw-retained crown is preferred today. (g) Definitive implant-supported crown UL2 and conventional crown UL3.Figure 7. CBCT scan illustrating the planned apical-palatal positioning (blue line) of an immediate implant. The osteotomy site is placed on the palatal aspect of the socket wall near, but just superior to, the apex.Figure 8.
(a) Failed UR1 post-crown restoration. (b) Radiographic image of failed UR1 post crown and absence of endodontic treatment. A vertical crack was present. (c) UR1 extraction socket. (d) Osteotomy site UR1 was prepared using a 2-mm twist drill using the palatal bone. (e) Direction indicator at UR1 osteotomy site. (f) Osteotomy completed, and the implant is being installed at UR1 site. (g) The bone level implant is positioned at the UR1 site so that the fixture head is just apical to the labial bone crest and a 2-mm marginal gap is present. (h) A temporary cylinder used to make a temporary crown. (i) Temporary screw-retained crown in place. (j) 3 months postimplant placement at UR1 site prior to impression making for definitive implant-supported crown construction. (k) Definitive implant-supported crown UR1 with optimal white and pink aesthetic results. (l) Radiographic image of the definitive implant-supported crown UR1.Figure 9.
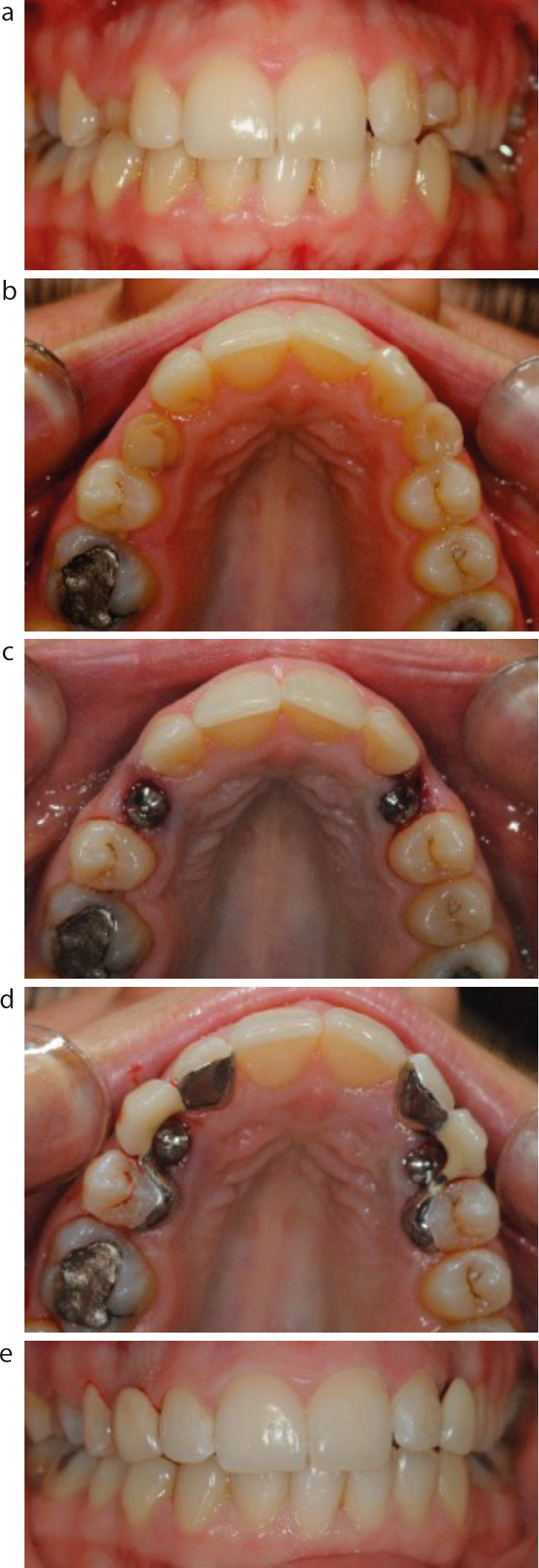
(a) Hypodontia of the UR3 and UL3 with retained URC and ULC. (b) Occlusal view of the retained URC and ULC. (c) Immediate implant placement UR3 and UL3 utilising a flapless approach. (d) Provisional fixed-fixed resin-retained bridges replacing the UR3 and UL3. RRBs are designed for easy removal. (e) Frontal view of provisional resin-retained bridges replacing the UR3 and UL3.Figure 10.
(a) Frontal view of failing maxillary dentition. (b) Occlusal view of failing UR12, UL12 teeth and retained roots of the UL34. (c) Standard implant placement UR35, and flapless immediate implant placement of the UR1, UL134. (d) Healing at 3 months prior to impressions. Second stage surgery was carried out in the UR53 area. (e) Maxillary full-arch definitive implant-supported bridge. (f) Frontal view of the maxillary full-arch definitive implant-supported bridge. The gingival replacement was contoured to allow effective interdental cleaning.
In some situations, a flap must be raised (Figure 6) to facilitate tooth extraction or a graft to repair minor bony defects. This can also facilitate the identification of any buccal plate perforation and aid implant angulation.
Step 2: Extraction
It is of paramount importance to avoid unnecessary trauma to the socket during the tooth removal, and minimize damage to the alveolus. This is to prevent the fracture and the loss of buccal and/or palatal plates or the undue compression on the walls, risking future necrosis. Difficult root morphology and curvatures can lead to traumatic dental extractions, which can preclude subsequent immediate implant placement.
The use of luxators and periotomes (Figure 6) to carefully loosen the tooth and sever the periodontal ligaments is helpful. These are to be used on the mesial, distal and palatal or lingual aspects of the root. Small labial plate fractures are less critical if the periosteum is intact. Should extraction forceps be used, maintaining apical force while carrying out rotational movements, particularly for upper central incisors, will reduce trauma to tooth sockets. Piezo-electric tips, which give superior control in terms of force and adaptability to the roots’ shape, could also be used for this purpose but can be time-consuming. The socket should be adequately curetted of any soft tissue if present. Another way of preserving the buccal cortical bone is the socket-shield technique, originally described by Hürzeler et al.18 This technique involves preserving the buccal aspect of the root while extracting the rest of it, followed by implant placement. The authors have not used this technique.
Step 3: Immediate implant placement
An increased primary stability is achieved by incorporating the palatal and lateral bone and using any bone available apical to the tooth socket. Ideally, this bone should be 4–5 mm long (Figures 7 and 8). If sufficient apical bone is unavailable, a delayed placement approach might be more appropriate. Implant placement directly in the extraction socket should avoid buccal plate perforation, which can lead to inferior primary stability and aesthetic outcomes.19 Therefore, the osteotomy in upper anterior teeth, for example, should be initiated by engaging the intact apical third of the palatal wall of the extraction socket. Drilling into the palatal tooth socket wall can be challenging, and the bur can slip unless firm guidance with a small round bur or a lance drill is used. Perforation of the palatal socket wall at about 120 degrees to the long axis of the socket should be followed by re-angulation to the desired osteotomy angulation.
A standard drilling sequence following the manufacturer's instructions should be followed. Optimal positioning and angulation of the drills can be facilitated by using tooth-borne surgical templates (Figure 4b) fabricated from the preextraction or diagnostic wax-up. Using the surgical guide will aid the positioning and alignment of the fixture to allow for a screw-retained restoration. Small departures from ideal placement can be managed at the prosthetic stages with some form of angle correction. Primary stability is a key factor in the success of immediate implants.
Maintaining a marginal gap of at least 2 mm between the coronal internal socket wall and the shoulder of the implant platform (Figures 4a and 8g) is recommended.20 This will reduce the amount of buccal bone resorption that will inevitably take place following the tooth extraction. It is anticipated that this gap will eventually be filled with bone as part of bone healing and osseo-integration.21 The gap will also facilitate the formation of the blood clot and provide a provisional connective tissue matrix in most cases. This space is also important if bone substitutes are used, which will eventually transform into regenerated bone. Should the gap be less than 2 mm wide, the formation of the provisional matrix will be affected, resulting in less thickness of the regenerated buccal bone. Food impaction in the marginal gap should be avoided.
This can be prevented by a temporary replacement, such as a partial denture, bridge, provisional implant-supported crown or healing abutment. On occasion, a periodontal dressing could be used.
The shoulder, or fixture head, of the implant placed, should be 0.5–1-mm apical to the buccal bone crest (Figure 8g). The fixture head should be in the palatal side of the socket, as guided by the surgical template, and is often slightly subcrestal relative to the proximal and palatal bone crests. This is to compensate for the vertical buccal bone and soft tissue resorption that may take place.
Buccal soft tissues can be supported by a connective graft harvested from the palate and inserted into the internal aspect of the facial bone to support the soft tissue.22 This is to compensate the anticipated horizontal buccal bone resorption. Another technique described by Tarnow et al23 is to use a very small particle bone substitute to graft the defect and coronal to the buccal bone crest into the soft tissue zone (dual zone technique), thereby, maintaining adequate soft tissue thickness. However, the authors have not used adjunctive soft or hard tissue grafting with acceptable results (Figures 4 and 8).
Step 4: Temporization following immediate implant placement
It is best to avoid subjecting the implant to any occlusal load while bone healing and osseo-integration take place. Hence, delayed loading with temporization of the extraction site using conventional methods, such as removable or fixed replacements, is advised. A partial denture or vacuumformed retainer that contains an acrylic/composite tooth replacement of the extracted tooth, should be trimmed adequately to avoid loading of the healing abutment. Another option is to provide an immediate provisional fixed resin-retained bridge (Figure 9d) or a provisional conventional bridge (Figure 6e). However, when treating patients with high aesthetic demands, these options might not be acceptable. Therefore, providing a provisional implant-supported restoration at the time of placement (type 1A protocol) might be required. This allows the peri-implant soft tissue to be shaped adequately around the implant24 should it achieve sufficient primary stability (torque 25–40N). The occlusion should be arranged so the provisional implant crown is not loaded.
Step 5: Loading
Implant placement and the loading protocol should be planned prior to tooth extraction. Studies have suggested that minimal movement of the implant during the osseo-integration phase can be withstood without adversely affecting the healing process. These movements should be less than 50 microns.25 Consequently, the restoration should be out of contact during the mandibular lateral excursive and protrusive movements to minimize the risk of osseo-integration failure.
Immediate and early loading (type 1A and type 1B)
Immediate loading of implants placed in fresh sockets showing good clinical outcomes have been reported26 when disclusion of the provisional restoration during function is obtained. However, Chen et al27 indicated a higher risk of gingival recession associated with immediate loading of immediate implants.
Delayed (conventional) loading (type 1C)
A systematic review conducted by Gallucci and colleagues28 concluded that delayed loading of an immediate implant is the only validated approach compared to immediate and early loading approaches. Delayed loading is advised in situations where a flap needs to be raised (to facilitate tooth extraction or graft to repair the minor bony defect) is required. Moreover, a delayed loading protocol should be adopted when the primary stability of the implant is not optimal and when bone augmentation is undertaken. The authors favour a delayed loading protocol.
Step 6: Definitive restoration
Definitive restoration can be provided within 2–3 months in keeping with most standard protocols. The palatal position of the immediate implant facilitates the provision of a screw-retained implant-supported crown, which is the preferred type of restoration. This is especially true when peri-implant health is considered. Provisional restorations can help develop soft tissue contours, but in many cases, are not required. A definitive restoration made to the ideal contour will blanch the peri-implant tissues on insertion. So long as this blanching from pressure resolves during the appointment, the outcome will be good. Persistent blanching would require adjustment to the emergence profile. With careful treatment planning, multiple immediate implants can be placed and restored (Figure 10). The clinical outcome is in keeping with other treatment protocols if provided in this way (Figure 11).
Figure 11.
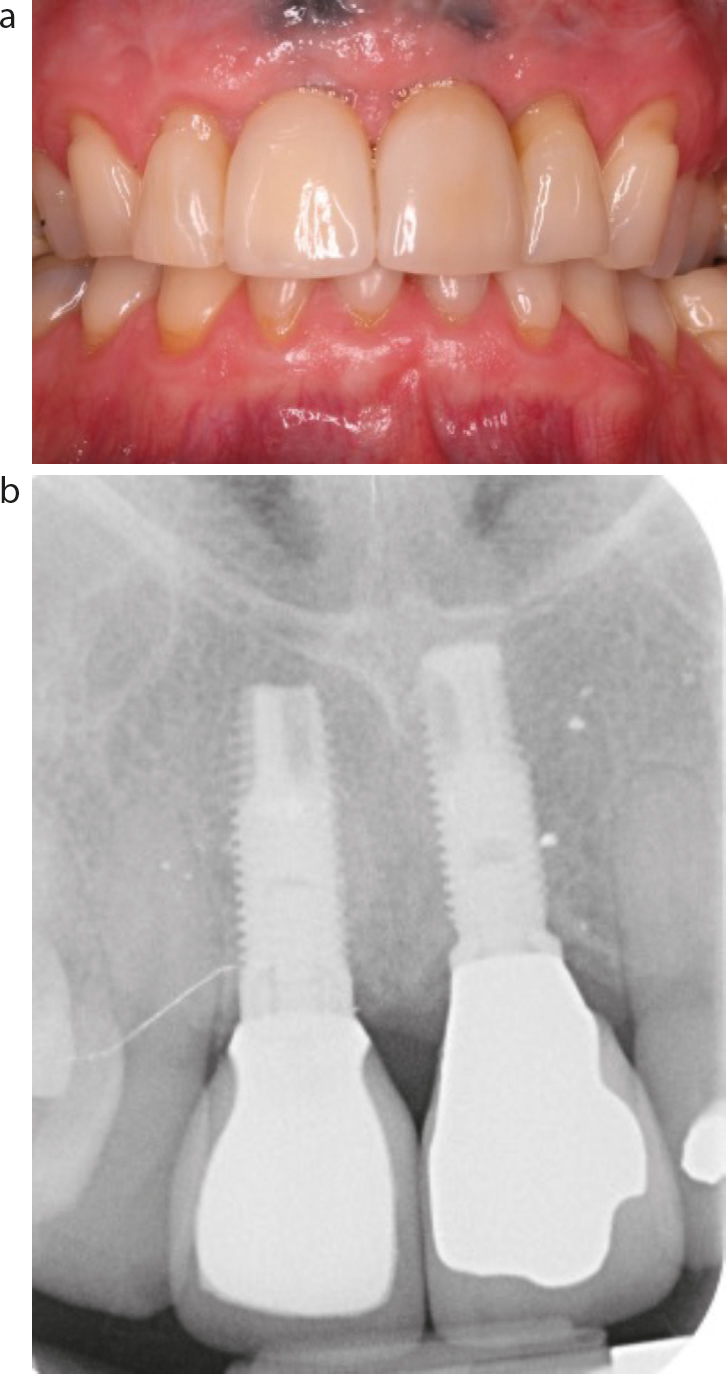
(a) Immediate implants UR1 and UL1 after 6 and 10 years, respectively. (b) Immediate implants UR1 and UL1 after 6 and 10 years, respectively, radiographic view. Two different implant systems were used for UR1 and UL1, Neoss (Sweden) and Nobelbiocare (Switzerland), respectively.
Conclusion
Immediate implant placement has its place in implant dentistry and should be considered in suitable cases. The placement of immediate implants requires appropriate training and experience to perform successfully. A flapless surgical procedure is preferred to avoid recession of the facial gingival margin. Patients appreciate the reduced surgical morbidity, time and cost. Factors for success include the absence of acute infection and recession, presence of an intact buccal socket wall, adequate apical bone volume and thick gingival phenotype. A standard delayed placement protocol should be followed if the clinical situation is not ideal.