Ryge G, Snyder M. Evaluating the clinical quality of restorations. J Am Dent Assoc. 1973; 87:369-377
Hickel R, Peschke A, Tyas M, Mjör I, Bayne S, Peters M, Hiller KA, Randall R, Vanherle G, Heintze SD. FDI World Dental Federation: clinical criteria for the evaluation of direct and indirect restorations – update and clinical examples. Clin Oral Investig. 2010; 14:(4)349-366
Deligeorgi V, Wilson NH, Fouzas D, Kouklaki E, Burke FJ, Mjör IA. Reasons for placement and replacement of restorations in student clinics in Manchester and Athens. Eur J Dent Educ. 2000; 4:153-159
Manhart J, Chen H, Hamm G, Hickel R. Buonocore Memorial Lecture: Review of the clinical survival of direct and indirect restorations in posterior teeth of the permanent dentition. Oper Dent. 2004; 5:481-508
Blum IR, Jagger DC, Wilson NH. Defective dental restorations: to repair or not to repair? Part 1: direct composite restorations. Dent Update. 2011; 38:78-84
Tyas MJ, Anusavice KJ, Frencken JE, Mount GJ. Minimal intervention dentistry – a review, FDI Commission Project 1–97. Int Dent J. 2000; 50:1-12
Moncada G, Fernández E, Martín J, Arancibia C, Mjör IA, Gordan VV. Increasing the longevity of restorations by minimal intervention: a two-year clinical trial. Oper Dent. 2008; 33:258-264
Setcos JC, Khosravi R, Wilson NH, Shen C, Yang M, Mjör IA. Repair or replacement of amalgam restorations: decisions at a USA and a UK dental school. Oper Dent. 2004; 29:392-397
Gordan VV, Mondragon E, Shen C. Replacement of resin-based composite: evaluation of cavity design, cavity depth, and shade matching. Quintessence Int. 2002; 33:(4)273-278
Banerjee A. “MI”opia or 20/20 vision?. Br Dent J. 2013; 214:101-105
Green DJ, Banerjee A. Contemporary adhesive bonding: bridging the gap between research and clinical practice. Dent Update. 2011; 38:439-450
Palotie U, Vehkalahti MM. Reasons for replacement of restorations: dentists' perceptions. Acta Odontol Scand. 2012; 70:485-490
McAndrew R, Chadwick B, Treasure ET. The influence of a short training program on the clinical examination of dental restorations. Oper Dent. 2011; 36:143-152
Bader JD, Shugars DA. Agreement among dentists' recommendations for restorative. J Dent Res. 1993; 72:891-896
Martin J, Fernandez E, Estay J, Gordan VV, Mjör IA, Moncada G. Management of Class I and Class II amalgam restorations with localized defects: five-year results. Int J Dent. 2013; 2013
Dörter C, Yildiz E, Erdemir U. Effect of operators' skills on increase in cavity volume of restorations. Quintessence Int. 2000; 34:(1)27-30
Burke FJ, Wilson NH, Cheung SW, Mjör IA. Influence of patient factors on age of restorations at failure and reasons for their placement and replacement. J Dent. 2001; 29:317-324
Sardenberg F, Bonifácio CC, Braga MM, Imparato JC, Mendes FM. Evaluation of the dental structure loss produced during maintenance and replacement of occlusal amalgam restorations. Braz Oral Res. 2008; 22:242-246
Lenzi TL, Marquezan M, Bonini GC, Camargo LB, Raggio DP. Repairing ditched amalgam restorations is less time and tooth structure-consuming than replacement. Eur Arch Paediatr Dent. 2013; 14:345-349
NICE Clinical Guideline 19. Dental Recall Guidelines October 2004.
Moncada G, Martin J, Fernández E, Hempel MC, Mjör IA, Gordan VV. Sealing, refurbishment and repair of Class I and Class II defective restorations: a three-year clinical trial. J Am Dent Assoc. 2009; 140:425-432
Cardoso M, Baratieri LN, Ritter AV. The effect of finishing and polishing on the decision to replace existing amalgam restorations. Quintessence Int. 1999; 30:413-418
Fernández EM, Martin JA, Angel PA, Mjör IA, Gordan VV, Moncada GA. Survival rate of sealed, refurbished and repaired defective restorations: 4-year follow-up. Braz Dent J. 2011; 22:134-139
Roberts HW, Charlton DG, Murchison DF. Repair of non-carious amalgam margin defects. Oper Dent. 2001; 26:273-276
Roggenkamp CL, Berry FA, Lu H. In vitro bond strengths of amalgam added to existing amalgams. Oper Dent. 2010; 35:314-323
Fruits TJ, Duncanson MG, Coury TL. Interfacial bond strengths of amalgam bonded to amalgam and resin composite bonded to amalgam. Quintessence Int. 1998; 29:327-334
Leelawat C, Scherer W, Chang J, Vijayaraghavan T, LeGeros J. Bonding fresh amalgam to existing amalgam: a shear and flexural strength study. J Esthet Dent. 1992; 4:(2)46-49
Jessup JP, Vandewalle KS, Hermesch CB, Buikema DJ. Effects of surface treatments on amalgam repair. Oper Dent. 1998; 23:15-20
Giannini M, Paulillo LA, Ambrosano GM. Effect of surface roughness on amalgam repair using adhesive systems. Braz Dent J. 2002; 13:179-183
Özcan M, Koolman C, Aladag A, Dündar M. Effects of different surface conditioning methods on the bond strength of resin composite to amalgam. Oper Dent. 2011; 36:318-325
Özcan M, Schoonbeek G, Gökçe B, Cömlekoglu E, Dündar M. Bond strength comparison of amalgam repair protocols using resin composite in situations with and without dentin exposure. Oper Dent. 2010; 35:655-662
Popoff DA, Gonçalves FS, Magalhães CS, Moreira AN, Ferreira RC, Mjör IA. Repair of amalgam restorations with resin composite and bonded amalgam: a microleakage study. Ind J Dent Res. 2011; 22:799-803
Özcan M, Salihoğlu-Yener E. A technical report on repair of amalgam-dentin complex. Oper Dent. 2011; 36:(5)563-566
Özcan M, Vallittu PK, Huysmans MC, Kalk W, Vahlberg T. Bond strength of resin composite to differently conditioned amalgam. J Mat Sci: Maters Med. 2006; 17:(1)7-13
Cehreli SB, Arhun N, Celik C. Amalgam repair: quantitative evaluation of amalgam-resin and resin-tooth interfaces with different surface treatments. Oper Dent. 2010; 35:337-344
Zoergiebel J, Ilie N. Evaluation of a conventional glass ionomer cement with new zinc formulation: effect of coating, aging and storage agents. Clin Oral Investig. 2013; 17:(2)619-626
Wu CH, Smales RJ. Occlusal wear of a resin-modified glass ionomer cement following three surface treatments. Clin Oral Investig. 2001; 5:26-30
Ivanovas S, Hickel R, Ilie N. How to repair fillings made by silorane-based composites. Clin Oral Investig. 2011; 15:915-922
Özcan M, Corazza PH, Marocho SM, Barbosa SH, Bottino MA. Repair bond strength of microhybrid, nanohybrid and nanofilled resin composites: effect of substrate resin type, surface conditioning and ageing. Clin Oral Investig. 2013; 17:1751-1758
Rathke A, Tymina Y, Haller B. Effect of different surface treatments on the composite-composite repair bond strength. Clin Oral Investig. 2009; 13:317-323
Dall'Oca S, Papacchini F, Goracci C, Cury AH, Suh BI, Tay FR, Polimeni A, Ferrari M. Effect of oxygen inhibition on composite repair strength over time. J Biomed Mater Res B Appl Biomater. 2007; 81:493-498
Gordan VV, Garvan CW, Richman JS, Fellows JL, Rindal DB, Qvist V, Heft MW, Williams OD, Gilbert GH How dentists diagnose and treat defective restorations: evidence from the dental practice-based research network. Oper Dent. 2009; 34:664-673
Pelka MA, Altmaier K, Petschelt A, Lohbauer U. The effect of air-polishing abrasives on wear of direct restoration materials and sealants. J Am Dent Assoc. 2010; 1:63-70
Papacchini F, Radovic I, Magni E, Goracci C, Monticelli F, Chieffi N, Polimeni A, Ferrari M. Flowable composites as intermediate agents without adhesive application in resin composite repair. Am J Dent. 2008; 21:53-58
Özcan M, Alander P, Vallittu PK, Huysmans MC, Kalk W. Effect of three surface conditioning methods to improve bond strength of particulate filler resin composites. J Mater Sci Mater Med. 2005; 16:21-27
Özcan M, Pekkan G. Effect of different adhesion strategies on bond strength of resin composite to composite-dentin complex. Oper Dent. 2013; 38:63-72
Loomans BA, Cardoso MV, Roeters FJ, Opdam NJ, De Munck J, Huysmans MC, Van Meerbeek B. Is there one optimal repair technique for all composites?. Dent Mater. 2011; 27:701-709
Staxrud F, Dahl JE. Role of bonding agents in the repair of resin composite restorations. Eur J Oral Sci. 2011; 119:316-322
Hickel R, Brüshaver K, Ilie N. Repair of restorations – criteria for decision making and clinical recommendations. Dent Mater. 2013; 29:28-50
Papacchini F, Magni E, Radovic I, Mazzitelli C, Monticellia F, Goracci C, Polimeni A, Ferrari M. Effect of intermediate agents and pre-heating of repairing resin on composite-repair bonds. Oper Dent. 2007; 32:363-371
Baur V, Ilie N. Repair of dental resin-based composites. Clin Oral Investig. 2013; 17:601-608
Shaffer RA, Charlton DG, Hermesch CB. Repairability of three resin-modified glass-ionomer restorative materials. Oper Dent. 1998; 23:(4)168-172
Maneenut C, Sakoolnamarka R, Tyas MJ. The repair potential of resin-modified glass-ionomer cements. Dent Mater. 2010; 26:(7)659-665
Pearson GJ, Bowen G, Jacobsen P, Atkinson AS. The flexural strength of repaired glass-ionomer cements. Dent Mater. 1989; 5:(1)10-12
Jamaluddin A, Pearson GJ. SEM analyses of repaired glass-ionomer cements. Asian J Aesthet Dent. 1993; 1:(1)19-23
Banerjee A, Watson T., 9th edn. Oxford: Oxford University Press; 2011
Minimally invasive long-term management of direct restorations: the ‘5 rs’ David Green Louis Mackenzie Avijit Banerjee Dental Update 2025 42:5, 413-426.
Professor of Cariology & Operative Dentistry, Hon Consultant in Restorative Dentistry, King's College London Dental Institute at Guy's Hospital, KCL, King's Health Partners, London, UK
The assessment and operative long-term management of direct restorations is a complex and controversial subject in conservative dentistry. Employing a minimally invasive (MI) approach helps preserve natural tooth structure and maintain endodontic health for as long as possible during the restorative cycle. This paper discusses how minimally invasive techniques may be applied practically to reviewing, resealing, refurbishing, repairing or replacing deteriorating/failed direct coronal restorations (the ‘5 Rs’) and provides an update of contemporary MI clinical procedures.
CPD/Clinical Relevance: The assessment and long-term clinical management of deteriorating/failing direct restorations is a major component of the general dental practice workload and NHS UK budget expenditure for operative dentistry.
Article
What is a ‘failing’ restoration?
A failing restoration can be described as one that has suffered biomechanical defect or damage resulting in immediate or subsequent detrimental clinical consequences to the patient. This may affect the restoration alone (eg bulk fracture, staining etc), the supporting tooth structure (eg fractured cusps, new caries at the tooth-restoration surface (CARS) etc) or, more commonly, both, affecting the collective tooth-restoration complex. Such failure can present as obvious fractures of this complex, possibly detectable active caries associated with restoration/sealant surface (CARS, previously described as secondary or recurrent caries) or can be more subtle, such as marginal discoloration of an anterior aesthetic resin composite restoration or marginal ditching of a posterior restoration.
A number of clinical indices have been developed to help classify the extent of restoration failure, including the Ryge & Snyder Index (1973), useful for research analysis as well as clinical management (summarized in Table 1).1 A more recent classification by Hickel et al (2010) defined the clinical criteria for the evaluation of direct and indirect restorations.2 This index includes three separate groups:
Clinical characteristic
Alpha
Bravo
Charlie
Marginal adaption (MA)
Probe does not catch or has one way catch
Probe falls into crevice
Dentine or base exposed
Anatomical form (A)
Contour follows tooth
Contour does not follow tooth
Overhang
Surface roughness (R)
No surface defects
Minimal surface defects
Severe surface defects
Marginal staining (MS)
No discoloration
<50% circumference discoloured
>50% discoloured
Occlusal contact (C)
Normal
Light
None
Lustre (L)
Shiny/enamel-like surface
Dull/opaque
Aesthetically displeasing
Secondary caries (SC)
No caries
N/A
Caries detected
Aesthetics (four sub-criteria);
Function (six sub-criteria); and
Biology (six sub-criteria).
Each restoration is evaluated against these criteria and given a score out of five, depending on the clinical findings. This classification has been proposed as a tool to evaluate and standardize new restorative materials, a method to determine if restorations require repair or replacement and a quality assessment tool for reviewing dental restorations. This classification has been shown to be more sensitive at determining differences between restorations than older classifications.2 There are a number of challenges, which include the universal uptake of the new classification system and how the scoring equates to long-term survival in longitudinal studies. However, with a degree of operator calibration, the new clinical criteria and scoring system is a flexible method which may reduce the risk of clinically unnecessary restoration replacement.2
A collective summary of those criteria that can be used to assess the extent of tooth-restoration complex failure is presented in Table 2. It must be stressed that this final diagnosis must include patient factors and the clinical/biological impact of the failure. A ‘failing’ restoration in a patient with a low caries risk and low aesthetic demands is likely to be managed very differently from a patient with a high caries risk and high aesthetic demands.2 Indeed, a restoration may present with a detectable defect that results in no medium- to long-term detrimental consequence to the patient. This potentially larger technical failure may be managed differently compared to a more minimal defect with a clear detrimental biological consequence (eg active CARS). Consideration of all factors is imperative before making the decision to intervene operatively. This decision-making process must take into account the patients' expectations and their attitude to taking responsibility for maintaining their personal oral health. Management options and discussions should be documented clearly and this process may be further enhanced by the use of consented clinical photographic records.
Restoration failure criteria
Causes/Comments
Colour match (aesthetics)
Important to get patients' views especially in the anterior aesthetic zone – they may or may not be concerned
Underlying discoloration from stained dentine
Superficial discoloration from margin/surface staining
Underlying discoloration from corrosion products (amalgam)
Aged tooth-coloured restorative materials become stained and discoloured due to water absorption leading to a gradual change in optical properties
Marginal integrity
Loss of marginal integrity (causing plaque stagnation) caused by:
– Long term creep/corrosion/ditching of amalgams
– Margin shrinkage of resin composites/bonding agent
– Margin dissolution/shrinkage of GICs
– Margin chipping under occlusal loading due to poor edge strength
– Presence of margin ledges/overhangs, poor contour
If patient can keep the failed margin plaque- and recurrent caries-free and it is not of aesthetic/functional concern, then this partial loss of integrity may not be a sole cause to repair/replace the restoration
Margin discoloration
Micro-/macro-defects at the tooth-restoration interface will permit exogenous stain penetration along the outer perimeter of the restoration as well as towards the pulp
Poor aesthetics
Is an indication of margin integrity failure
Not necessarily an indication for recurrent caries
Loss of bulk integrity
Restorations may be bulk fractured/partially or completely lost due to:
– Heavy occlusal loading – lack of occlusal analysis before restoring the tooth
– Poor cavity design leading to weakened, thin-section restorations (especially for amalgams)
– Poor bonding technique/contamination leading to an adhesive bond failure and lack of retention
Patients will often complain of a ‘hole in the tooth’ where food debris is trapped – ↑ caries risk
Bulk loss of restoration or occlusal wear may affect the bite/occlusal scheme
Why do restorations fail?
Even when placed in ‘ideal’ circumstances, the majority of dental restorations may be expected to deteriorate gradually and ultimately fail at some future point as a result of the biological environment and functional forces to which they are subjected. Even if the ‘ideal’ principles of tooth preparation/cavity design, material choice, handling and placement are followed judiciously, it is impossible to recreate nature's design for an indefinite period.
The aetiology of failure of the tooth-restoration complex can be divided into mechanical or biological, with the most common biological cause cited as CARS (summarized in Table 3).3 Manhart et al reviewed the clinical performance of direct restorations in the permanent dentition and determined their longevity and annual failure rates. The mean annual failure rates for posterior stress-bearing amalgam restorations were 3.0% and 2.2% for equivalent resin composites. The reasons for failure in this study included secondary caries, fracture, marginal deficiencies, wear and post-operative sensitivity.4 The management of failing restorations is associated with a significant amount of clinical time and replacement of amalgam and resin composite restorations constitutes approximately a quarter of all the conservative dentistry carried out in general dental practice in the UK.5,6,7
Poor cavity design can leave weak, unsupported/undermined enamel margins which fracture under occlusal load
Cavity preparation techniques (burs) cause sub-surface micro-cracks within the grain of enamel prisms, so weakening the surface ultrastructure
Adhesive shrinkage stresses on prisms at enamel surface can cause them to be pulled apart causing cohesive marginal failure in tooth structure and leading to a micro-leakage risk
Adhesive bond to hydrophilic dentine results in a poorer quality bond which hydrolyses over time leading to ↑ risk of micro-leakage
Deep proximal cavities often have exposed margins on dentine. Poor moisture control leads to compromised bonding technique, in turn ↑ risk of micro-leakage
Large restorations will weaken coronal strength of remaining hard tissue
Loss of marginal ridges/peripheral enamel will weaken the tooth crown
Cusps absorb oblique loading stresses and are prone to leverage/fracture
Can cause symptoms of food-packing, sensitivity
Often root-filled, heavily restored teeth (with post-core-crown) under heavy occlusal/lateral loads
Traumatic injury
Symptoms variable (pain, mobility, tenderness on biting) and radiographic assessment useful
New caries at a tooth-restoration gap with plaque accumulation
Detected clinically or with radiographs
Marginal stain is not an indicator of recurrent caries
Can affect a section of margin and not the whole restoration
Heavily restored teeth are more liable to pulp inflammation
Iatrogenic damage or ongoing disease may cause pulp necrosis
Examination of the periodontium required for loss of attachment, pocket depths, bone levels
Can be exacerbated by poor marginal adaptation of restorations (causing plaque and debris stagnation)/margins encroaching into the periodontal biologic width
Factors affecting tooth-restoration outcome
In order to minimize failure and promote clinical longevity, it is essential to appreciate the three fundamental factors which influence the long-term success of direct (or indirect) restorations:
The patient;
The tooth, and
The restoration itself.
Patient factors
The cornerstone to increasing restoration longevity is to reduce failure risk by modifying patient behaviour. Failure to educate and monitor adherence to recommended dietary and plaque control protocols will increase the likelihood of premature restoration failure.4 In many clinical situations, restorations with minor defects may be maintained successfully for many years by good oral hygiene practices alone.
Tooth factors
Preserving the quantity and integrity of healthy tooth tissue and maintaining endodontic health is essential in maximizing the long-term success of operative treatments. The biological impact of replacing restorations should be at the forefront of clinical decision-making.8,9 In a wide range of clinical situations, non-operative reviewing, refurbishment, resealing and repair may be considered superior to complete restoration replacement, in the maintenance of long-term oral health.
Restorative factors
The understanding of MI operative techniques with an appreciation of the histological properties of tooth substrate combined with restorative materials is critical to the long-term success of minimally invasive dentistry.10 It is essential to comprehend that, in the majority of cases, restorations can be repaired periodically with little or no unnecessary, irreversible tissue loss. The quality of the initial restoration placed by the operator has a positive influence on the overall longevity of that restoration. The mechanisms by which direct restorations achieve retention also influences the biological cost to patients. Amalgam restorations, which require macro-mechanical retention in the form of undercuts, slots, grooves and locks, require more destructive cavity preparations compared to adhesive techniques, which generally allow for significantly smaller cavity designs, the form of which is guided primarily by the extent of disease. This offers a more conservative alternative, with ‘adaptable cavity design’ relying on the use of dental adhesives to achieve minimally invasive micro- and nano-mechanical retention.11,12
The operator effect
The subjective diagnosis of restorative failure leads to significant inter-operator variability in its assessment.13,14,15 Complexities arise in the infinite variety of presentations of a failing tooth-restoration complex, coupled with patient factors. Differences in operator gender and system of remuneration have been reported,13 McAndrew et al demonstrated that training clinicians in the assessment and diagnosis of restoration failure increases the accuracy and predictability of decision-making and reduced the frequency of restoration replacement compared to a non-trained control group.14,15
Why repair restorations?
Restoration repair aims to promote tooth-restoration longevity and is less likely to result in detrimental, iatrogenic damage to hard tissues. The pulp, chairside clinical time is reduced and the need for local anaesthesia is often obviated.5,8 Replacing restorations tends to drive the restorative cycle towards failure by removing excessive and unnecessary quantities of natural tooth structure, further weakening the final tooth-restoration complex.16,17Table 4 lists the possible adverse consequences of regular total restoration replacement.
Increased loss of remaining tooth structure
Catastrophic tooth-restoration complex failure
Cusp fracture
Difficulty in re-restoring
Iatrogenic damage
Loss of pulp vitality
Biological width violation
The ‘5 Rs’
Minimally invasive non-operative management options for the failing tooth-restoration complex may be divided into five categories (Table 5):
Reviewing
The monitoring of minor defects, where there would be no clinical advantage to undertaking treatment
Refurbishment
The treatment of small defects present in the restoration which require intervention to prevent further deterioration
Resealing
The application of sealant into a non-carious, defective marginal gap
Repair
The placement of additional restorative material to an existing restoration
Replacement
The removal and replacement of an entire restoration
Review. If only minor defects are evident, such as surface roughness/irregularities without concomitant plaque biofilm stagnation, the restoration can be monitored. The primary factor in deciding to review restorations is that there would be no net benefit from operative intervention. As with all operative procedures, the patient must give informed consent and discussion of management options should be clearly documented. Assessment of the patients' caries risk and their commitment to preventive regimens is imperative. The use of clinical photography is recommended to help monitor restorations and recall frequency is prescribed on an individual patient basis, guided in part by the adherence to home care protocols.
Refurbishment may be indicated if there are small plaque-retentive defects in the restoration, which may be corrected by re-shaping or removal of marginal excess or surface material. The aesthetic appearance of restorations may be improved by refurbishing techniques, such as polishing to increase their functional longevity (Figure 1).
Resealing may be defined as the application of a sealant material into non-carious, marginal defects to reduce the risk of CARS. A variety of resin-based materials may be used and selection is based on the ability of the material to penetrate and seal the marginal defect (Figure 2).
Repair may be defined as the addition of material to a defect in an existing restoration. Repair may require modification or removal of the defective part of the tooth-restoration complex (Figure 3).
Replacement may be defined as complete removal of the existing restoration (Figure 4) before placement of a new restoration. Following diagnosis of the precise mode of failure, the cavity may require modification to enhance the restoration's retention and stability.
Figure 1. A tarnished amalgam restoration (a) refurbished with the use of simple polishing techniques using brown and green amalgam polishing stones (b).Figure 2. A non-carious marginal defect in this resin composite (a) was prepared with air abrasion, etched with 37% phosphoric acid and application of an adhesive bonding agent (b) and a fissure sealant placed (c).Figure 3. Repair of a fractured lingual cusp in amalgam. Retention features were prepared into the existing amalgam and the surface roughened prior to placement to facilitate cohesion (a). Amalgam repair at one year recall (b).Figure 4. Fracture of a buccal cusp in a restored upper premolar (a). The restoration was replaced with a minimally invasive direct resin composite due to the cumulative clinical failings of poor aesthetics and buccal cusp fracture (b).
It is imperative to understand that all the listed management options will require appropriate review intervals based on the individual patient's risk factors.
Contra-indications for repairing restorations
The factors which influence the decision to replace restorations include the quantity of the tooth-restoration complex that is lost and/or presence of significant levels of active caries undermining most of the restoration, especially if previous repair attempts have failed. Care also has to be taken if the existing material type cannot be ascertained, as the outcome of the technical repair procedure may be unpredictable.5 It is assumed that patients with a high caries risk, or those who were infrequent attenders, were less suitable for MI restorative techniques.5 It can be argued equally, however, that these patients would actually benefit more from MI restoration resealing, refurbishment and repair as opposed to multiple replacements.
MI techniques to manage failing direct restorations
Amalgam
Common modes of failure for dental amalgam restorations include CARS,3 tooth fracture and restoration fracture.18 Total replacement is the most common treatment for a defective amalgam restoration and may result in significant further tooth structure loss due to the provision of macro-mechanical retention requiring further cavity preparation.19 Refurbishment, resealing and repair offer a conservative alternative. Refurbishment or resealing ditched amalgam restorations reduces clinical time compared with replacing them and results in increased tooth preservation.20 The success of repaired amalgam restorations at 5 years for the repair of Class I and II restorations was reported to be as effective as total replacement but with less biological cost to the patient.13
Review
If only minor deficiencies are present in the restoration, such as a minimal surface defect, or tarnishing, reviewing the restoration is a sensible management option.21 If there is no clinical advantage to treating the restoration operatively, it should be reviewed.
Refurbishment
Refurbishment or re-finishing existing amalgam restorations is a useful treatment for anatomical form defects.12 Correction of anatomical form and removal of surface roughness are simple, conservative procedures which can enhance the longevity of amalgam restorations22 (Figure 1). In one study, the prevalence of decisions to replace amalgam restorations was reduced by 50% by finishing and polishing alone.23
Reseal
The application of a flowable resin-based material to seal a non-carious marginal gap defect in an amalgam restoration (Figure 5) has been shown to increase the longevity of the restoration.24 Prior to its application, the tooth-amalgam interface can be modified using a variety of techniques, including a rotary bur or air-abrasion, etching with phosphoric acid and application of a dentine-bonding agent.25
Figure 5. A tarnished amalgam restoration with several non-carious marginal leakage defects (one indicated by the blue arrow (a); the amalgam restoration was air-abraded (b); polished (c) and a resin sealant applied to marginal gaps (d). The refurbished and resealed amalgam restoration (e).
Repair
Amalgam restorations can be repaired with amalgam, resin composite or as a temporary/provisional measure with glass ionomer or resin-modified glass ionomer cements.
Amalgam to amalgam repair
Reports on shear bond strength between a newly placed and existing amalgam vary, with some reporting high values26 and others significantly lower.27,28,29 A number of methods have been proposed to increase the bond strength between existing and new amalgam, including macro-mechanical retentive undercuts, slots, pins, grooves, amalgam bonding28 (with a limited evidence base for successful use) and dentine adhesives.30 It is strongly recommended, whichever repair method is used, that the surface of the old amalgam should be roughened prior to the addition of new amalgam with the use of a rotary coarse diamond grit bur or 27–50 µm aluminum oxide air-abrasion, if available.31 The use of macro-mechanical features, such as retentive locks in the existing amalgam, should be considered to support the repair (Figure 6).
Figure 6. A fractured buccal cusp on a lower molar with a large amalgam restoration present (a). A resistance feature was cut into the existing amalgam and the surface roughened with a bur (b). Following immediate amalgam repair and refurbishment (c). Polished repair 5 years post-operatively (d).
Resin – amalgam repair
Resin composite repair of amalgam restorations is considered to be a suitable method providing the appropriate protocol is followed.32 Improved bond strengths have been reported between resin composite and amalgam, with more predictable bonding and less microleakage between the repair-tooth interface and repair-restoration interface compared with an amalgam repair.33,34 However, microleakage at both the restoration and tooth interface compared to that found in bonded amalgams was not eliminated completely. Surface conditioning of the amalgam prior to application of resin composite can be achieved using mechanical, micro-mechanical or chemical means. Micro-mechanical and chemical retention have been shown to be useful in situations where macro-mechanical retention alone is difficult to achieve, such as a fractured cusp on a premolar tooth (Figure 7).35
Figure 7. A fractured buccal cusp on an upper premolar with a large amalgam restoration in situ(a). Air abrasion was used on the amalgam surface and a silane coupling agent. A standard enamel and dentine bonding protocol was used to adhere to the tooth structure and resin composite applied (b). The repaired restoration 5 years later (c).
Various techniques to roughen the amalgam surface and increase micro-mechanical retention prior to bonding composite have been suggested.36 An appropriate method for bonding resin composite to amalgam is using air abrasion on the amalgam surface with silica oxide particles (CoJet-Sand, 30 µm SiO2 3M ESPE AG, Seefeld Germany) followed by a silane-coupling agent, a bonding agent and a resin composite.34 The silica has a tribochemical effect at the amalgam surface and, on application of silane, forms a polysiloxane network, which reacts with resin composite methacrylate groups.35
The type of adhesive has also been shown to influence the microleakage with etch and rinse adhesives (Types 1 and 2; 4th and 5th generation) performing better than self-etching primer adhesives (Types 3 and 4; 6th and 7th generation).37
GIC/RMGIC – amalgam repair
The properties of GIC make it an unsuitable long-term restorative material for load-bearing restorations in posterior teeth, even with newer materials such as Chemfil Rock (Dentsply).38 RMGIC is also unsuitable as a definitive restorative material owing to its increased water absorption and compromised aesthetics.39 Thus, GIC and RMGIC are only suitable for short- or medium-term repairs of amalgam restorations.
Resin composite
In contrast to dental amalgam, resin composite restorations present a more complicated substrate for repair. There is variation in the chemical composition of resin composites' matrix with additional disparities in inorganic filler quantity and type. Resin composites are based on two broad types of resin matrix: dimethacrylate-based or silorane-based.40
Ageing also has a significant effect on the bond strength between new to old resin composite restorations, decreasing with time.41,42 Newly placed resin composites gain cohesive strength owing to the presence of uncured resin monomer at the restoration surface due to air inhibition (the oxygen-inhibited layer). This degrades rapidly on the exposed surfaces in the oral environment due to water adsorption and abrasion and thus prevents further incremental addition of resin composite.43
Dentists have been shown to be more likely to intervene operatively when a resin composite restoration is present in contrast to an amalgam.44 This may be due to a perceived increased longevity of amalgam restorations in general and the lack of correlation between marginal breakdown and the presence of secondary caries adjacent to amalgam restorations.
Review
In parallel with amalgam, if there is no clinical advantage to treating the composite restoration operatively, it should be reviewed (Figure 8).
Figure 8. This resin composite restoration is showing signs of marginal discoloration but was clinically sound. As there was no advantage to operative intervention it was reviewed over a period of 10 years.
Refurbishment
Resin composite restorations can be refurbished where defects are adjustable without damaging the underlying tooth structure.2 Polishing, improvement in surface roughness and anatomical form of Class I and II resin composite restorations have been shown to maintain an improvement at 3 years.22 The use of intra-oral air abrasion devices is a useful technique to refurbish discoloured resin composite restorations by removing superficial extrinsic staining. Lower abrasive powders, such as ClinPro Prophy Powder™ (3M EPSE, Seefeld, Germany), are recommended to prevent excessive abrasion of restorative material (Figure 9).45
Figure 9. Poor aesthetics as a result of non-carious marginal deterioration of the resin composite in an anterior tooth (a). Initial refurbishment carried out with abrasive finishing discs (b). Polished refurbishment has significantly improved the appearance with minimal biological cost (c).
Resealing
Flowable resin composite has been proposed as a method for repairing methacrylate-based resin composite restorations producing significantly higher bond strengths compared to adhesive alone.46 Existing restorations may be air-abraded with aluminum oxide, etched with 37% phosphoric acid, adhesive and flowable resin applied.
Repair
Methods used to condition existing resin composite surfaces prior to the addition of new restorative material include surface roughening with a diamond bur, air-abrasion with aluminum oxide, bioactive glass particles, silica oxide (tribochemical particles), etching with 37% phosphoric acid and etching with 9.6% hydrofluoric acid.47
The literature identifies that one of the most important factors when repairing resin composites is the production of a strong cohesive bond between existing and new resin composites by using compatible materials of the same type, where possible, so producing a more predictable bond.45 As the majority of resin composites consist of similar properties, it is pragmatic to conclude that they can be repaired with any resin composite material. It is clear that operator technique is the most important variable in this repair process and that following a sound MI protocol is integral to producing successful outcomes.
Loomans et al investigated an optimal repair technique for all resin composites.49 The resin composites tested, notably nano-hybrid materials, micro-hybrid composite and hybrid composite containing quartz, exhibited repair bond strengths which varied, depending on the repair method used. A universal repair technique was difficult to achieve but, where the composition of the composite is unknown, a standard protocol would be roughening of the composite with a diamond bur then etching with 37% phosphoric acid for 20s or using air abrasion with silica oxide particles for 20s at a pressure of 1.5 bar at a distance of 20 mm. A combination of an organo-silane (which should be applied for 15s and gently air-dried) and bonding agent (adhesive resin applied for 20s, gently air-dried and cured for 20s) should then be applied prior to the addition of new resin composite.49 The presence of an adhesive was found to improve the strength of repair significantly (Figure 10).50
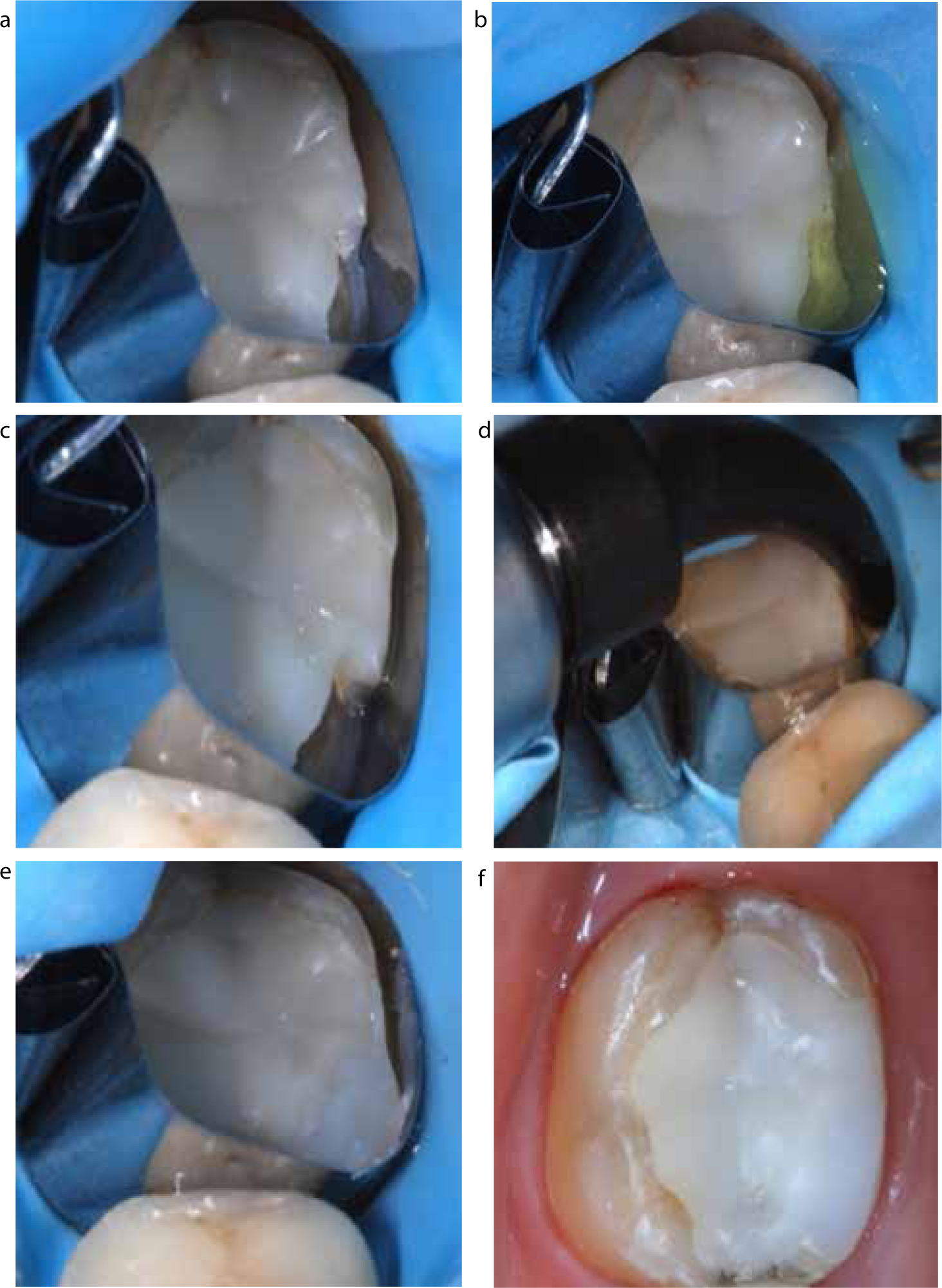
Figure 10. The repair of a fractured resin composite restoration, the restoration was isolated and the surface roughened with a diamond bur (a) or alternatively air-abraded. 37% phosphoric acid was applied and rinsed after 15 seconds (b), a silane coupling agent was applied to the old composite surface followed by an adhesive material which was light-cured (c). Resin composite was applied (d) and polished (e). The repaired resin composite immediately after operative intervention (f).
The mechanism of action of phosphoric acid is believed to be via removing surface contamination and increasing the reactivity of the silica within the composite, which promotes bonding with the silane coupling agent. As phosphoric acid etching does not result in significant increases in micromechanical retention, roughening with a bur is required prior to its application. Air abrasion using silica oxide particles results in mechanical roughening and a tribochemical silica coating promoting bonding to the silane.48,49
With all repair techniques, wherever possible it is recommended to optimize bonding to enamel adjacent to defects.
Repairing silorane-based composites
In parallel with methacrylate-based resin composites, the different surface treatments for silorane repairs have been discussed in the literature.51 The most tested repair technique was the use of a silane coupled with an adhesive in common with the methacrylate-based resin composites.52 The protocol for silorane repair is similar to that of a methacrylate-based material and, as discussed earlier, it is beneficial, but not essential, to use the same type of material where possible.51 Baur and Ilie investigated the effect composites of different chemical composition (methacrylate-based, silorane-based and ormocer-based) when used to repair each other. Interestingly, the silorane-based composites showed the highest bond strength when applied to the composites consisting of different chemical composition.53
Resin-modified glass ionomer cements (RMGICs)
In contrast to amalgam and resin composite restoration repair, techniques to repair RMGICs are scarce on account of their use as a provisional restorative material. The bond strength and thus repair potential of RMGIC with RMGIC decreases with time. Direct repair with RMGICs, even with prior roughening with a coarse diamond bur and application of phosphoric acid or polyacrylic acid, showed marked variation between brands, indicating unpredictable results with RMGIC-RMGIC bonding.54
Resin composite bonding produces more predictable bond strengths and is considered a more reliable method of repair. Thus, conversion of the original restoration to a RMGIC–resin composite laminate/layered/'sandwich’ restoration is the method of choice. Modifying the surface of the RMGIC prior to application of the resin composite with a bur was superior to phosphoric acid etching.55
Replacement of RMGIC
The total replacement of RMGICs is a more likely clinical occurrence than temporary repair due to it being an unsuitable long-term restorative material. A minimally invasive approach should consist of removing the restoration and conforming, where possible, to the cavity design, which is likely to involve an adhesive restoration such as resin composite (Figure 11).
Figure 11. Failure of a glass ionomer material which is unsuitable for load-bearing restorations (a). Total replacement with a resin composite restoration (b).
Glass ionomer cements (GICs)
The highest bond strengths of GICs were on newly set surfaces, which decreased with time, so the long-term viability of GIC repair is unknown.56
If the repair of temporary/provisional GIC restorations is necessary the application of phosphoric acid or roughening the surface followed by etching produces the highest bond strength prior to further GIC placement.57 Again, conversion of the original restoration to a GIC–resin composite laminate/layered/'sandwich’ restoration is often the method of choice, thanks to the more reliable bonding procedures between old GIC and new resin composite.
Summary
Utilizing the principles of minimally invasive dentistry (‘5Rs’: reviewing, resealing, refurbishment, repair and where necessary, replacement) encourages the preservation of tooth structure and maintenance of endodontic health, so extending the clinical life of the tooth-restoration complex. Current clinical evidence indicates that the ‘5Rs’ checklist described in this paper should be contra-indicated before justifying the total replacement of a failing direct restoration.
If amalgam to amalgam bonding is necessary the surface of the existing amalgam should be roughened with a coarse grit diamond bur or wet aluminium oxide air-abrasion. Amalgam bonding procedures have not shown any clinical benefit in the literature.
Resin composite repairs are more predictable and result in less microleakage.
For successful resin composite repair, the amalgam should be roughened with a diamond bur or air abraded with silica oxide. An organo-silane should then be placed followed by dental adhesive and finally resin composite.
A universal approach includes the use of diamond bur roughening, etching with 37% orthophosphoric acid or air-abrasion with silica oxide/bioactive glass powders. A silane-coupling agent should then be placed followed by dental adhesive and fresh resin composite.
The repair of temporary RMGIC is best achieved with initial surface modification with a coarse grit diamond bur followed by application of dentine adhesive and addition of a resin composite.
If a temporary/provisional GIC repair is necessary the surface should be roughened with a diamond bur or phosphoric acid etch prior to fresh GIC placement. Otherwise, addition of a resin-composite surface veneer (laminate restoration) should be the method of choice.