Bartlett D, Dugmore C. Pathological or physiological erosion – is there a relationship to age?. Clin Oral Investig. 2008; 12:S27-31 https://doi.org/10.1007/s00784-007-0177-1
Schlueter N, Luka B. Erosive tooth wear – a review on global prevalence and on its prevalence in risk groups. Br Dent J. 2018; 224:364-370 https://doi.org/10.1038/sj.bdj.2018.167
Shellis RP, Addy M. The interactions between attrition, abrasion and erosion in tooth wear. Monogr Oral Sci. 2014; 25:32-45 https://doi.org/10.1159/000359936
Grippo JO, Simring M, Schreiner S. Attrition, abrasion, corrosion and abfraction revisited: a new perspective on tooth surface lesions. J Am Dent Assoc. 2004; 135:1109-1218 https://doi.org/10.14219/jada.archive.2004.0369
Loomans B, Opdam N, Attin T Severe tooth wear: European Consensus Statement on Management Guidelines. J Adhes Dent. 2017; 19:111-119 https://doi.org/10.3290/j.jad.a38102
Sterenborg BAMM, Bronkhorst EM, Wetselaar P The influence of management of tooth wear on oral health-related quality of life. Clin Oral Investig. 2018; 22:2567-2573 https://doi.org/10.1007/s00784-018-2355-8
Mehta SB, Loomans BAC, Banerji S An investigation into the impact of tooth wear on the oral health related quality of life amongst adult dental patients in the United Kingdom, Malta and Australia. J Dent. 2020; 99 https://doi.org/10.1016/j.jdent.2020.103409
Hardan L, Mancino D, Bourgi R Treatment of tooth wear using direct or indirect restorations: a systematic review of clinical studies. Bioengineering (Basel). 2022; 9 https://doi.org/10.3390/bioengineering9080346
Gulamali AB, Hemmings KW, Tredwin CJ, Petrie A. Survival analysis of composite Dahl restorations provided to manage localised anterior tooth wear (ten year follow-up). Br Dent J. 2011; 211 https://doi.org/10.1038/sj.bdj.2011.683
Al-Khayatt AS, Ray-Chaudhuri A, Poyser NJ Direct composite restorations for the worn mandibular anterior dentition: a 7-year follow-up of a prospective randomised controlled split-mouth clinical trial. J Oral Rehabil. 2013; 40:389-401 https://doi.org/10.1111/joor.12042
Milosevic A, Burnside G. The survival of direct composite restorations in the management of severe tooth wear including attrition and erosion: a prospective 8-year study. J Dent. 2016; 44:13-19 https://doi.org/10.1016/j.jdent.2015.10.015
Tauböck TT, Schmidlin PR, Attin T. Vertical bite rehabilitation of severely worn dentitions with direct composite restorations: clinical performance up to 11 years. J Clin Med. 2021; 10 https://doi.org/10.3390/jcm10081732
Mehta SB, Lima VP, Bronkhorst EM Clinical performance of direct composite resin restorations in a full mouth rehabilitation for patients with severe tooth wear: 5.5-year results. J Dent. 2021; 112 https://doi.org/10.1016/j.jdent.2021.103743
Edelhoff D, Güth JF, Erdelt K Clinical performance of occlusal onlays made of lithium disilicate ceramic in patients with severe tooth wear up to 11 years. Dent Mater. 2019; 35:1319-1330 https://doi.org/10.1016/j.dental.2019.06.001
Hammoudi W, Trulsson M, Svensson P, Smedberg JI. Long-term results of a randomized clinical trial of 2 types of ceramic crowns in participants with extensive tooth wear. J Prosthet Dent. 2022; 127:248-257 https://doi.org/10.1016/j.prosdent.2020.08.041
Smales RJ, Berekally TL. Long-term survival of direct and indirect restorations placed for the treatment of advanced tooth wear. Eur J Prosthodont Restor Dent. 2007; 15:2-6
Vailati F, Gruetter L, Belser UC. Adhesively restored anterior maxillary dentitions affected by severe erosion: up to 6-year results of a prospective clinical study. Eur J Esthet Dent. 2013; 8:506-530
Vajani D, Tejani TH, Milosevic A. Direct composite resin for the management of tooth wear: a systematic review. Clin Cosmet Investig Dent. 2020; 12:465-475 https://doi.org/10.2147/CCIDE.S268527
Ning K, Bronkhorst E, Bremers A Wear behavior of a microhybrid composite vs. a nanocomposite in the treatment of severe tooth wear patients: a 5-year clinical study. Dent Mater. 2021; 37:1819-1827 https://doi.org/10.1016/j.dental.2021.09.011
Sterenborg BAMM, Bronkhorst EM, Wetselaar P The influence of management of tooth wear on oral health-related quality of life. Clin Oral Investig. 2018; 22:2567-2573 https://doi.org/10.1007/s00784-018-2355-8
Sterenborg BAMM, Kalaykova SI, Knuijt S Speech changes in patients with a full rehabilitation for severe tooth wear, a first evaluation study. Clin Oral Investig. 2020; 24:3061-3067 https://doi.org/10.1007/s00784-019-03174-7
Sterenborg BAMM, Maal TJJ, Vreeken R The facial effects of tooth wear rehabilitation as measured by 3D stereophotogrammetry. J Dent. 2018; 73:105-109 https://doi.org/10.1016/j.jdent.2018.04.014
Opdam N, Skupien JA, Kreulen CM Case report: a predictable technique to establish occlusal contact in extensive direct composite resin restorations: the DSO-technique. Oper Dent. 2016; 41:(S7)S96-S108 https://doi.org/10.2341/13-112-T
Abduo J. Safety of increasing vertical dimension of occlusion: a systematic review. Quintessence Int. 2012; 43:369-380
Mehta SB, Bronkhorst EM, Lima VP The effect of pre-treatment levels of tooth wear and the applied increase in the vertical dimension of occlusion (VDO) on the survival of direct resin composite restorations. J Dent. 2021; 111 https://doi.org/10.1016/j.jdent.2021.103712
Milosevic A, Burnside G. The survival of direct composite restorations in the management of severe tooth wear including attrition and erosion: a prospective 8-year study. J Dent. 2016; 44:13-19 https://doi.org/10.1016/j.jdent.2015.10.015
Lima VP, Crins LAMJ, Opdam NJM Deterioration of anterior resin composite restorations in moderate to severe tooth wear patients: 3-year results. Clin Oral Investig. 2022; 26:6925-6939 https://doi.org/10.1007/s00784-022-04647-y
Crins LAMJ, Opdam NJM, Kreulen CM Randomized controlled trial on the performance of direct and indirect composite restorations in patients with severe tooth wear. Dent Mater. 2021; 37:1645-1654 https://doi.org/10.1016/j.dental.2021.08.018
Oudkerk J, Eldafrawy M, Bekaert S The one-step no-prep approach for full-mouth rehabilitation of worn dentition using PICN CAD-CAM restorations: 2-yr results of a prospective clinical study. J Dent. 2020; 92 https://doi.org/10.1016/j.jdent.2019.103245
Naik VB, Jain AK, Rao RD, Naik BD. Comparative evaluation of clinical performance of ceramic and resin inlays, onlays, and overlays: a systematic review and meta analysis. J Conserv Dent. 2022; 25:347-355 https://doi.org/10.4103/jcd.jcd_184_22
Heintze SD, Cavalleri A, Forjanic M Wear of ceramic and antagonist – a systematic evaluation of influencing factors in vitro. Dent Mater. 2008; 24:433-449 https://doi.org/10.1016/j.dental.2007.06.016
Mitov G, Heintze SD, Walz S Wear behavior of dental Y-TZP ceramic against natural enamel after different finishing procedures. Dent Mater. 2012; 28:909-918 https://doi.org/10.1016/j.dental.2012.04.010
Edelhoff D, Sorensen JA. Tooth structure removal associated with various preparation designs for posterior teeth. Int J Periodontics Restorative Dent. 2002; 22:241-249
Yip K, Lam PPY, Yiu CKY. Prevalence and associated factors of erosive tooth wear among preschool children – a systematic review and meta-analysis. Healthcare (Basel). 2022; 10 https://doi.org/10.3390/healthcare10030491
Nijakowski K, Walerczyk-Sas A, Surdacka A. Regular physical activity as a potential risk factor for erosive lesions in adolescents. Int J Environ Res Public Health. 2020; 17 https://doi.org/10.3390/ijerph17093002
Samman M, Kaye E, Cabral H Dental erosion: effect of diet drink consumption on permanent dentition. JDR Clin Trans Res. 2022; 7:425-434 https://doi.org/10.1177/23800844211048478
El Aidi H, Bronkhorst EM, Huysmans MC, Truin GJ. Multifactorial analysis of factors associated with the incidence and progression of erosive tooth wear. Caries Res. 2011; 45:303-312 https://doi.org/10.1159/000328671
Donovan T, Nguyen-Ngoc C, Abd Alraheam I, Irusa K. Contemporary diagnosis and management of dental erosion. J Esthet Restor Dent. 2021; 33:78-87 https://doi.org/10.1111/jerd.12706
Ganss C, Klimek J, Giese K. Dental erosion in children and adolescents – a cross-sectional and longitudinal investigation using study models. Community Dent Oral Epidemiol. 2001; 29:264-271 https://doi.org/10.1034/j.1600-0528.2001.290405.x
Harding MA, Whelton HP, Shirodaria SC Is tooth wear in the primary dentition predictive of tooth wear in the permanent dentition? Report from a longitudinal study. Community Dent Health. 2010; 27:41-45
Amaechi BT, Higham SM, Edgar WM. Factors influencing the development of dental erosion in vitro: enamel type, temperature and exposure time. J Oral Rehabil. 1999; 26:624-630 https://doi.org/10.1046/j.1365-2842.1999.00433.x
Longevity and performance of materials used for the restorative management of tooth wear: a review Verônica P Lima Tatiana Pereira-Cenci Shamir B Mehta Subir Banerji Bas AC Loomans Dental Update 2025 50:10, 877-883.
Authors
Verônica PLima
BDS, MSc, PhD
Lecturer, Academic Center for Dentistry Amsterdam (ACTA), University of Amsterdam and Vrije Universiteit, Amsterdam, Netherlands; Guest Researcher, Radboud University Medical Center, Radboud Institute for Health Sciences, Department of Dentistry, Nijmegen, Netherlands
Programme Director MSc in Aesthetic Dentistry, Faculty of Dentistry, Oral and Craniofacial Sciences, King's College London; Visiting Professor, Department of Dentistry, Radboud University Medical Centre, Nijmegen, Netherlands
BDS, MClinDent (Prostho), PhD, FDS RCPS (Glasg), FCGDent (UK) ,FDTFEd (RCS Ed), Faculty of Dentistry, Oral and Craniofacial Sciences, King's College London; Professor, School of Dental Health and Care Professions, University of Portsmouth; Associate Professor, Department of Prosthodontics, Melbourne Dental School, University of Melbourne; Private Practice, Ealing, London
This article provides an overview of the available evidence on the performance, with particular consideration of the longevity of restorative materials used in the management of tooth wear. Different materials can be employed depending on whether a subtractive or additive strategy is used. Preference should be given to the latter to help preserve remaining tooth tissue. The use of both direct and indirect materials may yield acceptable survival results when considering data with at least 5 years of follow-up. Patients should be informed that because tooth wear is a continuous process, a certain level of maintenance of the restorations will be necessary and that this may impact on the success of the treatment.
CPD/Clinical Relevance: Conservative, adhesive strategies are suitable for the restorative management of tooth wear.
Article
The longer the natural dentition is maintained, the more likely it is to gain exposure to erosive, abrasive, and attritive challenges, culminating in the progressive loss of the mineralized tissues. Tooth wear is an irreversible, non-carious and cumulative physiological process that is also related to ageing.1,2 It has been estimated to affect between 20% and 45% of the permanent dentition.3
Primarily, tooth wear may be caused by chemical or mechanical factors, and in most cases, it will involve a combination of both. Exposure of the dental hard tissues to chemical factors will culminate in the transitional softening of tooth surfaces, rendering them susceptible to the effects of potential mechanical factors, resulting in the accelerated loss of the softened tooth structure.4 Chemical factors can be intrinsic, for example when the stomach's acidic content enters the oral cavity, or extrinsic, from acids in dietary or other external sources.5 Mechanical factors include intrinsic factors, such as contact between teeth (clenching or grinding) that can occur during functional or non-functional jaw movements, and extrinsic factors, caused by contact with external factors as biting nails, pens, etc.6 These factors often interact, and other processes may be concurrently involved.
As dental hard tissue surface loss progresses, the resultant tooth wear may become noticeable. In severe cases, the loss of dental structure can lead to a significant reduction of the clinical crown and even dentine exposure.7 Patients with tooth wear may experience a variety of symptoms, including aesthetic concerns, sensitivity, and possible negative consequences on their oral health-related quality of life.8,9 Preventive strategies, such as counselling and monitoring, form an important component of the management of tooth wear. However, when there are clear functional and/or aesthetic concerns, or when the patient's quality of life is significantly impacted by the level of their tooth wear, restorative treatment may be indicated.7 The aim of the restorative management of tooth wear is to re-establish the lost function and form, while simultaneously protecting the remaining tooth tissues from experiencing further wear. This article gives an overview of the available evidence on the performance, with particular consideration of the longevity, of restorative materials commonly used in the restorative management of tooth wear.
Restorative materials used in the management of tooth wear
In the past, common treatment options for patients with tooth wear were full- and partial-coverage conventionally retained crowns. However, developments in adhesive dentistry have expanded the available restorative options for the management of such cases and include direct or indirect techniques, using resin- and non-resin-based materials. The clinical performance of different types of restorations in the management of tooth wear (to include the management of localized and generalized tooth wear) has been reported by numerous studies, and some of the outcomes of these investigations with at least 5 years of follow-up have been summarized in Table 1. It should be noted that comparison between individual investigations reporting the performance of restorations may be challenging owing to a variety of factors, which include the application of differing nomenclature, variations in treatment protocols and the criteria used to determine outcomes. The present authors are of the view that reporting of success (or failure) should include a description of the survival percentage (after a certain observation time), or documentation of the annual failure rates (AFRs). However, despite the increasing number of such studies, there remains a lack of substantial evidence about the longer-term performance of the restorations commonly prescribed for the management of tooth wear.10
Table 1. A summary of studies reporting on the performance of restorative materials used for the management of tooth wear with at least 5 years of follow-up.
Direct resin composite; indirect resin composite; ceramic veneer
A
12
134
39.4
6
No catastrophic or major failures were observed. Only minor marginal defects between the palatal and buccal veneers were found
⊕
A: anterior; P: posterior; A/P: anterior and posterior; NA: not available;⊕: acceptable survival (including repaired restorations); ⊖: unfavourable survival.
Resin-based restorations
Many of the studies listed in Table 1 evaluate the performance of resin-based restorations employed the use of both direct and indirect application techniques for the rehabilitation of the worn dentition. Resin composite materials may offer a conservative and minimally invasive treatment option (Figure 1).7 Additionally, resin composite restorations provide further advantages:
Are minimally abrasive to antagonistic surfaces.21
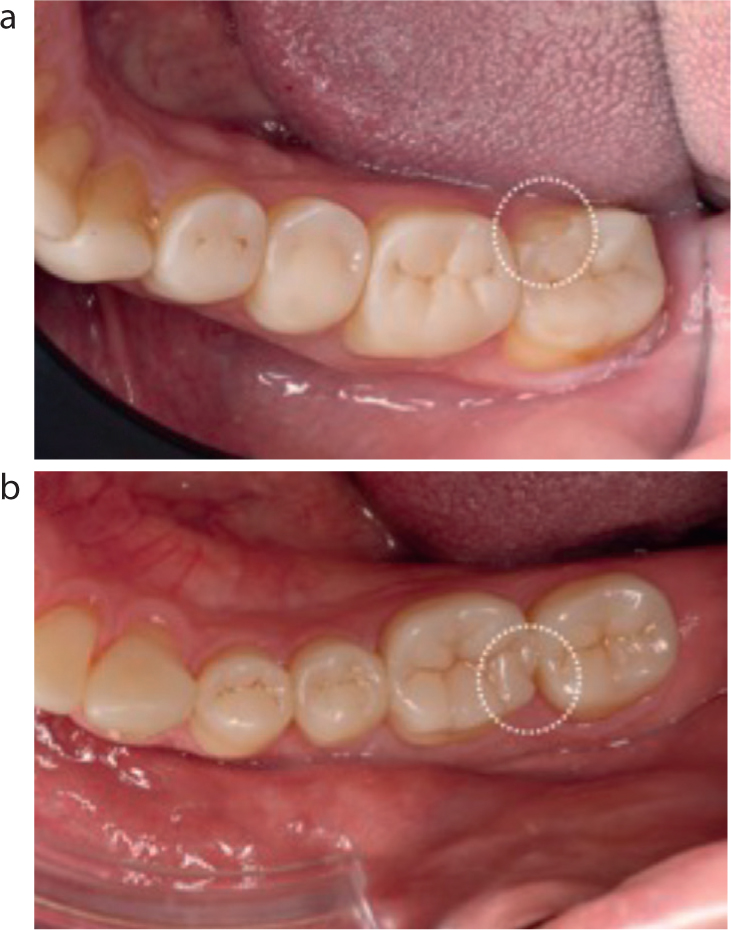
Figure 1. Case of full-mouth rehabilitation with resin-based restorations performed in a patient from the Radboud Tooth Wear Project. (a) Before restorative procedures; (b) after the completion of restorations.
Compared to other materials, such as metals or ceramics, a drawback of resin composite restorations is that, over time, they may show an accelerated wear rate and have a tendency towards discolouration and fracture,22 ultimately requiring repair or replacement.23 However, resin composite is a relatively inexpensive material, and when applied directly, it offers the possibility of a single-visit execution without laboratory costs. Direct resin composite restorations can also be used as a diagnostic aid to help evaluate the proposed functional and aesthetic changes that accompany the placement of these restorations, especially when further treatment planning may be anticipated that may involve the prescription of indirect restorative materials, which are far less amenable to adjustment in the oral cavity. However, the placement of direct composite restorations requires demanding technical skills, knowledge on the clinical procedure and perhaps longer chair-time.
While appraising the merits of a dental material for the rehabilitation of the worn dentition, it is not only relevant success and survival data, but also the scope to offer an improvement in the patient's oral health-related quality of life OHIP that should be considered.24 Direct resin composite restorations have been shown to provide an improvement in the patient's oral health-related quality of life with respect to aspects such as with speech,25 and orofacial appearance.26
Given the current evidence base, there is more information available for the direct application of resin composite for the purpose of treating localized and generalized tooth wear than for any other material, or application technique. However, with some exceptions (as discussed below), much of this evidence is limited because of the use of relatively small patient samples and/or shorter observation periods. Mehta et al15 reported on the performance of 1269 direct composite restorations placed in patients with moderate to severe tooth wear, with follow up for 5.5 years. Most of the reported failures were localized deficiencies that were still amenable to repair or refurbishment, and which could also be classified as a non-catastrophic type of failure. At the time of observation, 88.6% of the total restorations were free of any failure. In this study, anterior teeth were reconstructed using the ‘sandwich-technique’,27 receiving a palatal/lingual veneer restoration first, and then a buccal veneer restoration. When the two veneer restorations were not placed in the same treatment session, failure rates were higher. Based on this finding, the completion of direct anterior restorations (palatal and buccal veneer restoration) within a single appointment, is encouraged.
Table 2. How to improve the survival of restorations.
Obtain consciousness of the patient lifestyle (e.g. bruxism, reflux, drinking habits)
Control risk factors, whenever possible
Raise patient awareness that tooth and restoration wear is a lifetime event
Wear occlusal splints whenever tolerated by the patient
Ensure patients attend for follow-up visits, as necessary
Use proven clinical skills and materials
It has also been reported that an increase of up to 5 mm in the vertical dimension of the occlusion (VDO), may be prescribed without the risk of negative effects for the patient.28 In a follow up to the study above,15 using the same sample of restorations, Mehta et al29 reported a significant protective effect against failure with the placement of thicker restorations (while respecting the necessary aesthetic and biological parameters). This protective effect may have been due to the enhanced fracture resistance of the restorations; furthermore, knowing that the material will wear with time, the application of a thicker layer of material (perhaps even thicker than the original form of the tooth) could potentially reduce the longer-term susceptibility to future failure. In this investigation, higher levels of anterior tooth wear (assessed using the Basic Erosive Wear Examination – BEWE) were associated with increased levels failure.29 Such information may be helpful when planning care, and may support the prescription of restorative intervention before the pattern of tooth wear progresses substantially to help ensure the longevity of the restorations.23 However, further work is required in this area.
In another study with a relatively large sample,30 1010 direct composite restorations, mainly placed at the maxillary anterior teeth using a Dahl approach, were evaluated for 8 years. With a mean follow-up time of 34 months, 7% of the restorations failed; chipping or debonding were considered failure. The authors were able to repair or replace over half of the failed restorations, corroborating the repairability of composite resin, as also observed in other studies.14,18
The expectations for the performance of restorations for tooth wear patients should be adjusted for both clinicians and patients once the restorations will likely show early deterioration signs. Lima et al31 evaluated 270 anterior direct composite restorations placed in patients with moderate to severe tooth wear after 3 years. They observed that even as early as 1 month after placement, some signs of deterioration, such as surface irregularities, ditching and small chips, were visible. After 3 years, the surface irregularities had decreased, which was likely to be due to the progression of wear, while the occurrence of ditching and fractures increased. The aesthetic aspects found to be most affected by the deterioration were staining and loss of surface lustre, and for the functional criteria, the most affected were incisal contour and wear and marginal adaptation. Despite the deterioration observed, the restorations still exhibited scores considered clinically acceptable and amenable to repair or refurbishment.
The performance of indirect resin composite restorations for the treatment of tooth wear has also been documented; however, the available data is limited compared to direct restorations. One randomized controlled trial on the performance of direct and indirect restorations for the management of severe tooth wear,32 reported the absence of any significant differences in the survival of direct and indirect palatal surface maxillary anterior veneers; however, for first molar teeth, the indirect tabletop displayed a considerably higher failure rate (3.2 times) compared to direct resin restorations.32
Promising results have been reported on the short-term use of minimally invasive, additive, indirect, nanoceramic restorations (LAVA Ultimate, 3M) on all teeth.33 The 1-year results, which included 568 restorations, showed success rates from 97.2% to 100% (Figure 3).32 Moreover, polymer infiltrated ceramic networks (PICN), also placed in a minimally invasive, additive modality, showed favourable performance after 2 years for restorations fabricated at a mean molar tooth thickness of 0.55 ± 0.021 mm.33 In this study, 2-year survival and success rates of 100% and 93.5%, respectively, were reported (n=192 restorations). PICN materials comprise a previously sintered ceramic network (ceramic skeleton) infiltrated with a polymeric matrix (polymer phase) and have been suggested to offer an elastic modulus analogous to dentine, high mechanical compatibility with enamel and the aesthetic value of ceramic-based materials.
Figure 2. Example of failed indirect resin restoration (adhesive fracture) from a patient from the Radboud Tooth Wear Project.Figure 3. Example of failed nanoceramic restorations from patients from the Radboud Tooth Wear Project. (a) Adhesive fracture; (b) chipping fracture.
Non-resin-based restorations
Adhesive-retained ceramics
Two of the studies listed in Table 1 employed the use of ceramic partial restorations for the rehabilitation of the worn dentition.16,19 Some of the advantages of using ceramic restorations to treat cases of tooth wear are:
Less susceptible to surface wear and discolouration;35
Good biocompatibility and well tolerated by gingival tissues.
Ceramics are prone to failure owing to their brittleness and susceptibility to fatigue fracture.36,37 Although it is possible to have conservative ceramic restorations with minimal preparation, some degree of tooth structure removal is often necessary, especially to provide adequate thickness for the restoration(s) to ensure they offer the required mechanical properties and aesthetic outcome. Ceramic restorations are also costly, more difficult to repair or adjust intra-orally, and inadequate polishing may lead to increased abrasive wear of antagonistic teeth.38,39
Vailati et al19 described an approach where a palatal indirect composite veneer was combined with a buccal ceramic veneer to restore worn anterior teeth. After 6 years, they observed no major failures of the restorations. Minor marginal defects at the junction between the veneers were observed, but these restorations were still considered clinically acceptable, indicating the suitability of porcelain veneers for the improvement of the aesthetically compromised worn anterior dentition. In a prospective clinical study on the clinical performance of lithium disilicate occlusal onlays on posterior teeth exhibiting severe tooth wear,16 the authors reported a 100% survival rate over a period of up to 11 years (mean observation time: 7.9 years). The minor failures observed during the period were occlusal wear in 65% of the restorations, marginal discolouration in 3.9%, and marginal crack formation among 1% of the restorations. All these reported failures were scored as clinically acceptable. However, it is worth noting that the onlays were not placed using an additive strategy, with the need for a moderately invasive preparation form including approximal reduction and some (limited) occlusal reduction.
Crown restorations
Full coverage crowns are considered a more conventional approach, but need traditional tooth preparation to provide retention and resistance form.40 Thus, they do not offer a conservative solution because they are likely to require the removal of tooth structure from an already compromised worn tooth. This type of restoration might seem attractive to some practitioners owing to the relatively lower requirements for maintenance and superior longevity. However, their use often results in higher initial treatment costs, and when they fail, the failures tend to be catastrophic, and are frequently not amenable to repair.18 This is why the latest European Consensus on management of tooth wear states that the restorative treatment for tooth wear patients should be additive, rather than subtractive, and such conventional approaches involving traditional preparations should not be the first restorative choice, but judiciously applied in some cases.7 From the studies listed in Table 1, two studies employed the use of crowns for the rehabilitation of worn dentition with good results, but the repairs were difficult to deal with.17,18
Smales and Berekally18 reported the 10-year performance of metal–ceramic and gold crowns placed in 17 patients with worn teeth. The overall failures for metal–ceramic and gold crowns were 25.2% and only 3.6%, respectively. However, all involved major failures. Of the 65 failed metal–ceramic crowns, 13 were due to loss of restoration, in nine cases, the tooth needed a root canal treatment, and seven teeth needed to be extracted; the three gold crowns failed due to secondary caries, replacement of the crown, and root canal treatment. These types of failures related to lost restorations or pulpal problems and were probably related to the extensive tooth preparations required to accommodate the restorations.
A later clinical trial on the 6-year performance of lithium disilicate and translucent zirconia crowns for the management of 62 patients with extensive tooth wear17 reported a survival rate of 99.7% for both types of ceramic crowns, with no bulk fractures reported even though some crowns had areas of 0.6–1-mm thickness. One lithium disilicate crown exhibited loss of retention, and one tooth that received a zirconia crown exhibited a fracture at the cemento-enamel junction after 3 years. Other observed failures were the presence of apical lesions, minor ceramic fractures, or loss of the crown requiring re-bonding. Furthermore, the lithium disilicate crowns were evaluated as being more aesthetic than the translucent zirconia crowns, which might be especially significant when restoring anterior teeth.
Risk factors
Patients play a major role in the decision to select resin-based or non-resin-based materials. Moderate to severe tooth wear patients are considered patients at high risk of failure. There are known risk factors in children that could lead to tooth wear in adulthood, such as carbonated beverage drinking, the erosive potential of some medicines, gastro-oesophageal reflux and other dietary components.41 However, a clear causal relationship between the consumption of carbonated beverages factors and the progression of tooth wear is still unclear.41–44 Awareness of these risk factors may prevent future erosion, which is the most prevalent type of wear in all ages.45 In that regard, erosion in the primary dentition has been shown to be a predictive factor for erosive tooth wear in the permanent dentition.46,47 It is also well documented that males are more affected, and consume more soft drinks and acidic food variants than females.48 Several risk factors are immutable, and thus, consciousness of this group of patients is important.
Patients reported in Table 1 present a wide mean age range, from 35.3 to 64.9 years old. This means that the selection of the restorative material must take this into account. The sooner a more aggressive treatment is performed, the less sound structure will be preserved. However, if the patient, together with the clinician, decides that it is best to have a non-resin-based material to enhance aesthetic appearance, the risk of possible catastrophic failures must be carefully discussed. Where the patient may opt for direct restorative treatment, they should be clearly advised of the need for multiple repairs during their life cycle. Risk factor reduction is desirable along with the treatment plan. Discussion with the patients about those risks and how to manage future erosion may protect the remaining tooth structure.
In a similar manner, patients with a predominant mechanical aetiological factor for tooth wear (such as grinding or clenching) are most likely to continue to grind and clench after receiving restorative treatment. Among these patients, the prescription of an occlusal appliance might be advisable preventively, as a risk factor reduction strategy. However, creating consciousness of their diurnal bruxing behaviour may be an even more important factor in the preventive strategy.
Conclusions
This overview alludes to a lack of long-term evidence to support the success and efficacy of any given restorative material for the management of tooth wear. The evidence suggests that resin- and non-resin-based materials, as well as direct or indirect techniques can be used to rehabilitate the worn dentition. Restorative treatment should be delayed and executed only when appropriate, and preference should be given to additive restorative options. As per the evidence-base, the likely need for maintenance of the restorations, and the possible merits of intervention to the patient's quality of life should be clearly discussed at the outset.