Simon JH, Glick DH, Frank AL The relationship of endodontic-periodontic lesions. J Periodontol. 1972; 43:202-208
Al-Fouzan KS A new classification of endodontic-periodontal lesions. Int J Dent. 2014; 2014
Shenoy N, Shenoy A Endo-perio lesions: diagnosis and clinical considerations. Ind J Dent Res. 2010; 21:579-585
Singh P Endo-perio dilemma: a brief review. Dent Res J (Isfahan). 2011; 8:39-47
Fantozzi G, Leuter C, Bernardi S, Nardi GM, Continenza MA Analysis of the root morphology of European anterior teeth. Ital J Anat Embryol. 2013; 118:78-91
Rehman K, Khan FR, Habib S Diaphonization: a recipe to study teeth. J Contemp Dent Pract. 2015; 16:248-251
Aksel H, Serper A A case series associated with different kinds of endo-perio lesions. J Clin Exp Dent. 2014; 6:e91-e95
Lim JH, Lee JH, Shin SJ Diagnosis and treatment of teeth with primary endodontic lesions mimicking periodontal disease: three cases with long-term follow ups. Restor Dent Endod. 2014; 39:56-62
Gutmann JL Prevalence, location, and patency of accessory canals in the furcation region of permanent molars. J Periodontol. 1978; 49:21-26
Kambale S, Aspalli N, Munavalli A, Ajgaonkar N, Babannavar R A sequential approach in treatment of endo-perio lesion a case report. J Clin Diagn Res. 2014; 8:(8)ZD22-ZD24
de Miranda JL, Santana CM, Santana RB Influence of endodontic treatment in the post-surgical healing of human Class II furcation defects. J Periodontol. 2013; 84:51-57
Asgary S, Fazlyab M Management of failed periodontal surgical intervention for a furcal lesion with a nonsurgical endodontic approach. Restor Dent Endod. 2014; 39:115-119
Nirola A, Grover S, Sharma A, Kaur D Pulpal perio relations: interdisciplinary diagnostic approach – I. J Indian Soc Periodontol. 2011; 15:80-82
Di Angelo L, Di Stefano P, Bernardi S, Continenza MA A new computational method for automatic dental measurement: The case of maxillary central incisor. Comput Biol Med. 2016; 70:202-209
The importance of correct diagnosis and treatment in endo-periodontal lesions: a two cases comparison Sara Bernardi Christian Frascarelli Giulia Fantozzi Silvia Caruso Robert Gatto Gianna Maria Nardi Maria Adelaide Continenza Dental Update 2025 43:8, 766-771.
Authors
SaraBernardi
DDS
Molecular and Ulstrastructure Imaging European PhD, Department Of Life, Health and Environmental Sciences, University of L'Aquila, Via Vetoio 2, Coppito 2, 67100, L'Aquila, Italy, (sara.bernardi@graduate.univaq.it)
This paper illustrates two endo-periodontal lesions treated with the same standardized protocols with different prognoses. In the first case, the endodontics and periodontal therapies were performed with clinical and radiological healing of the lesion. In the second case, the tooth had to be extracted because of repeated inflammatory processes. In order to investigate the reasons for failure, the extracted tooth was submitted to clearing process, followed by stereomicroscope observation. It revealed a vertical fracture running along the palatal root, not detectable by radiographic examination. This pathway between pulpal and periodontal tissues determined the negative prognosis of the treatment.
CPD/Clinical Relevance: This report aims to highlight how root vertical fractures may not be readily detectable to the standard bi-dimensional radiograph.
Article
The endo-periodontal lesion results from bacterial infection involving the pulp and the periodontal tissues. According to the most widely used classification, Simon's,1 these lesions are first divided into pulpal and periodontal lesions and further classified into five subcategories:
Primary endodontic lesions;
Primary endodontic lesions with secondary periodontal involvement;
Primary periodontal lesions;
Primary periodontal lesions with secondary endodontic involvement;
True combined lesions.
In 2014, Al-Fouzan2 proposed the following new method of classification, based on primary disease with secondary effects:
Retrograde periodontal disease:
Primary endodontic lesion with drainage through the periodontal ligament;
Primary endodontic lesion with secondary periodontal involvement;
Primary periodontal lesion;
Primary periodontal lesion with secondary endodontic involvement;
Combined endodontic-periodontal lesion;
Iatrogenic periodontal lesions.
In the last category, the author cites the vertical root fractures resulting from trauma, as well as from the ‘cracked tooth syndrome’, and fractures spontaneously occurring on the root surfaces.
However, diagnosing a vertical root fracture by means of common bi-dimensional radiography is not so easy, and its misdiagnosis can be a reason determining the failure of treatment.3,4,5
The aim of this study was to illustrate how the standardized endo-periodontal treatment protocol and the patient's compliance was important in the healing of the teeth tissues with a correct diagnosis.
The successful therapy: Case 1
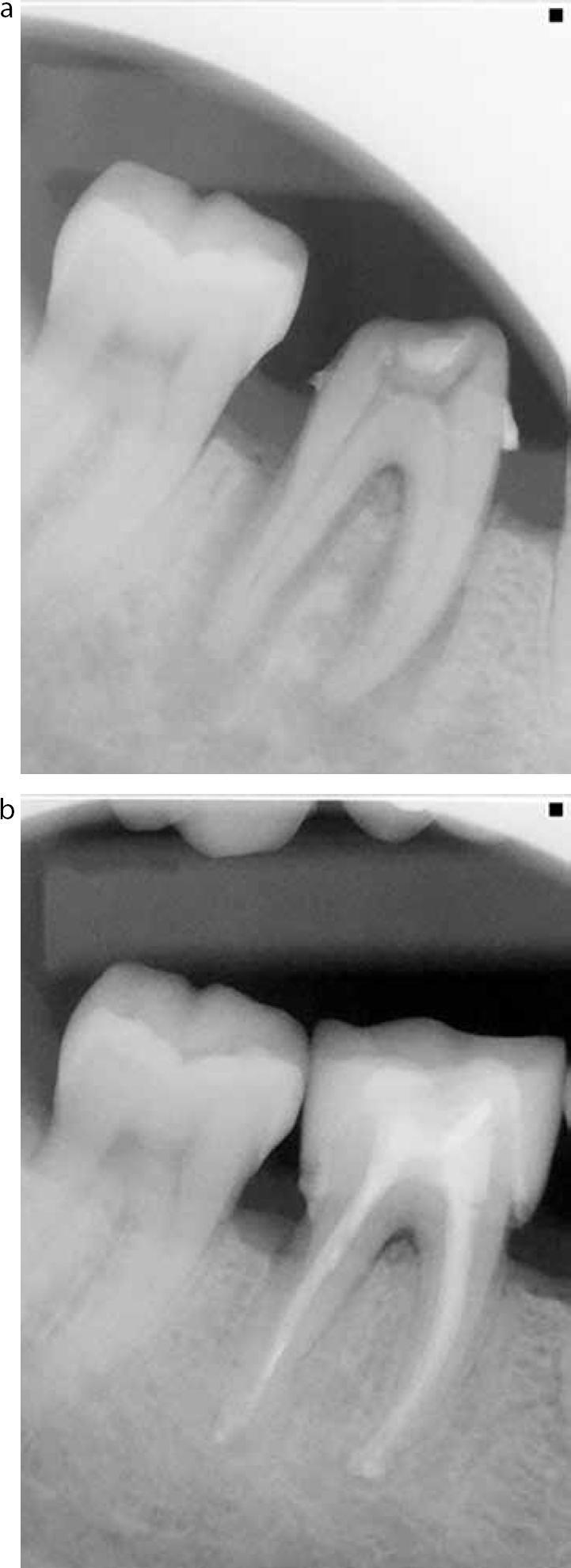
The patient, a 40-year-old male, presented with pain in the right side of the mandibular region during eating. Clinical examination highlighted a 12 mm deep gingival pocket on the disto-oral side at LR6, grade 2 damage at the teeth furcation area, a crown and grade 3 mobility. The tooth was tender to percussion and a vitality test was negative.
An orthopantomograph highlighted the presence of an area of osteolysis around the root apex and the furcation, typically of an endo-periodontal lesion (Figure 1a). The first step of the treatment was endodontic. The treatment protocol was:
Opening of the pulp chamber;
Probing of root canals by manual file instrument 10;
Irrigation with EDTA solution and the working length determined by electronic apex detector;
The root canals treated with nickel/titanium rotating instruments and disinfected with sodium hypochlorite 5.25%;
Finally, the canals sealed with Thermafill system.
Figure 1.
(a) Radiograph of the endo-periodontal situation. (b) Post-treatment situation.
At the 4th month of follow-up, it was possible to note the regression of the lesions:
The pocket probing was 5 mm (from the initial 12 mm);
The furcation damage became grade 1;
The mobility was reduced to grade 1.
After 6 months following the endodontic treatment, the scaling and root planing in each quadrant commenced. The patient was also prescribed chlorhexidine 0.5% gel and chlorhexidine 0.2% mouthrinses for a week.
At the 18th month of follow-up, the tooth had a 3 mm probing distally, no bleeding, no mobility and the furcation was grade 1 (Figure 1b).
The hidden fracture: Case 2
The patient, a 52-year-old male, presented a compromised periodontal situation, especially in the upper jaw. In particular, the clinical exam highlighted a probing pocket of 12 mm, grade 3 damage at the furcation and grade 3 mobility on UR7 (Figure 2a, b). A vitality test was negative.
Figure 2.
(a) Case 2 orthopantomography: (b) endo-oral RX of the injured tooth; (c) tooth after the clearing.
The treatment protocol was the same as applied for Case 1. However, two abscesses occurred in the two years following treatment.
After no obvious healing at the follow-up and due to the presence of the chronic inflammation and infection, the tooth has been extracted.
After the extraction, the tooth was processed to clearing to check if the endodontic treatment was performed adequately. Clearing is one of the oldest methods to investigate the inner anatomy of the tooth and is based on the clearing and the decalcification of the mineralized tissues.6 The protocol included washing with buffer solution, disinfection by Na-hypochlorite for 30 minutes, immersion in nitric acid for 24 hours and storage in methyl-salicylate solution.
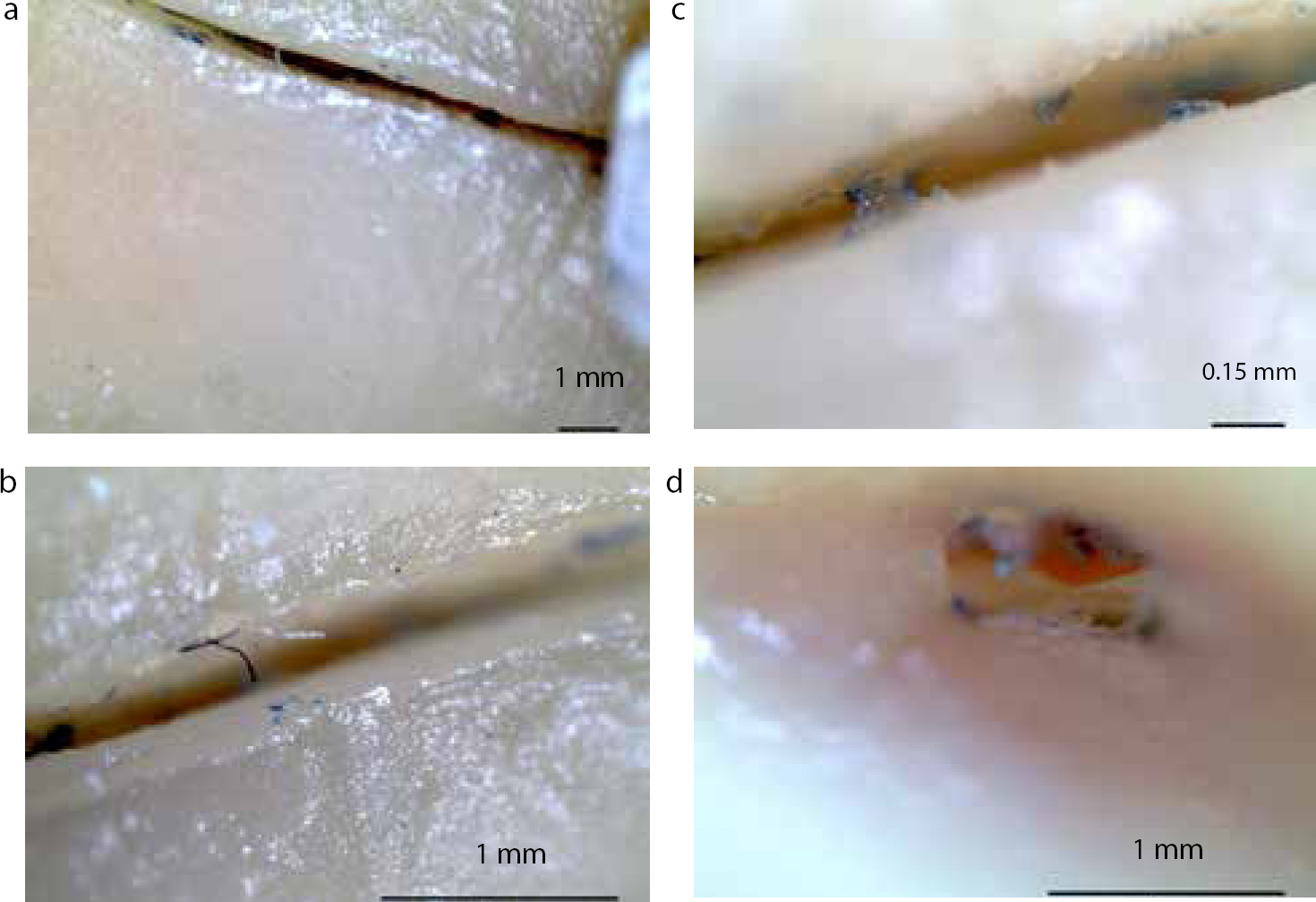
On examination by the naked eye, a dark long line extending from the root to the palatal apex could be seen (Figure 2c). The tooth was also examined by stereomicroscope (Leica LED2000). The investigation clearly showed the vertical fracture, starting directly from the cervical line, that is from the enamel-dentine junction. Also, it has been possible to note a small hole on the distal surface of the palatal apex (Figure 3).
To complete the study, the fracture line was investigated by Image J program, and the reported data were the mean values of measurements taken randomly in 15 points at 1x, 4x and 8x magnification.
The fracture resulted in being 9.8 mm long and to have a mean width of 0.37 mm externally.
Discussion
Endo-periodontal lesions may present a diagnostic challenge.
The first problem is the right approach in the identification of the tissue primarily involved: the operator has to solve this question in order to identify the first area to treat. The diagnosis stage is crucial and the use of vitality testing, which is reported to be quite sensitive,7,8 is compulsory. Furthermore, an infectious process localized in the root canal may frequently result in a chronic inflammatory reaction, involving the nearby periodontal tissue. If there are no signs of periodontal disease on other teeth, and if there is no vertical fracture, healing will occur with endodontic treatment only. In the furcation area, the healing in response to root canal treatments can be associated with the presence of accessory canals, but also to the permeability of dentine and cementum. In this regard, accessory canals can be found in 30–60% of molars' furcation area, exposing this region to communication between pulpal and periodontal tissues.9 Unfortunately, these accessory canals are mostly diagnosed only in the furcation area of mandibular molars.10
When periodontal and pulpal lesions occur at the same time, they are defined as a ‘combined lesion’. This condition therefore requires a combined treatment: if the endodontic treatment is adequate, the prognosis will depend on the severity of the periodontal damage and the efficacy of periodontal treatment will become determinant. If the loss of periodontal tissue is severe and if it cannot be replaced with periodontal regenerative techniques, the extraction of the tooth will be the only therapeutic option.
It was reported that root canal treatment, performed 2.5 months before the periodontal surgery, did not impair the periodontal healing.11 de Miranda et al suggest that endodontic treatment performed 6 months before the surgical debridement of the mandibular molars furcation did not impair the clinical progress of the periodontal tissue healing.12
In the case report, which reported a successful result, root canal treatment was performed 6 months before the periodontal surgery and no disruptive effect on the complete healing of the furcation lesion of the mandibular molar occurred. However, the same protocol applied to a tooth, presenting an undetected communication between the endodontic and periodontal tissues, was not successful.
The combined protocol of the two successful treatments, endodontic and periodontal, can lead to a complete healing of the tissues, but other contributing factors should always be considered to influence endo-perio lesions, such as the artificial pathways between periodontal and pulpal tissues like cracks or fractures. These types of lesions, especially the vertical fracture, decrees the loss of the tooth.3,13,14,15
It appears clear that a good diagnosis, following a good treatment protocol, together with the patient's compliance, are crucial to facing this clinical challenge.