Wishney M. Potential risks of orthodontic therapy: a critical review and conceptual framework. Aust Dent J. 2017; 62:86-96 https://doi.org/10.1111/adj.12486
Stanford N. ‘Alternative facts’ and orthodontic advertising in the United Kingdom. Am J Orthod Dentofacial Orthop. 2017; 152:729-730 https://doi.org/10.1016/j.ajodo.2017.09.013
Ray HA, Trope M. Periapical status of endodontically treated teeth in relation to the technical quality of the root filling and the coronal restoration. Int Endod J. 1995; 28:12-18 https://doi.org/10.1111/j.1365-2591.1995.tb00150.x
Gillen BM, Looney SW, Gu LS Impact of the quality of coronal restoration versus the quality of root canal fillings on success of root canal treatment: a systematic review and meta-analysis. J Endod. 2011; 37:895-902 https://doi.org/10.1016/j.joen.2011.04.002
Chen SC, Chueh LH, Hsiao CK,. An epidemiologic study of tooth retention after nonsurgical endodontic treatment in a large population in Taiwan. J Endod. 2007; 33:226-229 https://doi.org/10.1016/j.joen.2006.11.022
Kelleher M. How the General Dental Council and NHS UDAs crushed the compassion out of dentists. Br Dent J. 2022; 232:(8)509-513 https://doi.org/10.1038/s41415-022-4147-4
Kelleher MGD. The legal fallacies about ‘if it was not written down it did not happen’, coupled with a warning for ‘GDC experts’. Br Dent J. 2020; 229:(4)225-229 https://doi.org/10.1038/s41415-020-1995-7
Woolf H. Access to Justice: Final Report to the Lord Chancellor on the Civil Justice System in England and Wales.London: HMSO; 1996
Jackson R. Review of Civil Litigation Costs: Final Report Lord Justice Jackson.London: HMSO; 2010
Lewis K. Professional standards and their escalating impact upon the dental profession. Br Dent J. 2015; 218:381-383 https://doi.org/10.1038/sj.bdj.2015.251
Satisficing in Dentistry. Who decides? Who benefits? Part 3 Martin Kelleher Kevin Lewis Dental Update 2025 51:4, 232-241.
Authors
MartinKelleher
MSc, FDSRCS, FDSRCPS, FCGDent
MSc, FDSRCS, FDSRCPS, FDSRCS, FCGDent, Specialist in Restorative Dentistry and Prosthodontics, Consultant in Restorative Dentistry, King's College Dental Hospital, London
This series of articles challenges some popular myths about supposedly ‘ideal’ treatment plans and is designed to provoke reflection and stimulate debate. It explains the concept of ‘satisficing’ (as opposed to ‘maximizing’) in dentistry, and illustrates how subconscious bias and self-interests might lead supposed experts to promote arbitrary aspirational standards and confuse them with what the law expects (the Bolam Test standard) and what is genuinely in the best interests of an individual patient. It is argued that sound, patient-centred, pragmatic planning and treatment is equally valid, with wider applicability, than routinely defaulting to a self-serving ‘maximalist’ approach.
CPD/Clinical Relevance: The ‘satisficing ‘concept has wide and profound application across many fields of clinical (and non-clinical) dentistry.
Article
‘Satisficing’ is a word created by combining ‘satisfy’ and ‘suffice’. It may be unfamiliar to some readers but is not new, having been first described in 1956 by the US psychologist and economist Herbert Simon, who later won a Nobel Prize. It means approaching something in a way that is sufficient for it to be a satisfactory solution for the required purpose at the time in question. ‘Satisficing’ can be viewed as the polar opposite of ‘maximizing’ which involves seeking the single, supposedly ‘ideal’, outcome or solution to a problem. Maximizing tends to be a culture of idealism and excess, seeking out the most extreme, extensive, intricate or complicated approach - while satisficing aims to do what is necessary and achieve a perfectly reasonable, adequate outcome without the downside risks of that additional complexity and perhaps cost that maximizing tends to involve. Advocates of maximizing often claim that they are pursuing perfection, excellence or the ‘best’ solution, while satisficers may question the basis for, or the validity of, such claims.
This series of articles has been examining examples of satisficing and maximizing across a wide spectrum of both clinical dentistry and other aspects of our professional lives in UK dentistry. It is deliberately challenging and potentially controversial in the hope of prompting self-reflection and discussion about who decides which approach is preferable, and who benefits most from the choices we and others make. Readers may find it helpful to read the sections in their original order; Part 1 included several key references.1
In this third article we discuss how supposedly ‘ideal’ orthodontic and endodontic treatment plans are, like the other areas we discussed in Parts 1 and 2,2 often promoted by actual or self-styled ‘specialists’ and other clinicians with a narrow, sometimes vested, interest in (and passion for) their particular field within dentistry.
Some of those ‘authorities’ might harbour somewhat self-serving views about the importance of their speciality in overall healthcare. Their opinions and techniques are usually promoted as being in ‘the best possible interests of patients’, but that often provides cover for ‘my specific area of interest is more important than anyone else's in healthcare …and therefore needs more resources and prominence within dentistry …and indeed, within general healthcare’.
When a case lends itself to more than one treatment approach, this can lead to unseemly turf wars and desperate straw-grasping as the promoters of each approach make and justify their case, and draw up their defensive lines.
Lurking under the surface of apparently altruistic and selfless motives in many areas of dentistry one can often uncover somewhat less honourable motives, such as status, professional and personal ego, security, or protecting a precious and valuable income stream. This creates an ever-greater imperative for all of us, to look past the hype and self-interest, and focus on what is genuinely in the best interests of individual patients, i.e. ‘personalized dentistry’
Maximizing and satisficing in orthodontics
Examples of ‘maximizing’ in orthodontics include maintaining an unshakable belief that an Angle's Class 1 jaw relationship is the gold standard which ought to be the goal, regardless of what has to be done to achieve that, or equal consideration being given to the well-known problems of relapse, root resorption or other complications.3,4,5,6 As yet, there is no worthwhile scientific evidence that an Angle's Class1 optimises long-term function of the dentition, or produces greater long-term human happiness or guarantees success in life generally. Various types of aligner technology, which are now frequently used to improve the visible front teeth (which are the most important ones for attraction reasons) have ‘eaten a lot of the traditional orthodontic maximizers’ lunch’ because a pleasing smile ‘satisfices’ for so many patients. Few (if any) patients come skipping along asking for an Angle's Class 1 occlusion, please.
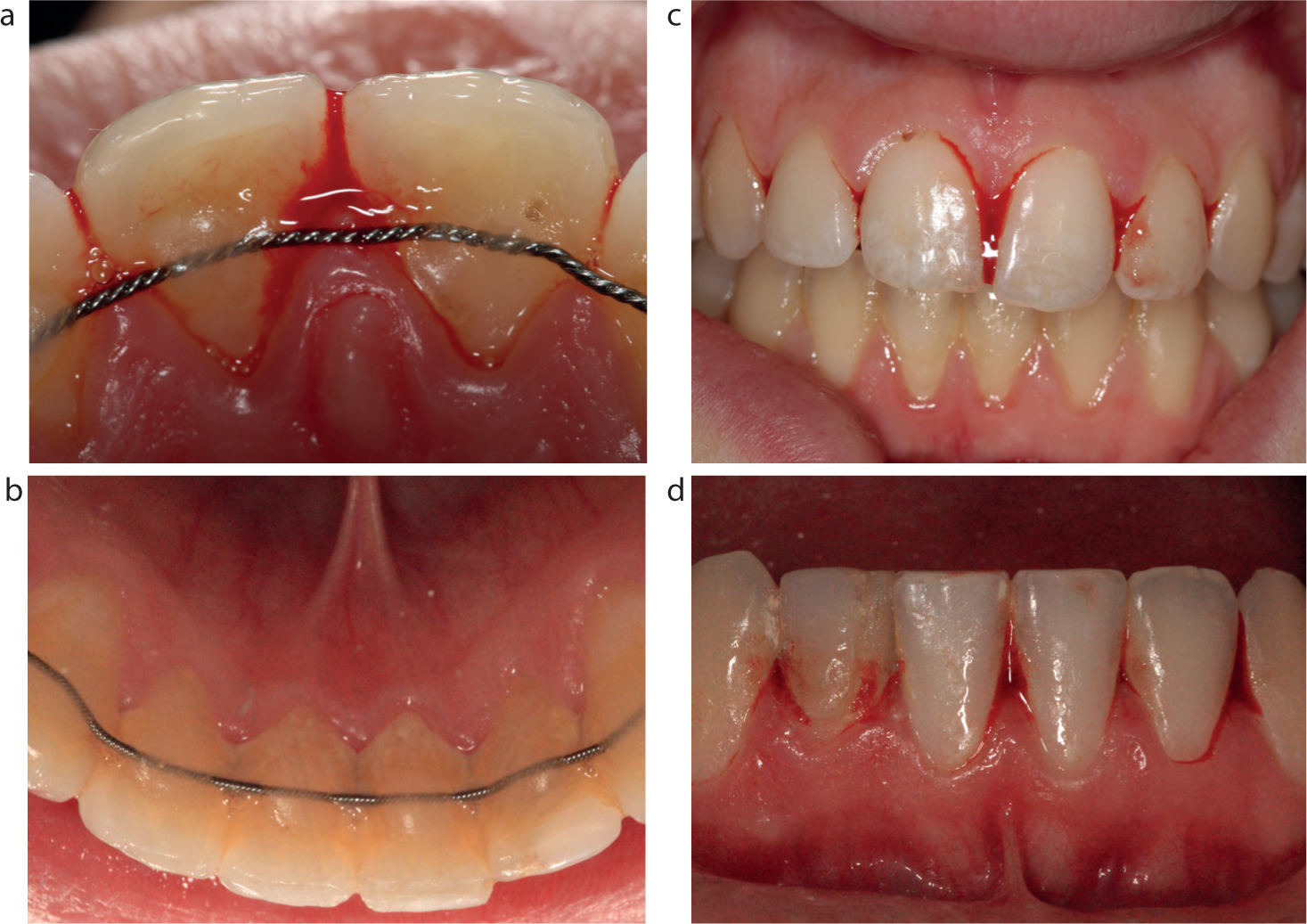
Advertising on various platforms and websites rarely draws enough attention to the possible longer-term implications of some types of orthodontic alignment, including probable long-term instability, or to the destruction of sound tooth tissue, sometimes undertaken by means of progressive interdental stripping to gain space, or to the downside risks, unpredictability and long-term time and costs of achieving and maintaining that desired appearance (Figure 1).3,4,5,6,7
Figure 1.
(a–d) Hyperplastic inflammatory periodontal disease caused by difficulties in cleaning due to the braided wire orthodontic retainers creating inaccessible areas (called ‘cols’)2 between the inflamed interdental papillae underneath them. Is that outcome a genuine long-term health gain?
In many cases viable alternative treatments exist to manage what appear at first blush to be traditional orthodontic problems, including post-orthodontic relapse. Some patients seeking changes in their dental appearance might not be fully aware of many other options of doing ‘sufficient treatment for it to be satisfactory’ (i.e. satisficing) to solve their perceived problems. The old adage attributed to Maslow, ‘to a man with a hammer, everything looks like a nail’, comes alive whenever there is a reluctance to look beyond one's own specialty or field of practice, for preferred solutions – and we can all be guilty of that to some extent.
Figure 2. Imbricated and irregular heights of lower incisors, and recession 6 years after 2 years of fixed appliances and ‘relapsodontics’. Note the probable dehiscences and the thin periodontal phenotype present.Figure 3. The patient's main concerns were the taller instanding lower right central incisor and the generally crooked incisors. Note the long and overlapping contact zones.Figure 4. ‘Relapsodontics’ after prolonged fixed orthodontic appliances. The patient's main concern was the instanding lower right central incisor and its visually taller tip.Figure 5. A reversible composite mock-up was carried out on the dried (un-etched) lower right central incisor to assess the patient's reaction to one possible concealment option. A Staedtler permanent black ink fine tipped pen was the used to draw just on the tip of the LR1 (taller tooth) to make it appear (temporarily) as being roughly the same visual height as the other incisors. The patient checked that outcome and approved those proposed changes being made for real, including the irreversible removal of the tip of the taller incisor because he felt sure that the demonstrated proposed outcome would ‘satisfice’ for him without undergoing further orthodontics, with progressive interdental stripping and then having to have a wire on the inside of his teeth, or having to wear a removable retainer indefinitely.Figure 6. At a subsequent appointment a 20-mm section of a Komet serration strip was used to check the ‘flossability’ of the contact zones. Two short non-cutting end sections of serrated thin metal strips (Komet) were placed to prevent phosphoric acid etching of the adjacent teeth. After 20 seconds, the etching gel was aspirated away and the lower right central incisor was washed and thoroughly dried so that it appeared frosty. Unfilled bonding resin was applied and air-thinned. The metal strips were removed before curing of that unfilled resin to prevent the unfilled resin from pooling against the strips. That thin layer of unfilled resin was then cured to leave an air-inhibited outer layer.Figure 7. Chilled hybrid composite was sculpted freehand to the labial of the lower right central incisor (LR1) and to incisal 3mm on the lingual of the tip of the lower left central incisor (LL1). Once cured, that longer (20 mm long) section of a Komet serration strip was re-used to cut through the unfilled resin on the adjacent un-etched teeth in seconds, thereby ensuring cleansability with floss. The taller tip of lower right central incisor (LR1) was shortened by bevelling just the lingual/incisal tip at 45 degrees to the vertical. Once again, a Staedtler black permanent ink pen was used to draw on the tip to check with the patient that this was the previously agreed amount for reduction of the LR1 incisor tip.Figure 8. Composite bonded on to the labial of lower right central incisor (LR1) and the lingual of the lower left central incisor LL1 before shortening and finishing and polishing with a Jet FG 7901 bur and a Komet H48 LQ bur.Figure 9.
(a–d) This ‘satisficing’ approach was done in minutes (apart from the mock-up & discussions) rather than attempting further speculative ‘alignerodontics’ over many months, which would have requiring much greater intrusion in to the mouth for progressive interdental stripping of several teeth as well as much greater time, inconvenience, discomfort and expense followed by a fixed wire retainer having to be worn indefinitely on all of the lower anterior teeth which would have had predictably adverse effects on his periodontal health.
Risk assessment and management
The teeth could have been left as they were, but having invested a lot of time, money and effort into the originally recommended orthodontic treatment, the patient wanted a quick, inexpensive and low-risk solution. The risks were minimal because of the diagnostic temporary composite bonding, which had confirmed in advance that these proposed limited changes would ‘satisfice’ for him, meaning that it would be ‘sufficient to satisfy him’. The benefits of adopting a ‘satisficing’ approach for that patient were:
The previous incisor irregularities were now less visible and the teeth had not been moved once again to unstable positions. Only the tip of one tooth was reduced, rather than multiple teeth being progressively stripped interproximally.
The now much flatter contact zone shape changes on the lower right central incisor (LR1) labial composite would not allow further drift because the now-wider composite flat contact zone shapes at the LR1 stopped any further drifting or relapse.
All teeth were easily flossable – unlike the outcome likely with a fixed wire retainer (Figure 1) on the inside of all the teeth, and he did not have to wear any removable aligners or removable retainer indefinitely. Incidentally, the patient was completely unconcerned about the upper teeth, but if he had been, they could have been tidied up in minutes with some direct bonding.
The main point of a ‘satisficing’ approach is to personalize the treatment to solve that individual's perceived problem(s) effectively, and to do no more than that. In Part 1 we highlighted the views of Phil Crosby, one of the world's recognized authorities on quality issues, who warned us against harbouring a self-indulgent, inward-facing perception of quality in a technical sense, when we should be measuring quality in terms of how well the product or service meets the needs, expectations and demands of the individual customer.
Clinical Case 2
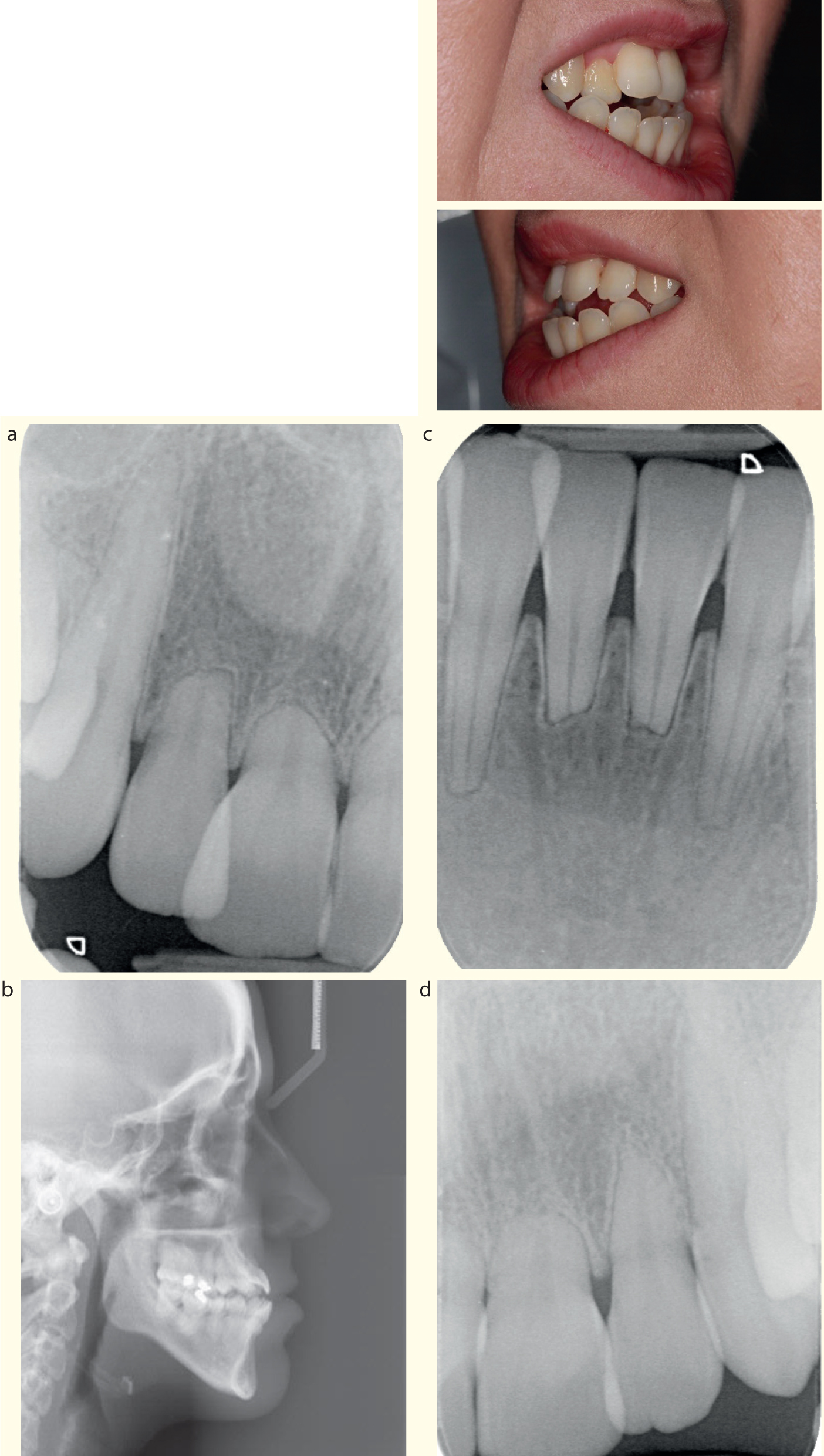
Figure 10. This female patient presented with an anterior open bite having had two courses of fixed orthodontic teatment and one with aligners, all of which had relapsed subsequently.Figure 11.
(a–d) Radiographs demonstrating the anterior open bite present, as well as the extensive root resorption at the upper and lower incisors. In spite of that radiographic appearance, the teeth were not particualrly mobile, probably because they sounded ankylosed when tapped and the AOB present prevented any occlusal contact or overload.Figure 12.
(a–d) The anterior open bite and other irregularities were concealed by standard nightguard vital bleaching of the side (‘framing’) teeth first of all, followed a week later by a single session of freehand direct bonding using chilled hybrid resin composite, with no laboratory wax-up or fiddly stent. That outcome was suffient to be satisfactory for that patient, i.e. it ‘satisficed’. The validity of her consent was strengthened because she had been given the opportunity to approve those proposed changes during discussions, after she had seen the diagnostic bond-up done on her dried (not etched) teeth.
For consent to be valid, clinicians need to inform patients of the risks, benefits and limitaions of what they are proposing, as well as the options of doing nothing, or considering various combinations of bleaching and bonding, or doing some other possible treatments that might satisfice for that particular patient. Quite legitimately, a clinician might favour a specific treatment approach, but should not recommend or pursue it if it is not in the patient's best interests. The clinician may not be able or prepared to carry out one or more of the possible treatment options personally, but the patient still has the right to know that they exist, and/or choose them, if necessary, from a different provider. The fact that a patient responds to a practice's marketing, and attends specifically requesting the advertised approach, should not be miscontrued as giving their valid consent. Any form of elective ‘cosmetic’ treatment carries particular risks from a consent perspective, as explained in Part 2 of this series.2
Satisficing and maximizing in endodontics
Some endodontists appear adamant that their sometimes dogmatic approaches, involving their preferred design and brand of single-use instruments, gadgets and microscopes, are all essential and required on every occasion to ensure complete instrumentation, copious irrigation and obturation of all variations of all canals to the radiographic apex (or whatever apical area is in fashion this week) (Figures 13 and 14).
Figure 13. Some maximalist endodontists proclaim that is essential for every root canal procedure to be carried out under rubber dam, and using a microscope together with a plethora of endodontic gadgets with copious irrigation. None of them routinely do endodontics under the NHS UDA system, but some have been known to testify on oath before the GDC that their aspirational standards are the required standard, rather than telling the truth, namely that it is the Bolam Test standard (of ‘reasonableness’) that is what the law demands of the average practitioner, and it requires a serious departure from even that ‘reasonable’ standard in order to satisfy the legal threshold for a finding of ‘misconduct’ by the GDC (see later in this article, and also in Part 1 of this series regarding the Bolam Test1).Figure 14. Two endodontic specialist clinicians and a nurse in full theatre warpaint doing a LocSSIP before doing an apicectomy on a ‘structurally knackered’ upper central incisor. Factually, despite all the changes in instrumentation, magnification and illumination, the overall tooth survival after endodontic interventions is not much better overall than many years ago. Assertions based upon some seriously biased, highly selected studies, often carried out by endodontic specialists in institutional settings (sometimes influenced by a Heisenberg effect and personal zealotry) are not the standard required of the average UK general dental practitioner, and they should not be intimidated into thinking that it is.
This insistence, perhaps deliberately, makes general practitioners more likely to refer patients for endodontics rather than attempt pragmatic, but effective, treatment themselves. Perhaps, less obviously, it also progressively de-skills general practitioners and makes them (and their patients) even more heavily dependent upon their specialist colleagues. The number of registered endodontic specialists (about 380) is clearly insufficient to meet the entire endodontic needs of the UK population (about 68,000,000) and so, as Marilyn Monroe and Dean Martin once pointed out, ‘Something's gotta give’.
Many endodontic gurus promote sundry variations of their beliefs, despite copious evidence from long-term authoritative studies that the coronal seal is probably equally important, or perhaps more important, in determining tooth survival than the endodontic obturation.8,9,10,11 However, that ardent, apparently altruistic, promotion of the ‘highest possible standards for all patients’ might not survive closer examination, scrutiny and challenge in relationship to conflicts of interests or possibly, commercial bias in some cases.
Whenever there is a claim about ‘a suboptimal root filling’ having to be redone by a specialist, the Van Niewenhuysen study12 is rarely cited – let alone pronounced – by some ‘endodontic experts’ instructed to act for some parasitic claims company, or by some opportunistic lawyers, or a supposedly well-informed and fair regulator. That Dutch study reported on over 1000 roots over a 6-year period and compared endodontic re-treatment of approximately half of those roots with radiographic monitoring of the other half.12
Technical assessment of the endodontic re-treatment group showed that the root filling was improved in about one-third of cases, was identical with the initial treatment in about 11%, and was worse than the first treatment in 3% of the canals. In other words, there was about a 50/50 chance of an improved technical outcome when re-done by a specialist endodontist using all the toys and irrigation, regardless of time and expense involved. Clinical assessment of the re-treatment of symptomatic roots showed that approximately 70% of the re-treatments were judged successful, 18% showed some healing and 2% had failed.
In the control group, monitoring radiographically (median time span 6 years) led to maintenance of the status quo in 95% of cases, healing in 2% and failure in 3% of the canals. When faced with a ‘suboptimal’, but asymptomatic root filled tooth, with a decent coronal seal and based on that rarely cited study, pragmatic ‘satisficers’ – both patients and dentists – might well be content enough to take a 95% chance of having no problems over an average of 6 years, versus about 50% not necessarily getting a technical improvement with endodontic re-treatment, which involves a very significant time and treatment commitment and additional financial outlay. And who could blame them?
Dispassionate ‘satisficers’, given odds of 95% of no problems with the observation approach for adequately coronally sealed, but incompletely root-filled teeth, might choose that approach as being a reasonable option. Taking that sort of pragmatic view would be supported further by the huge studies, involving millions of teeth, in a range of different countries that show that the vast majority of ‘non-ideally’ root-filled teeth with a decent coronal seal survive in a ‘satisficed’ state for a large number of years.10,11
Getting to the ‘root’ of the problem?
In recent years, the landscape of general dental practice has changed in many ways, but none more so than where endodontics is concerned. Recent graduates and young dentists view endodontics very differently from their counterparts in past generations.
This might be because they do not feel confident to carry out these procedures to an acceptable standard themselves, nor to weather the potential criticism if they were to decide to keep a questionable previous RCT under review. The safer option is to refer the patient to a specialist endodontist, or to consider an extraction. Or it may be the result of fear-inducing stories recounted by indemnity providers, or lectures from hungry endodontists who can display carefully selected high-res images of successful identification and obturation of more canals, accessory canals and lateral canals than most of us will encounter in a lifetime, and actively encourage the dentists to refer because of that subtly generated sense of inadequacy.
But given all of the above well-known evidence from a variety of well-respected sources,8,9,10,11 why has the fear of ‘underperformance’ and resulting litigation, or possible censure by the GDC, or the threat of hypercritical ‘audits’ by remote NHS agencies, aided by some endodontists’ aspirational ‘maximalism’ (very possibly skewed by their vested interests), resulted in the perverse outcome of the widespread unwillingness of many dentists to undertake pragmatic endodontics to the best of their ability, achieving a reasonable standard of disinfection and then properly sealing the coronal aspects of the teeth? Is that approach often more desirable for many patients than a rapid proposal and appearance of ‘the healing tongs’?
How, in the face of all the relevant evidence,8,9,10,11 has the prettiness of the radiographic appearance, at one end of the tooth, apparently trumped an equally important, if not more critical, emphasis on producing an effective coronal seal at the other?
One can readily understand the widespread reluctance among some NHS GDPs to be judged by some ‘maximalist’ (private) endodontist's aspirational beliefs, after having doing their best for the insultingly low UDA return in revenue. It is no secret that this has resulted in multiple molar extractions rather than the ‘satisficing endodontics’ being done for many in the UK population previously. All of these questionable molar extractions collectively carry a long-term legacy that is different from (but no less significant than) the restorative legacy of a ’heavy metal generation’ partly created by a previous NHS ‘drill and fill’ culture.
Even after the recent minor enhancements to the calculation of the UDA values for endodontics, the shamefully low financial reward for these demanding procedures, with their above-average operating cost in terms of time, materials and instrumentation, probably combined with fear of censure for anything less than a ‘perfect’ outcome, has crushed compassion out of many dentists and made extractions a more attractive ‘lower risk-higher return’ option for many busy practitioners.13
Assessing endodontic outcomes
Another probable cause for the misplaced primary focus on the apical seal and the radiographic ‘evidence’ of its existence, is the third-party monitoring of healthcare delivery by agencies such as the NHS Business Services Authority and Performance Assessment Groups. They use this as a measure of, and proxy for, the quality of endodontic treatment producing effective disinfection of the root canal system. That is not because the exact apical position is critically important or evidence based (the working length diktats change regularly), nor because it is logical to extrapolate in this way (it isn't), but simply because it is convenient and relatively cheap and easy to do remotely.
Unfortunately, it can also be (mis)used as a justification for referrals to the GDC, where those same flawed assumptions come into play for a second time and in some instances, the same experts get a second day out and a second payday. In most of these cases the patient reports no symptoms at all, and in many instances the radiographic appearance of the supposedly ‘sub-optimal’, ‘failed’ or ‘inadequate’ RCT has remained unchanged for many years.10,11,12 But curiously, that highly relevant and material context is rarely explored or even mentioned, perhaps because you can't see it on a two dimensional peri-apical radiograph.
The clinical records are another ‘proxy’ factor used by an ever-widening group of bodies such as the NHS Business Services Authority, the Dental Performance Advisory Groups of NHS England, some of the in-house, GDC-employed, but supposedly entirely ‘independent’ clinical advisers, and the GDC's go-to ‘hired gun’ prosecution ‘experts’, purportedly to assess the quality of care in endodontics.13,14 Especially in busy NHS practices where time is at a premium, clinical records can be easy enough to criticize most of the time, which is the main attraction of course, but hardly the fairest or most informative view when it comes to assessing the effectiveness of the equally (or more) important coronal seal of restorations on the treated teeth. Distant assessments based on the radiographic prettiness of readily available two-dimensional imagery are convenient, cheap and therefore attractive to those in this dubious ‘expert witness for hire’ or ‘clinical audit’ industry. But in hard evidential terms, they are a real cop out and a potentially misleading one too.
The process of calling in batches of clinical records for review and ‘audit’ has somehow come to be accepted as a valid proxy for quality assuring clinical dentistry. That myth needs to be busted, and the sooner the better. The methodology started as a clumsy means of validating NHS fee claims and/or the attempted recovery of fees from practitioners, but the authorities quickly realized that this could be widened to provide a cheap, quick and easy means of pressurizing practitioners out of claiming fees to which they were in fact perfectly entitled, on the spurious grounds ‘that if it's not in the records, it didn't happen’.14 Or worse still, ‘but even if it is in the records you can't assume that it happened’.
In former years the (then) Dental Reference Service had an in-house team of dentists who physically examined patients and provided reports and opinions. But logistically they could only ever reach a very small sample, and in England and Wales, they were eventually deemed not sufficiently cost effective. To compensate for their demise, the myth was perpetrated and actively promoted that the same information could be achieved by looking at paper and electronic records, and this also provided cover for non-dentists to be ‘trained’ to look for specific things and be used to carry out these reviews much more cheaply. Radiographs are, of course, two-dimensional and of variable quality anyway, but they are readily available and cost the authorities nothing and so, as a matter of deliberate policy, disproportionate significance started to be attached to them.
Incidentally, it is apparently not sufficient that you take a good quality radiograph or digital image and retain it for posterity; you must also record why and the fact that you did so, and preferably write a small PhD thesis level of report on what conclusions you drew from it at that time. Even if there were no material conclusions to draw. Maximizing (and duplication) is clearly alive and well in audit land.
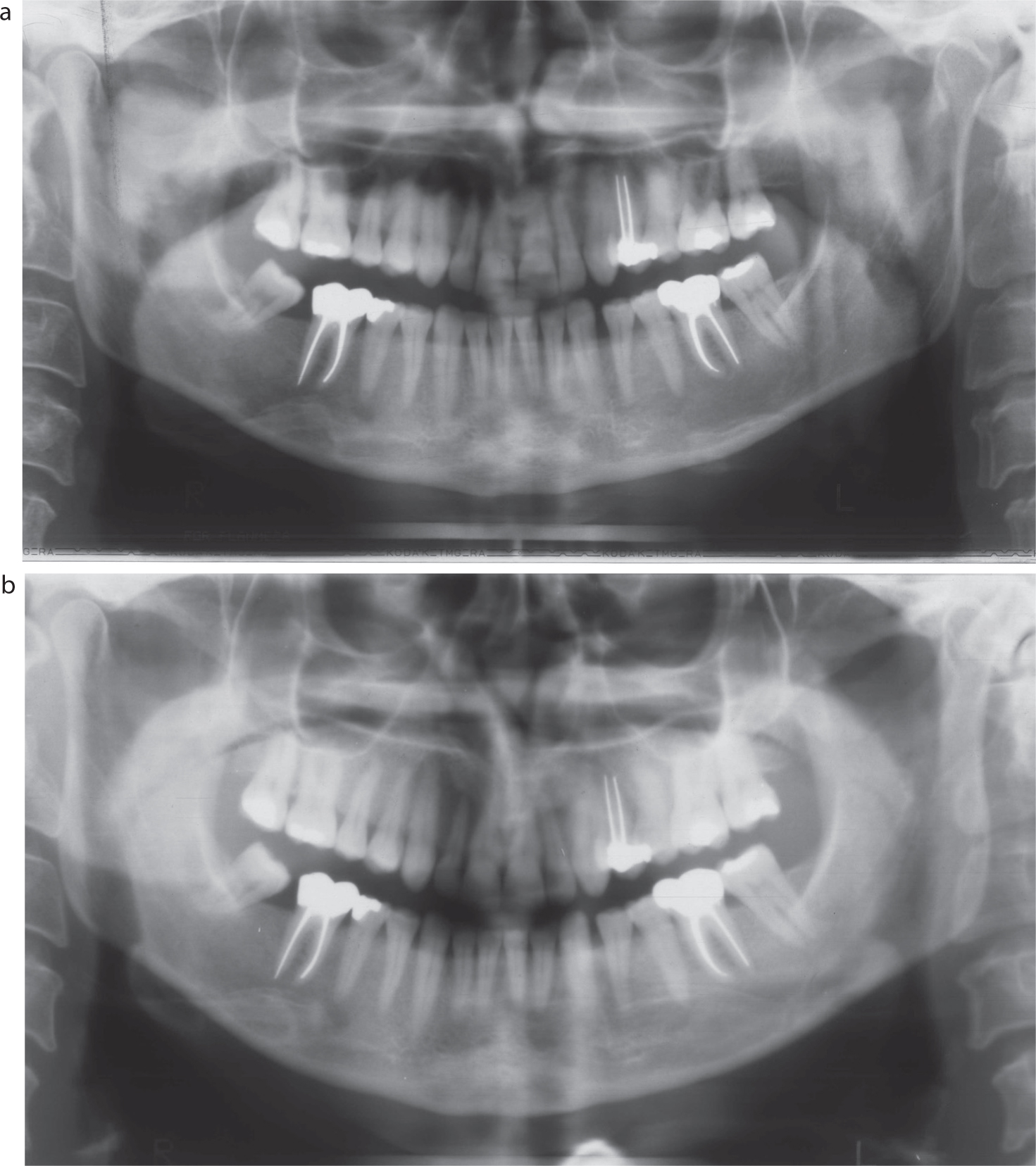
The inconvenient truth for ‘maximizing’ endodontists, or some self-styled ‘experts’ acting for no win-no fee law firms and/or the GDC, is that the vast majority of the bacterial load is in the coronal part of the tooth, and is not visible radiographically. Eliminating those micro-organisms effectively by disinfecting that area properly, first with prolonged ultrasonics and then endodontic instrumentation to allow copious irrigation prior to pragmatic obturation, and then stopping any re-infection by effective sealing, would not be evident radiographically. But just doing that probably ‘satisfices’ in more cases than the ‘maximalists’ might care to admit, and probably accounts for why so many supposedly ‘sub-optimally root-filled’ teeth survive for ages in those huge long-term studies (Figure 15).10,11
Figure 15.
(a) An OPT radiograph taken 35 years after three root canal treatments, followed by sealing crowns, had been carried out under the NHS in 1974. (b) An OPT taken 45 years after the original NHS treatment showed that the teeth survived with that ‘satisficing’ treatment
Finally, it is pertinent that the endodontic regeneration techniques, now getting increasing publicity, rely mainly on local disinfection and sealing in of bioactive materials with some very effective coronal bonding. Future generations of dentists are likely to express astonishment that, even when only a small part of the pulp was exposed, damaged or locally inflamed, that it was once deemed to be absolutely necessary to undertake aggressive and irreversible endodontic instrumentation for the whole root canal system, regardless of any structural damage done to the tooth in the process. These observers might be surprised that this was done for ‘maximalist’ (perhaps self-interested) beliefs at that time, or possibly for the sole purpose of ‘proving’ to third parties that all the contents of all the root canals had been mechanically removed and (implicitly) irrigated with powerful hypochlorite, prior to three-dimensional obturation. Even when judged on a two dimensional radiograph, which may seem crazy enough now and that might well seem even crazier when viewed by others in the future.
That is/was the nirvana for many (perhaps vested-interest) endodontic specialists, even though sensible ‘satisficing’ approaches, with a decent coronal seal, would probably have saved many compromised teeth for long periods of time, for lots of deserving patients at an affordable cost to them.8,9,10,11
Satisficing, the law and the GDC
The cost of professional indemnity for UK dentists is among the highest in the world, owing to a combination of a highly consumerist society with a well-developed ‘blame and compensation culture’, a legal environment that makes claims more likely, and a uniquely hostile and heavy-handed regulator in the shape of the GDC.
However, a further contributory factor is, surprisingly, to be found in the plethora of guidelines from a wide variety of sources, the majority of which fail to make clear whether they are intended to be viewed as minimum acceptable standards, or something much more aspirational.19, 20 It is entirely understandable that many organizations issue guidelines in good faith, with the laudable aim of driving up standards in a particular area of dentistry in which they have an interest, but ‘best practice’ and ‘minimum acceptable standards’ are very different things, and in the wrong hands can cause a great deal of harm if misunderstood or conflated.
This lack of clarity, even from some apparently ‘authoritative’ sources, some with scarcely concealed vested interests, as we saw in Part 1 of this series,1 is compounded when evidence-based, objective facts regularly appear alongside wholly subjective opinion of unclear provenance, within the same document(s). This creates a confusing and unhelpful pot-pourri for practitioners, making it more likely that some of that well-intended guidance will be taken out of its proper context, misunderstood and applied inappropriately. But it is also a trap for the unwary ‘expert’ who uses these guidelines and standards as a convenient point of reference without properly investigating and understanding them, or recognizing their inherent potential ambiguity.
A refreshing exception to this was the decision of FGDP(UK) in 2016 to update its suite of Standards documents with clear labelling of the intended interpretation of each stated standard, and this admirable approach has continued through FGDP's transition to the present-day College of General Dentistry (CGDent). At the time of making this change, FGDP explained:
‘In recent years the Faculty has heard complaints from practitioners that our previous editions of these guidelines have been misinterpreted. That aspirational guidance has been wrongly interpreted as essential requirements.’
Another laudable example was the Department of Health's original (2009) HTM01-05 Decontamination guidelines, which had clearly distinguished between a minimum standard to have been achieved by a specified date, and a more aspirational ‘direction of travel’ to strive for in the future. Examples like this are both rare and welcome.
Clinical negligence
It is no secret that the cost of clinical negligence claims brought against UK dentists has risen exponentially over the past two decades. The main driver for this was the 1999 Wolff (‘Access to Justice’) reforms to the Civil Justice system,15 which allowed conditional fee agreements (commonly known as ‘no win-no fee’) for the first time in this type of litigation. From 2001 to 2011, there was a sharp increase in the number of claims, and an even greater explosion in the legal costs associated with them.16 This unintended and undesirable consequence led to further reforms introduced in 2013,17 designed in part to rein back the excesses of the no win-no fee law firms who had ruthlessly plundered the opportunity created by the 1999 reforms, for their own benefit.
The damages (compensation) paid to a successful claimant comprises two elements: general damages (pain, suffering, inconvenience etc) and special damages (out of pocket costs including the cost of any remedial treatment and care costs, travelling, loss of earnings/income etc). When negotiating an appropriate level of special damages for a patient who has successfully brought a clinical negligence claim, it is a curious legacy of the Law Reform (Personal Injuries) Act of 1948, and subsequent changes made to the civil justice system that allows the calculation to be based upon the presumption that the patient will seek any remedial treatment privately, even if the original treatment was provided under NHS arrangements, and should be given sufficient financial resources to cover the full private cost of that from any provider of their choosing. This remains the case even if they are entitled to that treatment within the NHS, and even if they could access such theoretic treatment free of charge. There is no requirement that the patient should ever undergo that treatment privately, or at all. The compensation may be calculated on the assumption that the patient requires the most complex, extensive (and expensive) remedial treatment, but once they have the money they are free to choose simpler treatment, less treatment, cheaper treatment or no treatment at all. Indeed the patient might prefer to spend their winnings on a new kitchen, a car or a luxury holiday, or to pay off a credit card debt, all of which many claimants have been known to do.
Inflating the level of damages in this way has had a further knock-on effect in that it makes it easier for the no win-no fee law firms to justify claiming a much higher level of legal costs without breaching the ‘principle of proportionality’ (although the law has taken an unduly lenient and relaxed approach to that principle, which has adversely impacted dental claims in particular).
The ‘no win-no fee’ business model relies on identifying claims that are likely to succeed and then carrying out the maximum amount of chargeable legal work, even if that makes no difference to the financial outcome for their client, and even if it delays the patient receiving any compensation due to them. It is the legal equivalent of carrying out unnecessary and/or excessive dental treatment, and both involve a degree of deception, taking unfair advantage of the likely gulf in knowledge and understanding between the patient and the professional person whose advice and guidance they are seeking.
So a ‘maximizing’ approach has been expressly allowed by the legal system and the no win-no fee law firms have certainly made good use of that in recent years. But moves are now afoot to switch to a more ‘satisficing’ approach, requiring successful claimants to seek any remedial care and treatment from an available, satisfactory and reasonable source sufficient to meet their needs, rather than on the presumption that they will head for the most expensive provider in the land and perhaps have more treatment than they would ever have paid for themselves. The BMA has understandably been leading the charge in lobbying for this change, but the government and the NHS itself has skin in the game here too, because the cost of litigation regarding NHS treatment is spiraling out of control and this is taking precious money out of the system and away from the delivery of front-line NHS services at a time when the NHS faces unprecedented challenges and demands.
Some are going further, calling for a new requirement for the claimant at least to show that the money is indeed being used for the purposes for which it is being paid. It is a fair point that if the claimant is electing not to undergo the supposedly ‘necessary’ remedial treatment, then what is the justification for paying them for this ‘out of pocket’ expense that they will never incur? What it amounts to is an additional and disproportionate top-up of their general damages, when that is already being paid separately and in full.
A very topical illustration of the belated recognition that a ‘satisficing’ approach is often more appropriate than a ‘maximizing’ approach, is the government's announcement18 that, as from April 2024, recoverable legal costs will be fixed and capped for clinical negligence claims valued at up to £25,000, which would cover most dental claims. This hopefully brings an end to a shameful 20 years of opportunistic law firms claiming fees that are often many times greater than the damages received by the claimants they are supposedly representing.
The GDC's Fitness to Practise procedures
It is a fundamental principle of professional regulation in healthcare that any intervention should always be proportionate, and the minimum necessary for the protection of the public and the maintenance of public trust and confidence in the profession and its reputation. In summary, this is the epitome of a satisficing approach, enshrined in law, and the very opposite of a maximizing approach.
Reflecting this, any case being investigated under the GDC's Fitness to Practise procedures should always be concluded at the lowest possible level, consistent with these aims. In the very small minority of cases where a hearing is deemed necessary, and a finding of misconduct and current impairment is made, the relevant committee is required by law to begin its consideration of an appropriate sanction, from the lowest possible level, and then work upwards in stepwise fashion until the minimum appropriate, suitable and proportionate sanction is agreed by the committee, reserving the ultimate sanctions of suspension or erasure (‘striking off’) for only the most serious cases where no lesser sanction would suffice. Here again the law demands a satisficing approach. Rushing headlong to a disproportionate or maximizing approach would leave the GDC and its committee vulnerable to legal challenge, an outcome that nevertheless happens a lot more often than one might wish.
The GDC and its Professional Conduct Committee must make its decisions based on the evidence presented, and no finding of misconduct should ever be made unless there is clear evidence of a serious departure from standards that would be deemed to be acceptable and reasonable by a responsible body within the profession. This would, in general terms, need to be a much lower standard than that which would apply in a clinical negligence claim, as explained in Part 1 of this series.1 A modest or minor departure should not be sufficient to satisfy the legal test for a misconduct finding by the GDC. If the defendant dentist is a general practitioner, then their performance and conduct should be measured against that of other general practitioners, not against a higher or specialist-level standard. Similarly, a registered specialist providing treatment within that field should be measured against colleagues working in the same specialty.
Enter the ‘expert’ witnesses instructed by the prosecution (GDC) and defence, respectively. Where they choose to position the ‘bar’ suddenly becomes crucially important14,19,20 because if they knowingly, inadvertently or subconsciously, adopt an unreasonably ‘maximizing’ approach and maintain that the standard achieved by the dentist is ‘far below’ their version of an acceptable professional standard, in one or more respects, that is enough for a finding of misconduct. This is an ever-present risk not only when unclear published guidelines are misinterpreted (see above and references 19 and 20), but also when specialists are instructed to provide opinions on treatment provided by non-specialists. If they adopt a more reasonable ‘satisficing’ approach, their evidence might be that the standard was perhaps below what might be considered ‘best practice’, ideal (or desirable), or even below a reasonable or sufficient minimum acceptable ‘satisficing’ standard, but (crucially) it is not so far below as to constitute a ‘serious’ or ‘significant’ departure from such a standard. The stakes here are very high and until you are the dentist ‘in the dock’, it may not occur to you how dangerous it becomes if the profession slides unthinkingly into a ‘maximizing’ mindset. Before you know it, dentists are found guilty of misconduct by the GDC when the treatment they provided would be viewed as reasonably satisfactory by the majority of their peers.20
A cynic might observe that some experts, especially those who derive a significant proportion of their income from this source, might have a perverse incentive to nudge the ‘bar’ up or down according to which party is instructing them. But whether or not they realize it at the time, experts cannot do so with impunity.14
October 2013 marked the end of the era of the self-regulation of UK dentistry and proved to be something of a watershed moment. The incoming Chair (William Moyes) was a lay person, selected and appointed by the Privy Council without reference to the dental profession. Barely 6 months later, he gave a now-infamous lecture to the (then) Faculty of General Dental Practice (FGDP), the 2014 Pendlebury Address, in which he spelled out his determination to regulate the dental profession much more rigorously than hitherto.
‘A regulator must be seen to act. Any delay or hesitation leads politicians to question whether the public can have confidence in the regulator… which, of course tends to undermine public confidence. So, this is the era of conspicuous regulation, when rapid and tough intervention by a regulator, with maximum transparency and publicity, is the expected response to any failure in the healthcare system. And, of course, there are many occasions when that is a reasonable expectation.’
One is tempted to point out, even at a safe distance of more than 10 years, that there are also many occasions when that is certainly not a reasonable expectation, but nobody at the GDC was listening.
The 18 months that followed can best be described as regulatory humiliation, with the GDC being subject to withering criticism by its own regulator, the Professional Standards Authority, by the Commons Health Select Committee, and in the House of Lords, by the Courts (in losing a judicial review brought by the BDA) and by many authoritative bodies within the profession.
Bloodied but unbowed, the GDC continued on its chosen path and in early 2018, changed its Disclosure and Publications Policy21 so that details of upcoming Interim Orders Committee (IOC) hearings, and full details of IOC determinations, were openly publicized and communicated to the media, despite the fact that cases at the very early IOC stage mostly involve completely uncorroborated, untested, often anonymous and sometimes vexatious allegations against a dental registrant. The impact of this very public ‘naming and shaming’ was compounded by the lengthening delays in the GDC's Fitness to Practise system, meaning that very damaging information could appear against a dentist's public registration entry and elsewhere in the public domain for many months (or years) before the evidence is finally tested and perhaps demonstrates that in reality, the allegations were unfounded and/or vexatious, and that there was little or no case to answer. By that stage, however, the maximum damage would already have been done, and yet there would be no comeback or remedy for the dentist concerned. This is a vivid example of why the satisficing versus maximizing question is a live issue for all of us.
The GDC's approach here has, for some years now, not been the minimum necessary to protect the public, and moreover, it strikingly departs from that of the GMC in this respect.22 The GDC still appears to be determined to demonstrate its muscular style of regulation, and to ensure that its deliberations and decisions reach the widest possible audience, irrespective of the potential harm done to the registrant's health or their overall wellbeing. While the GMC adopts a considered, balanced ‘satisficing’ approach in this regard, the GDC prefers a ‘maximizing’ approach. That is a deliberate regulatory choice then, and it is not an inflexible statutory obligation.
One is drawn to the conclusion that the GDC's default approach has become a ‘maximizing’ one, calculated and intended to impress an external audience and being much less concerned about the adverse impacts upon registrants. Only when constrained by law does it rather reluctantly adopt a ‘satisficing’ approach.
Summary
Over this series of articles we have seen that examples of satisficing and maximizing are all around us, most of the time. Neither is inherently more desirable than the other, but there is a potential tension between the approach we might want for ourselves in various situations, and what we sometimes adopt for, or promote to, our patients.
When used in the right situation, and with the right motives, both approaches are potentially equally valid. But in a world where many resources are finite, while needs, demands and opportunities are infinite, it behoves us as healthcare professionals to think carefully about the choices we are making for ourselves, for our patients and society more generally.
Every new patient to one clinician, is another clinician's former patient. Many of yesterday's apparent triumphs are today's or tomorrow's failures and disappointments, and the fact that we only ever see a small proportion of our own treatment failures can reinforce our beliefs and prejudices about ‘ideal’ treatment and delude us into believing that we are more consistently successful than is actually the case. In this series we have seen plenty of supposedly ‘ideal’ treatment plans coming unstuck (often, literally), and hopefully we have all come to appreciate the value of pragmatism, an open mind and appropriate clinical/professional humility. We don't and can't know all the answers, but we can at least start to ask ourselves some of the right questions more often.