Cushley S, Duncan HF, Lappin MJ Pulpotomy for mature carious teeth with symptoms of irreversible pulpitis: a systematic review. J Dent. 2019; 88
Duncan HF, Galler KM, Tomson PL European Society of Endodontology position statement: management of deep caries and the exposed pulp. Int Endod J. 2019; 52:923-934
Dummer PM, Hicks R, Huws D. Clinical signs and symptoms in pulp disease. Int Endod J. 1980; 13:27-35
Mejàre IA, Axelsson S, Davidson T Diagnosis of the condition of the dental pulp: a systematic review. Int Endod J. 2012; 45:597-613
Ricucci D, Loghin S, Siqueira JF Correlation between clinical and histologic pulp diagnoses. J Endod. 2014; 40:1932-1939
Wolters WJ, Duncan HF, Tomson PL Minimally invasive endodontics: a new diagnostic system for assessing pulpitis and subsequent treatment needs. Int Endod J. 2017; 50:825-829
Randow K, Glantz PO. On cantilever loading of vital and non-vital teeth. An experimental clinical study. Acta Odontol Scand. 1986; 44:271-277
Nagaoka S, Miyazaki Y, Liu HJ Bacterial invasion into dentinal tubules of human vital and nonvital teeth. J Endod. 1995; 21:70-73
Smith AJ, Cassidy N, Perry H Reactionary dentinogenesis. Int J Dev Biol. 1995; 39:273-280
Ferrari M, Mason PN, Goracci C Collagen degradation in endodontically treated teeth after clinical function. J Dent Res. 2004; 83:414-419
Schneider BJ, Freitag-Wolf S, Kern M. Tactile sensitivity of vital and endodontically treated teeth. J Dent. 2014; 42:1422-1427
Helfer AR, Melnick S, Schilder H. Determination of the moisture content of vital and pulpless teeth. Oral Surg Oral Med Oral Pathol. 1972; 34:661-670
Sedgley CM, Messer HH. Are endodontically treated teeth more brittle?. J Endod. 1992; 18:332-335
Hashem D, Mannocci F, Patel S Clinical and radiographic assessment of the efficacy of calcium silicate indirect pulp capping: a randomized controlled clinical trial. J Dent Res. 2015; 94:562-568
Schwendicke F, Walsh T, Lamont T Interventions for treating cavitated or dentine carious lesions. Cochrane Database Syst Rev. 2021; 7:(7)
Asgary S, Eghbal MJ, Fazlyab M Five-year results of vital pulp therapy in permanent molars with irreversible pulpitis: a non-inferiority multicenter randomized clinical trial. Clin OralInvestig. 2015; 19:335-341
Qudeimat MA, Alyahya A, Hasan AA. Mineral trioxide aggregate pulpotomy for permanent molars with clinical signs indicative of irreversible pulpitis: a preliminary study. Int Endod J. 2017; 50:126-134
Taha NA, Abdelkhader SZ. Outcome of full pulpotomy using Biodentine in adult patients with symptoms indicative of irreversible pulpitis. Int Endod J. 2018; 51:819-828
Taha NA, Ahmad MB, Ghanim A. Assessment of mineral trioxide aggregate pulpotomy in mature permanent teeth with carious exposures. Int Endod J. 2017; 50:117-125
Tan SY, Yu VSH, Lim KC Long-term pulpal and restorative outcomes of pulpotomy in mature permanent teeth. J Endod. 2020; 46:383-390
Kakehashi S, Stanley HR, Fitzgerald RJ. The effects of surgical exposures of dental pulps in germ-free and conventional laboratory rats. Oral Surg Oral Med Oral Pathol. 1965; 20:340-349
Furuse AY, da Cunha LF, Benetti AR, Mondelli J. Bond strength of resin-resin interfaces contaminated with saliva and submitted to different surface treatments. J Appl Oral Sci. 2007; 15:501-505
Mohammadi Z, Dummer PM. Properties and applications of calcium hydroxide in endodontics and dental traumatology. Int Endod J. 2011; 44:697-730
Kundzina R, Stangvaltaite L, Eriksen HM, Kerosuo E. Capping carious exposures in adults: a randomized controlled trial investigating mineral trioxide aggregate versus calcium hydroxide. Int Endod J. 2017; 50:924-932
Tran XV, Gorin C, Willig C Effect of a calcium-silicate-based restorative cement on pulp repair. J Dent Res. 2012; 91:1166-1171
Niu LN, Jiao K, Wang TD A review of the bioactivity of hydraulic calcium silicate cements. J Dent. 2014; 42:517-533
Dutta A, Saunders WP. Calcium silicate materials in endodontics. Dent Update. 2014; 41:708-722
Możyńska J, Metlerski M, Lipski M, Nowicka A. Tooth discoloration induced by different calcium silicate-based cements: a systematic review of in vitro studies. J Endod. 2017; 43:1593-1601
Marciano MA, Duarte MA, Camilleri J. Dental discoloration caused by bismuth oxide in MTA in the presence of sodium hypochlorite. Clin Oral Investig. 2015; 19:2201-2209
Barrieshi-Nusair KM, Hammad HM. Intracoronal sealing comparison of mineral trioxide aggregate and glass ionomer. Quintessence Int. 2005; 36:539-545
Atmeh AR, Chong EZ, Richard G Dentin-cement interfacial interaction: calcium silicates and polyalkenoates. J Dent Res. 2012; 91:454-459
Kim J, Song YS, Min KS Evaluation of reparative dentin formation of ProRoot MTA, Biodentine and BioAggregate using micro-CT and immunohistochemistry. Restor Dent Endod. 2016; 41:29-36
AAE Position Statement on Vital Pulp Therapy. J Endod. 2021; 47:1340-1344
Ha H-T. The effect of the maturation time of calcium silicate-based cement (Biodentine) on resin bonding: an in vitro study. Appl Adhes Sci. 2019; 7
Kaup M, Dammann CH, Schäfer E, Dammaschke T. Shear bond strength of Biodentine, ProRoot MTA, glass ionomer cement and composite resin on human dentine ex vivo. Head Face Med. 2015; 11
Hashem DF, Foxton R, Manoharan A The physical characteristics of resin composite-calcium silicate interface as part of a layered/laminate adhesive restoration. Dent Mater. 2014; 30:343-349
Tulumbaci F, Almaz ME, Arikan V, Mutluay MS. Shear bond strength of different restorative materials to mineral trioxide aggregate and Biodentine. J Conserv Dent. 2017; 20:292-296
Hursh KA, Kirkpatrick TC, Cardon JW Shear bond comparison between 4 bioceramic materials and dual-cure composite resin. J Endod. 2019; 45:1378-1383
Arandi NZ, Rabi T. TheraCal LC: from biochemical and bioactive properties to clinical applications. Int J Dent. 2018; 2018
Chang SW, Cho BH, Lim RY Effects of blood contamination on microtensile bond strength to dentin of three self-etch adhesives. Oper Dent. 2010; 35:330-336
Silva EJNL, Pinto KP, Ferreira CM Current status on minimal access cavity preparations: a critical analysis and a proposal for a universal nomenclature. Int Endod J. 2020; 53:1618-1635
Clark D, Khademi J. Modern molar endodontic access and directed dentin conservation. Dent Clin North Am. 2010; 54:249-273
Salehrabi R, Rotstein I. Endodontic treatment outcomes in a large patient population in the USA: an epidemiological study. J Endod. 2004; 30:846-850
Tickle M, Milsom K, Qualtrough A The failure rate of NHS funded molar endodontic treatment delivered in general dental practice. Br Dent J. 2008; 204
Bhuva B, Giovarruscio M, Rahim N The restoration of root filled teeth: a review of the clinical literature. Int Endod J. 2021; 54:509-535
Aquilino SA, Caplan DJ. Relationship between crown placement and the survival of endodontically treated teeth. J Prosthet Dent. 2002; 87:256-263
Pratt I, Aminoshariae A, Montagnese TA Eight-year retrospective study of the critical time lapse between root canal completion and crown placement: its influence on the survival of endodontically treated teeth. J Endod. 2016; 42:1598-1603
Sequeira-Byron P, Fedorowicz Z, Carter B Single crowns versus conventional fillings for the restoration of root-filled teeth. Cochrane Database Syst Rev. 2015; 2015:(9)
Mannocci F, Bertelli E, Sherriff M Three-year clinical comparison of survival of endodontically treated teeth restored with either full cast coverage or with direct composite restoration. J Prosthet Dent. 2002; 88:297-301
Mannocci F, Bhuva B, Roig M European Society of Endodontology position statement: The restoration of root filled teeth. Int Endod J. 2021; 54:1974-1581
Gillen BM, Looney SW, Gu LS Impact of the quality of coronal restoration versus the quality of root canal fillings on success of root canal treatment: a systematic review and meta-analysis. J Endod. 2011; 37:895-902
Haque A. How should root filled posterior teeth be restored? A systematic review and survey to general dental practitioners.: University of Liverpool; 2020
Apelian N, Vergnes J-N, Bedos C. Is the dental profession ready for person-centred care?. Br Dent J. 2020; 229:133-137
Abu-Awwad M. Dentists' decisions regarding the need for cuspal coverage for endodontically treated and vital posterior teeth. Clin Exp Dent Res. 2019; 5:326-335
Bandlish RB, McDonald AV, Setchell DJ. Assessment of the amount of remaining coronal dentine in root-treated teeth. J Dent. 2006; 34:699-708
Samet N, Jotkowitz A. Classification and prognosis evaluation of individual teeth – a comprehensive approach. Quintessence Int. 2009; 40:377-387
Dawood A, Patel S. The Dental Practicality Index – assessing the restorability of teeth. Br Dent J. 2017; 222:755-758
Naumann M, Schmitter M, Frankenberger R, Krastl G. ‘Ferrule comes first. Post is second!’ Fake news and alternative facts? a systematic review. J Endod. 2018; 44:(2)212-219
Reeh ES, Messer HH, Douglas WH. Reduction in tooth stiffness as a result of endodontic and restorative procedures. J Endod. 1989; 15:512-516
Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: part 2: tooth survival. Int Endod J. 2011; 44:610-625
Laske M, Opdam NJM, Bronkhorst EM Risk Factors for dental restoration survival: a practice-based study. J Dent Res. 2019; 98:414-422
Murphy F, McDonald A, Petrie A Coronal tooth structure in root-treated teeth prepared for complete and partial coverage restorations. J Oral Rehabil. 2009; 36:451-461
Agustín-Panadero R, Martín-de Llano J-J, Fons-Font A, Carda C. Histological study of human periodontal tissue following biologically oriented preparation technique (BOPT). J Clin Exp Dent. 2020; 12:e597-e602
Edelhoff D, Sorensen JA. Tooth structure removal associated with various preparation designs for anterior teeth. J Prosthet Dent. 2002; 87:503-5009
Bader JD, Rozier RG, McFall WT, Ramsey DL. Effect of crown margins on periodontal conditions in regularly attending patients. J Prosthet Dent. 1991; 65:75-79
Veneziani M. Posterior indirect adhesive restorations: updated indications and the morphology driven preparation technique. Int J Esthet Dent. 2017; 12:204-230
Restorative management of the posterior tooth that has undergone a pulpotomy Nicholas N Longridge James S Hyde Fadi Jarad Sondos Albadri Dental Update 2025 50:11, 932-940.
Pulpotomy is increasingly being recognized as a treatment option for the management of permanent teeth with extremely deep caries. These teeth can present with or without symptoms of pulpitis. Traditionally, irreversible pulpitis has been managed with pulp extirpation and root canal treatment. Contemporary research has shown that pulpotomy may be suitable to manage permanent teeth diagnosed with irreversible pulpitis. This article discusses the options and decision-making process of how to restore posterior permanent teeth that have undergone a pulpotomy. In addition, the article highlights diagnostic and material considerations relating to the role of pulpotomy in managing deep caries.
CPD/Clinical Relevance: Clinicians should be aware of the use of pulpotomy in management of extremely deep caries or partial irreversible pulpitis in permanent teeth.
Article
Pulpotomy is a minimally invasive endodontic procedure that simultaneously manages pulpitis, while maintaining the radicular pulp. It is one of several management strategies for carious lesions and exposed pulps that, collectively, are categorized as vital pulp therapies (VPT)(Table 1). The numerous benefits of maintaining pulpal vitality have been highlighted in the literature (Table 2) and management of carious lesions with partial and full pulpotomy is well documented in children and becoming increasingly more prevalent in adults. Short-term success rates in adults have been reported as high.1 While the literature pertaining to the clinical management and subsequent healing of the exposed pulp is increasing, the restorative management of teeth that have undergone pulpotomy has had minimal attention. Therefore, this article discusses contemporary pulpal diagnoses, and the restorative management of posterior permanent teeth that have undergone a pulpotomy as part of the management of a carious lesion.
Table 1. Vital pulp therapy definitions taken from European Society of Endodontology position statement.2
Direct pulp cap
Class I: No pre-operative presence of a deep carious lesion. Pulp exposure judged clinically to be through sound dentine with an expectation that the underlying pulp tissue is healthy (exposure due to a traumatic injury to the tooth or an iatrogenic exposure)
Class II: Pre-operative presence of a deep or extremely deep carious lesion. Pulp exposure judged clinically to be through a zone of bacterial contamination with an expectation that the underlying pulp tissue is inflamed
Partial pulpotomy
Removal of a small portion of coronal pulp tissue after exposure, followed by application of a biomaterial directly onto the remaining pulp tissue prior to placement of a permanent restoration
Full pulpotomy
Complete removal of the coronal pulp and application of a biomaterial directly onto the pulp tissue at the level of the root canal orifice(s), prior to placement of a permanent restoration
Pulpectomy
Total removal of the pulp from the root canal system followed by root canal treatment, prior to placement of a permanent restoration
Table 2. Reported benefits of maintaining tooth vitality.
The clinical assessment of pulpal inflammation in a tooth with a carious lesion remains challenging. The conventional clinical method for assessing pulp status relies upon patient-reported symptoms, sensibility testing and clinical findings. It has previously been documented that the clinical diagnoses of reversible/irreversible pulpitis may not correspond to the actual histological diagnosis,3,4,5 and a contemporary, biologically focused attempt to redefine pulp status has been published,6 with further research required to support its routine use.
Carious lesions have various clinical presentations and can present asymptomatically, as well as with clinical diagnoses of reversible and irreversible pulpitis. Reversible pulpitis remains an operational term, based on the clinical findings of a heightened response to thermal testing that resolves within 20 seconds following stimulus removal (Table 3).14 These cases frequently respond to carious lesion management such as selective removal of carious tissue, which should be delivered alongside tailored preventative advice.15 Contrary to historical beliefs, for irreversible pulpitis, findings have shown that symptoms associated with this diagnosis may only represent irreversible pulpal inflammation confined to the coronal pulp.5 This finding has been the foundation for a number of clinical studies investigating vital pulp therapies in permanent teeth such as partial/full coronal pulpotomy.16,17,18,19,20 While these studies are reporting high short-term success rates, the necessity to periodically review pulp status in these teeth is recommended because of the possibility of delayed pulpal necrosis or pulp canal obliteration.2
Table 3. Current pulpal diagnostic terminology and possible management strategies. (Adapted from Ricucci et al,5 Wolters et al6 and Hashem et al14).
Diagnoses
Diagnostic criteria
Mild reversible pulpitis
Heightened and lengthened response to thermal/sweet stimuli lasting up to 20 seconds. Settles spontaneously
Severe reversible pulpitis
Increased pain to stimuli for more than several minutes that may require analgesics
Irreversible pulpitis
Persistent dull throbbing
Pain, sharp spontaneous pain and tenderness to percussion or pain exacerbated by lying down
Therefore, in clinical practice not all patients presenting with symptoms of ‘irreversible pulpitis’ will require pulpectomy. In some cases, pulpotomy will be sufficient to remove the non-saveable, irreversibly inflamed coronal portion of the pulp allowing the minimally inflamed radicular pulp tissue to heal.
Essential pulp management
Because of the role of micro-organisms in the inflammation and necrosis of the dental pulp,21 disinfection of the operative site, including the exposed pulpal tissue and the surrounding dentine is imperative. In line with this, non-selective (complete) removal of carious tissue is recommended when pulpotomies are being performed.2 This should involve a systematic approach to caries removal progressing from the amelodentinal junction (ADJ) to the pulpal roof prior to pulpal exposure. Contaminated instruments should be changed prior to pulp exposure. Disinfection and removal of infected dentine chips should be performed with careful irrigation with sodium hypochlorite (NaOCl 0.5–5%) using a sterile side-vented, endodontic needle. Dental dam isolation is mandatory because maintaining sterility provides an optimal environment for pulpal healing and resin-bonding when restoring.22
Pulpotomy materials
Following amputation of the inflamed pulpal tissue, and haemostasis using cotton pellets soaked in NaOCl, a material suitable for direct contact onto the pulp is required. For several decades, calcium hydroxide served as the capping material of choice for pulpal exposures, owing to its high alkalinity and antibacterial properties.23 More recently, hydraulic calcium silicate cements (HCSCs) such as mineral trioxide aggregate (MTA) have demonstrated superior healing24 and a more consistent dentine bridge when used intracoronally for vital pulp therapy.25 The bioactivity of HCSCs is beyond the scope of this article.26
Multiple formulations of HCSCs are now available, some of which are resin-based (e.g. Theracal LC Bisco, USA).27 While initial formulations were associated with crown discolouration,28 newer-generation HCSCs, such as Biodentine (Septodont, France) and premixed varieties such as TotalFill BC RRM Putty (FKG Dentaire, Switzerland) appear to have reduced the risks of discolouration by replacing bismuth oxide,29 and simultaneously improved handling properties and setting times.
The hydraulic nature of HCSCs makes these materials suitable for direct placement onto the amputated pulp during pulpotomy. A superior dentine seal has also been reported with in vitro studies compared with glass ionomer cements (GIC),30 thanks to the formation of a ‘mineral infiltration zone’. Histological animal studies have demonstrated minimal pulpal inflammation and the presence of an intact odontoblastic layer.31,32
Direct restorative considerations
At present, HCSCs are used as dentine replacement materials and as such, lamination with a more conventional and definitive restorative material is currently still required. Both immediate (one-stage) and delayed (two-stage) lamination with a definitive restorative material have been advocated.33 Initial setting times for commonly used HCSCs, such as Biodentine and TotalFill BC RRM fast-set putty, are reported to be 12 and 20 minutes, respectively, which can add considerable length to treatment times if attempting immediate lamination. These initial setting times should be observed prior to lamination where possible. In contrast, delayed lamination requires a second clinical appointment for permanent restoration that may not be deemed appropriate, especially for anxious patients or those with irregular attendance patterns.
While evidence has identified that chemical maturation of HCSCs can improve resin-bond strengths,34,35,36,37 the bond strengths reported between HCSCs and composite resin are, at best, comparable to the bond of GIC to dentine. As such, it has been suggested that the choice of HCSC for pulpotomy should not be influenced by the resultant HCSC–composite bond strength,38 but greater consideration should be placed on the dentine seal provided by the ‘mineral infiltration zone’. Furthermore, the surface area of the remaining cavity wall will be larger than the HCSC-restored cavity floor. Therefore, bond strengths on the cavity floor are potentially a less significant factor when compared with the overall surface area for resin–dentine bonding. The American Association of Endodontists position statement on vital pulp therapy recommends immediate placement of the permanent restorative material.33 While light-curable HCSC formulations are available, further research is required to understand the influence of (di)methacrylate monomers in pulpal irritation and healing.39 While the ability to bond immediately to the HCSC is desirable, the overall aim for pulpotomy procedures should be to avoid further pulpal irritation and promote healing. Figure 1 demonstrates the potential approaches to definitively restoring a posterior tooth following pulpotomy.
Figure 1. Restorative strategies for definitive restoration of a posterior tooth following pulpotomy. HCSC: hydraulic calcium silicate cement; GIC: glass ionomer cement; composite: bonded resin composiste. Created with BioRender.com
In summary, practitioners are faced with a clinical decision whether to perform immediate or delayed lamination that requires consideration of multiple patient and tooth factors. In the absence of long-term prospective trials, the authors favour immediate two-layer lamination with GIC/resin-modified GIC (RMGIC) and composite resin to minimize treatment visits, optimise coronal seal and reduce the risk of additional tooth reduction during temporary restoration removal. Alternatively, clinicians may opt for a single layer of composite resin onto the set HCSC.
Long-term restorative management
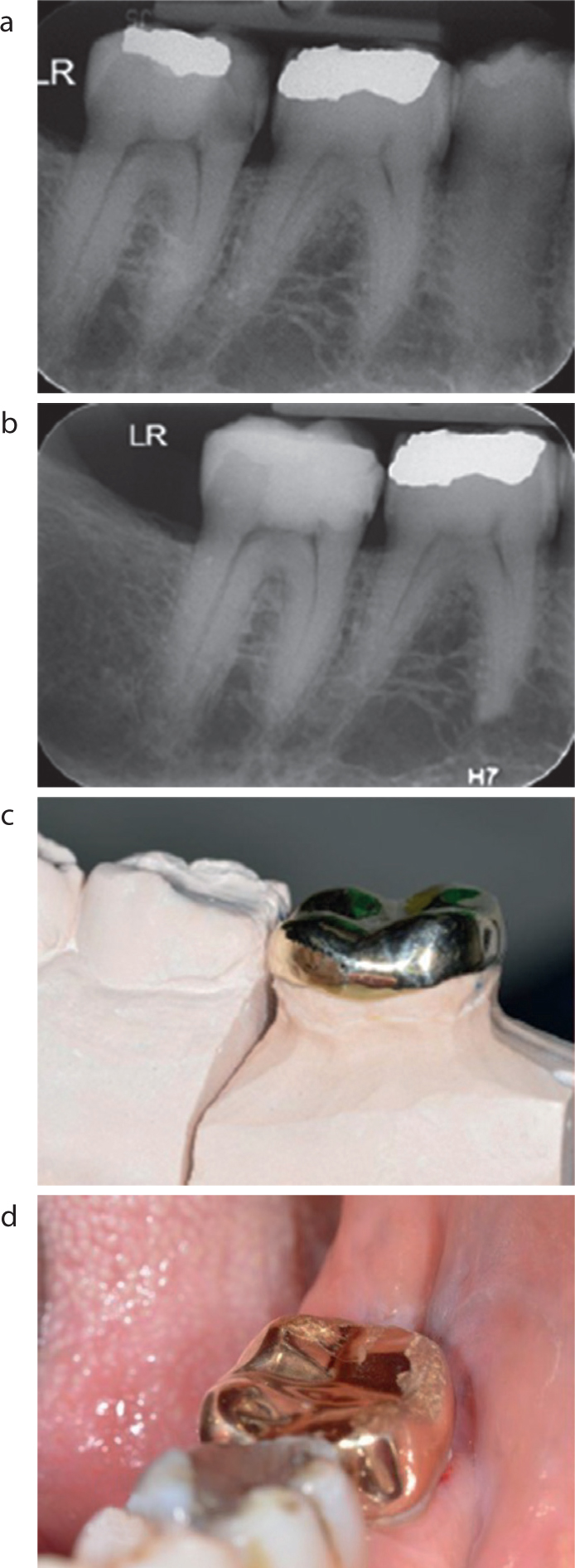
Following the pulp management described above, prevention of any further bacterial ingress and microleakage is central to the protection of the underlying dental pulp. As such, the need for a well-sealed definitive restoration is paramount, and resin-bonding in saliva-free and blood-free environments is mandatory.22,40 In many cases, direct composite resin will serve as the long-term definitive restoration in teeth with minimal occlusal access cavities, absence of cracks and favourable occlusal schemes. Minimally invasive access cavity designs, such as caries and restorative-driven access cavities, are becoming more common and may be appropriate where less invasive VPTs, such as direct pulp capping or partial pulpotomy, are being performed.41 However, good visualization of the exposed pulpal tissue is required, and this will usually require the removal of the roof of the pulp chamber when full pulpotomy is being performed. When teeth present with more extensive coronal tooth tissue loss, for example large proximal cavities or cusp fractures, then cuspal coverage restorations in the form of onlays (partial coverage crowns) or crowns may be required. Figure 2 shows a full coverage gold shell crown on a last-standing lower molar following partial pulpotomy with Biodentine (Septodont). Extensive bucco-lingual extension of the mesial cavity, a distal crack line and signs of parafunction necessitated a full coverage restoration.
Figure 2. Definitive restoration with Biodentine (Septodont, France)of a mandibular last-standing molar following partial pulpotomy. (a) Pre-operative peri-apical radiograph. (b) Post-pulpotomy peri-apical radiograph at 3 month review. (c) Definitive full coverage gold shell crown. (d) Gold shell crown in situ. (Images courtesy of Dr Abdul Rahman Hamza-Aly.)
Indications for cuspal coverage restorations
The literature pertaining to the management of pulpotomy-treated teeth with cuspal coverage restorations is limited. Studies often have small sample sizes and are further complicated by the number of different restoration types.20 By extrapolation, similar comparisons can be made to the restorative management of teeth that have undergone endodontic treatment (ET). However, it seems logical to presume that teeth undergoing pulpotomy may often have greater coronal tooth tissue remaining and will have lost less peri-cervical dentine,42 which occurs during endodontic access and biomechanical preparation of the root canal. This may confer restorative benefits as outlined in Table 2.
When considering the restoration of a root-filled tooth, the decision-making process is complex and multifaceted. While multiple studies support the use of cuspal coverage restorations to improve the survival of endodontically treated teeth, these studies are often descriptive or retrospective with limited data collected regarding the overall condition of the tooth prior to restoration.43,44,45,46,47 Similarly, studying the quality of coronal restoration is complicated by the lack of agreement regarding the best restorative strategies with no standardized assessment for restoration quality. The paucity of high-quality evidence has been highlighted in both narrative45 and systematic reviews,48 the latter comparing single crowns with conventional fillings for post-endodontic restorative treatment. This systematic review contained only one study, which included post-crown restorations in premolars, and this cannot be extrapolated to pulpotomy-treated teeth.49 Further well-designed prospective studies are required to inform these decisions. At present, the European Society of Endodontology (ESE) recommends that each case should be assessed individually based on a number of factors including: tooth structure loss; occlusal factors; presence of cracks; and position within the arch, that is terminal and non-terminal teeth.50 The circumferential presence of ferrule remains an important factor when considering the restorability of a tooth prior to any endodontic management.
While the type of restoration required remains equivocal, evidence from a meta-analysis demonstrates that a good coronal restoration is important for peri-apical health,51 which is equally important for VPTs. Recent research has shown that the healthcare setting and, in particular, the remuneration strategy (state funded versus privately funded) has more influence than patient choice,52 which is limited when considering indirect restorations.53 Furthermore, there appears to be greater uncertainty regarding the need for cuspal coverage restorations on vital teeth when compared with endodontically treated teeth.54 Considering all of the above factors, the authors are of the opinion that indications for cuspal coverage restorations on pulpotomy-treated teeth include:
Loss of marginal ridge(s);
Last-standing teeth;
Thin or undermined cusps (<1.5 mm thickness);
Previous cusp fractures, cracked teeth or craze lines;
Unfavourable occlusal relationships;
Parafunction.
Restorability indices
To facilitate the assessment of restorability, a number of indices have been proposed.55,56,57 Despite the potential positives of these indices and attempts at validation, fundamentally, there remains an element of subjectivity that makes comparison challenging. Most indices serve as a clinical assessment of remaining coronal tooth structure and draw on the literature from in vitro and retrospective studies, which have highlighted the importance of a number of factors including: ferrule;58 loss of marginal ridges;59 presence of both proximal contacts;60 peri-cervical dentine;42 and parafunction.61 These factors have been explored in great detail in relation to endodontically treated teeth elsewhere.45 More recently, attempts to quantitatively assess remaining tooth structure using digital techniques have been reported. The most recent of these indices, the ‘Dental Practicality Index’ provides clinicians with a structured approach to assessing ‘whether to restore’, but evidence-based support for the decision regarding ‘how to restore’ is lacking.
Minimum intervention restorative treatment
In line with a general shift towards minimum intervention dentistry and as outlined above, when cuspal coverage is planned, the authors favour partial-coverage over full-coverage crowns for pulpotomy-treated teeth. The perceived benefits of partial cuspal coverage restorations are presented in Table 4. While full cuspal coverage restorations present a reliable treatment for the heavily restored tooth, the reduction of up to 65% of coronal tooth tissue with a conventional metal–ceramic crown preparation is unnecessarily destructive where circumferential enamel is present for adhesively retained partial coverage crowns/onlays. A small sample, clinical study by Murphy et al showed that teeth prepared for full coverage crowns could have up to 45% greater reduction in coronal tooth volume when compared to partial coverage crowns.62 It is generally accepted that coronally positioned margins allow for easier dental dam isolation, tooth preparation and restoration cementation, while also reducing the potential for further thermal and chemical insult to the remaining dental pulp where minimal vital pulp therapies have been performed. In these cases, equigingival or subgingival horizontal crown margins may expose dentinal tubules that still communicate with the remaining dental pulp, as well as complicate the ability for future sensitivity testing (Figure 3). The use of vertical crown margins as part of the biologically oriented preparation technique (BOPT) has been reported, and may provide a suitable alternative to conventional horizontal margins for teeth where intra-sulcular preparations are required.63
Table 4. Perceived benefits of partial coverage crowns/onlays when providing cuspal coverage restorations of posterior teeth following pulpotomy.
Preservation of coronal tooth tissue
Full coverage coronal restorations (all ceramic and metal-ceramic) can remove up to 72% of coronal tooth tissue64
Greater restorative treatment options should failure occur
Easier clinical review of supra-gingival restorative margins and pulp sensibility
Visible supra-gingival (tooth) tissue enables easier assessment of marginal adaptation and sensitivity testing with cold (refrigerant spray) and electric pulp testers compared to full coverage crowns
Greater cleansibility of margins, i.e. reduced periodontal inflammation and pocketing with supracrestal margins65
More coronal restorative margins
Enables placement of preparation margin within greater depth of enamel,66 thus reducing risk of preparation into dentine to enable improved bond strengths for adhesively retained restorations
More superficial dentine has a smaller volume of dentinal tubules per square mm
Easier isolation for restoration and cementation
Easier clean up and polishing of margins
Greater stiffness of tooth and less flexure when margin is within enamel compared with dentine
Restorative margins do not involve dentinal tubules that communicate with the dental pulp below the level of the vital pulp therapy, thus reducing chemical, mechanical and thermal insult to the pulp and the odontoblast processes
Figure 3. Potential for further pulpal irritation with full coverage horizontal crown margins on dentine. Created on Biorender.com
Improvements in the strength of adhesive resin cements and bonding systems mean that in many of these cases with circumferential enamel, further tooth reduction to provide conventional mechanical retention and resistance is not necessary. For adhesively retained restorations, a meticulous bonding protocol must be followed, and the authors consider dental dam isolation to be the gold standard. There are currently no prospective clinical studies investigating the use of pulpotomy-treated teeth as bridge abutments, and as such, the use of these teeth in more complex prosthodontic treatment plans should be considered carefully because of the potential need for future endodontic treatment.
Preparation design and material choice
Prior to undertaking any restorative treatment, a thorough assessment of the patient should take place. This should include patient factors such as parafunctional habits, mouth factors such as occlusal relationship and tooth factors such as tilting, rotation or loss of adjacent contacts. It is vitally important when planning tooth preparation for cuspal coverage restorations that all these factors are considered because there is no one ideal preparation that will be suitable for all cases. For example, teeth with interocclusal space between opposing cusps may require less occlusal reduction than those with heavy static and dynamic contacts. A contemporary approach to the planning of indirect partial coverage crowns has recently been advocated that highlights the importance of pre-operative occlusal space.67 This technique involves the chair-side addition of composite to assess appropriate tooth preparation, while maintaining adequate restoration thickness. This technique is comparable to the Galip Gurel technique proposed for porcelain laminate veneers,68 whereby veneer preparation is performed through an intra-oral mock-up in bis-acryl resin to optimise restorative space and minimize tooth substance removal. Alternatively, the use of cast study models or intra-oral scanners can enable the precise assessment of restorative space and tooth preparation required to optimise material thickness.
The range of materials currently available for indirect restorations continues to evolve and preparation requirements are varied. While conventional casting and pressing laboratory techniques are used extensively, additive and subtractive manufacturing have presented a new range of materials and production techniques. Table 5 presents the possible materials available for cuspal coverage restorations. Precious alloys such as gold remain a popular choice for posterior teeth where aesthetics are of less importance and in patients with parafunctional habits because of favourable wear characteristics.69 Resin composite, placed directly or indirectly offers an aesthetic alternative.70
Table 5. Material considerations for partial coverage crowns/onlays on pulpotomy-treated teeth.
Direct composite
Technically difficult
Avoids need for temporization between appointments
No laboratory stages or costs
Easily accessible and cheap
Tooth coloured, ability to ‘blend’ with natural tooth margin
Moderate fracture resistance
Can use injection moulding techniques
Amalgam
Technically very difficult
No laboratory stages or costs
Easily accessible and cheap
Avoids need for temporization between appointments
Non-tooth coloured
No inherent ability to bond to tooth structure
May be subject to leakage
Indirect composite
Familiar material to clinicians for bonding protocols
Easy to repair/polish/adjust
Tooth coloured
Softer than opposing enamel, thus reduces wear of antagonist teeth
Metallic alloys (precious/non-precious)
Non-tooth coloured
As little as 1-mm occlusal thickness needed
Long-term evidence of clinical survival
Excellent fracture resistance
Glass-matrix ceramics (e.g. lithium disilicate)
Tooth coloured, good aesthetics
Minimum 1-mm occlusal ceramic thickness when adhesively bonded
More difficult to repair
Similar bonding protocol to composite
More abrasive to antagonist teeth
Polycrystalline ceramics (e.g. zirconia)
Tooth coloured
Highest strength and fracture toughness of ceramic materials
Minimum 0.5-mm occlusal thickness for posterior teeth (1.0 mm recommended)
Most difficult to repair/adjust/replace
More abrasive to antagonist teeth unless highly polished
Resin-matrix ceramics
Tooth coloured
Improved strength over indirect composite
Less brittle
1.0-mm occlusal reduction
Ability to adhesively bond
Easy to adjust/repair
Glass-matrix ceramics such as lithium disilicate have high translucency, which offers excellent aesthetics with adequate compressive strength for the majority of patients. This material is a popular choice for posterior teeth in the aesthetic zone where buccal marginal preparation may extend gingivally for aesthetic purposes. Polycrystalline ceramics, such as zirconia, offer higher compressive strengths and fracture toughness, but reduced translucency. The more predominant form of 3 mol% yttria-stabilized tetragonal zirconia polycrystal (3Y-TZP), is suitable for monolithic restorations on posterior teeth. Newer-generation zirconia ceramics with increased yttria content (4Y and 5Y-TZP) have further improved the optical properties of zirconia, making it an alternative to glass-matrix ceramics for posterior teeth in the aesthetic zone. Alternatively, resin-matrix (hybrid) ceramics such as Vita Enamic (Vita-Zahnfabrik, Germany) contain approximately 25% acrylate polymer (by volume), making them less brittle than conventional ceramics, with the ability to accept repair with composite. Lava Ultimate (3M ESPE, Germany) is an alternative resin nanoceramic with zirconia–silica nanoparticles in a resin matrix. Figure 4 demonstrates a full sequence pulpotomy treatment on a maxillary molar with Biodentine (Septodont, France), followed by deep margin elevation with composite resin and a Vita Enamic partial coverage onlay.
Figure 4. Full-sequence pulpotomy and definitive restoration with a partial coverage onlay. (a) Pre-operative radiograph with extensive disto-occlusal carious lesion. (b) Intra-oral pre-operative presentation. (c) Non-selective carious tissue removal and pulp exposure. (d) Biodentine placement. (e) Biodentine preparation and sectional matrix band placement (Palodent V3, Dentsply, UK). (f) Deep margin elevation with direct composite resin. (g) Meticulous dental dam isolation for onlay cementation. (h) Definitive restoration with Vita Enamic Onlay bonded with composite resin. (i) 3 month radiographic review. (Courtesy of Dr Shakil Umerji.)
Clinical considerations
Preparation
Design and dimensions of tooth preparation and occlusal reduction will vary based on various prosthodontic factors including static and dynamic occlusal contacts and material selection. A range of potential materials is available for clinicians (Table 5). The authors favour the use of resin-matrix ceramics, where possible, to allow for ease of access and restoration repair should further endodontic treatment be required. Preparation principles outlined in the morphology-driven preparation technique are recommended where possible.66 The use of ‘deep margin elevation’ techniques may be employed where existing proximal restorations are extensive.66 These techniques involve the meticulous isolation and restoration of equigingival and marginally subgingival cavities using dental dam, sectional matrix bands and composite resin. Elevation of the margin to a supragingival location can facilitate indirect restoration preparation and bonding.
Restoration-tooth margin
Many patients are likely to be more familiar with the conventional full-coverage crown restoration, and the designs of partial-coverage crowns or onlays require detailed discussion. It is important as part of a valid consent process that the patient is aware of the benefits of partial-coverage compared with full-coverage restorations (Table 4). For posterior teeth in the aesthetic zone, it should be made clear that the restoration-tooth margin buccally will be ‘high up on the tooth’ and so is likely to be visible. This may be a more significant factor in maxillary premolar teeth, or for patients with a high smile line or aesthetic concerns. Some patients may feel that it would be unacceptable to see ‘the join,’ and an alternative design of restoration should be considered.
Temporization
For indirect restorations, more minimal tooth preparations will make it less predictable to temporize with conventional techniques. Temporary crowns made chairside are unlikely to be retained in the absence of conventional retention and resistance form of the preparation. Successful temporization can be achieved with the use of bisacryl resin used with ‘spot-etching’, light-cured resin-based materials, such as Telio CS Onlay (Ivoclar Vivadent, Leicestershire, UK), or Poly-F Plus (Dentsply Sirona, Germany) for temporization. The latter of which is weakly adhesive to dentine and requires careful removal with an ultrasonic scaler to avoid damaging the underlying preparation.
Bonding
More coronally placed finish margins create a preparation with reduced retention and resistance forms. As mechanical retention is reduced, the necessity of adhesive bonding becomes more important. The use of dental dam is considered the gold standard for bonding, and coronally positioned margins should allow for easily isolation at this stage. The bonding protocol will vary between restorative materials, with some requiring additional laboratory or clinical stages, for example zirconia.
Conclusions
Pulpotomy is becoming a more widely accepted and evidence-supported treatment option for teeth with extensive caries and early pulpal inflammation. General dental practitioners will be challenged with restoring these teeth on a more frequent basis. Initial pulp management with hydraulic calcium silicates cements is recommended and immediate lamination with a well-sealed composite resin restoration may serve as the definitive restoration of choice. Where more extensive coronal breakdown is observed or where patient factors dictate the need for cuspal protection, partial coverage crowns or onlays can offer a long-term minimum intervention approach. While material choice may vary by patient and clinician preferences, these restorations rely heavily upon adhesive technology and a meticulous bonding protocol under dental dam is highly recommended.