Feloutzis A, Lang NP, Tonetti MS, Burgin W, Bragger U, Buser D IL-1 gene polymorphism and smoking as risk factors for peri-implant bone loss in a well-maintained population. Clin Oral Implants Res. 2003; 14:(1)10-17
McDermott NE, Chuang SK, Woo VV, Dodson TB. Complications of dental implants: identification, frequency, and associated risk factors. Int J Oral Maxillofac Implants. 2003; 18:(6)848-855
Tjan AH, Miller GD., The JG. Some esthetic factors in a smile. J Prosthet Dent. 1984; 51:(1)24-28
Cairo F, Pagliaro U, Nieri M. Soft tissue management at implant sites. J Clin Periodontol. 2008; 35:(8 Suppl)163-167
Wilson DJ. Ridge mapping for determination of alveolar ridge width. Int J Oral Maxillofac Implants. 1989; 4:(1)41-43
Allen F, Smith DG. An assessment of the accuracy of ridge-mapping in planning implant therapy for the anterior maxilla. Clin Oral Implants Res. 2000; 11:(1)34-38
Luk LC, Pow EH, Li TK, Chow TW. Comparison of ridge mapping and cone beam computed tomography for planning dental implant therapy. Int J Oral Maxillofac Implants. 2011; 26:(1)70-74
Olsson M, Lindhe J. Periodontal characteristics in individuals with varying form of the upper central incisors. J Clin Periodontol. 1991; 18:(1)78-82
Olsson M, Lindhe J, Marinello CP. On the relationship between crown form and clinical features of the gingiva in adolescents. J Clin Periodontol. 1993; 20:(8)570-577
Tarnow DP, Magner AW, Fletcher P. The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. J Periodontol. 1992; 63:(12)995-996
Choquet V, Hermans M, Adriaenssens P, Daelemans P, Tarnow DP, Malevez C. Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retrospective study in the maxillary anterior region. J Periodontol. 2001; 72:(10)1364-1371
Schropp L, Wenzel A, Kostopoulos L, Karring T. Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodont Restor Dent. 2003; 23:(4)313-323
Tarnow D, Elian N, Fletcher P, Froum S, Magner A, Cho SC Vertical distance from the crest of bone to the height of the interproximal papilla between adjacent implants. J Periodontol. 2003; 74:(12)1785-1788
Gastaldo JF, Cury PR, Sendyk WR. Effect of the vertical and horizontal distances between adjacent implants and between a tooth and an implant on the incidence of interproximal papilla. J Periodontol. 2004; 75:(9)1242-1246
Lee DW, Park KH, Moon IS. Dimension of interproximal soft tissue between adjacent implants in two distinctive implant systems. J Periodontol. 2006; 77:(6)1080-1084
Chiapasco M, Zaniboni M, Boisco M. Augmentation procedures for the rehabilitation of deficient edentulous ridges with oral implants. Clin Oral Implants Res. 2006; 17:136-159
Siebert JS. Reconstruction of deformed, partially edentulous ridges, using full thickness onlay grafts. Compend Contin Educ Dent. 1983; 4:(1)437-453
Allen EP, Gainza CS, Farthing GG, Newbold DA. Improved technique for localized ridge augmentation. A report of 21 cases. J Periodontol. 1985; 56:(4)195-199
Cochran DL, Hermann JS, Schenk RK, Higginbottom FL, Buser D. Biologic width around titanium implants. A histometric analysis of the implantogingival junction around unloaded and loaded nonsubmerged implants in the canine mandible. J Periodontol. 1997; 68:(2)186-198
Hermann JS, Buser D, Schenk RK, Higginbottom FL, Cochran DL. Biologic width around titanium implants. A physiologically formed and stable dimension over time. Clin Oral Implants Res. 2000; 11:(1)1-11
Kim Y, Oh TJ, Misch CE, Wang HL. Occlusal considerations in implant therapy: clinical guidelines with biomechanical rationale. Clin Oral Implants Res. 2005; 16:(1)26-35
Rangert B, Krogh PH, Langer B, Van Roekel N. Bending overload and implant fracture: a retrospective clinical analysis. Int J Oral Maxillofac Implants. 1995; 10:(3)326-334
Siu AS, Li TK, Chu FC, Comfort MB, Chow TW. The use of lipiodol in spiral tomography for dental implant imaging. Implant Dent. 2003; 12:(1)35-40
Kim YK, Park JY, Kim SG, Kim JS, Kim JD. Magnification rate of digital panoramic radiographs and its effectiveness for pre-operative assessment of dental implants. Dentomaxillofac Radiol. 2011; 40:(2)76-83
Orentlicher G, Abboud M. Guided surgery for implant therapy. Dent Clin North Am. 2011; 55:(4)715-744
Harris D, Buser D, Dula K, Grondahl K, Haris D, Jacobs R EAO guidelines for the use of diagnostic imaging in implant dentistry. A consensus workshop organized by the European Association for Osseointegration in Trinity College Dublin. Clin Oral Implants Res. 2002; 13:(5)566-570
Grondahl H, Grondahl K. Radiographic examination of the implant patient, 5th edn. In: Lindhe J, Lang NP, Karring T (eds). Copenhagen: Blackwell Munksgaard; 2008
Weber H, Buser D, Belser UC. Examination of the candidate for implant therapy, 5th edn. In: Lindhe J, Lang NP, Karring T (eds). Copenhagen: Blackwell Munksgaard; 2008
Implant assessment Dean Barker Dental Update 2025 39:2, 128-134.
Authors
DeanBarker
BDS, DDS, FDS RCSEd, FDS(Rest Dent) RCSEd, FDTFEd
Consultant and Honorary Clinical Senior Lecturer in Restorative Dentistry, University of Aberdeen Dental School and Hospital, Cornhill Road, Aberdeen AB31 6NL, UK
Meticulous planning in implant dentistry is essential in order to achieve a predictable and successful outcome for both the operator and the patient. This paper summarizes the important aspects of planning, including factors related to clinical and radiographic examination and the use of study models.
Clinical Relevance: This paper has relevance to practitioners carrying out implant treatment and also to colleagues who are likely to refer patients for implants.
Article
Success in treating patients with implant-retained restorations is dependent on careful pre-operative assessment and planning. Implant therapy should not be seen as a single treatment modality and must be incorporated into a comprehensive treatment approach. This should begin with a careful evaluation of the patient's expectations, motivation and compliance for prolonged and costly treatment. A thorough history, including the reasons for tooth loss, medical history and social history are all essential.
Caution needs to be exercised in treating patients who have lost teeth due to uncontrolled caries or periodontal disease and even the cause of traumatic tooth loss must be considered. A competitor in a combat sport for example would be at high risk of sustaining further damage in the future.
Any medical condition or medication that may affect the surgical procedure or wound healing should be considered a relative contra-indication at least, but there are few absolute contra-indications. In all cases a risk:benefit assessment must be made. Similarly, smoking is a risk factor for implant failure and this is an even greater concern in patients with periodontitis.1,2 Many sources are available that consider the impact of various medical conditions and smoking on implant success and this will not be considered further in this paper.
Extra-oral assessment
Examination of the patient begins with an extra-oral assessment. A standard approach, including checking for any swellings of the head and neck region and palpation of the temporomandibular joints and musculature, is performed. Particular attention should be placed on the degree of mouth opening, as the instrumentation involved with various stages of implant therapy requires the patient to be able to open wide. This is especially true when considering the use of handpieces and screwdrivers in the area of the posterior dentition (Figure 1). Assessment of the smile line and how much gingival tissue is exposed should also be carried out. Problems in achieving a satisfactory aesthetic result can be anticipated by assessing how much of the teeth and gingival tissues are exposed.
Figure 1. The patient needs to be able to maintain sufficient mouth opening to allow instrumentation to be used, particularly in the posterior region of the mouth.
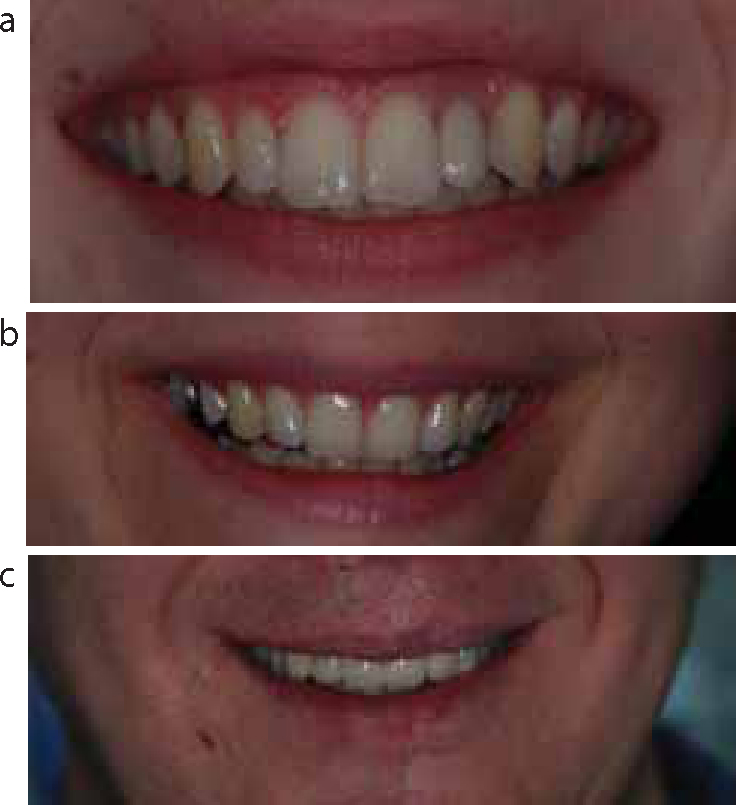
In 1984, Tjan et al classified smile lines as low, average and high (Figure 2).3 A low smile line reveals no gingival tissue and only around 75% of the teeth. An average, or level, smile reveals more of the teeth and the tips of the interdental papillae, while a high smile shows all of the teeth, interproximal papillae and buccal gingivae. This distribution of the three types is roughly 20%, 69% and 11%, respectively, but varies in relation to age, sex and ethnicity. Asking a patient to enunciate the letter ‘E’ in an exaggerated fashion gives a reasonably good estimate of the maximum dentogingival exposure. Similarly, a resting lip position can be achieved by asking the patient to say ‘m’ two or three times gently before allowing their lips to part.
Figure 2. Smile lines may be described as high when all the gingival margin is displayed (a), level when only the tips of the papillae are revealed (b) or low when no gingiva is shown (c).
Intra-oral assessment
An assessment of facial and dental asymmetry should also form part of the extra-oral assessment. Intra-orally, the gingival margin profile should be looked at in dentate patients when replacing teeth in the anterior ‘aesthetic zone’. In this circumstance, predicting the final gingival contour dictates the position and choice of implant, as well as the need for additional hard and soft tissue surgery. Soft tissues should also be assessed in respect to the amount of keratinized gingiva. The significance of a band of keratinized tissue around implants is controversial but it is generally felt to be of benefit with regard to maintenance.4 It is also possible to assess the thickness of the tissue by trans-gingival probing. This is done when ridge-mapping in order to gain an understanding of the underlying bone contour, often carried out with ridge-mapping calipers.5 However, this technique is becoming less commonly used with improvements in imaging and more predictable techniques for simultaneous guided bone regeneration. It has also been shown to be unpredictable, particularly when the labial bone face is concave and/or the ridge is resorbed.6,7
Examination of the soft tissues also includes an assessment of the patient's gingival architecture or phenotype, which is essential when planning restorations in the aesthetic zone of the anterior maxilla. Two major types have been described, namely ‘scalloped-thin’ (Type I) and ‘fat-thick’ (Type II).8,9 Scalloped-thin gingiva has a very contoured architecture with delicate tissues and long, pointed interdental papillae. It surrounds triangular-shaped crowns with small interdental contacts towards the incisal edge. It tends to react to surgery or prosthetic intervention with recession and can therefore be unforgiving of surgical technique. Fat-thick tissue, on the other hand, reacts to surgery and prosthetic insults with pocket formation, but resists recession. Square, bulbous crowns with long contact points are surrounded by dense fibrotic tissue.
Furthermore, in relation to papillae, the position of the bone crest relative to adjacent teeth must also be considered. In the natural dentition, where the alveolar margin is within 5 mm of the proposed contact point, it can be expected that a full papilla will reform after surgery. However, where this distance is around 6 mm, complete filling of the space by a papilla is only seen in 50% of cases and this drops further to around 25% when the distance is 7 mm or more.10 Specific work looking at implants adjacent to teeth has shown that papilla heights tend to be consistently around 4 mm and is dependent on the attachment level of the tooth.11 It must also be remembered that, when a single tooth is extracted, the height of the adjacent papilla is reduced by about 1mm.12
When more than one adjacent tooth requires replacement, the regeneration of interdental papillae becomes increasingly challenging, as the papilla between the teeth and the alveolar ridge crest between is often flattened. The height above the bone crest of the inter-implant soft tissue (‘implant papilla’) is typically 3.4 mm, with 90% of measurements between 2–4 mm.13 Furthermore, between implants, the ‘papilla’ only fills the entire space when the distance from the bone crest to the contact point of the restorations is <4 mm, as stated above.14 This distance is independent of the implant design.15
Following examination of the soft tissues, attention is then placed on the bone volume in the proposed implant site. Clearly, there needs to be enough bone to accommodate the implant. In the horizontal plane, at least 1 mm of facial and palatal bone over the implant is required to ensure stable hard and soft tissue outcomes. Where examination suggests the ridge is deficient in width, an assessment should be made with regard to augmentation in some form as indicated by the extent of the deficiency (Figure 3).16
Figure 3. A resorbed alveolar ridge may require to be augmented before an implant can be successfully placed.
Ridge deficiencies can be classified based on the type and amount of tissue loss.17,18 A Class I defect has loss of tissue buccolingually (horizontal), a Class II defect has apicocoronal (vertical) tissue loss, while a Class III defect is a combination of Class I and II and has a combination of horizontal and vertical loss. The amount of tissue loss can be described as mild (<3mm), moderate (3–6mm) and severe (>6mm).
The examination of any removable partial dentures the patient may present wearing can be a very useful guide to the degree of ridge resorption, particularly in a horizontal plane. A labial flange on a denture generally means that some labial bone loss has taken place, providing of course that it does not stand proud of the adjacent ridge. The thickness of the flange can signify the degree of resorption and its shape may reflect any bony undercuts present.
In addition to the volume of bone required to surround the implant, it must be ensured that there is adequate distance between the fixture and any adjacent implants or natural teeth in order to accommodate healthy peri-implant tissues. This essentially means enough space around the implant to allow a physiologically formed and stable, biologic width of attachment to be established in much the same way as that formed around teeth (Figure 4).19,20
Figure 4. Implants placed too close to one another compromise the final outcome. The unfavourable proximity of the implants is shown with the healing abutments (a) and impression copings (b) in contact. A poor aesthetic result, particularly in relation to the soft tissue is produced (c).
This results in the widely accepted rule that a minimal distance of 1.5mm is required from the implant shoulder to an adjacent tooth and 3 mm is required between adjacent implants. Therefore, to replace a single central incisor with a 4 mm wide implant, a space of 7 mm is required between the two neighbouring teeth (1.5 + 4 + 1.5 mm). To replace both central incisors with the same implants, a space of 14 mm is needed (1.5 + 4 + 3 + 4 + 1.5 mm), and so on. Clearly, the use of different width implants changes these distances but only in respect to the change in implant width; the biologic width remains unchanged.
A third dimension that must be assessed is the occlusal space required for the prosthetic components. Different implant systems vary with regard to the lowest restoration option, but generally the inter-arch distance between the mucosa and opposing teeth is 4–5 mm. This space needs to be available when considering both static and dynamic occlusal relationships. The opposing teeth driving through a space during excursive or protrusive movements may eliminate what appeared to be an adequate gap.
Occlusal relationships also need to be looked at with a view to how guidance will be distributed between implant-retained restorations and natural teeth. Generally it is better to have excursive movements guided by the natural dentition as much as possible and, where there is no option but to include implant-retained restorations, group function should be sought. This is particularly the case when short implants are used or where the implants support bridgework, especially cantilever bridges.21 Signs of bruxism should be looked for as, along with improper occlusal designs, parafunctional activity can be associated with implant bone loss or fracture of the implant or prosthesis.22
This paper has deliberately avoided references to the condition and status of any remaining dentition in favour of concentrating on the general principles of implant assessment. Clearly, however, this cannot be avoided in practice. A careful clinical and radiographic examination of the teeth and periodontium in respect of both disease and also restorative status is critical in planning implant treatment. This applies not only to the tooth or teeth to be replaced, but also whether further teeth should be electively removed in order to achieve the best overall outcome for the patient. It must also be remembered that implant-retained and supported restorations are only one way of restoring missing teeth and the whole mouth needs to be considered, along with the wishes of the patient. It may be that an alternative treatment modality, such as a conventional prosthesis of some form – or simply accepting a space – may be the treatment approach of choice. Notwithstanding this statement, no further reference to the condition of the remaining dentition will be made.
Study models and diagnostic set-ups
Accurate models, preferably articulated, allow careful reflection and measurement of many of the factors examined during the clinical examination. They also allow a diagnostic wax-up of the proposed restorations to be performed which acts as an aid in planning the position and number of implants so that the teeth on the final prosthesis are positioned correctly. A try-in of the teeth in wax can also be produced so that the patient can gain a further understanding of what the final restoration will look like.
Once a diagnostic set-up has been finalized, it can be used to produce guides for radiographic examination and/or surgery. With regard to the former, various methods have been used including the incorporation of radio-opaque markers, coating the surface of the teeth with a material such as barium sulphate, or processing the whole stent in acrylic incorporating a radio-opaque material such as lipiodol ethiodized oil.23 Radiographic denture teeth are also available and radiographic guides incorporating these can be very useful in relating the bone and anatomical structures relative to the desired final tooth position (Figure 5).
Figure 5. Radiograph showing how the use of radiographic teeth on a denture base can assist in relating the desired position of the teeth with the underlying bone. (Image taken from a CBCT scan.)
Metallic markers of a known diameter are helpful in planning the size and length of implant indicated as various images, and particularly panoramic views, are generally magnified. The magnification in panoramic images varies between different machines but is often around 120–130%, particularly in the anterior mandible.24
Various designs of guide to assist in the surgical placement of implants are available. In the edentulous case, these are often duplicates of a denture made with the teeth in the ideal position and generally processed in clear acrylic. Typically, the guide is cut away in the desired area to allow drilling to take place, but custom-made drilling sleeves may be incorporated. A similar principle is utilized in the partially dentate case, but here a diagnostic set-up has established the idealized tooth position. The author favours a vacuum-formed surgical guide that is made on a stone duplicate of the diagnostic set-up (Figure 6).
Figure 6. A vacuum-formed surgical guide in position.
Custom-made drilling templates to allow image-guided surgery are becoming increasingly common and development in this area is rapid. These guides allow precise placement and angulations of implants determined using software applied to three-dimensional scans. The templates are constructed and applied at the time of surgery so that the implants may be placed as close as possible to the intended position.25
Radiographic examination
Even the most thorough clinical examination cannot give a full representation of the underlying bone. Radiographs provide information relating to bone volume, the angulation of adjacent tooth roots, pathology within the bone or around the roots of teeth and the existence of unerupted teeth. Revealing the position of anatomical structures, such as the maxillary antra and inferior dental canals and the presence of bony undercuts to the ridge or jawbone, can allow the placement of an implant to be as safe a procedure as possible.
Generally, a primary examination utilizing panoramic and/or intra-oral radiography is made. The choice of which particular combination of radiographs is adopted is dictated by the individual case, but advice on appropriate imaging has been published. One of the most widely known guidelines is that produced by a consensus workshop of the European Association of Osseointegration (EAO).26Table 1 summarizes the recommended standard radiographic techniques to be used in implant planning in different areas of the mouth. Cross-sectional imaging modalities may be required in circumstances where further information is required in relation to the position and size of anatomical structures, such as the incisive and mandibular canals, mental foramen or extent of the maxillary sinus. Additionally, it is used where clinical doubt exists with regard to the shape of the alveolar ridge.26
Intra-oral radiography
Panoramic imaging
Cephalometric lateral skull
MAXILLA
Single tooth
✓
Partially dentate
✓
✓
Edentulous
✓
✓
MANDIBLE
Single tooth
✓
Partially dentate
✓
✓
Edentulous
✓
✓
Cross-sectional images can be obtained using spiral tomography or conventional computed tomography (CT). The relatively recent introduction of cone beam or digital volume tomography (CBCT) has created another option for three-dimensional imaging of the hard tissues at a much lower radiation dose than conventional CT. CBCT is becoming exceedingly popular for maxillofacial imaging and may well become the standard technique with which partially dentate patients requiring implants are examined.27
A second consensus workshop of the EAO was held in October 2011 and an update to the guidelines is to be published soon.
Summary
Meticulous planning for patients for whom implant-retained restorations are proposed is crucial in order to achieve a successful treatment outcome with regard to function and aesthetics. This paper has identified various factors that may favourably or adversely affect the outcome of treatment. Table 2 summarizes some of these factors and categorizes them in relation to the risk that they may present in securing a satisfactory result.