Raskin R, Terry H. A principal-components analysis of the Narcissistic Personality Inventory and further evidence of its construct validity. J Pers Soc Psychol. 1988; 54:890-902 https://doi.org/10.1037//0022-3514.54.5.890
Diagnostic and Statistical Manual of Mental Disorders, 5th edn. Arlington VA, USA: APA; 2013
Pinchi V, Barbieri P, Pradella F Dental ritual mutilations and forensic odontologist practice: a review of the literature. Acta Stomatol Croat. 2015; 49:3-13 https://doi.org/10.15644/asc49/1/1
Kelleher MG, Djemal S, Lewis N. Ethical marketing in ‘aesthetic’ (‘esthetic’) or ‘cosmetic dentistry’. Part 1. Dent Update. 2012; 39:313-324 https://doi.org/10.12968/denu.2012.39.5.313
Sampson A, Jeremiah HG, Andiappan M, Newton JT. The effect of viewing idealised smile images versus nature images via social media on immediate facial satisfaction in young adults: a randomised controlled trial. J Orthod. 2020; 47:55-64 https://doi.org/10.1177/1465312519899664
Narcissism, pride, envy, lust and dentistry Martin Kelleher J Tim Newton Dental Update 2025 50:11, 914-922.
Authors
MartinKelleher
MSc, FDSRCS, FDSRCPS, FCGDent
MSc, FDSRCS, FDSRCPS, FDSRCS, FCGDent, Specialist in Restorative Dentistry and Prosthodontics, Consultant in Restorative Dentistry, King's College Dental Hospital, London
Platforms such as Instagram have normalized self-adulation and this has affected many patients, and some dentists, in different ways. Some posts demonstrate excessive pride in the appearance of the mouth or face, and seem designed to induce envy in others. The resultant emotional impacts on envious followers can increase demands to have a similar sort of appearance, which can lead to over-treatment, or to potentially dangerous procedures being carried out on their mouth and face regions. This article explores the nature of narcissism and the increasing likelihood of it being ‘normalized’ as one significant factor in the increased demand for, and the delivery of, some questionable dental, oral and/or facial treatments. We outline how the narcissistic traits in some dental healthcare professionals might lead them to undertake elective, biologically risky, and irreversible procedures, which can invoke ‘the law of unintended consequences’ for patients and/or themselves. The terms ‘destructodontics’ ‘relapsodontics’ and ‘alignerodontics’ are suggested as being appropriate descriptions for some dentistry, which is carried out mainly for appearance reasons, but which can produce long-term biological and other problems.
CPD/Clinical Relevance: The normalization of narcissism, as demonstrated by some posts on Instagram and other platforms and in dubious advertising has many worrying implications and possible consequences for patients and the dental profession.
Article
Most people have some narcissistic characteristics, including the present authors. Narcissism is best viewed as a continuum, with the majority of patients and dentists being somewhere around the middle of a normal distribution (‘Bell’) curve. However, some people with serious narcissistic traits, including dental professionals, can pose significant problems.
Narcissists seek attention, praise and/or admiration from others. Many seek external validation from others (‘likes’), and some exaggerate their appearance, social experiences or accomplishments to achieve this. Narcissists can be passive–aggressive and self-critical, but many are hypersensitive to even mild external criticism. They can be arrogant and entitled (‘pride’), but not all appear so at the first encounter. Narcissists are often manipulative and hold grudges, and many are excessively envious of others (‘envy’). Some ‘lust’ after a facial or smile appearance that is to their exact specifications (to match their ‘brand’), and which they are convinced is their absolute right.
Some dentists, probably those with increased narcissistic tendencies themselves, appear to lust after lots of money (‘greed’), or for greater power, and/or for wider recognition of their artistic or other talents.
However, any failure to achieve a narcissistic patient's expectation of achieving their desired outcome, even if it was unrealistic and previously unexpressed, risks complaints, general aggravation and sometimes litigation.
This article outlines some of the problems involved, and makes some suggestions about how to identify patients (and dentists) with significantly increased narcissistic traits in order to reduce some of the dangers involved.
History, definition and characteristics of narcissism
Narcissism is named after a mythical Greek character called Narcissus who walked beside a pool of water and stopped to take a drink from it. He saw his own reflection in the water and became completely entranced by it. He killed himself because he could not have his object of desire.
Narcissism is defined as ‘… a grandiose sense of self-importance or uniqueness; a preoccupation with fantasies of unlimited success, power, brilliance, beauty, or ideal love; exhibitionism; an inability to tolerate criticism, the indifference of others, or defeat; entitlement, or the expectation of special favours – without assuming reciprocal responsibilities; interpersonal exploitativeness, relationships that alternate between extremes of over-idealization and devaluation; and a lack of empathy.’2,3
Please note that ‘fantasies of unlimited…beauty’ are included in this definition. That means that someone with increased narcissistic traits is likely to seek dental and facial aesthetic enhancement treatments because that is the interface where health and beauty issues collide.
Narcissism can be conceived of as a continuum, with the most extreme manifestation being a psychiatric disorder called ‘narcissistic personality disorder’ (NPD), which is described in the Diagnostic and Statistical Manual of Diseases (DSM-5) (Table 1).4
Table 1. Diagnostic criteria for narcissistic personality disorder (adapted from DSM-5).4
A pervasive pattern of grandiosity, need for admiration and lack of empathy. Begins in early adulthood and presents in a variety of situations. It is indicated by five or more of the following:
▪ Grandiose sense of self-importance (exaggerates their achievements and talents, expects to be recognized as superior without matching achievements)
▪ Preoccupied with fantasies of unlimited success, power, brilliance, beauty or ideal love
▪ Believes that they are ‘special’ and unique, that they can only be understood by, or should associate with, other high status individuals or institutions
▪ Requires excessive admiration
▪ Sense of entitlement
▪ Interpersonally exploitative
▪ Lacks empathy
▪ Often envious of others or believes others are envious of them
▪ Arrogance
Because these criteria are used for the diagnosis of a psychiatric disorder, they focus mainly on the behaviour of the individual and tend to ignore the underlying thought processes that relate to the disorder. Those thought processes give some insight into the characteristics of the individual. Any dental professional considering doing any elective treatment, which would change someone's appearance significantly, should be alert for potential patients, who, while they would not fulfil the criteria for classic NPD, nonetheless display significant signs of narcissism.
Many people exhibit milder versions of the characteristics outlined in Table 1.4 However, these become really problematic when they impinge upon an individual's ability to engage in socially, legally and/or morally appropriate actions.
Problems and issues related to narcissism in dentistry
We are all somewhere on a spectrum of narcissism. Most of the time, we try to look presentable in public and to project an appropriate image. We wear clothes and other things that we think are suitable, and we do enough grooming for the situation. However, most of us do not dwell inordinately on the current fashion, nor consider our facial or dental appearance as being the most important thing in our lives. Positive well-being and self-esteem are good things, and helping patients to achieve and maintain those are among many of the traditional aims of ‘decent dentistry.’
Genuine self-esteem (along with authentic pride) is positively related to successful social relationships and mental health. However, narcissistic self-aggrandizement (along with hubristic pride) is often co-related with aggression and some other antisocial behaviours.
Some individuals, including dentists, now seem to regard the area around the mouth and its contents as being a sort of fashion accessory. Some ‘consumers’ seem to think that their teeth should be made available to them in any positions, shapes, colours or modifications that they desire in order to suit their current ‘brand image’, and some dentist's post on social media what was done to achieve these appearance changes.
Some very image-conscious individuals will go to considerable lengths and costs, often involving unnecessarily destructive or unstable dentistry, or having Botox, or sometimes unproven fillers injected in to their lips and/or elsewhere in order to achieve their desired ‘look’ and thereby, lead or belong to their current chosen ‘tribe’.
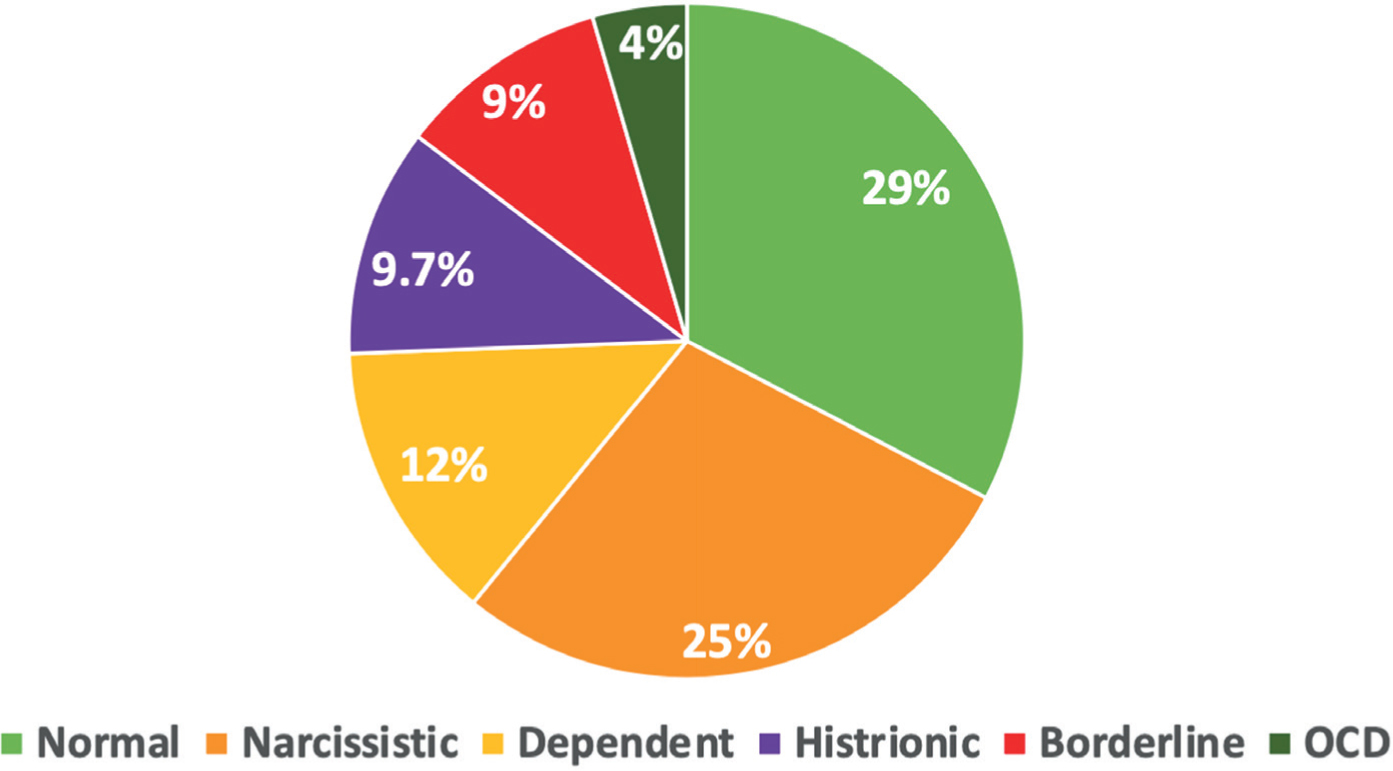
Seductive advertising on all media by some companies, and/or by some dentists, of various allegedly ‘cosmetic’ treatments to achieve a supposedly ‘perfect smile’ can feed into those perceptions. This can result in some individuals with narcissistic traits seeking speculative, potentially problematic, treatments from ‘cosmetic dentists,’ or ‘facial aesthetic’ enthusiasts, who just might be providing them for very mixed motives. However, the plastic surgery literature contains stark warnings. Approximately 50% of patients presenting for plastic surgery have a recognizable personality disorder.5 It is likely that there will some similarities in those people actively seeking out extensive dental or facial appearance-altering treatments.
Meaning of ‘cosmetic’ and the beauty business
The word ‘cosmetic’ is derived from the Greek ‘cosmetikos,’ meaning an adornment. Strictly speaking, a ‘cosmetic’ should be temporary, superficial, transient and have to be applied every time one wants to achieve an effect, for example lipstick or eyeshadow. If one did not apply it, one would not have the desired effect. A cosmetic should not adhere long-term to the underlying surface, nor alter it irreversibly, nor damage it. Above all, a true cosmetic ought to be readily reversible.
The global beauty industry is worth about £360 billion, or roughly 170 times what the UK government contributes (NB not ‘authorizes’) for the whole of NHS dentistry.
L'Oréal tops that list, followed by Gillette, Nivea, Estée Lauder and Clinique. Lipsticks of different colours are true cosmetics. They are temporary, superficial, transient and readily reversible. However, it is increasingly common for various fillers and chemicals, which are not readily reversible, to be demanded and used to produce exaggerated lip sizes, shapes and colours.6 The lack of effective regulation of the wide variety of facial fillers and products now being used is now a major concern, particularly as some of the supposedly non-resorbable fillers are known to disappear in to the fascial planes of the face and neck, with known and unknown long-term consequences.6
Overfilled lips often draw attention to the mouth to reveal an alleged ‘Hollywood smile’ featuring big, usually ‘lavatorially white’ ceramic veneers or crowns, arranged in a repetitively formulaic pattern. Strictly speaking, such things should not be called ‘cosmetic’ because they are not readily reversible
Changing faces and smiles
Changing various aspects of facial or dental appearance is not new, nor is it limited to Western cultures. Mutilation, sharpening or removal of teeth often have social and anthropological significance, which can be influenced by geographical, religious and/or cultural factors. Dental ritual mutilations were, and are, practised for religious and tribal ritualistic purposes, for aesthetic reasons and/or because they represent a symbol of status, or signify belonging to a particular social group or tribe.7
One might argue that the current fashion for some ‘consumers’ to demand exaggerated lips, or strikingly obvious teeth, and/or oral and facial piercings and tattoos is rooted in their desire to appear to belong to their chosen tribe or cult. However, many responsible dentists are concerned that mutilating sound natural teeth rapidly by using a high-speed drill to provide someone with brittle ceramic restorations, or some other material quickly, under the cover of satisfying consumer demand for their version of a ‘perfect smile,’ borders on an abuse of professional privilege.
Some posts on Instagram (e.g. by Beverly Hills' dentist, Connolly, about Post Malone; Figure 1) have normalized gross dental destruction to produce what some might regard as an exercise in personal autonomy and a fashion statement by the patient (but also perhaps by the treating dentist), but for others, it might emit a faint whiff of rewards-driven ‘destructodontics’.
Figure 1. Post Malone's dental appearance changes and their costs were described by his dentist, Dr Connolly, in one of his posts. The hip-hop superstar's subsequent album was entitled ‘Twelve Carat Toothache’.
Narcissism and ‘destructodontics’
‘Destructodontics’ is that branch of dentistry, not taught in any reputable dental school, which promotes the wilful destruction of sound tooth structure in order to replace it with ceramic or other unproven materials. Those who practice it are called ‘destructodontists’ and many are not shy or retiring, as judged from some of their self-congratulatory Instagram posts.
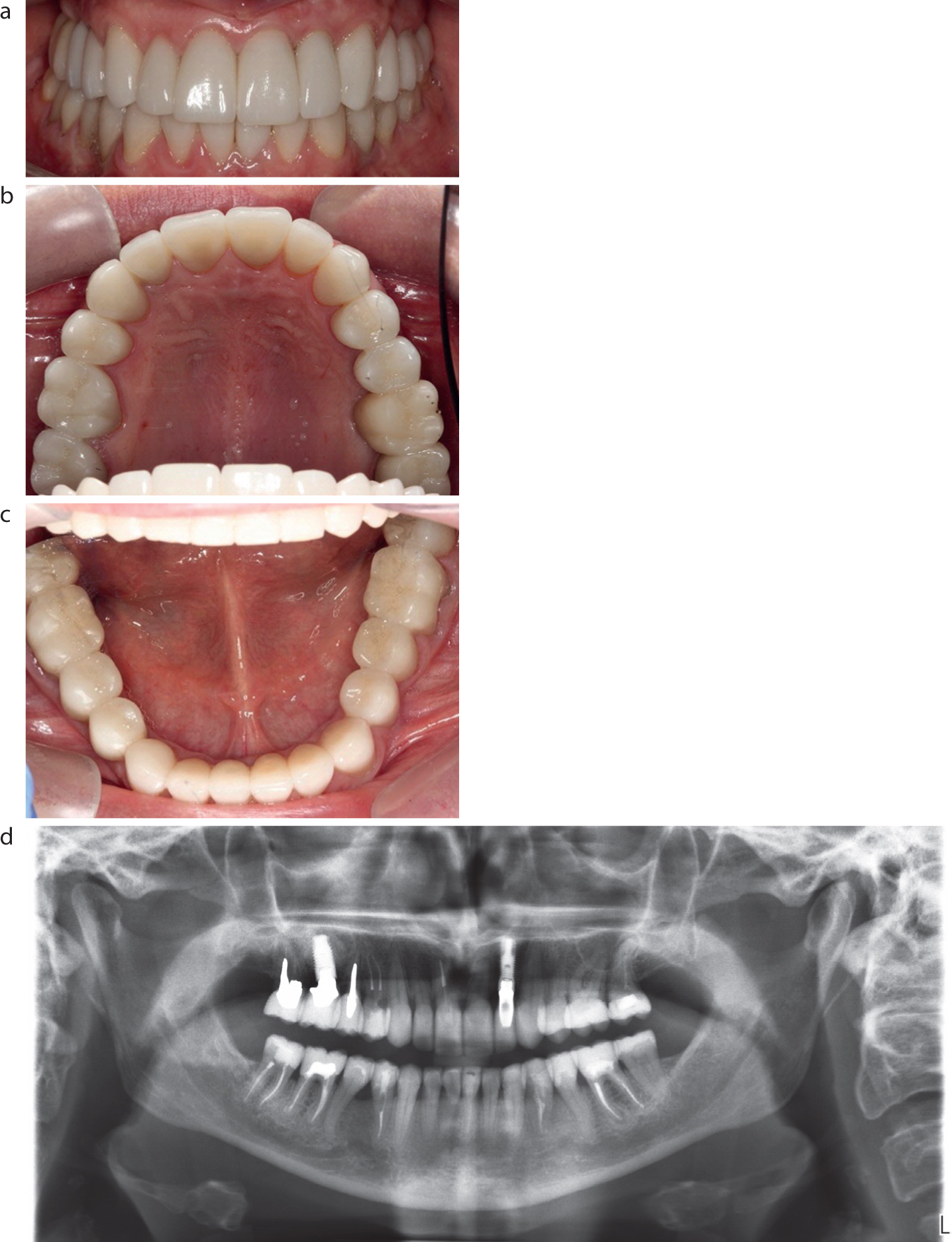
Many seem impervious to any scientific, biological or ethical criticisms about the long-term consequences of their elective actions. For instance, Figure 2 shows an example of a ‘ceramic cemetery’ where formerly sound teeth were murdered first, root-filled or disposed of next, and then buried under ceramic and, presumably, all done in pursuit of a ‘Hollywood smile’ by some well-intentioned ‘cosmetic dentist’.
Figure 2. (a–d) A ‘ceramic cemetery’ where the remains of formerly sound teeth were buried. Some were killed and root-filled first. Others were assassinated and then removed, possibly in order to cure the patient of their ‘titanium and ceramic deficiency disease’. This was the result of the third ‘rehabilitation’. The patient was seeking legal redress.
None of that skilfully done dental mutilation looks particularly ‘readily reversible’, which should be the hallmark of a ‘cosmetikos’ (as discussed above). Possibly narcissistic destructodontists are rarely troubled by self-doubt or overly concerned about pulp health or basic structural engineering principles, just so long as their benefits for doing any requested treatments are rewarded adequately, possibly in different ways.
Increasingly some dentists, perhaps for mixed motives, seem eager to address the demand/fashion for elective dental changes using destructodontics and/or unstable ‘alignerodontics’, or both. Some imply through the use of websites and posts as electronic word of mouth (‘ewom’), that they are able to produce a ‘perfect smile’ quickly, predictably and to any patient's prescription, even in those patients who they have not yet examined, and who might be blissfully unaware that they had any real problems, until some smooth ‘cosmetic dentist’ draws their attention to some minor flaw – as that dentist perceives things.
It might be because some dentists genuinely want to help an individual to achieve their version of beauty, and they believe very strongly that every patient has an absolute right to exert their autonomy about altering any aspect of their body, regardless of any adverse long-term outcomes, provided that they genuinely understand what is involved enough for their consent to be valid. However, it could be partly because they have significant narcissistic traits themselves. While some dentists enjoy doing extensive elective dentistry for artistic and personal satisfaction, others might lust after serious financial rewards, or a perceived social status as a ‘celebrity dentist’.
Whatever the possible mix of reasons involved, few dentists have received formal training in the relevant psychological evaluation of patients before undertaking extensive, elective and irreversible procedures for potentially very demanding patients. Some technical tips might be gleaned from attending a weekend course near an airport on how to achieve a formulaic ‘Hollywood smile’, or possibly by worshipping at the feet of some guru in some dubious academy or institution, some of which promote very precise tooth destruction under various largely unscientific, pseudo-academic, guises.
A failure to assess properly the potential dangers of serious narcissistic traits (or other psychiatric problems) being present in a patient, before undertaking elective irreversible, allegedly ‘cosmetic treatment’ can pose all sorts of unexpected problems later on. These can include multiple extra time-consuming treatments and technical costs to try to resolve what the treating dentist would then term ‘unreasonable demands’, often realizing too late that the patient's real problems are located north of their maxillary plane.
Prolonged and distressing legal or regulatory consequences can follow (Figure 2).8
Assessment prior to elective irreversible facial or dental changes
The changing trends, demands and requests from different patients pose complex, difficult and dangerous conundrums for many dentists.8
The possible reasons for demanding those changes now might include a desire to have their currently perceived ideal ‘look’ for an important social event, or to improve their attraction for others, and/or social status.8 The exact drivers for a particular individual to want to change their smile and/or their facial appearance immediately need to be determined in advance of treating them irreversibly. Divining those real reasons requires time and appropriate skills because they are likely to be subjective and complex. An ethical clinician should give neutral balanced information to the patient so that the patient can assess their material risks and the potential benefits of different approaches to their issues as they perceive them.9 Patient questions need to be answered honestly, and enough time ought to be allowed between consultations for someone to evaluate their realistic options in an unhurried manner in order for their consent to be valid.9
Visualizing the outcome in advance and ‘Montgomery consent’
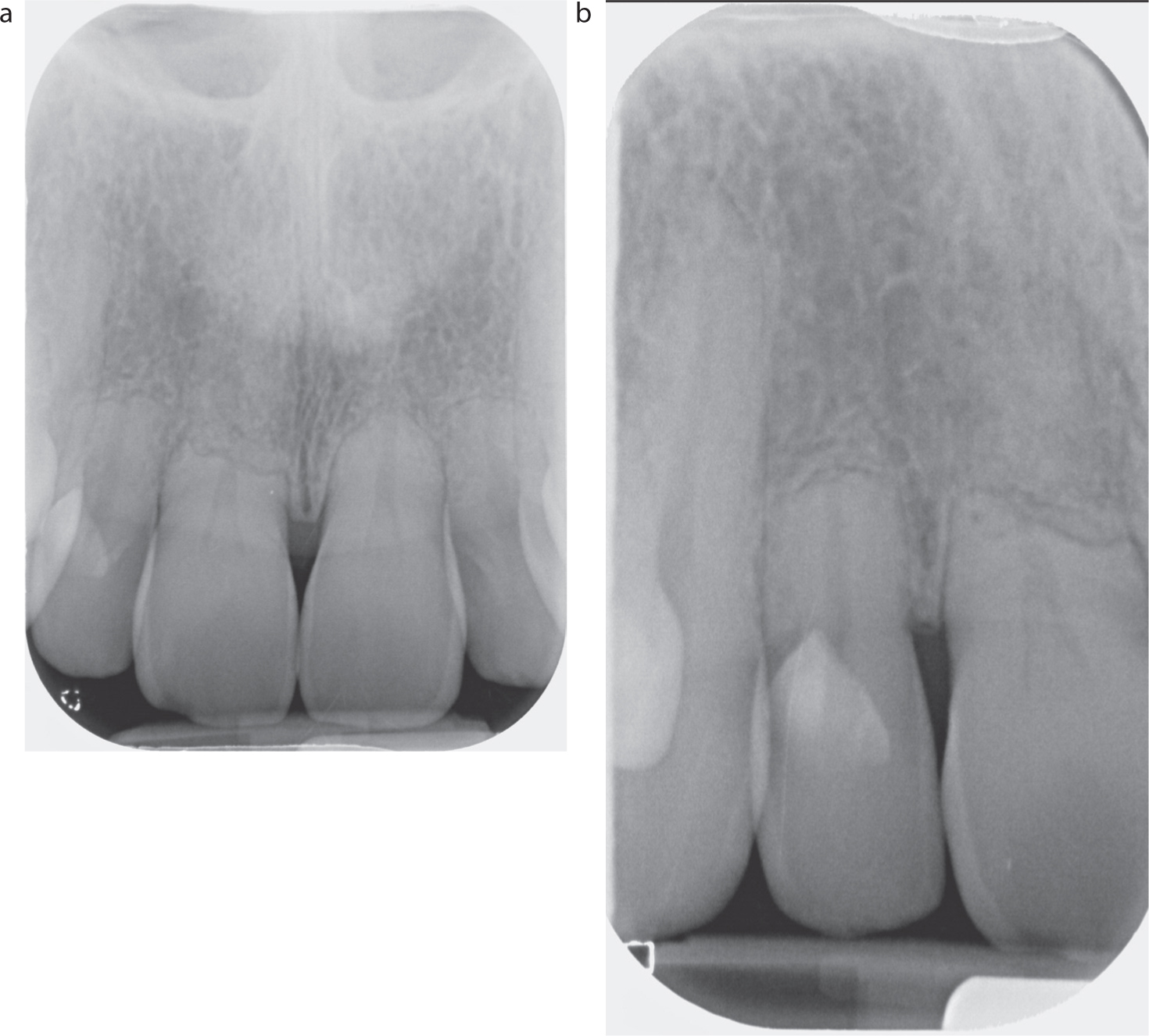
A direct composite mock-up, carried out quickly on the dried (not etched) teeth is often a swifter and safer way to assess patients and their likely demands than time-consuming and expensive laboratory wax-ups or using some slick computer software, which often bears no relationship to clinical reality without doing serious dental destruction. If that mock-up it does not impress the patient quickly, it is often safer to flick off the cured composite and walk away. If it does impress them (even though it is unfinished or polished), then some clinical photographs (including some taken on the patient's phone of ‘before and after’) acts as a record of what has been promised – no more and no less (Figure 3).
Figure 3. (a,b) Montgomery consent issues.9 A chilled hybrid composite mock-up, carried out on the dried (not etched) enamel of this bulimic patient's eroded upper teeth gave her a realistic chance to assess one of her options. This was an additive composite approach to protect her teeth and produce a modest improvement, as opposed to the ‘measuring and monitoring with BEWE’ approach that her dentist had been adopting for many years. Incidentally, in this situation the composite is being used as a ‘cosmetic’ because it is temporary, superficial and readily reversible at this stage.
Occasionally, the mock-up can be left for any ‘significant others’ to assess it before getting the patient to flick it off later using a nail file.
Unstructured appraisal
An experienced dental clinician, faced with a potential patient, might just get an uneasy feeling of something ‘not being quite right’. That sixth sense often provides a valuable early protective warning.
One should concentrate on, and record, two aspects of the individual's behaviour:
How does the person talk about other people? Generally, people with narcissistic traits do not have empathy for the feelings of other people. It is worth asking questions about the individual's perception of how others might perceive them, or the treatment being considered, such as ‘Do you think most people would want that treatment?’ or ‘How many people do you know who have had these treatments?’ and ‘What do your friends, partner or family think about you having those sorts of treatments?’
How does the other person make you feel? It is a common reaction to find that people dealing with someone who has narcissistic traits feel themselves belittled or devalued, as if they are unimportant.
The clinician should trust their initial ‘gut feeling’ about that potential patient's behaviour and how they feel themselves respond emotionally to it. Ask yourself: ‘honestly, do I really want to be feeling like this all the time that I am treating this person’ and/or ‘will I be quite happy treating this person?’ If the answer is ‘no’ to either question, then think carefully before getting involved further, because they could well turn out to be the ‘patient from hell’ for you.
Structured history taking
Structured history taking is important in detecting serious narcissistic traits early on. Open questions are a good start, and can help greatly, but only if the answers are listened to attentively, without interruption, with the whole clinical team keeping their eyes and ears fully open, but keeping their mouths largely shut, while being ‘fully present’ throughout.
It is important to concentrate particularly on non-verbal clues and body language, and focus intently on any inconsistencies, curiosities or apparent contradictions. That is because there is often a complex picture unfolding, which includes subtle psychological and emotional revelations about the patient's perceptions based on their information to date, and possibly influenced by social media, thereby raising various consent issues.9,10
One should record the exact words chosen, and how they are used, while focusing on interpreting correctly that individual's artistic, fashion or cultural beliefs. Clarification and confirmation are vital to check that one has understood that individual's perspectives correctly. Into that maelstrom of immeasurables, a dentist now has to add in their own feelings, opinions, beliefs, business pressures, ethical responsibilities, and factors such as legal concerns.8,9,10
Complex, time consuming and difficult? You bet. However, one useful idea to screen for concerns in any potential patient who requests significant elective changes to their smile or face is to get them to complete a document, in their own time, preferably well away from the practice, using some simple visual analogue scales. Such a form could be something uncomplicated, such as Table 2, but there are others available, which can be modified and validated, as desired.
Table 2.
If there are any serious concerns raised by the details completed on the form, then more detailed evaluation by an appropriately skilled individual is indicated.
Structured assessment tools for narcissism and NPD
Narcissism can be difficult to identify because the individual, particularly those who have an ability to manipulate their ‘self-presentation’ may mask their grandiose ideas and sense of entitlement. Typically, that mask is not resistant to adversity or challenge, and often falls off if the individual is denied something to which they feel entitled.
The gold standard for assessment of narcissistic personality disorder (NPD) is a structured psychiatric interview. Traditional questionnaire measures also exist, such as the Narcissistic Personality Index.2,3
Those are useful in screening for individuals who should be referred for more formal assessment well in advance of undertaking any significant appearance-altering treatments for them.
Narcissism, ‘information’ and the responsibility to disclose material risks for ‘Montgomery’ consent9
Social media and internet sites can lead to people seeking inappropriate dental treatment in two main ways: through inducing dissatisfaction; and through normalizing narcissism. Previous research10 has identified that the high standards of physical appearance portrayed in social media and on internet sites (often the result of photo-manipulation) can induce dissatisfaction and low mood in individuals, particularly those who are vulnerable to associating their self-esteem with their appearance. This can certainly have the effect of directing such individuals to seek extensive elective treatment.11,12
Social media can provide a standard of superficial visual ‘excellence,’ to which an individual with narcissistic traits will feel entitled, and therefore seek treatment to achieve that, while often providing an outlet for their grandiose self-acclamation.
Some patients wishing to have significant changes made to their appearance have erroneous beliefs that ‘cosmetic’ dentistry and facial aesthetics are predictable and largely risk free.11,12 Some of those perceptions can be based on misinformation and disinformation, both of which are readily available on various platforms and provided quickly by typing in key words into search engines.
Unfortunately, the words misinformation and disinformation often get used interchangeably; however, there are marked differences in the meaning, based on the intent involved. Misinformation is information that is false, but the person who is disseminating it believes that it is true. Disinformation is information that is false, and the person who is disseminating it knows that it is false. Disinformation involves telling a deliberate lie to deceive people (such as using propaganda in wars).
Unfortunately, variable amounts of both appear on the internet, on television, in the content of some journals (including advertisement-strewn dental journals), and also on some dentists' websites.
Some dentists' glossy websites can create the illusion that they can cure all the real and imagined dental and appearance problems of people they have never met, let alone examined properly. Many omit ‘extraneous negatives’ about significantly destructive or fundamentally unstable treatments, while highlighting the visual benefits, presumably to improve ‘consumer uptake’. Commercial designers of websites are not, however, under the same duty of care as healthcare professionals, who are obliged, ethically and legally, to give the balancing negative information to potential patients, and to inform them properly of the various benefits, risks, alternatives and doing nothing (‘BRAN’), even if doing that does not result in a lucrative sale.8,9
Unfortunately, some naïve dental professionals are vulnerable to much of the misinformation and disinformation being spouted by charismatic ‘gurus’, or by surreptitiously sponsored key opinion leaders (‘KOLs’), at various conferences, or online, or in WhatsApp groups, or in chat rooms. Some KOLs are paid, directly or indirectly, to promote unproven products or techniques for curing patients of their supposed ‘ceramic deficiency syndrome’ or some invented ‘cosmetic disease’.
It was Peter Drucker, a pioneer of management consultancy who quipped that ‘Americans prefer the word ‘guru’ because they can't spell the word ‘charlatan.’ However, ‘cosmetic dentistry gurus’ no longer need to be imported. Home-grown ones, some barely out of dental nappies, seem blissfully unencumbered by any self-doubt, social constraints, modesty or prolonged GDC-supervised and accredited training.
Some websites trumpet self-congratulatory hagiographies, dubious testimonials and/or supposedly valid 5-star ratings, which are all readily accessible courtesy of Professor Google. Some, having attended short courses or paid to become a member of some important-sounding ‘academy,’ or institution, magically create the illusion that this is equivalent to, or is recognized as, a GDC CST specialist qualification. It isn't. Some self-nominate and, in effect, pay for some dubious ‘Best Cosmetic Dentist in Middle Earth’ type of award. They sometimes use that superficially impressive membership, or glitzy award and/or pay to use key words on various search engines possibly to lure in ‘consumers’, scrolling on their surgically attached mobile phones for ‘the best dentist for’… whatever the consumer desires.
Many years ago, Australian regulators banned dentists from using any self-promotional advertising in any medium that might encourage patients to seek unnecessary cosmetic or other dentistry, but in the UK, dubious advertising often goes unchallenged.
Do dentists owe a duty of care to prevent narcissistic patients from elective dental damage?
This is a complex, multiply conflicted arena. Some of the issues involve patient autonomy and aspirations, patient and commercial pressures, fashion trends, freedom of expression, different dentist's beliefs, ethical issues, geographical and/or cultural differences, financial considerations, as well as complicated consent and/or legal/regulatory issues.
One danger is that a failure to draw enough attention to the ‘material risks’9 involved in some proposed elective, but irreversible, appearance-altering treatment, and being able to prove that the other viable alternatives, including having no treatment or some much-less damaging treatment, were described fairly, leaves that clinician vulnerable to a later charge of not having had valid ‘Montgomery’ consent prior to undertaking that particular destructive, or unstable, treatment.14
Some veneer cases shown on Instagram, or websites, actually illustrate an artistic ceramic technician's elegant skills rather than the dentist's. However, some potentially narcissistic, or commercially focused dentists edit out any destructive preparation pictures (or don't take them) and prefer to take all the credit for their successful, perhaps best ever, end result (Figure 4). Presumably, they do that to seduce other vulnerable, naïve ‘punters’ to have similar treatments in their cosmetic casino. However, given the importance of managing expectations realistically pre-operatively, especially in someone they have never met, let alone assessed properly, dentists can set up dangerous situations where their own self-promotion can result in serious disappointment in someone who has had their expectations heightened enormously by that dentist's displayed images. Wise dentists know that it is much wiser to under-promise and over-deliver than doing it the other way around.8 Even marginal failure to achieve some narcissistic patient's unchallenged idealized outcome risks complaints and/or litigation, and the potential delights of discussing absolute terms in the English language, such as ‘perfect’, with the patient's Doberman lawyer.
Figure 4. (a,b) Before and after views. Misinformation or disinformation on a website? Could the failure to emphasize enough that up 30% of their largely sound, if mildly worn, tooth structure was probably removed for these quick, but destructive, ceramic veneers possibly invalidate someone's consent.9 Is it likely that the realistic options of doing nothing, or of standard bleaching, possibly with minor additive direct bonding, were discussed fairly beforehand?9,14
Figure 5 at least gives an honest picture to potential narcissists (and dentists) of what damage was involved in this person having a ‘veneer makeover’ to satisfy their aesthetic aspirations. People with serious narcissistic traits might still be willing to have this amount of destructive dentistry carried out, and possibly to get the added bonus of the gingival inflammation shown later, if it meant they could have their ‘perfect smile’ quickly.
Figure 5. (a–c) A case appearing on a dentist's website highlighting the ‘before and after’ views. In this case, the dentist demonstrated their ‘opportunistic pathogen’ skills in destroying sound teeth very precisely, presumably partly to make other dentists envious.
Even copiously typed or written clinical notes, or alleged records of the discussions, might not reflect accurately what the actual messages were conveyed, nor what some potentially narcissistic patient actually understood. Some develop a convenient amnesia about earlier warnings in later disputes. Some dentists appear very happy to provide what some might term ‘porcelain pornography’,14 perhaps for mixed motives, possibly including some pride, envy and/or greed. However, what is very doubtful indeed is if they would have that extensive mutilation done to their own sound teeth, or would do that to their own child, or indeed to anyone about whom they really cared (Figures 1, 2, 4 and 5).
Internet platforms and narcissistic traits
Facebook, which has over one billion users, had interesting connections with dentistry and facial aesthetics in some earlier versions, such as Facemash (2003), which morphed in to The Facebook in 2004, before then becoming Facebook, concentrating on facial appearance and attraction. Mark Zuckerberg's father, Edward, is a practising dentist. Over time, various internet sites and apps were developed for communicating, ‘dating’ and (ahem) other purposes, based on attraction, appearance and personal desires. Many ‘dating sites’ show the lips and teeth very clearly. Understandably, many normal people want to portray the best version of themselves to improve their chances of a mutually agreeable contact. That projected image can be helped by digital manipulation/filters, but sometimes ‘cosmetic tweakments’ can be a euphemism for risky and irreversible dental or facial treatments.
Instagram (‘Insta’) arrived in 2010 and is now worth $19 billion. Insta is home to an army of ‘influencers’ peddling their often commercially driven views about ‘beauty’ and their idealized lifestyle to their cult-like followers.10,11,12 Many ‘influencers’ exhibit a distinct lack of empathy for other people's situations, which rather confirms their egocentric, grandiose and socially unaware narcissistic aspects.2,3,4
Sadly, many young people have been bombarded by idealized images from an early age, making some feel inadequate or unattractive.10,11,12 Many are targeted unmercifully with advertisements for changing their appearance, based on data scraped from vulnerable youngsters' online activity on their mobiles and then sold on to unscrupulous advertisers or more simply, through retargeted advertising.15
Slick advertising for ‘dodgy dentistry’ has exploded in different media, including about direct-to-consumer orthodontics. Many glib advertisements make unsubstantiated claims for biologically dubious treatments, which are not challenged effectively enough by the Advertising Standards Authority (ASA), or other authorities. The apparently risk-free messages being promoted heavily might account, partially, for some vulnerable people presenting to some commercially driven, ineffectively regulated companies, or to dentists, or to orthodontists, requesting very significant, potentially unstable, changes in the positions and appearance of their teeth.16,17
Orthodontics, ‘alignodontics’ and ‘relapsodontics’
‘Relapsodontics’ could be a cynical name for some orthodontics, because many initial orthodontic results relapse over time.16,17
There has been an explosion in the demand for perfect-looking straight teeth. Unfortunately, some aligner companies advertise widely, but appear not to draw enough attention to the well-known biological dangers and fundamental instability produced by some of their allegedly invisible tooth-aligning technology. Advertisements appearing on mainstream television and on new media certainly do not emphasize enough the long-term need for indefinite retention and all their associated biological and other costs (Figures 6 and 7).
Figure 6. (a,b) This patient had two courses of fixed orthodontic appliance therapy, both of which relapsed. She had further orthodontic treatment with direct-to-consumer aligners to get them ‘perfectly straight’ again. At a subsequent consultation she complained that the teeth felt loose. They were. Was her consent valid (‘Montgomery’)?9Figure 7. (a–d) ‘Relapsodontics’ after 2 years of orthodontics, followed by fixed braided wires in both arches and removable retainers, allegedly being worn nightly…until they did not fit. Some pragmatic direct resin bonding of the lower and upper incisors took under an hour to conceal the problems, and change the shape and contact anatomy of the lower right lateral incisor (LR2) so that it could not relapse again. Direct bonding was probably a realistic option to address the alignment problem initially, without any orthodontics at all being involved (‘Montgomery consent’ again.9)Figure 8. A pie-chart showing the breakdown of personality types attending for plastic surgery.5 It is possible that there will be some similarities with those people now attending dentists requesting extensive facial appearance-altering treatments.
Why have the problems increased recently?11,12,13,16
There has generally been an increased emphasis on appearance and beauty in affluent societies, with a myriad of providers of products and interventions competing fiercely on new media platforms. That reality has coincided with the commercialization of healthcare generally, with that becoming progressively more apparent in dentistry in the UK.
Dentistry sits uneasily on a boundary between commercial business and healthcare, with the government-determined co-payments and the independent contractual basis of dental practice involving complex commercial considerations. The net income from government contributions when ‘authorizing’ (i.e. not paying for all of it, as it claims) NHS dental treatments has dropped dramatically in real terms over the past 20 years, while there have been massively increased demands and costs associated with practice, thus squeezing profits.
Most dentists want to look after their patient's interests in different ways by doing solid, sensible, dentistry that satisfies most patients' reasonable aesthetic demands. Many compassionate dentists now prefer different systems to do that, rather than relying on the not-so-great-or-glorious NHS multiply flawed UDA system. However, some dentists, some of whom might have a rather grandiose sense of their own talents, might make the decision to really maximize their income through undertaking expensive elective treatments that are attractive to individuals who are willing to pay a lot to look their very best as they both perceive things (Figures 1, 2, 4 and 5)
Possible warning signs include search engine-optimised (SEO) advertising of high-end treatments, often with little evidence of formal GDC-supervised courses or undertaking specialist training programmes. More subtle signs include curating a high-profile media and social-media presence, as well as the active seeking of testimonials from ‘celebrity clients.’ Some of those apparently delighted clients might not realize fully that they have been ‘doubly mugged’ for their invaluable sound tooth structure, as well as their money, until some complications occur.13,14
The reasons why a potential patient shows up at a particular dentist might be traced to that dentist's ‘Insta’ account, or other social media profile, or to their adept advertising strategy. However, one real danger in targeting that group with adequate discretionary disposable income (aka ‘affected by affluenza’), it is possible that there might be an over-representation within that targeted group of people with mild to severe narcissistic traits, as well as others with some other psychiatric problem.5
Conclusion and concerns
Some dental professionals and many indemnifiers are concerned by the overtly commercial trends in dentistry generally, and some regard the self-adulation, or indulgent self-promotion as being manifestations of narcissism. Many suspect that some questionable behaviours by some dentists, whether they are due to narcissisism, pride, envy, lust or other reasons, might not always be in some patients' long-term best interests.18
Some are also seriously worried that they are not in the best interests of the wider dental profession in the long term either, with the probable end result that dentistry is no longer perceived as being a responsible healthcare profession by the public at large.