Welbury R, Kinirons MJ, Day P, Humphreys K, Gregg TA. Outcomes for root-fractured permanent incisors: a retrospective study. Pediatr Dent. 2002; 24:(2)98-102
Gorduysus M, Avcu N, Gorduysus O. Spontaneously healed root fractures: two case reports. Dent Traumatol. 2008; 24:(1)115-116
Feiglin B. Clinical management of transverse root fractures. Dent Clin North Am. 1995; 39:(1)53-78
Feely L, Mackie IC, Macfarlane T. An investigation of root-fractured permanent incisor teeth in children. Dent Traumatol. 2003; 19:(1)52-54
Calişkan MK, Pehlivan Y. Prognosis of root-fractured permanent incisors. Endod Dent Traumatol. 1996; 12:(3)129-136
Kositbowornchai S, Sikram S, Nuansakul R, Thinkhamrop B. Root fracture detection on digital images: effect of the zoom function. Dent Traumatol. 2003; 19:(3)154-159
Andreasen JO, Hjørting-Hansen E. Intra-alveolar root fractures: radiographic and histologic study of 50 cases. J Oral Surg. 1967; 25:(5)414-426
Camp JH. Management of sports-related root fractures. Dent Clin North Am. 2000; 44:(1)95-109
Andreasen JO, Andreasen FM, Mejàre I, Cvek M. Healing of 400 intra-alveolar root fractures. 1. Effect of pre-injury and injury factors such as sex, age, stage of root development, fracture type, location of fracture and severity of dislocation. Dent Traumatol. 2004; 20:(4)192-202
Cvek M, Andreasen JO, Borum MK. Healing of 208 intra-alveolar root fractures in patients aged 7–17 years. Dent Traumatol. 2001; 17:(2)53-62
Andreasen FM, Andreasen JO. Resorption and mineralization processes following root fracture of permanent incisors. Endod Dent Traumatol. 1988; 4:(5)202-214
Andreasen JO, Andreasen FM, Mejàre I, Cvek M. Healing of 400 intra-alveolar root fractures. 2. Effect of treatment factors such as treatment delay, repositioning, splinting type and period and antibiotics. Dent Traumatol. 2004; 20:(4)203-211
Diangelis AJ, Andreasen JO, Ebeleseder KA International Association of Dental Traumatology guidelines for the management of traumatic dental injuries: 1. Fractures and luxations of permanent teeth. Dent Traumatol. 2012; 28:(1)2-12
von Arx T, Filippi A, Lussi A. Comparison of a new dental trauma splint device (TTS) with three commonly used splinting techniques. Dent Traumatol. 2001; 17:(6)266-274
Addy LD, Durning P, Thomas MB, McLaughlin WS. Orthodontic extrusion: an interdisciplinary approach to patient management. Dent Update. 2009; 36:(4)212-218
Heithersay GS. Combined endodontic-orthodontic treatment of transverse root fractures in the region of the alveolar crest. Oral Surg Oral Med Oral Pathol. 1973; 36:(3)404-415
Mantzikos T, Shamus I. Forced eruption and implant site development: soft tissue response. Am J Orthod Dentofacial Orthop. 1997; 112:(6)596-606
Bragger U, Lauchenauer D, Lang NP. Surgical lengthening of the clinical crown. J Clin Periodontol. 1992; 19:(1)58-63
Cuoghi OA, Bosco AF, de Mendonca MR, Tondelli PM, Miranda-Zamalloa YM. Multidisciplinary treatment of a fractured root: a case report. Aust Orthod J. 2010; 26:(1)90-94
Andreasen FM. Pulpal healing after luxation injuries and root fracture in the permanent dentition. Endod Dent Traumatol. 1989; 5:(3)111-131
Cvek M, Mejàre I, Andreasen JO. Conservative endodontic treatment of teeth fractured in the middle or apical part of the root. Dent Traumatol. 2004; 20:(5)261-269
Bramante CM, Menezes R, Moraes IG, Bernardinelli N, Garcia RB, Letra A. Use of MTA and intracanal post reinforcement in a horizontally fractured tooth: a case report. Dent Traumatol. 2006; 22:(5)275-278
Andersson L, Emami-Kristiansen Z, Hogstrom J. Single-tooth implant treatment in the anterior region of the maxilla for treatment of tooth loss after trauma: a retrospective clinical and interview study. Dent Traumatol. 2003; 19:(3)126-131
Versiani MA, de Sousa CJ, Cruz-Filho AM, Perez DE, Sousa-Neto MD. Clinical management and subsequent healing of teeth with horizontal root fractures. Dent Traumatol. 2008; 24:(1)136-139
Root fractures are uncommon following dental trauma but are mostly diagnosed shortly after the injury, although occasionally at routine dental appointments. This paper presents the management of the different types of root fractures and the types of healing response suggesting the appropriate follow-up of these injuries.
Clinical Relevance: A thorough clinical examination supplemented with radiographs, vitality tests, appropriate treatment planning and subsequent follow-up of root fractured teeth can improve the prognosis for these teeth and also minimize the need for subsequent extractions. Immature teeth with root fractures have a better chance of healing compared to teeth with fully formed roots.
Article
Root fractures of the teeth are rare compared to other forms of dental trauma. In the primary dentition, root fractures usually occur between 3–4 years of age when root resorption has started. The incidence is reported to be 0.5–7% of all injuries in the permanent dentition.1 Root fractures are defined as those that involve cementum, dentine and pulp. Horizontal root fractures occur more often in the maxillary central incisors and are commonly found in the middle third of the root2 followed by the apical and coronal thirds. Root fractures can be classified according to the direction, extent, number or the portion of the root affected as shown in Table 1.
Direction
Horizontal, Vertical or Oblique
Number
Single or Multiple
Location
Cervical (coronal), Middle or Apical
Extent
Partial or Complete
Root fractures involve damage to the pulp, dentine, cementum, bone and periodontium and usually occur as a result of a horizontal severe impact. These injuries are sometimes associated with other injuries, eg concomitant fracture of the alveolar process in the lower incisor region. The position of the fracture line and its communication with the gingival crevice are important factors in determining the long-term prognosis for the tooth. Long-term prognosis of fractures at the coronal or gingival third is poorer than for a root fracture in the middle or apical third.2,3,4 The chance of healing with calcified tissue is poor when the fracture is very close to or communicating with the gingival crevice.1 Root fractured teeth with immature roots have a better chance of healing compared to teeth with fully formed roots and the majority of the root fractured permanent teeth in children show good healing.5 An explanation could be that teeth with open apices have a greater potential for maintenance of pulp vitality than those with closed apices. Figures 1 and 2 show a maxillary central incisor with horizontal root fracture in the coronal third and middle third, respectively.
Figure 1. Coronal third root fracture of the maxillary central incisor.Figure 2. Middle third root fracture of a maxillary central incisor.
Clinical examination and diagnosis
Fractured roots are mostly diagnosed shortly after injury although, if the patient does not attend the dentist at the time, they may sometimes be found at subsequent routine dental appointments. Clinically, on presentation, teeth with root fractures may be slightly extruded and are frequently displaced. The traumatic force tends to displace the coronal fragment in a lingual or palatal direction, but generally the apical fragment retains its position. It is difficult to distinguish clinically between displacement due to root fracture and luxation injury. Usually, the tooth will be tender to percussion. Sometimes, a transient red or grey discoloration of the crown is seen. If the pulp loses its vitality and becomes infected, a sinus tract may be seen on the buccal mucosa adjacent to the fracture site.
Most pulp tests assess the innervation to the pulp and not the vascular supply. Sensibility testing at the time of trauma is important as a reference point for evaluation of the pulpal status at follow-up appointments. However, these tests carried out immediately after the trauma are sometimes unpredictable as sensitivity responses can be temporarily or permanently decreased after an injury and normal reaction can return after a few weeks or months. Also, mobile teeth may elicit pain from pressure of the electric pulp tester prior to immobilization. Hence it is important to monitor the status of the pulp at regular intervals with follow-up controls. At least two signs and symptoms are required to make a diagnosis of necrotic pulp.
Radiographic examination
More than one radiograph may be required to detect root fractures as they can occur in a diagonal plane and sometimes are not radiographically diagnosed owing to the initiation of healing. Fractures that occur in the cervical third of the root can usually be detected in the regular 90° intra-oral periapical film, as they are generally horizontal. However, with oblique fractures that are common in the middle and apical thirds, two additional intra-oral periapical radiographs can be taken at +/- 15° to the original, or an occlusal film is more likely to confirm the fracture line. According to a study, 31% of root fractures were coincidentally identified during subsequent radiographic examination.6
Digital imaging as an alternative to conventional radiography for the detection of root fractures has not been found to be of added benefit and zooming function in digital imaging also does not affect the detection of root fractures.7 However, use of advanced digital imaging, eg Cone Beam CT, may be of added benefit.
Healing of root fractures
Andreasen and Hjørting-Hansen, in 1967, classified fracture healing into four groups of repair sequelae. 8 It has been reported that the majority of root fractures undergo healing.6,9 In a retrospective study of 400 intra-alveolar root fractures, healing was noted in 78% of the cases, with 22% developing necrosis.10 The ideal healing is by reunion of the fragments with hard tissue.
Hard tissue healing
In the case of a pulp that retains its vitality and absence of infection, a dentine callus forms between the fragments followed by cementum deposition. This fracture heals with growth of cells from the apical half of the pulp. Sometimes a slight widening of the root canal close to the fracture line is seen (Figure 3) indicating internal surface resorption, followed by the hard tissue healing in the resorption cavity as well as the fracture site. A clinical study has revealed that 30% of root fractures show healing by hard tissue union.10
Figure 3. Evidence of widening of the root canal close to the fracture site at 6 weeks.
Clinically, teeth in this group tend to respond normally to percussion. However, they may elicit a normal/decreased response to pulp tests and, radiographically, the fracture line may be visible. Partial pulp canal obliteration of the apical fragment is a common finding.
Connective tissue healing
If the pulp is partially severed or moderately stretched at the level of the fracture, in the absence of bacteria, healing is either by growth of cells from the pulp, or dominated by cells from the periodontal ligament, leading to union of the fragments with connective tissue. Peripheral rounding of the fracture edges, ie external surface resorption, may be noted.
Clinically, teeth tend to feel firm or slightly mobile and are slightly tender to percussion. The sensibility test results may be within the normal range and depend on the severity of the pulpal injury. Radiographically, a narrow radiolucent area separates the rounded fractured ends. A picture of external and internal surface resorption, pulp canal obliteration of usually both apical and coronal aspects of the root canal may be often seen in the early stages.
Bone and connective tissue healing
This type of healing is seen in teeth that are traumatized prior to completion of growth of the alveolar process whereby the apical fragment remains in the jaw and eruption of the coronal fragment continues.
Clinically, following healing, teeth feel firm and usually react normally to the pulp tests.1 Radiographically, bone separates the fragments, but a normal periodontal space exists around both the fragments.
Healing with granulation tissue
If pulpal infection follows a root fracture, this normally occurs in the coronal pulp and the apical fragment contains vital pulp tissue. Pulp necrosis leads to granulation tissue accumulating between the fragments and hence there is non-union.
Clinically, the teeth tend to show signs of infection, for example, fistulae on the buccal mucosa at the level of the fracture line with a loose coronal fragment. They are often slightly extruded and tender to percussion. The teeth respond negatively to sensibility testing. Radiographically, a widening of the fracture line can be seen.
Factors affecting healing
There are many factors that influence the type of healing. A young patient, immature root formation, lack of mobility or dislocation of the coronal fragment and positive sensibility test at the time of injury, are all good prognostic indicators and tend to lead to good pulpal healing and hard tissue repair of the fracture.10 Hard root tissue union is more likely to occur in a vital pulp and in the absence of horizontal or extrusive displacement.3 Repositioning of teeth also increases the chances of healing with hard tissue repair.11 Concomitant enamel-dentine crown fracture has been reported to be significantly associated with loss of pulp vitality.3 The type of injury (ie concomitant presence/absence of luxation) and the diastasis between fragments are significantly related to healing.10
Root resorption processes within the root canal may occur in the first year after injury as a stage of fracture healing and have been reported to occur in up to 60% in one study of permanent incisors.12 The resorption types commonly observed are:
External inflammatory resorption;
External surface resorption;
External replacement resorption (ankylosis);
Internal surface resorption;
Internal tunnelling resorption.
These resorption processes are often found during fracture healing. External inflammatory resorption needs endodontic treatment (Figures 4a, b). Resorption of bone at the level of root fracture is indicative of pulp necrosis. Ankylosis cannot be treated, except by extraction or maintaining the tooth until it is lost. The other types of resorption processes following root fracture are usually related to healing processes, and require no interceptive treatment.12
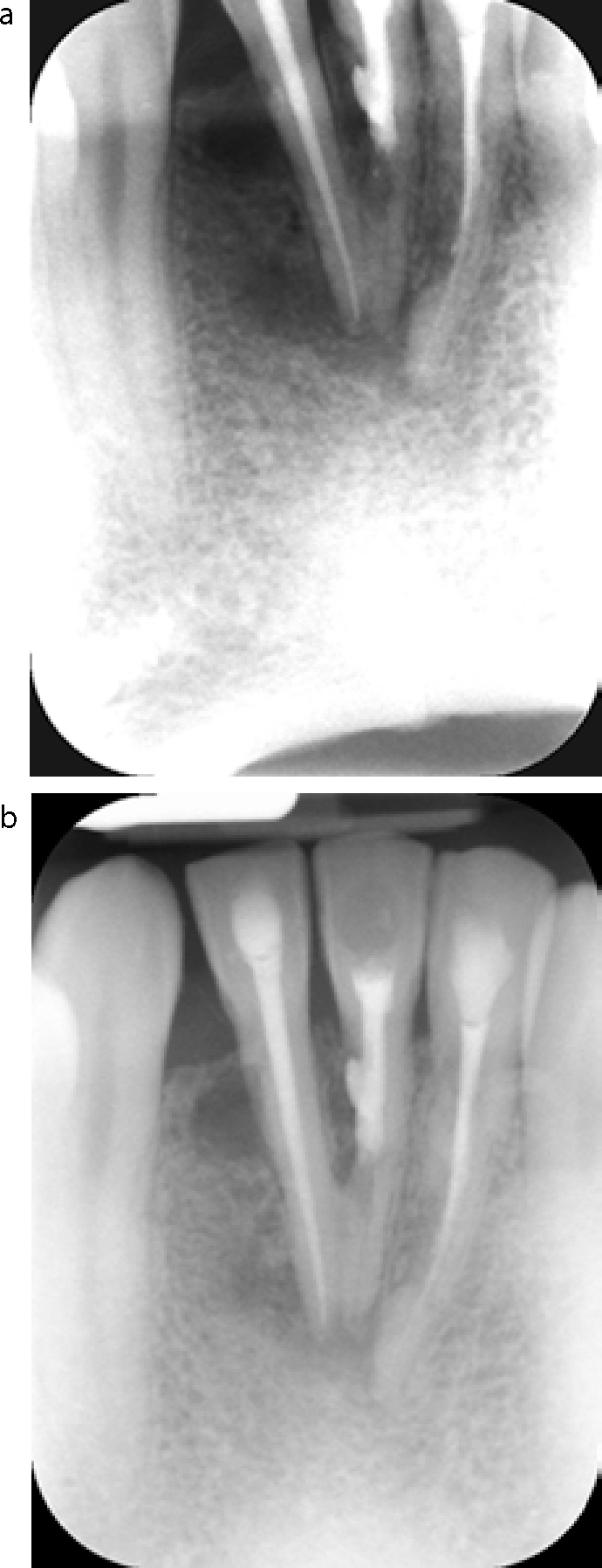
Figure 4.
(a) A case of external root resorption of the lower central incisors following trauma, which was treated by endodontic treatment. (b) Six months later, partial healing is evident and the resorption has responded to the endodontic treatment.
Treatment of root fractures
Reduction of the displaced coronal fragments and immobilization with splinting are the basis of treatment of root fractures in permanent teeth whereas incomplete fractures in teeth with immature roots may heal spontaneously.
Root fractured primary teeth, with no dislocation, should be left to exfoliate normally. Splinting is not advised. Any mobile coronal fragment of the primary teeth should be removed but the apical fragment can be left for physiologic resorption in order to avoid trauma to the developing permanent tooth.
Immature teeth with incomplete root fractures may usually heal by hard tissue union, but may be included in a splint, depending on the clinical situation, eg involvement of multiple teeth.
Following a root fracture in permanent teeth, if there is no mobility and displacement of the coronal fragment and the patient is asymptomatic, no treatment may be required. Long-term follow-up is important as pathological changes can occur several years following the trauma. Teeth with root fractures can spontaneously heal if the vitality of the pulp is preserved and displacement of the fragments is prevented.3
In permanent teeth, if displacement or mobility of the coronal root fragment has occurred, the coronal fragment should be repositioned by digital manipulation as soon as possible under local anaesthesia and its position confirmed radiographically. Resistance to repositioning is usually indicative of fracture of the socket wall and hence repositioning of the fractured bone prior to reduction of the root fracture is important. This can be carried out under local anaesthesia with firm pressure over the bone plate, followed by appropriately directed pressure at the incisal edge of the coronal fragment for repositioning the fragment into its original position.
Immobilization
Immobilization may be achieved with a flexible splint like a wire-composite splint13 and should include at least one neighbouring tooth on either side. Rigid splints, like acrylic or gold cap splints, can lead to increased chances of pulp necrosis. The passive splint should not interfere with occlusion, oral hygiene, speech and should maintain physiologic tooth mobility. Splinting avoids repeated displacement during periodontal healing. In the maxillary arch generally, the splint is placed on the labial tooth surfaces and in the mandible on the lingual surfaces to avoid occlusal interferences. Healing in permanent teeth is usually good when there is no communication between the fracture line and the gingival crevice.
Flexible wire-composite splint
The splint should be as free of the gingival surfaces as possible. Isolation is achieved using cottonwool rolls and 37% phosphoric acid gel is applied for 30 s to the mid-portion of the labial crown surfaces of the injured and the neighbouring teeth, avoiding etching interproximally. An orthodontic wire of 0.5–0.75 mm diameter is adapted to fit against the labial surfaces of the teeth to be included in the splint. The wire is then embedded into composite placed on the labial surface of the non-injured teeth first and then the injured tooth is finally included in the splint. The position of the tooth is maintained with finger pressure (Figures 5a, b). It is important to avoid composite in the interdental areas as otherwise the splint may be converted into a rigid one.
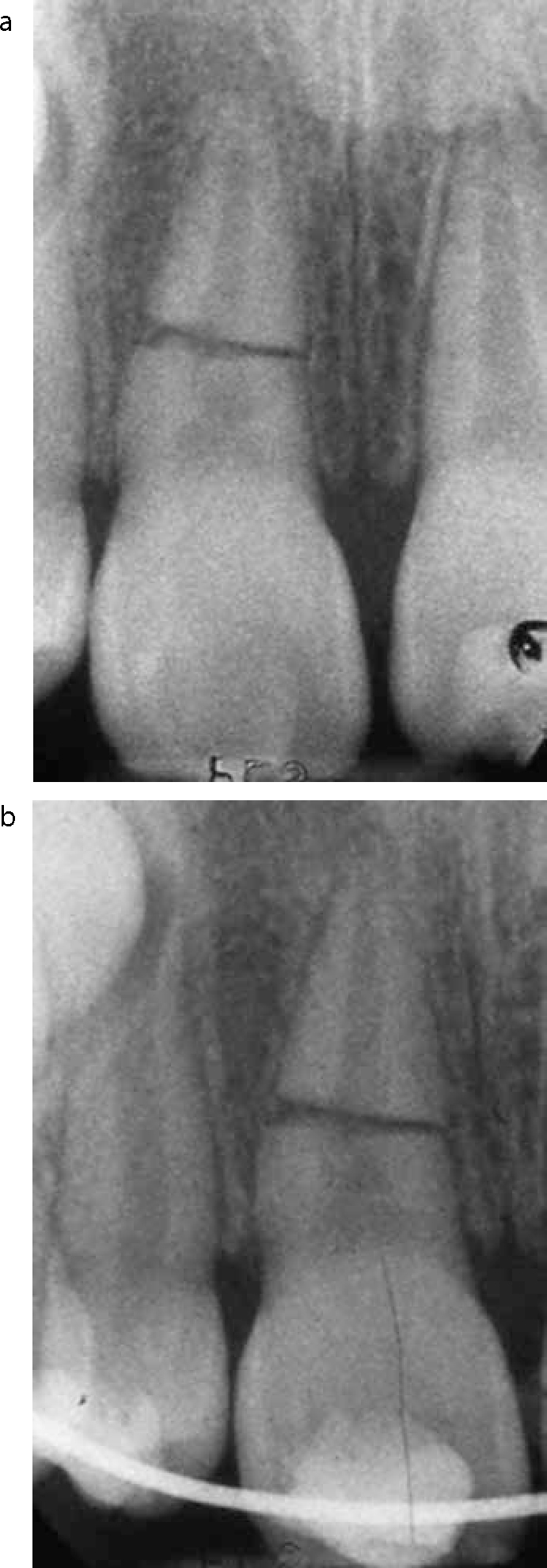
Figure 5.
(a) A root fracture of the maxillary right central incisor. (b) Immobilization of root fracture UR1 with a wire-composite splint.
Patients should be advised to brush with a soft brush and rinse with chlorhexidine mouthwash to prevent accumulation of plaque during the splinting period (Figure 6). As periodontal ligament healing begins in 10 days and gets completed in about a month, the splinting period should be as short as possible, and about 4 weeks' splinting time is recommended. If the fracture is near the cervical area of the tooth, then stabilization for up to 4 months is recommended.14 Sometimes, a conservative approach, including a relatively long splinting period, is recommended when the fracture line is located at the cervical third of the root, below the crestal bone, and the patient's oral hygiene is good. Fixation of the mobile coronal fragment to the adjacent healthy teeth with composite resin proximally at the contact areas can be carried out.1 The duration of splinting can be determined individually according to the severity of the injury, clinical outcome and the radiographic findings at follow-up appointments.
Figure 6. Good oral hygiene maintenance during the 4-week period following the provision of a splint.
There are various other types of splint suggested, for example the Foil-cement splint, the Titanium–Trauma splint, the Fibreglass splint and the Orthodontic Bracket splint. A retrospective study of 208 root fractured teeth did not reveal any significant effect of splinting methods, splinting or no splinting, or duration of splinting on the frequency of healing of root fractures.11 However, this study included teeth that had been treated in the period before the era of adhesive dentistry and most of these root fractures were rigidly splinted with either gold or acrylic cap splints or arch bars. In another study, on the comparison of splinting techniques, it was noted that the reduction of lateral tooth mobility was significantly reduced in resin splints.15 In a study of the healing of intra-alveolar root fractures of 400 permanent incisors, the highest frequency of healing with hard tissue was noted with fibreglass splints and the lowest frequency with rigid cap splints.13
As for treatment factors, there is no significant relation demonstrated between the time that treatment is given after injury and the type of healing, but optimal repositioning favours healing. Antibiotics have not been reported to be particularly beneficial and further studies are needed to assess their efficacy.13 The treatment for a vertical root fracture is usually extraction owing to the poor prognosis.
Coronal (cervical) fractures and alternative treatment
Root fractures that occur at the cervical margin leave tooth margins either sub-gingival or sub-crestal and this makes it difficult to restore the remaining root. When there is a communication between the fracture line and the gingival crevice, a decision needs to be made regarding whether:
To extract the coronal fragment followed by orthodontic extrusion of the apical portion of the root. Provided that the remaining root is of adequate length to support a post crown, orthodontic extrusion of the root can be attempted to provide sufficient supra-gingival tooth tissue. The factors which need to be considered before orthodontic extrusion is planned are:
The technique of extruding the fractured root portion with orthodontic treatment was first described by Heithersay.17 Orthodontic extrusion can be carried out using either removable or fixed appliances. The choice of the appliance will depend on the number of anchor teeth available. Forces between 0.7N–1.5N have been shown to be ideal.18 If the extrusion is carried out too rapidly, it could lead either to stretching of the periodontal fibres or breakdown of the periodontal ligament, leading to relapse or ankylosis post-extrusion. To minimize the risk of relapse, fibreotomy, both before and immediately after extrusion, has been recommended.19 There should be a period of retention post-extrusion to allow remodelling of the soft tissues. The time period for this varies in different studies, but a month for every mm of extrusion has been recommended.20 A recent case report by Cuoghi et al describes the orthodontic, periodontal and prosthetic multidisciplinary management of a case with a root fracture to improve aesthetics and function.21
Alternatives are:
To extract the coronal fragment and perform periodontal surgery following definitive endodontic treatment, maintaining the biologic width when placing the restoration margins.
The root-treated radicular part could subsequently have a post and core crown constructed, possibly with a diaphragm (Figures 7 a, b), although more modern concepts would suggest that it is wiser to extend the crown on to the root face to maximize the ferrule effect.
To extract the coronal fragment and preserve the apical fragment to submerge it intentionally; it can be covered with a mucoperiosteal flap to maintain height and width of the alveolar bone which is also beneficial for implant placement in the future.
To extract the whole tooth.
Figure 7.
(a, b) A post and core constructed with a diaphragm.
Endodontic treatment
The chances of pulp maintaining its vitality following root fracture is better than that with luxation injuries with no fracture of the root.22 Sensibility testing following trauma can give an irregular response due to the inflammation, injury and tension to the apical nerve fibres. A negative sensibility response immediately after the injury does not indicate necrosis; a return to sensibility could be possible. Regular, combined clinical and radiographic examination following injury is essential and helps to diagnose pulpal necrosis, should it develop. Endodontic treatment should be carried out if needed, according to the dental pulp status and patient's symptoms, following any required reduction and immobilization. In apical or middle third fractures, the endodontic treatment is usually confined only to the coronal part/fracture line, as the apical fragment usually retains its vitality, demonstrated by presence of an intact lamina dura on radiograph and pain on exploration (Figures 8 a–c). The coronal portion of the canal should be temporarily dressed with non-setting calcium hydroxide prior to obturation with gutta-percha and this appears to be the treatment of choice for non-vital root fractured teeth.23 Mineral trioxide aggregate can be used as an alternative to fill the coronal canal after dressing the canal with calcium hydroxide.24
Figure 8.
(a) Root fracture of a maxillary central incisor in the middle third. (b) Endodontic treatment was instituted to the fracture line and filling of the root canal in the coronal fragment was carried out with mineral trioxide aggregate (radiograph 8 months post trauma). (c) Radiograph 12 months after the injury shows periodontal healing and absence of any periapical radiolucency.
The choice between retaining the fractured root (Figure 9) or its extraction should take into consideration the patient's age, maturity of the root, fracture position and possibility of future replacement with an implant.25 Any extraction should be carried out carefully, with minimal loss of the labial bone, using a flap surgery procedure if necessary, to aid the removal of the apical fragment through the socket. As the apical fragment usually retains its vitality, this portion should only be extracted when there is a specific clinical indication.
Figure 9. A root fracture and dislocation of a maxillary central incisor with a completely separated apical fragment that was extracted.
Follow-up of root fractures
Normally, root fractures have a good prognosis as a result of re-establishment of a collateral circulation between the pulp and the periodontal ligament, easing the tension in the pulp vessels.26 A minimum of one year, and preferably up to 5–10 years follow-up is advisable to determine the ongoing status of the pulp.26 Suggested follow-up procedures for permanent teeth with root fractures include review at 4 weeks and splint removal, clinical and radiographic examination at 6–8 weeks, 4 months (also the same period for splint removal in cervical third fractures), 6 months, 12 months and up to 5 years after injury.14
The treatment of root fractures is summarized in Table 2.
Clinical
Radiographic Findings
Treatment
Review and Follow-up
There may be:
mobility and displacement of the coronal fragment;
bleeding from gingival sulcus;
tenderness to percussion;
sometimes a transient discoloration of the crown;
a sinus tract. Sensibility testing may be unpredictable initially.
For fractures in the:
coronal third of the root the root – regular 90° intra-oral periapical film;
middle and apical thirds – two additional intra-oral periapical radiographs taken at +/- 15° to the original, or an occlusal film usually confirms the fracture.
Repositioning of the displaced coronal fragment to be carried out as soon as possible;
Immobilize with a flexible splint for 4 weeks. If the fracture is near the cervical area of tooth then stabilization for up to 4 months is recommended.
Monitor healing for at least 1 year. A minimum of 1 year and preferably up to 5–10 years follow-up is advisable to determine the ongoing status of the pulp;
Review at 4 weeks, 6–8 weeks 4 months, 6 months, 12 months and up to 5 years after injury. If pulp necrosis develops endodontic treatment of the coronal fragment to the fracture line is advised.
In the case of vertical root fractures there may be:
mobility;
a localized swelling or a sinus tract;
isolated deep probing depth or visible separation of fractured root segments.
Sometimes, there is:
visible separation of fractured segments;
halo pattern of resorption along the root surface;
a distinct radiolucent line indicating a fracture.
Extraction/removal of the fractured root is the treatment generally advised. This could mean hemisection or root resection for a multi-rooted tooth.
Prognosis for a vertically fractured tooth is poor.
Sequelae of root fracture
Uncomplicated healing.
Pulp canal obliteration, seen as a decrease in the size of the pulp cavity, is a common sequelae of root fractures. This could be partial or complete. It is also seen in cases of healing, eg in the apical portion of the root canal in cases of healing with hard tissue formation. Hence, if pulp necrosis is suspected in such teeth, the examiner should carefully determine the pulp status as the coronal part of the root canal could be the only part affected and the apical part could be obliterated.1 A study by Calişkan and Pehlivan of 56 root-fractured permanent incisors revealed partial or complete obliteration of the pulp space in 62.5% of the cases and partial or total pulp necrosis was noted in 37.5% of the teeth.6
In some cases, a slight yellow discoloration of the crown could be suggestive of coronal pulp canal obliteration. Sensibility testing should be carried out and other criteria, ie resorption of bone, loss of lamina dura and enlargement of the periodontal space at the fracture level, should be noted and treatment instituted if necessary.
Pulpal necrosis – There has been no relationship demonstrated between the frequency of pulp necrosis and the position of the fracture line. Root canal treatment should be carried out in cases with pulpal necrosis and usually confined only to the coronal segment to the depth of the fracture line as the apical fragment usually retains its vitality.
Root resorption – As discussed earlier, internal or external surface resorption could be noted during the healing of root fractures.
Conclusion
Immature permanent teeth with root fractures, root fractured teeth with no communication between the fracture line and gingival crevice and with minimally displaced coronal fragments have a favourable prognosis. A thorough clinical examination supplemented with radiography and vitality tests is essential for the diagnosis. Appropriate treatment planning with subsequent follow-up is essential for a good prognosis. Sometimes, a multidisciplinary approach is needed for optimization of the treatment outcome.