Bourguignon C, Cohenca N, Lauridsen E International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations. Dent Traumatol. 2020; 36:314-330 https://doi.org/10.1111/edt.12578
Scarfe WC, Farman AG, Sukovic P Clinical applications of cone-beam computed tomography in dental practice. J Can Dent Assoc. 2006; 72:75-80
May JJ, Cohenca N, Peters OA Contemporary management of horizontal root fractures to the permanent dentition: diagnosis – radiologic assessment to include cone-beam computed tomography. Pediatr Dent. 2013; 35:120-124
Patel S, Brown J, Semper M European Society of Endodontology position statement: use of cone beam computed tomography in Endodontics. Int Endod J. 2019; 52:1675-1678 https://doi.org/10.1111/iej.13187
Incidental finding of a horizontal root fracture when considering a tooth for root canal treatment Nadine Amin Alison Qualtrough Dental Update 2025 51:2, 117-119.
Authors
NadineAmin
BDS (Lond)
Dental Core Trainee in Restorative Dentistry and Oral Surgery, Manchester University Dental Hospital
A 44-year-old female patient was referred to the restorative department at Manchester University Dental Hospital for root canal treatment of the maxillary right lateral incisor, which appeared to have a sclerosed root canal. The tooth had a history of trauma when the patient was 6 years old. A cone beam computed tomography scan of the tooth revealed an incidental finding of a transverse root fracture that was otherwise not visible on the peri-apical radiograph. This highlights the diagnostic challenge of peri-apical radiographs and emphasizes the value of three-dimensional imaging in endodontics. It also highlights the importance of timely referral and management of traumatic dental injuries to reduce the risk of complications in the future.
CPD/Clinical Relevance: This case report emphasizes the value of three-dimensional imaging in diagnosis.
Article
Traumatic dental injuries are common in adults and children. It has been reported that 25% of all school children experience dental trauma at some point, and 33% of adults have also experienced dental trauma to the permanent dentition.1 Root fractures are one of the potential outcomes of dental trauma. Transverse root fractures tend to be less commonly reported (0.5–7%) compared with other dental injuries, and most commonly involve the maxillary central and lateral incisors. Management of these root fractures depends on several factors including the location and angulation of the fracture, degree of displacement, tooth mobility and vitality. Typically, the more apical the fracture is, the better the prognosis. It is crucial to closely monitor teeth with root fractures to assess the healing and pulp survival status. Pulp necrosis and infection of the coronal fragment may occur as a direct response to the trauma around 3–4 months after the injury. Alternatively, necrosis and infection may occur years later and may be due to ingress of bacteria through cracks or fractures.2
Pulp canal obliteration is the rapid deposition of hard tissue on the internal walls of the root canal and pulp chamber space, which leads to the pulp system becoming narrowed and possibly blocked.3 The exact cause of pulp canal obliteration is unclear, but it is usually a sequela of traumatic injuries to teeth. Approximately 4–24% of traumatized teeth develop a degree of pulpal obliteration that is evident by radiographic loss of pulp space, or clinical yellow discolouration of the crown. These teeth prove to be challenging to treat from an endodontic perspective.4 A comprehensive clinical and radiographic examination is crucial to correctly diagnose the injury and provide appropriate treatment to ensure the best prognosis for the tooth.
Peri-apical radiographs are a useful diagnostic tool to show bone levels, peri-apical pathology, root morphology, apical resorption and obvious displacement of root fracture lines. Therefore, if a transverse root fracture is suspected, the first line of approach is to take peri-apical radiographs, which may reveal a root fracture. In some cases, two-dimensional imaging is sufficient for diagnosis and treatment planning. In instances in which two-dimensional radiographs do not provide sufficient information, a three-dimensional imaging scan should be considered.
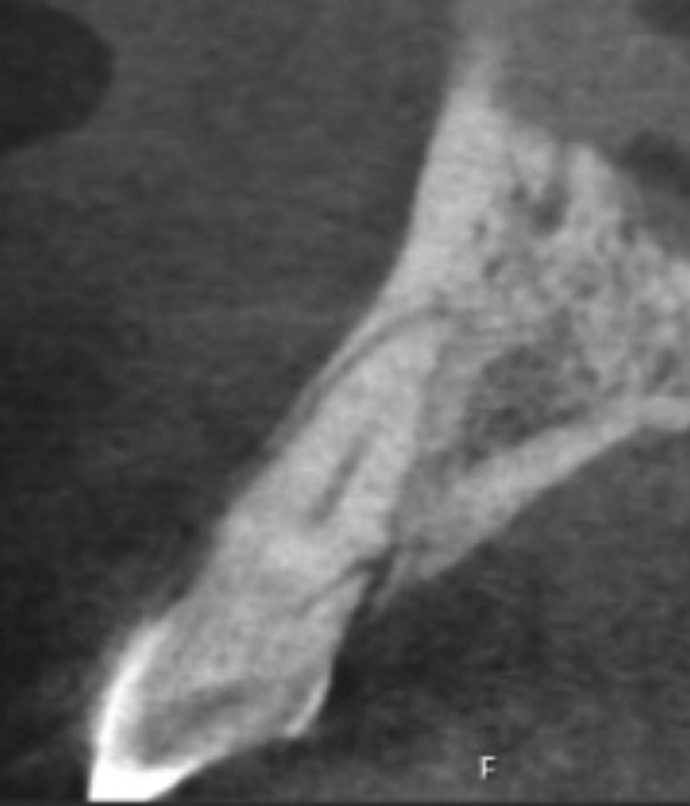
Figure 1. Peri-apical radiograph displaying canal sclerosis of UR2.Figure 2. CBCT scan revealing oblique root fracture of UR2.
Cone beam computed tomography (CBCT) is a medical imaging technique that uses divergent X-rays to form a cone to create a three-dimensional image. It has become a key part of diagnosis and treatment planning in several areas of dentistry, including implant dentistry, oral surgery and endodontics.5 CBCT scans are a useful diagnostic tool and are indicated for suspected transverse root fractures if they are not visible on a periapical radiograph.6
In accordance with IRMER 2017 guidance, clinicians should start with low-dose imaging and consider CBCT only if the findings are insufficient.7 The European Society of Endodontology advises that the possible benefits of CBCT over conventional imaging must outweigh the increased radiation exposure levels. CBCT should be considered on a case-by case basis after completion of a detailed clinical exam and where intra-oral radiographs do not offer sufficient diagnostic information. In such cases, a CBCT scan is indicated if the potential additional information will improve diagnosis, treatment planning and subsequent clinical management. Specific examples of this include management of dento-alveolar trauma, endodontic assessment of anatomically complex root canal systems and detecting root fractures that are not clearly identified in clinical assessment or conventional radiography.8
The majority of primary dental care settings do not have CBCT scanning machines and therefore it would be the general dental practitioner's responsibility to refer the patient to secondary care for appropriate imaging to be conducted.
Case report
A 44-year-old female patient was referred to the Restorative Dentistry Department at Manchester University Dental Hospital by her general dental practitioner (GDP) for root canal treatment of her maxillary right lateral incisor, UR2. Root canal treatment had been attempted by the GDP; however, challenges were encountered during treatment because the root canal appeared to be sclerosed. The patient presented with pain from this tooth. The patient's history revealed that she had been in a car accident when 6 years old and, as a result, had lost her maxillary right central incisor (UR1) and canine (UR3). The patient had an implant replacing the missing tooth, UR1. The patient was medically fit and well with no known drug allergies.
On examination, extra-orally there were no abnormalities detected and the intra-oral soft tissues appeared healthy. No intra-oral swellings or sinus tracts were noted. UR2 was of normal colour and was not mobile. The tooth was tender to percussion and did not respond to sensitivity testing with cold spray (Roeko Endo-frost) suggesting potential loss of vitality and peri-apical pathology. A peri-apical radiograph was taken (Figure 1), which showed bone loss and what appeared to be a sclerosed canal and pulp chamber, but no signs of apical pathology or fracture.
As part of further radiographic assessment of the sclerosed canal and endodontic treatment planning, a CBCT scan was taken. The CBCT scan revealed calcification of the pulp and the root canal in the coronal 40% of the root, as suspected. It also revealed an incidental finding of an oblique fracture line in the root, running from the distal and palatal aspects of the root at the level corresponding to where the root canal became visible (Figure 2). There was no convincing sign of peri-apical pathology.
Clinical management
The clinical and radiographic findings were discussed with the patient. The treatment options presented to the patient consisted of first, leaving and monitoring the tooth. This option was not deemed suitable by the clinician because the patient had presented in pain. The second option presented was extraction of UR2 and consideration of replacement, including a denture, bridge or an implant. The patient opted for extraction of the tooth and was keen to have an implant. The patient was referred for a second opinion from the joint implant clinic at Manchester University Dental Hospital.
Discussion
Despite the fracture, the tooth had maintained its vitality as demonstrated by the slow obliteration of the canal. This raises the question that, perhaps, elective root canal treatment when the canal is patent, in situations such as this, is a sensible approach. The delayed presentation, 38 years after the trauma, meant that tertiary dentine laid down resulted in pulp canal obliteration and canal sclerosis, thus rendering the tooth no longer suitable for root canal treatment. This is an unusual case and it encompasses two common side effects of dental trauma: transverse root fracture and canal sclerosis. The prognosis of root fractures is generally good; however, in this case, the position of the root fracture and the reaction of the pulp laying down tertiary dentine over the years deemed this tooth an unfavourable prognosis. This highlights the importance of early intervention, appropriate referral and close monitoring after dental trauma.
Conclusions
This case highlights the advantages of three-dimensional imaging techniques compared with two-dimensional imaging in aiding diagnoses, because conventional radiography has its limitations. It also highlights the importance of appropriate imaging, correct diagnosis and timely management of traumatic dental injuries: delayed presentation may complicate treatment. Appropriate diagnosis and timely intervention allow optimum long-term outcomes for patients. In cases where three-dimensional imaging techniques are not available in primary care, appropriate referral to secondary care should be strongly considered when indicated.