Eisenburger M, Gray G, Tschernitschek H. Long term results of telescopic crown retained dentures – a retrospective study. Eur J Prosthodont Rest Dent. 2000; 8:87-91
Beschnidt SM, Chitmongkolsuk S, Prull R. Telescopic crown retained removable partial dentures: review and case report. Compend Contin Educ Dent. 2001; 22:927-940
Wise MD.London: Quintessence Publishing Co; 1995
Widbom T, Löfquist L, Widbom C, Söderfeldt B, Kronström M. Tooth supported telescopic crown retained dentures: an up to 9 year retrospective clinical follow-up study. Int J Prosthodont. 2004; 17:29-34
Cheung GSP. Fate of vital pulps beneath a metal-ceramic crown or a bridge retainer. Int Endo J. 2005; 38:521-530
Lundgren D. Prosthetic reconstruction of dentitions seriously compromised by periodontal disease. J Clin Periodontol. 1991; 18:390-395
Wöstmann B, Kothe A, Ferger P. Dental impact on daily living of telescopic crown retained partial dentures. Int J Prosthodont. 2008; 21:419-421
Griess M, Reilmann B, Chanavaz M. Telescopic retained overdentures in mentally handicapped and schizophrenic patients – a retrospective study. Eur J Prosthodont Res Dent. 1998; 6:91-95
Valderhaug J, Heloe LA. Oral hygiene in a group of supervised patients with fixed prostheses. J Periodontol. 1977; 4:221-224
Sorensen JA. A rationale for comparison of plaque retaining properties of crown systems. J Prosthet Dent. 1989; 3:264-269
Behr M, Kolbeck C, Lang R, Hahnel S, Dirschl L, Handel G. Clinical performance of cements as luting agents for telescopic double crown retained removable partial and complete overdentures. Int J Prosthodont. 2009; 22:479-487
Bayer S, Zuziak W, Kraus D, Keilig L, Stark H, Enkling N. Conical crowns with electroplated gold copings: retention force changes caused by wear and combined off-axial load. Clin Oral Impl Res. 2011; 22:323-329
Uludag B, Sahin V, Ozturk O. Fabrication of zirconium primary copings to provide retention for a mandibular telescopic overdenture: a clinical report. Int J Prosthodont. 2008; 21:509-510
Mundt T, Heinemann F, Golecki G, Schwahn C, Biffar R. Retention force of secondary crowns to copings after temporary cementation: the effect of crown material and luting agent. Biomed Tech. 2010; 55:335-340
Gϋngör MA, Artunç C, Sonugelen M. Parameters affecting retentive forces for conus crowns. J Oral Rehab. 2004; 31:271-277
Malik K, Tabiat-Pour S. The use of a diagnostic wax set-up in aesthetic cases involving crown lengthening – a case report. Dent Update. 2010; 37:303-307
Nyman S, Lindhe J, Lundgren D. The role of occlusion for the stability of fixed bridges in patients with reduced periodontal tissue support. J Clin Periodontol. 1975; 2:53-66
Wise MD. Stability of gingival crest after surgery and before anterior crown placement. J Prosthet Dent. 1985; 53:20-23
Kamansky FW, Tempel TR, Post AC. Gingival tissue response to rotary curettage. J Prosthet Dent. 1984; 52:380-383
The coping-retained bridge: a modified approach to conventional bridge design – review and case report Stuart C Campbell Amy L Harper Kenneth H Scott Dental Update 2025 40:8, 606-612.
Authors
Stuart CCampbell
BDS, MFDS RCS(Edin)
General Dental Practitioner, Loanhead Dental Practice, 50 Fountain Place, Midlothian EH20 9DU, UK
Missing teeth may be restored with conventional bridgework. A modified approach to traditional bridge design may be necessary to restore edentulous spaces in the presence of poorly aligned abutment teeth and abutment teeth of guarded prognosis. The coping bridge is a useful technique in the dentist's armamentarium for patients in whom implant-supported or removable prostheses are inappropriate. This paper examines the use of coping-retained bridges as a modification on traditional design and discusses how these appliances may be applied in general practice. A case report is presented describing the application of this design in general practice.
Clinical Relevance: Applying a modified approach to bridge design may allow complicated edentulous spaces to be restored successfully in general practice.
Article
Patients are motivated to seek dental treatment to replace missing teeth. In general practice, conventional bridgework can be used to restore the functional and aesthetic problems created by missing teeth.
The restoring dentist may encounter challenges when fixed bridgework is planned:
Abutments of questionable prognosis;
Poorly aligned abutments;
The need to plan for future modification;
Large edentulous spaces.
Although these challenges may be overcome with orthodontics or implant dentistry, these approaches are not appropriate to all patients and a modified approach to bridge design may be necessary.
Conventional bridge design can be modified by using telescopic copings to retain a fixed bridge. Copings may be described as inner crowns or sleeves which are permanently cemented to prepared abutment teeth. The fixed bridge superstructure is then cemented onto the copings using a weak cement. This allows removal of the bridge should further treatment of the abutment teeth be necessary. This technique was first described in 1886 by Starr,1 and is in common practice in Sweden and Germany.2
Advantages of the coping bridge
Retrievability
Beschnidt et al3 and Wise4 describe retrievability as being the main advantage of the coping bridge. Removal of the bridge superstructure from the copings can permit future modifications of the bridge without the need for a costly remake. In cases where an abutment tooth is of doubtful prognosis, removal of the bridge simplifies endodontic or periodontal treatment of the offending abutment tooth. If multiple abutments with copings have been used, a failed abutment can be extracted and the relevant retainer converted to a pontic by being filled with composite. As long as sufficient abutments remain, the bridge can be recemented without difficulty. For these reasons, Widbom et al5 describe the coping bridge as a favourable alternative in situations where it is not possible to provide conventional or implant-supported appliances.
Alignment problems
Malaligned abutment teeth can complicate the path of insertion of fixed bridgework.4,6,7 Attempting to correct the malalignment of abutment teeth with excessive tooth preparation can compromise the vitality of the pulp and the resistance/retention form of the abutment6,8 (Figure 1). Copings can be made to improve the path of insertion of divergent abutments, allowing the dentist the simpler task of preparing the abutment teeth down their long axis.4,5,7,9
Figure 1. Malaligned abutments of guarded prognosis and horizontal ridge defect.
Correction of undercuts
Copings may be used to remove undercuts in abutment tooth preparation, reducing complications in the manufacture and cementation of the bridge.
Stress relief
Functional and parafunctional loading of a bridge can cause mechanical failures such as porcelain fracture, loss of cementation and abutment fracture. A further advantage of the coping technique is that it provides a stress relief system. The weak cement mixture used to cement the superstructure breaks in areas of heavy loading, leaving the cemented copings in place. The superstructure may then be recemented without difficulty.
Protection of abutments
Copings have been described as offering the abutment tooth protection from caries, chemical and thermal irritation.3,4
Connection of teeth to implants
A bridge may be jointly retained by teeth and implants so that a fixed appliance may be provided. This somewhat controversial design may be considered if the alternative was an unfavourable cantilever design using implants alone.4,10 Teeth may also be connected to implants if it is considered desirable to retain tooth proprioception within the bridge design. Attaching a coping to the tooth in these situations simplifies bridge construction, maintenance, oral hygiene and retrievability.
Patient acceptance
A recent study11 evaluated the impact of coping-retained appliances on the daily life and wellbeing of patients. It was reported that these appliances have a positive effect on patient quality of life, especially in patients with few remaining teeth. They also act to avoid the psychological impact of further tooth loss.
Longevity
Eisenburger et al2 have described the functional life of the appliance and the survival time of the abutment teeth as the two most important factors associated with long-term success of prosthodontic treatment. Based on these criteria, studies2,12 have reported the short-term success rates of appliances retained on two abutments with copings as 95–100% after 2 years and 79–92% after 4 years. The same studies reported long-term success rates of 91% after 7 years and 89.5% after 20.5 years when two canine and two first premolar teeth were used as abutments.
Widbom et al5 reports greater success rates in patients with a higher number of abutment teeth compared with patients with appliances supported by fewer abutment teeth.
Presumably, the higher number of abutment teeth in the appliance will permit greater opportunity for future modifications to the appliance.
Evidence base
Clinical data regarding the long-term success of coping-retained appliances are provided by prospective and retrospective studies.2,5,10
Oral hygiene
The margins of the coping and superstructure are usually placed supra-gingivally. This facilitates oral hygiene measures and contributes to gingival health.13
Disadvantages of the coping bridge
Aesthetic problems
Aesthetic problems are created by the need for the prepared abutments to accommodate both the coping and the superstructure, which can result in the creation of a bulbous metal-ceramic bridge. Further aesthetic compromises result from the coping having a margin milled onto it to which the superstructure fits. As these margins are placed supra-gingivally (Figure 2), both a coping margin and a superstructure margin can be visible.
Figure 2. Supra-gingival position of milled gold alloy copings.
Gingival problems
Over-contoured restorations have been associated with a negative effect on gingival health.14 Bulbous restorations can lead to poor gingival aesthetics secondary to plaque-induced inflammatory changes.
Bridge becomes uncemented
The superstructure is typically fixed to the copings using a weak cement. Wise4 describes the use of a mixture of one part petroleum jelly (Vaseline) from a 2 ml syringe and two parts each of a zinc oxide eugenol base and catalyst (Temp Bond, Kerr). Cementing the bridge in this way permits appliance removal should the treatment of an abutment tooth be required. This may, however, be an unwelcome feature for the patient if the appliance becomes uncemented during normal function.
A recent study5 found loss of cementation was more likely to occur in the maxilla compared with the mandible, presumably due to the effects of gravity and off-axial loading.
Behr et al15 describe this problem as the most frequently occurring maintenance procedure for coping bridges. A further disadvantage for both patient and dentist may be additional surgery time required for re-cementation procedures.
Retention of the superstructure may be augmented by sandblasting the copings with 50 mm alumina.
Suboptimal direction of occlusal forces
Copings may be fabricated to correct malaligned abutment teeth. However, this may result in portions of the coping being cantilevered and unsupported by tooth margin. Where teeth are tilted, occlusal forces may be directed down the long axis of the coping but not the long axis of the tooth. This relationship may lead to the transfer of traumatic forces from the appliance to the tooth.3
High level of technical support
A high level of technical skill is required to manufacture the coping bridge. Widbom et al5 describe the need for a well trained and experienced dental technician for the fabrication of these appliances. Good communication between dentist and technician is another absolute prerequisite.
Cost
Manufacture of a bridge with the additional costs of copings can be expensive. Traditionally, copings are manufactured using high grade gold alloy (Figure 3), although base metal alloys1 titanium16 and zirconium16,17 copings have also been described (Figures 4 and 5).
The dentist decides how many copings will be used to retain the superstructure following a thorough clinical and radiographic examination. As previously discussed, higher success rates are observed for appliances retained by a greater number of copings. The use of two canines and two first premolars has been associated with high survival rates.
The preparation features of teeth for copings have been described in the literature:3,5,9,15
1.2 mm circumferential chamfer margin;
6° taper.
Following tooth preparation and impressions, the laboratory is instructed to fabricate the copings (Figures 6 and 7).
Figure 6. Abutments prepared for copings.Figure 7. Telescopic copings attached to prepared abutment teeth.
The materials that may be used to fabricate copings are:
High grade gold alloys containing >70% by weight gold content (Degunorm, Dentsply) are described as the material of choice2,3,16 but are expensive;
Base alloy is inexpensive but is technically difficult to use;1
Zirconium may be more aesthetically acceptable to some patients and has shown promising retentive properties during in vitro testing.16 A further advantage is the elimination of galvanic current between the coping and superstructure, which may cause thermal irritation to some patients.17
Titanium has been described for use in patients with allergies.5
The copings are manufactured to a minimum thickness of 0.3 mm3,16 with a 2° angulation and a milled chamfer margin. These dimensions are consistent regardless of which material has been used.
The copings are tried-in, and attached to, the abutment teeth using a temporary cement (Temp Bond, Kerr). A master impression is recorded with the copings in place. The impression and copings are sent to the laboratory together with a jaw registration and appliance prescription.
The laboratory is instructed to manufacture the metal-ceramic bridge superstructure in the chosen shade and with the necessary porcelain characteristics (Figure 8).
Figure 8. Bridge superstructure attached onto the copings.
Once received from the laboratory, the copings are permanently cemented. The use of zinc phosphate and glass ionomer cements have been reported2,3,4,15,18,19 for this purpose but self-adhesive resin cements (Rely-X Unicem, 3M ESPE) have recently shown promising results.15
The superstructure is tried in over the copings (Figure 9). The cement used to secure this is prepared according to the recommendations previously discussed.
Figure 9. Four unit superstructure fitted onto copings. Note visible coping margins and use of pink porcelain to mask alveolar defect.
The patient is given oral hygiene advice and appropriate maintenance visits are arranged.
Case report
Patient A is a 77-year-old lady who presented in general practice with functional and aesthetic problems. Her upper denture was in poor repair and she was unable to tolerate her lower denture (Figure 10). She reported that it was painful to chew food and that she was dissatisfied with her appearance. Her medical history revealed well controlled hypertension and previous surgery to remove a benign growth from the right carotid. She was a non-smoker.
Figure 10. Lower denture on presentation.
The lip line at rest and during maximal reveal displayed only the maxillary denture teeth and not the acrylic flange area (Figure 11). The gingival margins of the lower teeth were not displayed.
Figure 11. Patient A on presentation.
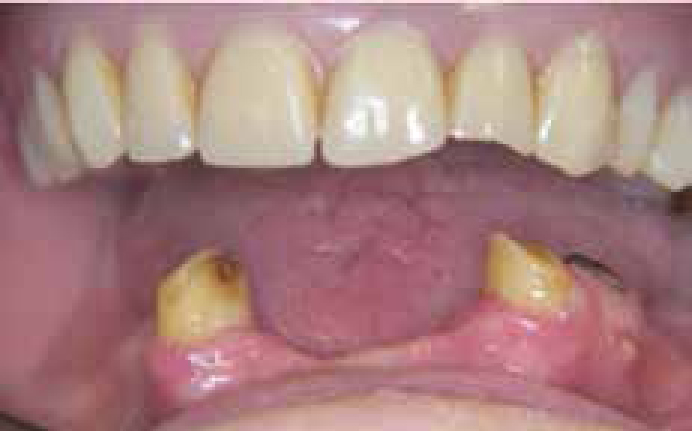
Intra-oral examination revealed a poor complete upper denture which was severely worn. Roots were retained in UR7, UL7 and LL4. Teeth LR3/LL3 were present, but both were compromised by severe tooth surface loss. Caries was noted in LR3 and root surface caries in UL7.
A buccal sinus was noted adjacent to LR4. The periodontal assessment revealed no mobility and no probing depths >4 mm were noted. Attached gingiva and buccal sulcus depth was reduced. Mild alveolar bone loss had resulted secondary to loss of teeth (Figures 12 and 13). Plaque control was satisfactory.
Figure 12. Patient A on presentation – note horizontal ridge defect and reduced attached gingivae.Figure 13. Note mesial caries in lower right canine and buccal sinus associated with lower left first premolar.
A history of sensitivity was reported in unit LR3, though this tooth responded to sensibility testing. Radiographic assessment revealed moderate horizontal bone loss associated with LR3 and periapical radiolucency associated with LL4. Close proximity of the pulp chamber to the most coronal aspect of teeth LR3/LL3 was noted.
The treatment options discussed with the patient were:
No treatment;
Implant-retained prostheses;
Extractions and conventional complete dentures;
Conventional upper denture and lower overdenture;
Conventional upper denture and coping-retained lower overdenture;
Crown lengthening and conventional upper denture and lower coping-retained bridge;
Crown lengthening and conventional upper denture and lower conventional bridge.
The patient considered her current situation unsatisfactory and wished to proceed with treatment. Implants were declined due to cost. Owing to the previous difficulties with a lower denture, the presence of caries in, and history of sensitivity with, LR3 the patient elected to have treatment with a complete denture opposing a coping-retained bridge.
Initial therapy was directed at removal of UL7 and LL4. Oral hygiene and periodontal scaling was carried out.
The clinical heights of LR3/LL3 were augmented with crown lengthening surgery (Figure 14). A lower surgical stent was made to plan the procedure.20
An eight unit canine-to-canine bridge with first premolar cantilever pontics was proposed. This design was based on work carried out by Nyman et al,21 which documented the success of long span bridgework supported by a few isolated abutments.
A review appointment was made 20 weeks following crown lengthening surgery. It has been demonstrated that stability of the gingival crest after surgery occurs at this time.22
Primary maxillary denture impressions were recorded in impression compound using modified metal stock trays. Units LR3/LL3 were prepared for copings (Figure 15) using the guidelines outlined above. A double retraction cord technique3,4,7 was used and impressions were taken in modified stock trays (Figure 16) using polyether (Impregum, 3M ESPE). Master maxillary denture impressions were recorded in zinc oxide eugenol paste (SS White materials, Prima Dental Group) using a special tray.
Figure 15. Preparations for coping retainers.Figure 16. Master impression in modified stock tray.
Copings were manufactured in gold alloy and tried-in. Fit was satisfactory and temporary cement (Tempbond, Kerr) was used to fix the copings to teeth LR3/LL3.
The lower anterior ridge was anaesthetized and a periodontal probe used to measure the distance from the gingival crest to the alveolar ridge. A gingival rotary curettage technique was used to score the ridge7,23 to allow space for fabrication of ovate bridge pontics (Figure 17). Ovate pontics have been shown to reduce bending of the appliance in response to functional loads and create a favourable emergence profile.7. A master impression was recorded in polyether (Impregum) and jaw registration and facebow transfer were recorded. The shade and porcelain characteristics were prescribed to the technician.
Figure 17. Gingival rotary curettage to aid fabrication of ovate pontics.
A visit was arranged for trial assessment of the complete denture which was approved by both the operator and the patient. Caries removal from LR3 was carried out and confirmed using caries indicator dye (Snoop, Pulpdent). The copings were re-tried on the abutment teeth and cemented permanently (Figure 18) using zinc phosphate cement (Heraeus Kulzer Ltd). A resin-based lute may also be used for this purpose and conveys the advantage of having a thinner viscosity, which may reduce problems of incomplete coping seating.
Figure 18. Copings cemented with zinc phosphate.
The bridge framework was tried-in and fit was satisfactory. The casting was returned to the laboratory for porcelain application.
The finished superstructure was received from the laboratory after the application of porcelain. The fit was again verified to ensure no distortion had occurred after porcelain application. The patient was shown and approved the appliance. The superstructure was cemented to the copings using the technique described by Wise4 (Figures 19 and 20). The complete maxillary denture was fitted and bilaterally balanced occlusal contacts were observed (Figure 21).
Figure 19. Bridge superstructure.Figure 20. Bridge and denture fitted.Figure 21. Patient A on completion of treatment.
Discussion
The use of a coping-retained bridge allows the restoring dentist to provide the patient with a fixed solution for the replacement of missing teeth while overcoming the problems of poor abutment tooth alignment and abutment teeth of uncertain prognosis. The technique can allow the dentist to plan for future modifications without the need for costly appliance remakes. Patients for whom dental implants or removable dentures are unsuitable may benefit from this technique.
When planning this procedure, dentists and their patients should be aware of the higher cost of manufacture compared with conventional bridgework due to the need to fabricate copings.
The aesthetic compromise created by the presence of visible coping and bridge margins means that careful evaluation of the lip line and the patient's aesthetic expectations are required. The use of zirconium copings may improve aesthetics in some cases but it should be noted that the appliance may be considered over-contoured compared with a conventional bridge.
The main advantage of these appliances is their retrievability. Removal of the superstructure is afforded by using a weak cement to attach it to the copings. While this allows great flexibility for future treatment planning, both patient and dentist need to be aware that this may contribute to the superstructure becoming uncemented at an inconvenient time.
Coping selection is important for future treatment planning and the use of multiple abutments allows more flexibility in this regard. The use of two canine and two premolar abutments has been recommended as a favourable design.
When prescribed in appropriate cases the coping bridge may provide a long lasting and modifiable solution for the fixed replacement of missing teeth.