Ash MM, Nelson SJ, 8th edn. Amsterdam: Elsevier Science; 2003
Lin S, Pilosof N, Karawani M Occurrence and timing of complications following traumatic dental injuries: a retrospective study in a dental trauma department. J Clin Exp Dent. 2016; 8:e429-e436 https://doi.org/10.4317/jced.53022
Lin JC, Lu JX, Zeng Q Comparison of mineral trioxide aggregate and calcium hydroxide for apexification of immature permanent teeth: a systematic review and meta-analysis. J Formos Med Assoc. 2016; 115:523-530 https://doi.org/10.1016/j.jfma.2016.01.010
Murray PE, Garcia-Godoy F, Hargreaves KM Regenerative endodontics: a review of current status and a call for action. J Endod. 2007; 33:377-390 https://doi.org/10.1016/j.joen.2006.09.013
Kim SG, Malek M, Sigurdsson A Regenerative endodontics: a comprehensive review. Int Endod J. 2018; 51:1367-1388 https://doi.org/10.1111/iej.12954
Ostby BN The role of the blood clot in endodontic therapy. An experimental histologic study. Acta Odontol Scand. 1961; 19:324-353
Nygaard-Ostby B, Hjortdal O Tissue formation in the root canal following pulp removal. Scand J Dent Res. 1971; 79:333-349 https://doi.org/10.1111/j.1600-0722.1971
Lee BN, Moon JW, Chang HS A review of the regenerative endodontic treatment procedure. Restor Dent Endod. 2015; 40:179-187 https://doi.org/10.5395/rde.2015.40.3.179
do Couto AM, Espaladori MC, Leite APP A systematic review of pulp revascularization using a triple antibiotic paste. Pediatr Dent. 2019; 41:341-353
Malu K, Khubchandani M Triple antibiotic paste: a suitable medicament for intracanal disinfection. Cureus. 2022; 14 https://doi.org/10.7759/cureus.29186
Ruparel NB, Teixeira FB, Ferraz CC, Diogenes A Direct effect of intracanal medicaments on survival of stem cells of the apical papilla. J Endod. 2012; 38:1372-1375
Galler KM, Krastl G, Simon S European Society of Endodontology position statement: revitalization procedures. Int Endod J. 2016; 49:717-723 https://doi.org/10.1111/iej.12629
Araújo L, Goulart TS, Gil ACK Do alternative scaffolds used in regenerative endodontics promote better root development than that achieved with blood clots?. Braz Dent J. 2022; 33:22-32 https://doi.org/10.1590/0103-6440202204746
Narang I, Mittal N, Mishra N A comparative evaluation of the blood clot, platelet-rich plasma, and platelet-rich fibrin in regeneration of necrotic immature permanent teeth: a clinical study. Contemp Clin Dent. 2015; 6:63-68 https://doi.org/10.4103/0976-237X.149294
Lolato A, Bucchi C, Taschieri S Platelet concentrates for revitalization of immature necrotic teeth: a systematic review of the clinical studies. Platelets. 2016; 27:383-392 https://doi.org/10.3109/09537104.2015.1131255
Altaii M, Richards L, Rossi-Fedele G Histological assessment of regenerative endodontic treatment in animal studies with different scaffolds: a systematic review. Dent Traumatol. 2017; 33:235-244 https://doi.org/10.1111/edt.12338
Digka A, Sakka D, Lyroudia K Histological assessment of human regenerative endodontic procedures (REP) of immature permanent teeth with necrotic pulp/apical periodontitis: a systematic review. Aust Endod J. 2020; 46:140-153 https://doi.org/10.1111/aej.12371
Minic S, Vital S, Chaussain C Tissue characteristics in endodontic regeneration: a systematic review. Int J Mol Sci. 2022; 23 https://doi.org/10.3390/ijms231810534
Botero TM, Tang X, Gardner R Clinical evidence for regenerative endodontic procedures: immediate versus delayed induction?. J Endod. 2017; 43:(9S)S75-S81 https://doi.org/10.1016/j.joen.2017.07.009
Chaniotis A, Chanioti A Long-term complications of previously successful regenerative endodontic procedures after orthodontic movement: a report of 3 different complications after 4, 8, and 11 years. J Endod. 2022; 48:951-960 https://doi.org/10.1016/j.joen.2022.04.002
Lin LM, Ricucci D, Huang GT Regeneration of the dentine–pulp complex with revitalization/revascularization therapy: challenges and hopes. Int Endod J. 2014; 47:713-124 https://doi.org/10.1111/iej.12210
Mazzocca AD, McCarthy MB, Chowaniec DM Platelet-rich plasma differs according to preparation method and human variability. J Bone Joint Surg Am. 2012; 94:308-316 https://doi.org/10.2106/JBJS.K.00430
Innovative Paradigms and Established Strategies in Tooth Revitalization: A Review Ahmad Shah Khan Zahid Mehmood Khan Palwasha Ishaque Muhammad Zubair Syeda Fatima Tu Zahra Sana Ashfaq Dental Update 2025 51:8, 570-576.
Authors
Ahmad ShahKhan
Postgraduate Resident, Operative Dentistry and Endodontics, Armed Forces Institute of Dentistry, Rawalpindi, Pakistan
Revitalization has emerged as an innovative treatment approach for immature permanent teeth with necrotic pulp. This article presents a comprehensive analysis of revitalization, focusing on its principles, clinical protocols and outcomes. The article highlights the importance of thorough diagnosis and assessment of the pulp and peri-apical condition to determine the suitability of revitalization. Various factors influencing the success of revitalization, such as the use of scaffolds, growth factors and stem cells, are discussed. Additionally, a case that was treated with a PRP scaffold is also presented. Overall, revitalization shows promise in promoting pulp regeneration and improving treatment outcomes in selected cases of pulp necrosis.
CPD/Clinical Relevance: To introduce research-based knowledge to GDPs about the procedure and prognosis of tooth revitalization.
Article
The natural mechanism of crown and root development of a tooth is a complex process that consists of three distinct stages: bud, cap and bell stage. Hertwig's epithelial root sheath, a double layer of cells derived from ectoderm, provides guidance for root development when the crown is about to be completed. On average, it takes 1.5–3.5 years for the root to completely form after tooth eruption.1 During this time, the tooth is susceptible to damage by trauma or caries, which may have a detrimental effect on the pulp, sometimes resulting in pulp necrosis. This inhibits the flow of blood, adequate nutrients and growth factors, which are required by the developing root to fully mature and form an apex.2
Patients presenting with necrotic pulp and an immature root apex have historically been treated by apexification, by using calcium hydroxide. Although more convenient than other treatment protocols, the end results are not always favourable. The osteo-dentine barrier formed at the apex is often porous with thin dentinal walls, often resulting in root fractures and loss of the tooth.3 Calcium silicate-based cements, such as mineral trioxide aggregate (MTA), have been recommended as a root-end filling material. Although MTA provides a better apical seal, it still does not provide strength to the partially developed root.3
Murray et al defined revitalization/regenerative endodontic therapy (RET) as follows: ‘Biologically based procedures designed to replace damaged structures, including dentin and root structures, as well as cells of the pulp-dentin complex’.4
Revitalization basically applies principles of biology and engineering technology to provide an ideal environment capable of regenerating the dentine–pulp complex. It has been advocated as the treatment of choice for immature permanent teeth with necrotic pulp and apical periodontitis. The success of these procedures can be evaluated by resolution of symptoms, an increase in root length, and at times, a positive response to thermal stimuli.5
History
Revitalization was first studied by Nygaard-Ostby6 and Nygaard-Ostby and Hjortdal,7 who induced bleeding from the peri-apical tissues into the canal space of teeth. Iwaya et al8 further developed the concept by using a combination of antibiotics to disinfect the root canal. Banchs and Trope9 modified Iwaya et al's protocol by adding minocycline and using MTA as an intracanal barrier. This protocol has been widely used, recommended and has resulted in successful cases of revitalization.
Since then, several studies and case series have been published that investigated the use of different regenerative approaches, such as the use of different scaffold materials (e.g. platelet-rich plasma and platelet-rich fibrin), collection and implantation of autologous dental pulp stem cells directly inside the root canal, as well as the effect of different intracanal medicaments on the success rate of revitalization.
Treatment approach
In revitalization, a critical decision in fostering tissue regeneration depends on the approach as to how to incorporate stem cells into the root canal space. For this purpose, two techniques have been employed, namely the cell homing and cell-based transplantation techniques.
Cell homing relies on the chemotaxis of stem cells and endogenous cells from the injured peri-apical tissue by stimulating a host response via biological signalling molecules.10 This approach capitalizes on the natural regenerative potential of the patient's own cells without the need for exogenous cell transplantation. In contrast, cell-based transplantation depends on the active isolation and collection of human mesenchymal stem/progenitor cells (MSCs) from reservoirs, such as bone marrow, adipose tissue or dental pulp, and which are later incorporated into the pulp chamber along with a scaffold.10
Each approach has its merits and challenges. Cell homing is less invasive and more aligned with the biological principles of regeneration, while cell-based transplantation allows for precise control over the cell population and may be advantageous in cases where endogenous cell availability is limited.10 Most studies rely on the cell homing technique because it is easier to apply, more economical and does not rely on advanced laboratory equipment to first collect stem cells. This article focuses primarily on the cell homing technique.
Treatment protocol
An analysis of various clinical protocols for revitalization has shown that a wide range of differences exist across all studies.11 As a result, different treatment protocols may lead to varying treatment outcomes, making it challenging to accurately assess the true success rate of revitalization as a treatment method.
Numerous clinical studies have been published highlighting the steps taken for revitalization. It is typically performed in several stages, and may vary depending on the specific case and the techniques used by the clinician. Here is a general overview of the steps involved in revitalization via cell homing technique:
Diagnosis and treatment planning: A comprehensive history, clinical examination, and investigations are carried out to establish the pulpal and peri-apical diagnosis, in order to determine the extent of the damage to the pulp tissue and the potential for regeneration. This is required to assess the availability, or salvageability, of vital pulp. For such cases, vital pulp therapy (VPT) can provide a better treatment prognosis. Revitalization, on the other hand, should only be considered for immature permanent teeth that are necrosed or have sustained irreversible pulp damage. Restorability of the tooth is also considered before deciding the treatment modality along with written consent.
Access and cleaning: After application of local anaesthesia, isolation is established with a rubber dam. Disinfection of the crown and surrounding area is carried out and an access opening is prepared in the tooth to reach the pulp chamber and remove any infected or damaged pulp tissue. Minimal cleaning and shaping is done to preserve the already fragile root walls. The root canal is thoroughly irrigated with 1.5% sodium hypochlorite to remove any debris present, as well as to minimize any potential damage to viable stem cells present at the peri-apex.
Disinfection: Calcium hydroxide, triple antibiotic paste (TAP) containing minocycline, ciprofloxacin and metronidazole, or double antibiotic paste (without minocycline) is placed inside the canals for 2–4 weeks to eliminate any remaining bacteria and to initiate healing of the peri-radicular tissue.
Re-entry and induction of bleeding: After rubber dam application and regaining access to the pulp canal space, a small amount of bleeding is induced by inserting a file through the canal 2–3 mm beyond the apical limit. This bleeding helps to create a scaffold for new tissue growth.
Stem cell activation: It has been reported that many mesenchymal stem cells are present in the peri-apical area, such as stem cells of the apical papilla (SCAP).12 These cells have been categorized to be similar to dental pulp progenitor cells. In the presence of adequate morphogens/growth factors, these cells are stimulated, resulting in tissue regeneration. These growth factors, already trapped in the dentine matrix, can be released by the action of EDTA, or can be directly provided as part of the scaffold such as in PRP or PRF.
Scaffold placement: A biocompatible scaffold material is placed into the canal space to support the growth of new tissue. The scaffold is also thought to provide a physical barrier that prevents the ingrowth of epithelial cells into the canal space. The scaffold material may be composed of a variety of materials, such as blood, PRP, PRF, collagen, chitosan or hydroxyapatite.13
Barrier placement: A calcium silicate-based cement, such as MTA or Biodentine (Septodont, Saint-Maurdes-fossés, France) is placed over the scaffold and acts as a coronal barrier to prevent coronal leakage and ingress of micro-organisms. It acts as a biocompatible material, capable of inducing dentine formation, which also provides a better marginal seal than other restorative materials (e.g. glass ionomer cement).3
Final restoration: After hardening of the MTA, the tooth is permanently restored with a suitable material to protect the tooth, improve aesthetics, and restore its function.
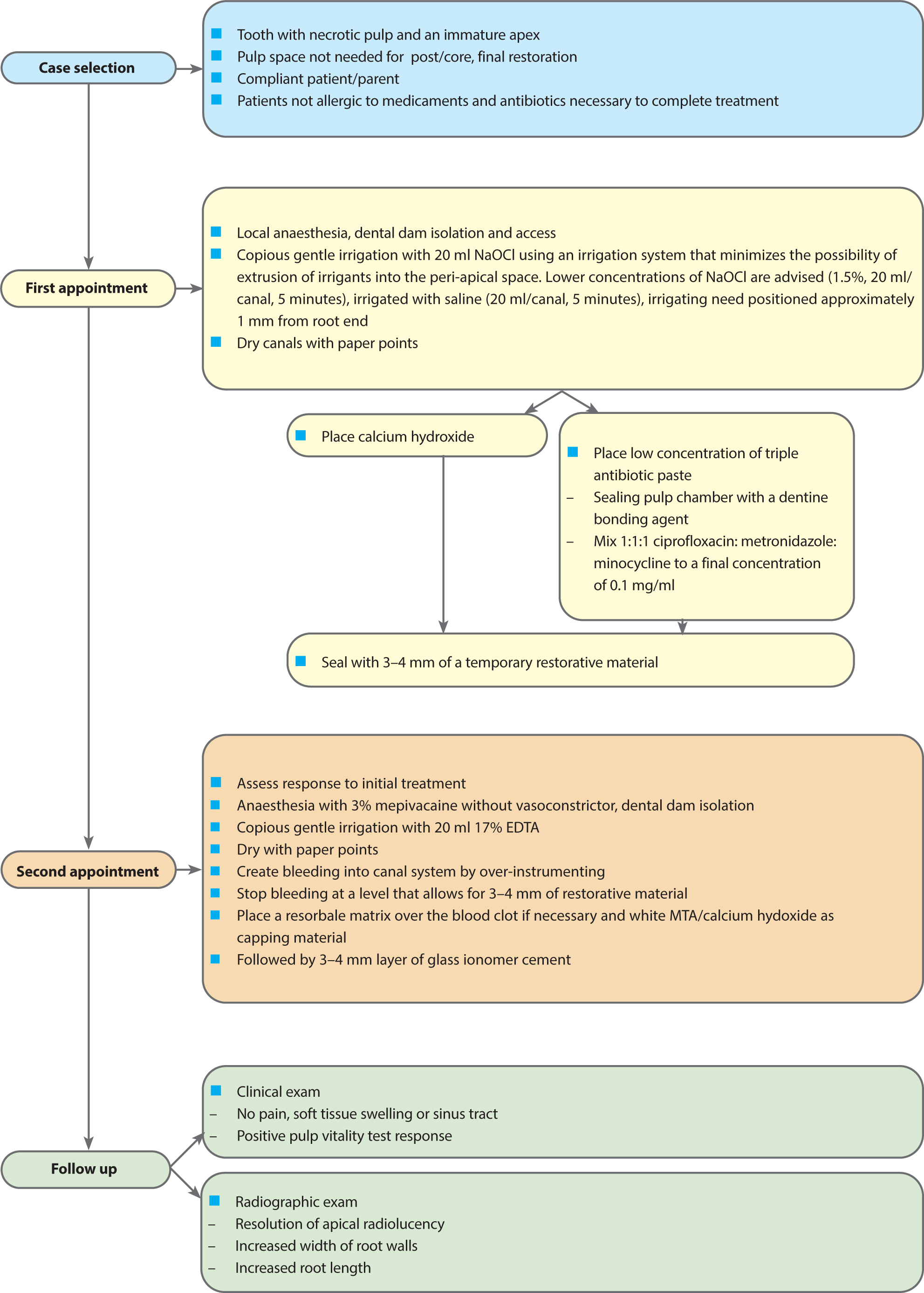
Keeping in view, all these different approaches to revitalization, Lee et al14 published a standard treatment protocol, courtesy of the American Association of Endodontists (AAE) (Figure 1).
Figure 1. The current considerations for revitalization/regenerative endodontic treatment procedures.14
Intracanal medicaments
The significance of intracanal medicament in revitalization lies in its pivotal role in establishing a conducive environment for tissue regeneration within the root canal. These medicaments are instrumental in disinfecting the canal, eliminating microbial contaminants and minimizing inflammation, thereby creating an optimal milieu for stem cell survival and differentiation. Triple antibiotic paste (TAP) has been recognized as an excellent material for canal disinfection, with many published cases of successful revitalization.15 However, it should be kept in mind that the overall concentration of TAP should not exceed 0.1 mg/ml, as recommended by the American Association of Endodontics.14
TAP provides effective action against micro-organisms, while also reducing the chance of antimicrobial resistance. It is also known to cause tooth discolouration, primarily due to minocycline.16 At a higher concentration, TAP can exhibit cytotoxic effects on the SCAP cells,17 as well as significantly reducing the micro-hardness of the pulp–dentine complex, when compared to MTA at the same concentration. This can be attributed to minocycline causing calcium chelation from dentine. Alternative medicaments, such as amoxicillin and cefaclor, as well as dentine-bonding agents, can mitigate this issue.16
Taking into account these drawbacks, in their position statement on revitalization procedures, the European Society of Endodontology preferred calcium hydroxide as an intracanal medicament.18
Scaffolds
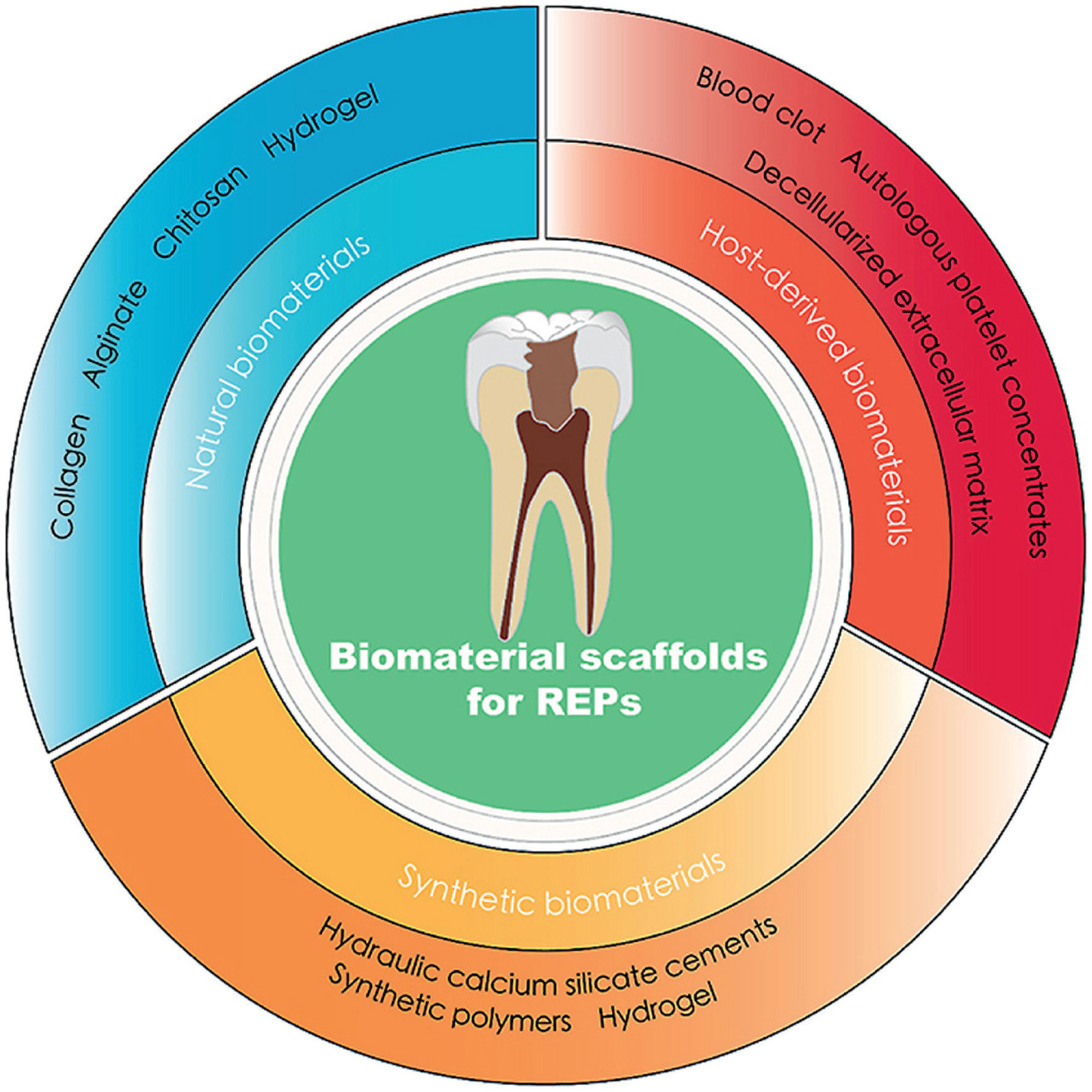
Scaffolds are solid biomaterials with a three-dimensional (3D) porous structure to facilitate the correct spatial positioning of cells, promote interactions between cells and the biomaterial, and allow for the transport of nutrients, gases and regulatory factors necessary for cell survival and differentiation. Various materials have been used as scaffolds for revitalization and can be classified as shown in Table 1,19 as well as a diagrammatic overview of available scaffolds is shown in Figure 2.20 Although all the mentioned scaffolds have been used in stem cell therapy and revitalization,19 an integrative study published in the Brazilian Dental Journal claimed that the majority of alternative scaffolds were similar to a blood clot, while only PRF and PRP showed significantly better results than a blood clot, in terms of stimulating root development.21
Cell-free scaffoldsScaffolds seeded with stem cells
Figure 2. Diagrammatic overview of available scaffolds.20
Several research studies have compared the efficacy of using PRP and PRF as scaffolds in revitalization, but the results have been inconsistent. PRP and PRF are used in place of a blood clot because they contain growth factors that can help regenerate the dentine–pulp complex. A study by Narang et al in 2015,22 which compared blood clot, PRP and PRF, found that PRF produced better clinical results compared to PRP or blood clot. However, a comprehensive analysis of clinical trials discovered that there was no meaningful difference in the effectiveness of PRP or PRF compared to blood clot in promoting the thickening of the canal walls or continued root development in revitalization.23
Histological assessment
One of the main goals of revitalization is the replacement of necrosed pulp tissue inside the canal. However, several studies, both animal and human, have shown that the newly induced pulp tissue is different from normal pulp parenchymal tissue.
In 2017, Milad et al24 published a systematic review on the histological assessment of revitalization in animal studies with different scaffolds, which claimed that when blood clot was used a as a scaffold, dentine-like tissue was found in 4% of canals, 64% had cementum-like tissue and 10% had bone-like tissue. The observed vital tissues were mostly connective tissue with infiltrating fibroblast-like cells and blood vessels.25
There are some general histological characteristics that may be observed in newly regenerated pulp tissue after revitalization:25,26
Fibrous connective tissue: The newly regenerated pulp tissue often consists of a dense network of fibrous connective tissue, which contains collagen fibres, spindle-shaped fibroblasts, mesenchymal cells, and extracellular matrix proteins.
Blood vessels: One of the key goals of revitalization is to promote angiogenesis within the pulp tissue. Newly regenerated pulp tissue may contain numerous blood vessels, which can be visualized using histological staining methods.
Nerve fibres: The regeneration of nerve fibres within the pulp tissue after revitalization is still an area of active research. Positive response to thermal stimulus has been demonstrated in many cases, which shows active neurogenesis.
Cellular infiltrate: Inflammatory cells, such as macrophages, neutrophils and polynuclear leukocytes, may be present in the early stages of pulp tissue regeneration.
Mineralization: Depending on the extent of the initial tissue damage, newly regenerated pulp tissue may undergo a process of mineralization, in which calcium deposits accumulate within the tissue in the form of newly formed cementum tissue along the dentinal walls.
Complications
Revitalization is a relatively new and still-evolving field of endodontics, and as with any medical procedure, there are potential complications and risks that should be considered. Some possible complications associated with revitalization include:27,28
Incomplete regeneration: Despite the high success rates reported in some studies, not all cases of revitalization result in complete regeneration of pulp tissue. In some cases, the newly regenerated tissue may not be fully functional or may not fully replace the original pulp tissue.
Infection: Revitalization involves the use of growth factors and other biological materials, which can increase the risk of infection if not handled properly. Additionally, if the original infection is not completely eliminated before the procedure, it can lead to persistent infection and treatment failure.
Pain and discomfort: Patients may experience pain or discomfort during and after the procedure, especially if the tooth was severely damaged or infected. This can be managed with pain medications and other supportive care measures.
Root resorption: In rare cases, revitalization may cause internal root resorption, which is the loss of root structure as a result of the body's immune response. Initial studies carried out by Ostby et al suggested the newly formed tissue within the canal was dissimilar to normal pulpal tissue with the majority of the tissue being fibrous in nature with internal resorption of root canal walls.29
Tooth discolouration: The use of certain materials and techniques in revitalization can lead to tooth discolouration, such as MTA and TAP, which can be a cosmetic concern for some patients.
Failure of the procedure: In some cases, revitalization may not be successful in saving the tooth, and the tooth may need to be extracted. Most commonly, failure occurs when the canal or peri-apical area is not adequately disinfected.
It is important for patients to discuss the potential risks and benefits of revitalization with their endodontist or dental professional and to carefully follow post-treatment instructions to optimize the chances of success and minimize the risk of complications.
Case report
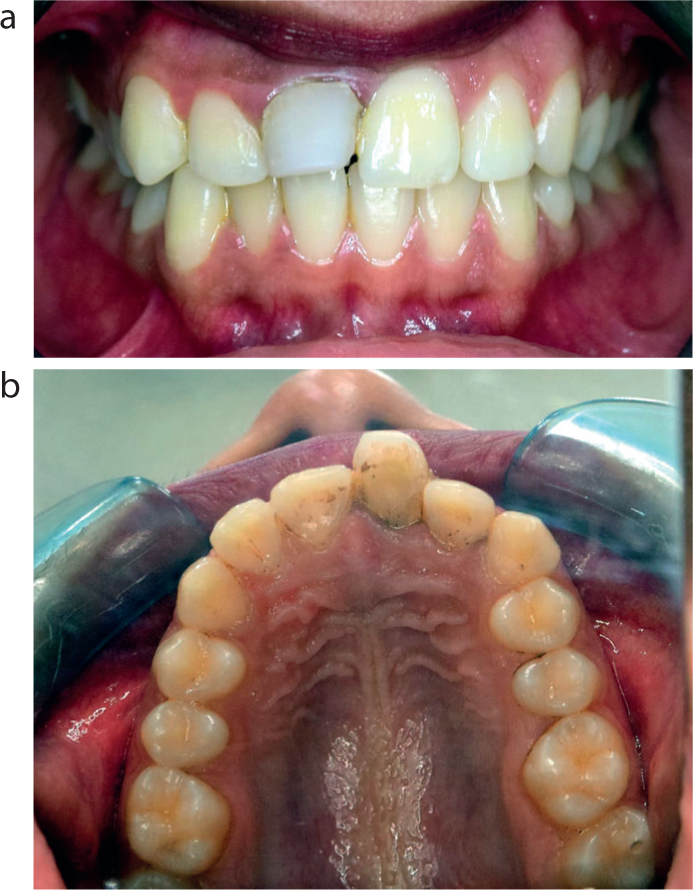
An 18-year-old female reported to the Department of Operative Dentistry and Endodontics, Armed Forces Institute of Dentistry, with a complaint of dull throbbing pain in the maxillary right central incisor for the previous 3 days, along with compromised aesthetics resulting in low self-esteem when smiling. The patient had a history of a fall down stairs, which resulted in trauma to the maxillary right central incisor and fractured incisal edge, 9 years previously. She reported to a local dentist who had restored the tooth. Her past medical, surgical, personal, family, and drug history were non-contributory, and she belonged to a lower middle-class family. Extra-oral examination revealed that she had a symmetrical face with no swelling, abscess, scars or jaw deviations. Intra-oral examination revealed a restored maxillary right central incisor that was discoloured, poorly contoured with excessive bulk on the labial surface and was tender on percussion. No caries was detected on any other teeth. Localized gingival inflammation and subgingival calculus were present around tooth UR1. Overall, the gingiva was firm, with normal contours and resilient in consistency (Figure 3).
Cold, heat and electric pulp testing elicited no response in UR1, while the response within normal limits was seen in UR2 and UL1. Peri-apical lesion and immature root apex can be observed on Peri-apical Radiograph compared with UL1. The diagnosis was pulp necrosis with chronic apical abscess of maxillary right central incisor along with incomplete formation of root apex (Figure 4).
Treatment options, including apexification, revitalization, extraction, and observation, were presented to the patient and hers parents. After detailed discussions about the different treatment options, along with their advantages and disadvantages, revitalization was selected. Written informed consent was obtained from the patient prior to treatment procedures.
First treatment visit
The tooth was isolated with rubber dam. The access cavity was prepared, and the working length of the canal was determined radiographically by placing a hand #80 K-file into the root canal. Without mechanical instrumentation, the pulp chamber and the root canal was gently irrigated with 20 ml 1.5% sodium hypochlorite (NaOCl). The canal was dried with sterile paper points. Equal proportions of metronidazole, ciprofloxacin and minocycline were ground to powder and mixed with distilled water into a creamy consistency to form a triple antibiotic paste (TAP) to be used as an intracanal medication. TAP was placed in the canal below the cemento-enamel junction to minimize crown staining. The access cavity was sealed temporarily with glass ionomer cement and a sterile cotton pellet. The patient was scheduled for a second visit after 3 weeks.
Second treatment visit
A local anaesthetic solution was administered without epinephrine, the tooth was isolated with rubber dam, and the temporary restoration was removed. The tooth was again irrigated with 20 ml 1.5% sodium hypochlorite for 5 minutes. Final irrigation was completed with 17% EDTA (20 ml/5 min), after which the root canals were dried with paper points. With the use of dental loupes, bleeding was induced in the canal space by irritating the peri-apical tissues with a #25 K-file introduced into the canal through the immature apex. The presence of bleeding in the apical one-third of the canal was verified with paper points. To prepare the PRP, 10 ml of whole blood was drawn from the median cubital vein of the patient. The blood was collected in a tube containing 1 ml 3.2% sodium citrate and was centrifuged immediately using a tabletop centrifuge (DM0506 DLAB Centrifuge Machine, China) at 3200 revolutions per minute for 15 minutes, according to the method described by Mazzocca et al.30 The PRP was activated with calcium gluconate before placing inside the canal to transform into a gel state after 10 minutes. A 3-mm thickness of white mineral trioxide aggregate (MTA) was placed directly over the PRP scaffold, and the tooth was temporarily restored with glass ionomer cement. Three days later, permanent restoration of the tooth was carried out with bonded resin composite. The patient was scheduled for recall visits and subsequent evaluation.
Follow-up examinations
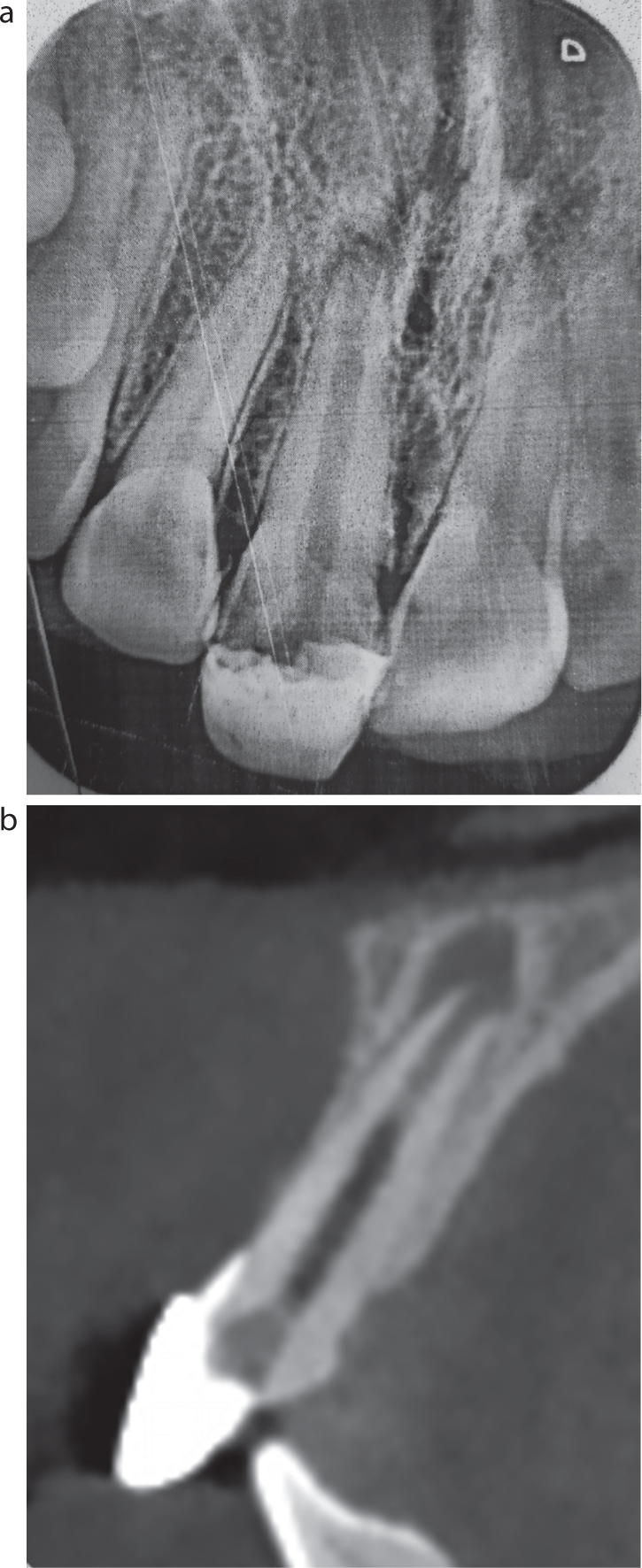
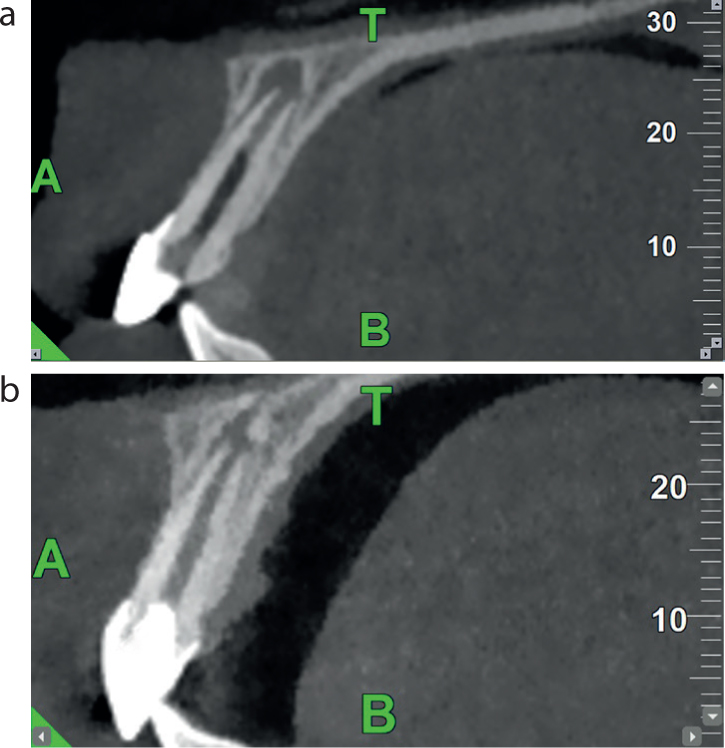
The patient was recalled for review after 1 month, 3 months, 6 months and 1 year. The patient was asymptomatic. CBCT scans were carried out pre-operatively and after 1 year, the sagittal view of which showed resolution of the peri-apical infection, an increase in dentine thickness and root length, as well as the initiation of apex closure (Figure 5).
Figure 5. CBCT scans. (a) Pre-operative; and (b) at 1 year post-operatively.
Conclusion
Tooth revitalization marks a new era in both biological and clinical aspects of endodontic treatment. It is now widely recognized as the preferred treatment approach for immature permanent teeth with necrotic pulp, thanks to the success demonstrated in numerous documented cases. Over time, our understanding of the clinical protocols has advanced, aiming not only to eliminate pulp infection, but also to stimulate the potential of stem cells within the canal and release growth factors trapped in the dentine walls. Although the current protocols achieve repair rather than complete regeneration, there is optimism that further research in stem cell-based pulp engineering will enable true regeneration and enhance treatment outcomes.