Aptel S, Lecocq-Teixeira S, Olivier P Multimodality evaluation of musculoskeletal sarcoidosis: imaging findings and literature review. Diagn Interv Imaging. 2016; 97:5-18 https://doi.org/10.1016/j.diii.2014.11.038
Moretti AJ, Fiocchi MF, Flaitz CM Sarcoidosis affecting the periodontium: a long-term follow-up case. J Periodontol. 2007; 78:2209-2215 https://doi.org/10.1902/jop.2007.070117
Grimaldi L, De Santis R, Brandi C, D'Aniello C Mandibular intrabony lesion as first sign of sarcoidosis: case report. Int J Oral Maxillofac Surg. 2004; 33:613-6134 https://doi.org/10.1016/j.ijom.2003.09.012
Batal H, Chou LL, Cottrell DA Sarcoidosis: medical and dental implications. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999; 88:386-390 https://doi.org/10.1016/S1079-2104(99)70049-1
Serrat Soto A, Lobo Valentín P, Redondo González LM Oral sarcoidosis with tongue involvement. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997; 83:668-671
Kasamatsu A, Kanazawa H, Watanabe T, Matsuzaki O Oral sarcoidosis: report of a case and review of literature. J Oral Maxillofac Surg. 2007; 65:1256-1259 https://doi.org/10.1016/j.joms.2005.09.028
Golnik KC Neuro-ophthalmologic manifestations of systemic disease: Rheumatologic/Inflammatory. Ophthalmol Clin North Am. 2004; 17:389-396 https://doi.org/10.1016/j.ohc.2004.05.004
Suresh L, Aguirre A, Buhite RJ, Radfar L Intraosseous sarcoidosis of the jaws mimicking aggressive periodontitis: a case report and literature review. J Periodontol. 2004; 75:478-482 https://doi.org/10.1902/jop.2004.75.3.478
Fritz D, van de Beek D, Brouwer MC Clinical features, treatment and outcome in neurosarcoidosis: systematic review and meta-analysis. BMC Neurol. 2016; 16:1-8 https://doi.org/10.1186/s12883-016-0741-x
Sarcoidosis involving the facial bones is rare; however, it may be identified as mild changes on dental radiographs. Awareness of this pathology is important to ensure early referral. Dental structures (if affected) should be preserved where possible.
CPD/Clinical Relevance: Awareness of the typical presentation of sarcoidosis, and the potential clinical signs, is relevant to dental practice.
Article
Sarcoidosis is systemic multi-organ granulomatous condition characterized by non-caseating granulomas. This condition was first described by Hutchinson in 1875 and was termed ‘sarcoidosis’ by Boek in 1899.1 This condition most commonly affects the lungs, and presents with bilateral hilar lymphadenopathy; 20% of patients are asymptomatic. Multi-organ involvement occurs in moderate and severe cases, and can result in parotid gland enlargement.
Intra-osseous sarcoidosis is rare,2 and typically involves the hands and feet.3 This is termed sarcoid dactylitis (described as Perthes–Jungling disease in classical parlance),4 and involves 7% of cases. Radiographic diagnosis can be challenging because this condition is difficult to distinguish from degenerative arthropathies.4
Intra-osseous sarcoidosis involving the facial bones is rare. The published literature is limited to case reports.5,6 The majority of these report soft tissue lesions affecting the oral mucosa and periodontal tissues. These suggest that sarcoidosis can involve the oral tissues, periodontal tissues with and without bone loss, and the facial bones/alveolar mucosa without oral soft tissue lesions There are few cases reporting on involvement of the facial skeleton and alveolar bone. We present a case in which the dental manifestations of sarcoidosis were managed conservatively, with subsequent improvement in dental health with regression of the sarcoid lesion. This case highlights the importance of early diagnosis, early medical treatment, and limited operative intervention. A review of the literature shows that there does not appear to be a similar case of what appears to be complete resolution of an intra-osseous sarcoid lesion.
Case report
A 50-year-old female was referred to the oral and maxillofacial surgery department in 2015 with a 2-cm persistent, firm and discrete neck swelling. Ultrasound examination demonstrated a discrete lesion in the left parotid tail. A biopsy identified aberrant strands of lymphoid tissue alongside a non-caseating granuloma. This was suggestive, but not diagnostic of sarcoidosis. A repeat biopsy was performed alongside Ziehl–Neelsen and Wade Fite stains to exclude mycobacteria and therefore, tuberculosis. These tests supported the diagnosis of sarcoidosis involving the left parotid gland.
Further investigation by a rheumatologist identified no chest symptoms or lung pathology. Forced expiratory volume (FEV1) was determined to be 120% of the expected range. There was no contributory history, including no known allergies, exposure to pets, dust or mould. The patient had never smoked. Serum angiotensin-converting enzyme (ACE), erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels were increased.
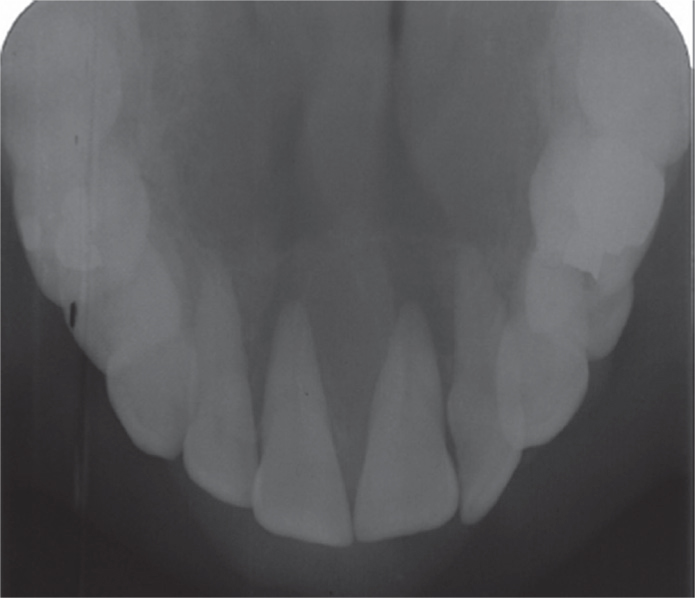
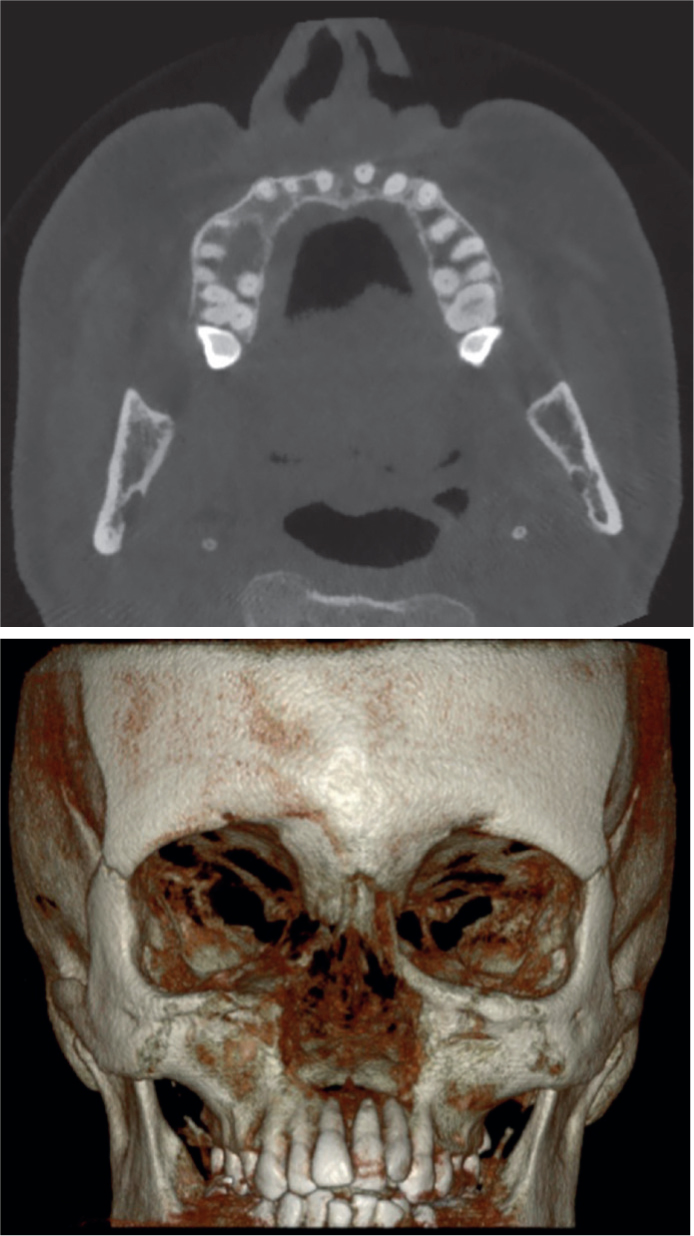
Initial management involved close observation. The lesion progressed over 1 year to involve skin. Hydroxychloroquine treatment was attempted, but ceased following development of an urticarial rash. The region of involvement increased, resulting in nasal obstruction and development of a right cheek lump. Biopsy of the cheek lump confirmed this as a further site of sarcoidosis. The patient complained of mobile anterior teeth and was referred on from dermatology to oral medicine. As part of this referral, an upper occlusal radiograph acquired some weeks earlier by the general dental practitioner was reviewed. This demonstrated a strikingly bland appearance of the anterior maxilla, with complete loss of the normal cortical outlines of the nasal cavity, maxillary antra, nasopalatine canal and lamina dura around the anterior maxillary dentition (Figure 1). Subsequent cone beam computed tomography (CBCT) confirmed extensive bone loss involving a large area of the nasal cavity floor, anterior maxilla and alveolar bone. The extent of this is shown in Figure 2. A biopsy of the lesion identified granulomatous inflammation with no evidence of mycobacterium. Sino-nasal involvement of sarcoidosis was consequently confirmed as the cause of this bone destruction.
Figure 1. Upper occlusal radiograph taken as part of the investigation of mobile anterior teeth, prior to confirmation of sino-nasal involvement of sarcoidosis. There is complete loss of normal bony cortices, including those of the nasal cavity, maxillary antra and nasopalatine canal, as well as the lamina dura around the anterior teeth. The resultant ‘bland’ appearance could easily be overlooked owing to its bilaterality, but is striking when the expected appearance of these structures is known.Figure 2. CBCT volume-rendered image (VRI) acquired prior to commencement of medical management, demonstrates marked bony destruction of the midface with complete loss of the osseous support of the anterior maxillary teeth.
The patient was referred to restorative dentistry owing to persistent pain from the anterior maxilla, pain on biting, and increasing mobility of teeth. The upper anterior teeth were grade III mobile. All pocket probing depths were less than 4 mm indicating an absence of active periodontal disease. There was recession involving the upper anterior teeth and all of these teeth were tender to buccal palpation and percussion. All teeth responded normally to pulp sensibility testing.
Following discussion at a multidisciplinary clinic, prednisolone 30 mg once daily and cyclophosphamide 15 mg/kg as six pulses were prescribed owing to the severity of the sarcoid lesion involving the anterior maxilla. Surgical intervention and dental extractions were considered to be inappropriate because of the extent of the lesion, and the possibility of further degeneration or compromised healing.
Dental health was optimised using primary prevention and professional mechanical plaque removal.
The patient was transitioned to methotrexate 20 mg once daily for 2 years and close monitoring. Anti-resorptive therapy was considered a feasible addition if the extent of osseous involvement increased.
The maxillary lesion was monitored with biennial CBCTs between 2017 and 2022. These demonstrated a progressive return of radiodensity within the dimensions of normal (and pre-existing) bony architecture. This is shown in Figure 3. Mobility of the upper anterior teeth reduced. UL1 was grade II mobile at the previous review, whilet the remaining upper anterior teeth were grade I mobile. Recession and pocket probing depths remained stable throughout treatment. The patient maintained compliance with oral hygiene protocols. Furthermore, pulp sensibility tests remained within normal limits, and no tooth discolouration was noted. Pain from the upper anterior teeth resolved within the first year of medical treatment.
Figure 3. CBCT volume-rendered image (VRI) acquired to assess response to medical management demonstrates significant recovery of bone in the anterior maxilla. Multiplanar reconstructions demonstrated return of normal corticated borders including the nasal cavity floor, lamina dura around the teeth, and nasopalatine canal.
While the upper anterior teeth remain of a guarded prognosis, we have continued to monitor these with supportive care, as the risk for suboptimal healing remains.
Medical treatment involving prednisolone and cyclophosphamide was completed in 2021. The patient was reviewed medically to ensure no recurrence of sarcoidosis. The patient was discharged by the rheumatology team in February 2023. Clinical dental review continues with recall examinations yearly to ensure stability of the anterior teeth.
Discussion
Sarcoidosis is a chronic granulomatous disease of unknown aetiology. Sarcoidosis has an increased prevalence in patients aged between 20 and 40 years, and has a slight female predominance.7 It is also more common in individuals of North African inheritance.8 It most commonly affects the lungs, and rarely involves bone. There is a dearth of evidence reporting improvement following involvement of the facial skeleton including a reduction in tooth mobility.
A provisional diagnosis of sarcoid is typically based on clinical and radiographic features: however, this differential diagnosis is rarely considered, leading to concerns that patients may receive surgical intervention and subsequent disfigurement.9 The radiographic appearance of sarcoid on plain films may show diffuse changes, which may be misinterpreted as a normal radiographic appearance. Knowledge of the appearance of dental anatomy on plain films is important when screening for maxillofacial changes.
The most common presentation of sarcoid in the head and neck region is with cervical lymphadenopathy (commonly as firm and non-tender lumps). Involved nodes have non-specific appearances on imaging. Biopsy is usually necessary to exclude neoplasia. The face and oral cavity should be assessed for swellings and involvement of cranial nerves, although these are rare. Soft tissue lesions associated with oral sarcoidosis are typically non-tender, well circumscribed and firm nodules. These can affect almost any part of the oral mucosa including the tongue.10,11 Cranial nerve involvement can progress to a palsy, altered sensation or hearing loss.12,13,14 There is no consensus regarding the need for further radiographic examination to assess bony involvement.
Furthermore, it is common for ACE, ESR and CRP levels to be elevated.
The majority of sarcoidosis cases resolve spontaneously. In cases where treatment is deemed necessary, this typically involves systemic steroid therapy; however, resolution of sarcoidosis involving bone is unpredictable and slow. Alternatives, such as methotrexate and hydroxychloroquine, have been reported.5,15
We recommend that a conservative approach should be considered. There may be merit in delaying surgical intervention owing to the risk of deformity and progression of disease. While the remaining dentition may have a guarded prognosis, prosthetic rehabilitations would have been challenging, given the morphology of the supporting tissues.