Peck CC, Goulet JP, Lobbezoo F Expanding the taxonomy of the diagnostic criteria for temporomandibular disorders. J Oral Rehabil. 2014; 41:2-23 https://doi.org/10.1111/joor.12132
Eberhard D, Bantleon HP, Steger W. The efficacy of anterior repositioning splint therapy studied by magnetic resonance imaging. Eur J Orthod. 2002; 24:343-352 https://doi.org/10.1093/ejo/24.4.343
Oruba Z, Malisz P, Sendek J Flattening of the articular eminence is associated with the loss of occlusal support: radiological study. Aust Dent J. 2020; 65:53-57 https://doi.org/10.1111/adj.12736
Antony PG, Sebastian A, D A Comparison of clinical outcomes of treatment of dysfunction of the temporomandibular joint between conventional and ultrasound-guided arthrocentesis. Br J Oral Maxillofac Surg. 2019; 57:62-66 https://doi.org/10.1016/j.bjoms.2018.11.007
Toller PA. Use and misuse of intra-articular corticosteroids in treatment of temporomandibular joint pain. Proc R Soc Med. 1977; 70:461-463
Monje-Gil F, Nitzan D, González-Garcia R. Temporomandibular joint arthrocentesis. Review of the literature. Med Oral Patol Oral Cir Bucal. 2012; 17:e575-581 https://doi.org/10.4317/medoral.17670
Emshoff R, Rudisch A. Determining predictor variables for treatment outcomes of arthrocentesis and hydraulic distention of the temporomandibular joint. J Oral Maxillofac Surg. 2004; 62:816-823 https://doi.org/10.1016/j.joms.2003.12.020
Rosenbrg I, Goss AN. A modified technique of temporomandibular joint arthroscopic operative surgery of the superior and inferior joint spaces. J Maxillofac Oral Surg. 2020; 19:561-570 https://doi.org/10.1007/s12663-019-01291-0
Nyberg J, Adell R, Svensson B. Temporomandibular joint discectomy for treatment of unilateral internal derangements – a 5 year follow-up evaluation. Int J Oral Maxillofac Surg. 2004; 33:8-12 https://doi.org/10.1054/ijom.2002.0453
Dimitroulis G. The interpositional dermis-fat graft in the management of temporomandibular joint ankylosis. Int J Oral Maxillofac Surg. 2004; 33:755-760 https://doi.org/10.1016/j.ijom.2004.01.012
Dimitroulis G. The interpositional dermis-fat graft in the management of temporomandibular joint ankylosis. Int J Oral Maxillofac Surg. 2004; 33:755-760 https://doi.org/10.1016/j.ijom.2004.01.012
Sidebottom AJ. UK TMJ replacement surgeons; British Association of Oral and Maxillofacial Surgeons. Guidelines for the replacement of temporomandibular joints in the United Kingdom. Br J Oral Maxillofac Surg. 2008; 46:146-147 https://doi.org/10.1016/j.bjoms.2006.12.001
Johnson NR, Roberts MJ, Doi SA, Batstone MD. Total temporomandibular joint replacement prostheses: a systematic review and bias-adjusted meta-analysis. Int J Oral Maxillofac Surg. 2017; 46:86-92 https://doi.org/10.1016/j.ijom.2016.08.022
Horton CP. Treatment of arthritic temporomandibular joints by intra-articular injection of hydrocortisone. Oral Surg Oral Med Oral Pathol. 1953; 6:826-829 https://doi.org/10.1016/0030-4220(53)90286-2
Liu Y, Wu J, Fei W Is there a difference in intra-articular injections of corticosteroids, hyaluronate, or placebo for temporomandibular osteoarthritis?. J Oral Maxillofac Surg. 2018; 76:504-514 https://doi.org/10.1016/j.joms.2017.10.028
Onishi M. [Arthroscopy of the temporomandibular joint (author's transl)]. Kokubyo Gakkai Zasshi. 1975; 42:207-213
He D, Yang C, Zhu H, Ellis E Temporomandibular joint disc repositioning by suturing through open incision: a technical note. J Oral Maxillofac Surg. 2018; 76:948-954 https://doi.org/10.1016/j.joms.2017.12.006
Zhou Q, Zhu H, He D Modified temporomandibular joint disc repositioning with mini-screw anchor: part ii-stability evaluation by magnetic resonance imaging. J Oral Maxillofac Surg. 2019; 77:273-279 https://doi.org/10.1016/j.joms.2018.07.016
Martin-Granizo R, Varela E, Martinez I Resorbable pin effectively maintains disc repositioned in arthroscopy of the temporomandibular joint, two years later. A case report. Int J Oral Maxillofac Surg. 2017; 46 https://doi.org/10.1016/j.ijom.2017.02.1214
McKenzie W, Louis P. Complications following temporomandibular joint replacement: a 10-year retrospective review. J Oral Maxillofac Surg. 2015; 73 https://doi.org/10.1016/j.ijom.2015.08.681
Temporomandibular disorders. Part 5: surgical management Charles Crawford Emma Foster-Thomas Funmi Oluwajana Peter Clarke Martin James Sunil Khandavilli Athanasios Kalantzis Dental Update 2025 49:8, 620-625.
Authors
CharlesCrawford
Lead Clinician TMD Clinic, University Dental Hospital of Manchester
The temporomandibular joint (TMJ) is a complex arrangement with high functional requirements. Surgery is therefore only considered when conservative management has not been successful. Surgery may not always benefit and carries the risk of the condition worsening. There is a range of techniques available to the surgeon. The most commonly used is arthrocentesis and this is also the least invasive. The end-stage option for patients is total joint replacement. Whichever surgery the patient has received, it is likely that they will be in need of careful management by the primary care team for their continuing care. This article, the fifth in a series of six, outlines the scope of TMJ surgery.
CPD/Clinical Relevance: A range of techniques is available for TMJ surgery, and many post-surgery patients will require routine dental management in the primary care setting.
Article
For some patients with a temporomandibular disorder (TMD), the conservative management techniques discussed in this series so far will not provide adequate relief of pain, or acceptable function, and therefore a surgical intervention may be considered.
This article discusses the main surgical options for the management of TMD. These are described to demonstrate the range of techniques available to address conditions such as internal derangements of the joint, arthritic degenerations or congenital abnormalities.
General considerations
The temporomandibular joint (TMJ) is a synovial joint atypical in its range of movements and the functions that are required of it. No other joint in the body is equipped with the kind of functionality required for the precise and repetitive movements needed for mastication and speech, plus the ability to endure the heavy load of the maximum bite force. Surgery for this joint has specific challenges to overcome in order for these functions to be maintained or improved.
Surgical options range from relatively conservative to complex and extensive. An overview list of the different techniques and their indications is found in Table 1. It should be stated that the general expert consensus is to reduce the number of surgeries that a patient undergoes, so as not to compromise the outcome of a joint replacement where this is predicted as the inevitable endpoint. The three main techniques discussed are:
Arthrocentesis
Discectomy and arthroplasty
Total joint replacement
Procedure
Indications
Arthrocentesis
Disc displacement without reduction
Painful arthritis
Arthroscopy
Disc displacement without reduction that has relapsed following arthrocentesis
Simple injections
Painful arthritis
Arthralgia
Disc stabilization
Disc displacement without reduction that has relapsed following arthrocentesis and where the disc condition is favourable
Discectomy
Disc displacement without reduction that has relapsed following arthrocentesis and the disc condition has deteriorated
Arthroplasty
Recurrent subluxation
Boney hyperplasia
Total joint replacement
Functional breakdown of the temporomandibular joint (see Table 3)
As with all surgery there is the risk of complications. A list of those particular to the local anatomy of the temporomandibular joint is contained in Table 2.1
Risk
Comment
Perforation of the external auditory canal or cranial fossa
These anatomical structures border the TMJ posteriorly and superiorly
Facial nerve injury
The temporal and zygomatic branches lie between the temporal fascia
Frey syndrome
Sweating or flushing of the skin in the pre-auricular area following damage to the auriculotemporal branch of the trigeminal nerve
Neuropathic pain
Following damage to the somatosensory system
Haemorrhage
High vascularity due to branches of the carotid artery
Heterotopic bone and ankylosis
Either restriction of the joint space by abnormal bone formation or complete restriction due to the fusion of the condyle to the fossa
Airway compromise
Close proximity to the parapharyngeal space
Arthrocentesis
Arthrocentesis is a technique in which cannulas are inserted into the joint space in order to lavage it with a solution of the surgeon's choice. The most common indications for arthrocentesis are disc displacement without reduction, arthrosis with limited function, or a painful osteoarthritis.2,3
In disc displacement without reduction, the disc is most commonly anteriorly displaced. Rather than returning to its normal site on top of the condylar head (typically with a characteristic ‘click’ during opening), it creates an obstruction to the translation of the mandible down the articular eminence (commonly presenting as a closed lock). Patients frequently complain of a reduction in mouth opening, particularly if the closed lock is bilateral. Because of the absence of disc recapture, an anterior repositioning splint is unlikely to be of benefit.4 Arthrocentesis, therefore, aims to release the disc and break any fibrous adhesions that have been created.
Arthrosis/osteoarthritis typically results in the loss of the normal anatomy, with flattening of the condylar head and/or the articular eminence. In addition, some patients may be aware of a characteristic crepitus during function; however, in most instances, neither of these observations will have any clinical relevance. It has been observed that high body mass index has an association with osteoarthritis in the hip and knee joints, and so it is postulated that loading may be a key factor in the aetiology of the disease in the TMJs. In the case of the TMJ, this may be a result of parafunction, diet or adverse occlusal arrangement. Oruba et al5 noted that flattening of the articular eminence seen on orthopantomographs (OPG) may be associated with a loss of occlusal support.
If the change in articular anatomy progresses, it can affect the range of movement of the joint. When this is compounded by fibrous adhesions, arthrocentesis may offer some improvement. Furthermore, some patients will experience an associated pain resulting from the accumulation of inflammatory waste products. The release of cytokines and neuropeptides results in hard and soft tissue damage, inflammation and pain perception. In such cases, arthrocentesis may provide some relief as these chemicals are flushed away or at least diluted.
In severe cases, the loss of anatomy can result in more frequent disc displacements, subluxations or other joint dysfunctions. If these are present, arthrocentesis alone is unlikely to be sufficient, and more invasive surgery may need to be considered.
Arthrocentesis is the least invasive of the available surgical procedures. It can be performed under a local anaesthetic with sedation, or under general anaesthetic. However, the use of general anaesthetic allows the added advantage of adequate joint manipulation, which aids the process both from a diagnostic and therapeutic point of view, because the surgeon can feel the mandibular movement more easily. The technique involves entering the superior space with either hypodermic needles or cannulas with the aim to lavage the joint space in order to remove inflammatory metabolites and release any adhesions, thereby improving pain and function of the TMJ.
In terms of technique, arthrocentesis can be performed with a single puncture access, where two cannulas enter through same site, or by a double puncture access, where the two cannulas enter through separate sites.6,7
For the lavage, the operator can use a simple isotonic saline or Ringer's solution. Then, following the lavage, a medicinal solution can be introduced to offer longer-term pain relief. Different authors have described the use of corticosteroids, sodium hyaluronate, opiates, bupivacaine and other medicaments. The use of corticosteroids has been controversial owing to reports of further degeneration of already damaged joints with concerns about condylar resorption, atrophy and necrosis as potential side effects.8
A systematic review reported positive results in 83.5% of arthrocentesis procedures9 with outcome measures of the reduction of pain on a visual analogue scale or an improvement in the maximum mouth opening. Thus, it can be regarded a procedure with a high success rate that carries a relatively low cost and less morbidity when compared to most other surgical techniques. There are some reports that suggest chronic pain patients respond less well to the procedure than acute patients.10
In cases of disc displacement without reduction, it would seem logical to assume that the underlying condition of the disc would make a difference to success, so a severely deteriorated, perforated or macerated disc would not reduce as successfully as one that exhibits healthy anatomy. In addition, pathology of the lateral pterygoid muscle, which attaches onto the disc, may adversely affect the success of the surgery. For this reason, it is still advisable to implement conservative measures to relax the musculature prior to considering a surgical intervention. Having said that, arthrocentesis should not be delayed unnecessarily, as in cases with a short history of closed lock in a young adult patient, with little myofascial pain, the prognosis should be excellent with early arthrocentesis and post-operative exercises.
Discectomy and arthroplasty
Where the arrangement of the joint is causing persistent pain, and/or reduced function, which has not responded to more conservative management, then surgical alteration to that anatomy may be considered. The most common approach for this open surgery is an incision from the pre-auricular aspect to the root of the zygomatic arch. Care is needed to avoid damage to the facial nerve's temporal and zygomatic branches11 and any resulting palsy.
Removal of the disc, discectomy, can be used to free the movement of joints that have not released following arthrocentesis12 and remain symptomatic. Following its removal, the surgeon has a number of options for replacing the disc. Local structures may be re-deployed as a replacement. These include fat pads or aspects of temporalis muscle. It is also quite possible that the surgeon may decide not to replace the disc, but simply advance the retro-discal tissues. Success rates of 87% have been reported for discectomy without replacement at 5-year follow-up12 (where success was measured by reductions in the levels of functional pain and increases in mandibular movement). However, in recent years surgeons have commonly looked to replace the disc with a dermis-fat graft taken from the groin.13
Arthroplasty involves the reshaping of bony aspects of the joint and may include the condylar head, glenoid fossa, articular eminence and the removal of osteophytes. An arthroplasty may be used to create space for the free movement of the mandible where it has been restricted, or where the patient has suffered from frequent subluxations. In particular, the eminectomy procedure will, in most cases, create a significant increase in the volume of the superior joint space.14 Anecdotally, surgeons are generally cautious about planning this treatment owing to the unpredictability of the result and the very real risk of making things worse.
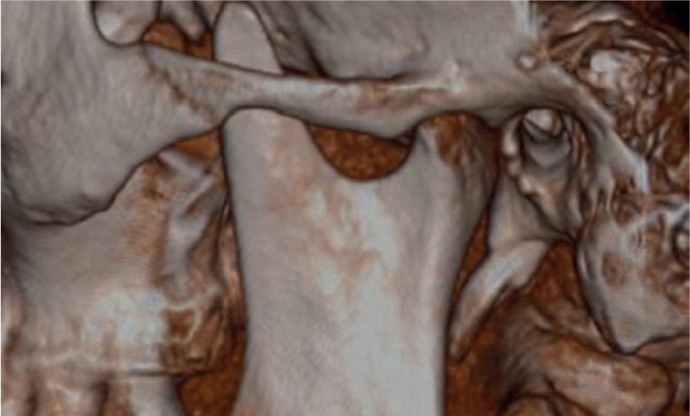
Variations on the procedure are made according to the presentation, and the nature of the osteoplasty is case dependent. For example, Figure 1 shows an unusual presentation of hypertrophy of the coronoid process.
Figure 1. Closed mouth view showing coronoid hyperplasia extending superiorly to the zygomatic arch. The phenomenon had left the patient with long term trismus, and the physical obstruction could only be released by removal of the bony projection (coronoidectomy) to allow full movement to be established.
Total joint replacement
Replacement of a temporomandibular joint is a significant technical challenge. The range of movements, complexity of attachments, and the functional requirements all create difficulties that need to be overcome in order to deliver a successful outcome. As such, a joint replacement is generally considered to be an end-stage option, and is only indicated in a small number of presentations (see for example Figures 2 and 3). This may include cases where there are significant congenital defects or advanced degeneration of the bony surfaces of the TMJs. A guide to these can be found in Table 3.15 The aims of surgery are to improve pain score, mouth opening (typically to 30–35 mm), and diet, and to normalize the occlusion if necessary. Therefore, careful patient selection (based on the predictions of achieving the above aims by an experienced surgeon as part of a multidisciplinary team) may be more important than the absolute indications or fulfilment of strict criteria.
Figure 2.
(a) Clinical and (b) radiographic view in a closed-mouth position of a patient with an 8-year history of bilateral TMJ dislocation following tooth extractions requiring bilateral joint replacement due to degenerative changes to the joints.Figure 3.
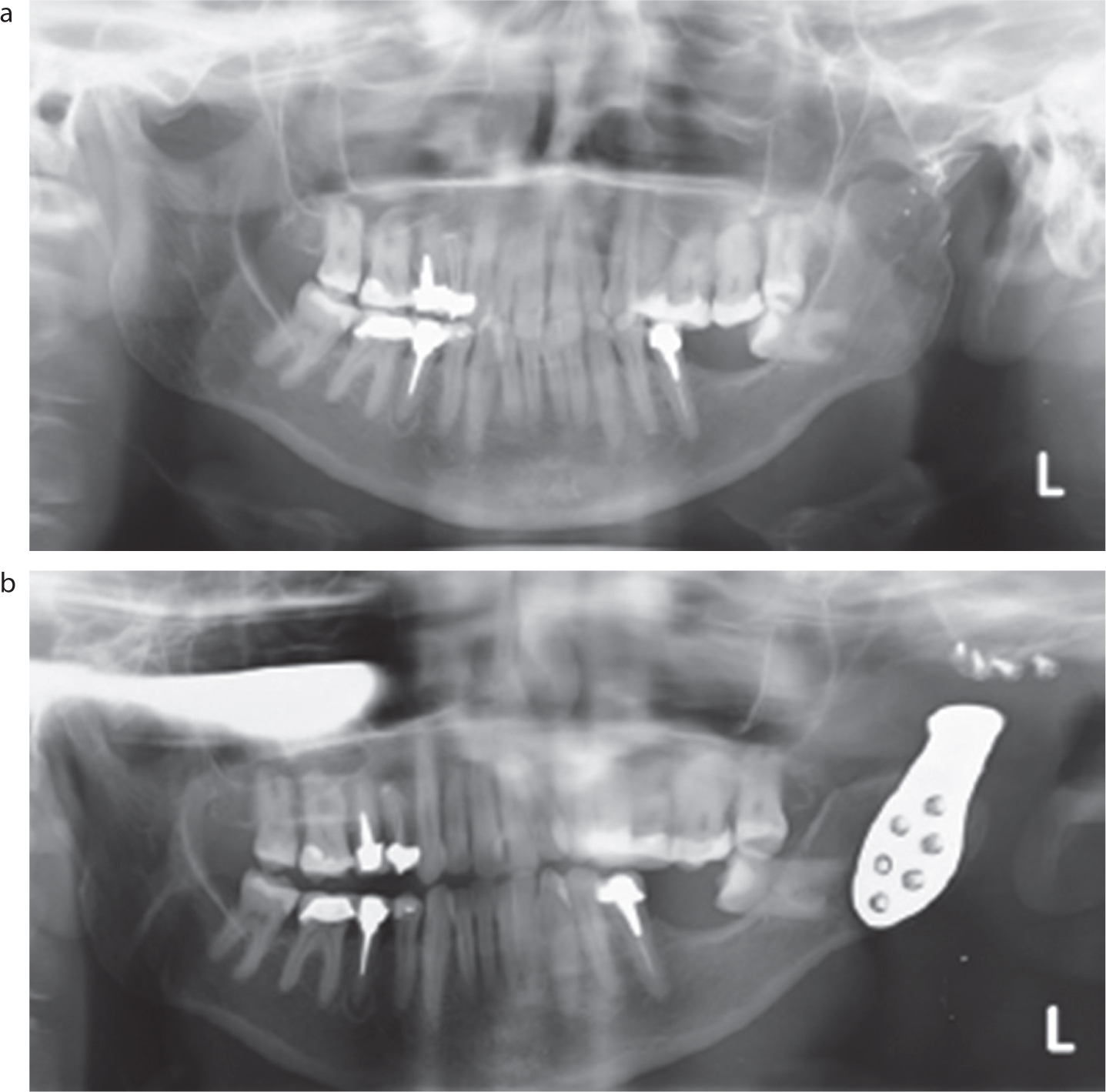
(a) Pre- and (b) post-operative radiographs of a unilateral TMJ total joint replacement subsequent to avascular necrosis following fixation of a condyle fracture. Note that a left coronoidectomy had previously been carried out in an attempt to improve function
Severe arthritis (degenerative or inflammatory)
Condylar hyperplasia or tumour (eg osteochondroma)
Failure of previous surgical treatments (including previous replacement)
Digital planning using computed tomography reconstructions from which digitally designed custom prosthetic joints can be manufactured for the patient is preferred (Figure 4). The final desired dental occlusion is incorporated into the planning process where necessary, so it is important that a restorative dentist is involved. In some circumstances, pre-surgical orthodontic treatment may be required in order to position the teeth in the optimum position for the envisaged surgical outcome.
Figure 4.
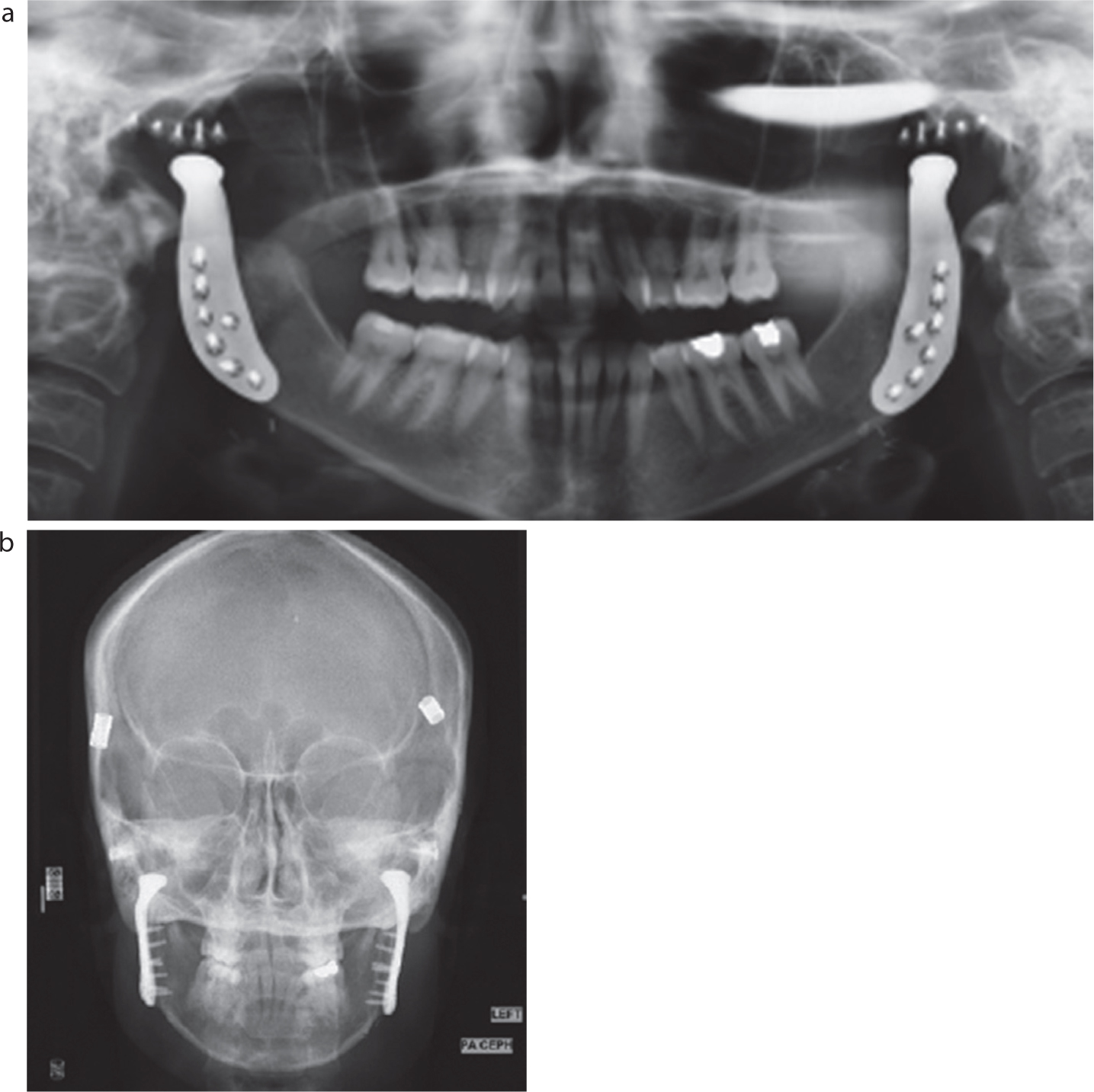
(a, b) Post-operative radiographs of a patient managed with bilateral TMJ total joint replacements. Note some hair decoration artefacts are present on the images.
A number of different systems are available to choose from for the manufacture of the prosthetic joints. These systems can employ stock or custom components. The systems that employ stock components rely on the need for them to be modified during surgery to fit the specific patient. In either case, they will typically comprise three parts:
A ramus/condyle (made from titanium or cobalt–chrome)
A fossa (made from ultrahigh molecular weight polyethylene or cobalt–chrome)
Screws (titanium or cobalt–chrome)
Various systems are available (an example of which is seen in Figure 5). A systematic review showed no significant difference between the systems in relation to pain score improvements or patient's diet.16
Figure 5. Example of a prosthetic temporomandibular joint. Courtesy of Zimmer Biomet.
Other surgical procedures
The literature describes some other surgical treatment options that are described briefly here.
Simple injections
Simple injections to the joint were first described by Horton in 1953.17 They differ from arthrocentesis as the objective is solely to insert pharmacological agents into the joint, and not to lavage or mobilize it; however, they can be combined in the same procedure. A systematic review compared the injection of corticosteroids, sodium hyaluronate and placebo injections post-arthrocentesis in patients with osteoarthritis.18 It was found that both agents were better than placebo for relieving pain, but that hyaluronate was preferable because there is some evidence that it may have a wider applicability and does not carry the same risk of side effects. Hyaluronate is already a component of synovial fluid and, therefore, its use does not risk further degeneration of the joint.
Arthroscopy
Arthroscopy is more invasive than arthrocentesis, as it differs by the introduction of a camera to view the internal aspects of the joint.19 The technique was pioneered in Japan in the 1970s.20 It can achieve the same goals as arthrocentesis (lavage of the joint and release of the disc), but the extra visualization can aid diagnosis, and allows for subsequent endoscopic techniques, such as minor arthroplasty or disc stabilization.
Disc repositioning and stabilization
A disc that persistently displaces can potentially be surgically repositioned and fixed into place in order to prevent relapse. Various techniques have been described to create this fixation, such as a suture that can be used to hold the disc to the auricular cartilage, a mini-screw can be placed to hold it to the condyle, or a resorbable pin.21,22,23 It should be kept in mind that the indications for this technique are limited, and so it is rarely performed.
Recovery
The time taken to recover from TMJ surgery depends upon the invasiveness of the surgery combined with any patient comorbidities. After the initial inflammation has resolved, it is important that from an early stage, patients begin to move the joint through the full range of motion to ensure that the increased function is maintained.
Patients who have had total joint replacement will have a much longer recovery process. Again, it is important that following the resolution of the initial inflammation they begin to move the joint through the full range of motion, but they will require close post-operative review to assess for:
Primary healing;
Early dislocation of the joint;
Control of pain;
Signs of infection. This has been reported in 4–5% of cases and can result in the loss of the prosthesis;24
Signs of damage to the facial nerve. Around 45% of cases will have initial nerve dysfunction, and for around 20% it will be permanent.23 Follow up neurosurgery may be required to correct these;
Signs of rejection of the prosthesis;
A satisfactory occlusion;
Appropriate early exercise regimen.
Even then the journey is not complete. Once the prosthesis is in place and the surgeon is confident that it has been accepted, there will be the need for restorative dentists and orthodontic specialists to assess the delivered occlusion and the functional capabilities. Depending on their assessment, post-operative treatment will often need to be instigated.
Management of the surgical patient in general practice
For many patients after surgery, the most daunting activity they have to carry out is a visit to the dentist. Opening the mandible far enough to allow reasonable access, and having to maintain that, are enough to exacerbate symptoms or even bring about a relapse. Similarly, for the dentist there may be much anxiety about seeing post-surgical patients. A conscientious clinician wants to be able to fully visualize the oral cavity to carry out high-quality work, yet in no way wants to jeopardize the surgical outcomes.
In order to achieve a comfortable, sustainable protocol for all concerned the dentist should:
Talk to the patient and determine what levels of mouth opening are comfortable to achieve and maintain. In this way realistic treatment plans can be constructed and carried out;
Correspond with the surgeon over the particular nature of the procedure undertaken and what the expected outcomes are;
Use a mouth-prop to support the joint for all but brief visits;
Where intra-oral imaging risks over-stretching the joint, revert to extra-oral imaging such as OPGs;
Where a satisfactory outcome cannot be achieved, the GDP should refer to secondary care, where a multidisciplinary approach may be implemented.
Conclusion
The surgical techniques described here can reduce pain and improve function for patients with particular TMD diagnoses. They are not used in isolation, but should be implemented alongside other more conservative modalities. General practitioners should take a detailed history of a post-surgery patient to understand their individual circumstances, and liaise with colleagues in secondary care, as required, to obtain all the necessary information. Dental treatment plans may need to be adjusted in order to accommodate the patient's circumstances and avoid exacerbation of symptoms.