Stephan RM, Miller BF. A quantitative method for evaluating physical and chemical agents which modify production of acids in bacterial plaques on human teeth. J Dent Res. 1943; 22:45-51
Poyser NJ, Briggs PF, Chana HS The evaluation of direct composite restorations for the worn mandibular anterior dentition – clinical performance and patient satisfaction. J Oral Rehabil. 2007; 34:361-376 https://doi.org/10.1111/j.1365-2842.2006.01702.x
Al-Khayatt AS, Ray-Chaudhuri A, Poyser NJ Direct composite restorations for the worn mandibular anterior dentition: a 7-year follow-up of a prospective randomised controlled split-mouth clinical trial. J Oral Rehabil. 2013; 40:389-401 https://doi.org/10.1111/joor.12042
Gulamali AB, Hemmings KW, Tredwin CJ, Petrie A. Survival analysis of composite Dahl restorations provided to manage localised anterior tooth wear (ten year follow-up). Br Dent J. 2011; 211 https://doi.org/10.1038/sj.bdj.2011.683
Bartlett D, Ganss C, Lussi A. Basic Erosive Wear Examination (BEWE): a new scoring system for scientific and clinical needs. Clin Oral Investig. 2008; 12:S65-8 https://doi.org/10.1007/s00784-007-0181-5
Robb ND, Smith BG, Geidrys-Leeper E. The distribution of erosion in the dentitions of patients with eating disorders. Br Dent J. 1995; 178:171-175 https://doi.org/10.1038/sj.bdj.4808695
Kelleher MG. McNamara's Fallacies in Dentistry. 2: Tooth surface loss fallacies. Dent Update. 2021; 48:343-356
Kelleher M. How the General Dental Council and NHS UDAs crushed the compassion out of dentists. Br Dent J. 2022; 232:509-513 https://doi.org/10.1038/s41415-022-4147-4
Milosevic A, Burnside G. The survival of direct composite restorations in the management of severe tooth wear including attrition and erosion: a prospective 8-year study. J Dent. 2016; 44:13-19 https://doi.org/10.1016/j.jdent.2015.10.015
Mehta SB, Lima VP, Bronkhorst EM Clinical performance of direct composite resin restorations in a full mouth rehabilitation for patients with severe tooth wear: 5.5-year results. J Dent. 2021; 112 https://doi.org/10.1016/j.jdent.2021.103743
The ‘satisficing’ additive composite approach to bulimia Martin Kelleher Khawer Ayub Dental Update 2025 50:10, 869-875.
Authors
MartinKelleher
MSc, FDSRCS, FDSRCPS, FCGDent
MSc, FDSRCS, FDSRCPS, FDSRCS, FCGDent, Specialist in Restorative Dentistry and Prosthodontics, Consultant in Restorative Dentistry, King's College Dental Hospital, London
Bulimia (‘ox hunger’) is a serious, potentially dangerous, eating disorder that is often associated with anxiety about weight and body shape. People with bulimia ‘binge’, meaning that they eat large amounts of food, and then vomit afterwards to ‘purge themselves’ in order to get rid of those recently ingested calories. Frequent vomiting of the stomach hydrochloric acid and other ingested acids (pH 1–2) produces variable, but often catastrophic, erosion of the palatal aspects of the upper teeth in particular.
‘Satisficing’ is a word made from combining ‘sufficient’ and ‘satisfactory’. It means seeking an outcome that meets the essential requirements for it to be ‘sufficient to be satisfactory for that situation’.
These authors recommend pragmatic early additive direct resin composite bonding as being a ‘satisficing’ approach to help manage tooth surface loss in bulimic patients, and the article provides clinical examples of some dental problems caused by bulimia being solved in that way.
CPD/Clinical Relevance: This article addresses a number of controversial issues in the dental management of patients with bulimia nervosa (‘bulimia’).
Article
Bulimia nervosa (commonly abbreviated to ‘bulimia’) is a psychological disorder characterized by compulsive overeating followed by vomiting. It has been known about for centuries in different cultures, but in 1979, Gerard Russell, a psychiatrist practising in South London, described it as an ominous variant of anorexia.1
Teeth dissolve below a pH of 5.5.2 During vomiting, the regurgitated stomach contents, which have a pH of about 1–2, due to the hydrochloric acid in the stomach, often mixed with variable recently ingested acidic foods and drinks, passing over the top of the protruded tongue before contacting the palatal aspects of the upper teeth, thereby eroding the upper front teeth primarily. The lower anterior teeth are usually protected by the various protruded movements of the tongue lying on top of them during the violent expulsion of the stomach contents.
Pragmatic direct resin composite bonding is a clinically proven, effective, and efficient approach for managing various problems, including tooth surface loss (TSL).3–5
This article endorses the diagnosing and recording of tooth surface loss and giving appropriate preventive advice to any patients suspected of having bulimia. However, it also advocates a ‘satisficing’ approach (meaning one that is ‘sufficient to be satisfactory’) by undertaking early direct composite bonding of any eroded surfaces seriously damaged by (or at most at risk from) the hydrochloric and other acids. This may be regarded as being a compassionate, practical, protective, preventive and reparative approach.
These authors favour that ‘satisficing’ combined approach, rather than a mainly monitoring one that involves passive ‘measuring’, recording, giving preventive advice and then ‘monitoring’ the TSL (sometimes with fluoride applications). However, as discussed in detail below, we challenge strongly the dogmatic BEWE protocol advice to avoid the use of any restorations (presumably including preventive/reparative resin ones) until a threshold of BEWE 13 is reached.
How does bulimia pose a major problem for teeth?
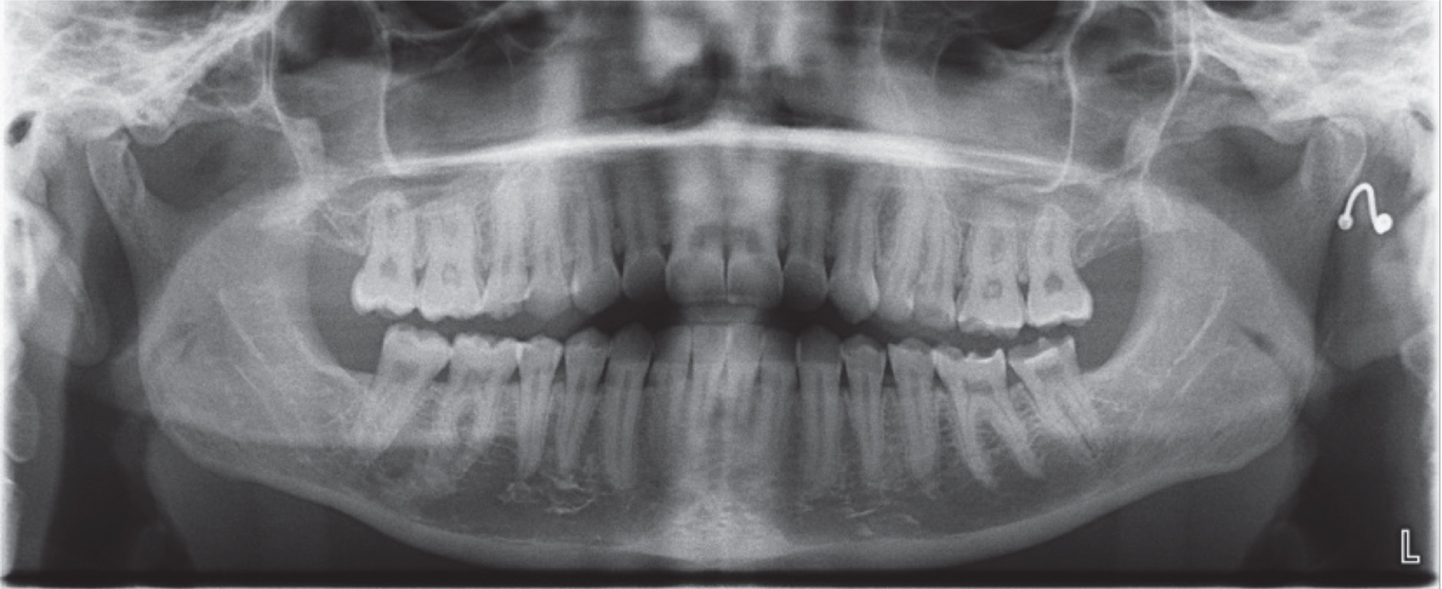
Teeth dissolve below a pH of 5.52 and vomited stomach hydrochloric acid has a pH of 1–2 depending on which foods and drinks were consumed during the ‘bingeing’ phase that precedes the vomiting episodes. That combination of erosive acids passes over the palatal aspects of the upper anterior teeth on their way out of the mouth. If vomiting occurs frequently, it can become catastrophic quickly for the health and the shape of the maxillary incisor teeth in particular (Figure 1). Other teeth can be affected to a variable extent, all depending on a number of factors (Figures 2–4).
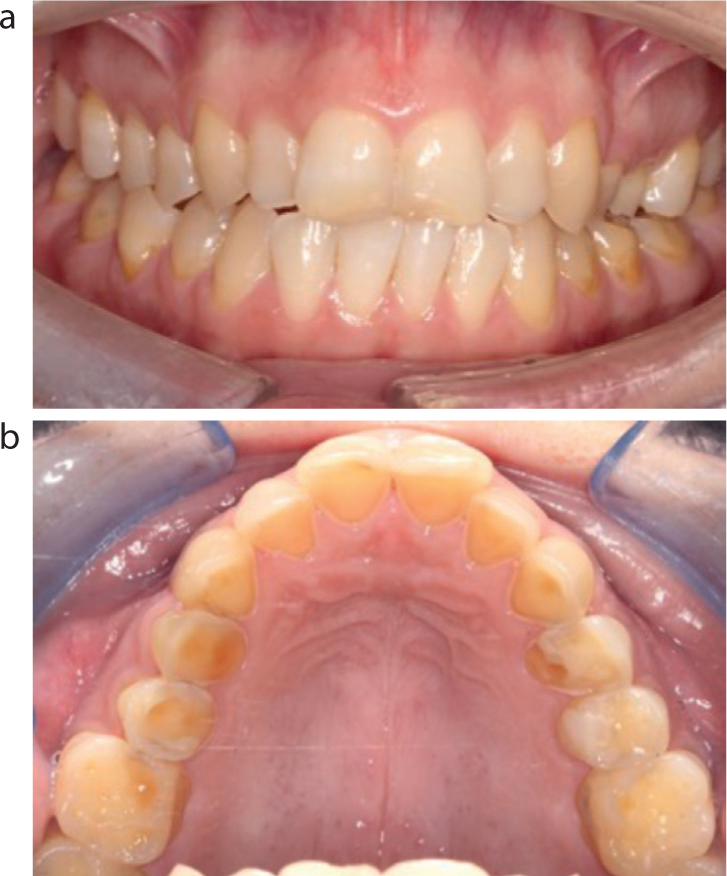
Figure 1. Severe localized erosive tooth surface loss (TSL) of the maxillary incisor teeth in a patient with chronic bulimia. The diagnostic ‘clincher’ that this was almost certainly due to acid, rather than being due to attrition, is that the usually bigger upper front teeth now have a greatly reduced height to width ratio, while the usually smaller mandibular anterior teeth have a more normal ratio. The protruded tongue lies on the lower teeth during the vomiting episodes and thereby protects them from the worst effects of the multiple hydrochloric acid attacks. The heuristic rule (a ‘rule of thumb’) is that ‘if the upper incisors are short relative to their widths, but the lower ones look normal, it means that the TSL problem was due overwhelmingly to acid erosion’. The clinical significance of making that diagnosis early on is profound because it means that any reparative material must only resist acid in the future – rather than attritive forces – and that means direct composite can be used confidently.Figure 2. (a,b) The ‘satisficing ‘purpose of adding resin composite, at an arbitrary vertical dimension, was to protect the bulimic patient's residual ‘dental capital’ (meaning her enamel/dentine/pulps/periodontal health). Apart from making the pragmatic occlusal contacts reasonably even, no real attempt was made to produce idealized occlusal anatomy, or to restore the palatal aspects of the eroded premolar teeth to full contour. Doing so could have placed the direct composite in to shear or tensile stress. Composite is a great material when placed in thick section and bonded primarily over the remaining enamel and when loaded in compression, but it is not good in thin sections, or when subjected to serious shear or tensile stresses or on obliquely exposed dentine. Rapid adaptation to various different (but functional) occlusal contacts is aided by the exquisitely innervated periodontal ligament mechanoreceptors.Figure 3. Chemical erosion caused ‘thinning and greying’ of the incisal edges of this 19-year-old patient who experienced bulimia.Figure 4. Quick diagnostic tip: in erosion cases, the upper anterior teeth shown on an OPT appear to be darker than the lower ones or the back teeth. That is because chemical dissolution of the maxillary teeth ‘thins’ them, so that they now look darker on the OPT than their opposing lower anterior tooth, whose greater remaining tooth structure now offer proportionately more resistance to the passage of the radiographic beam.
When should direct bonding be discussed with suspected bulimic patients?
This is a consent issue that involves discussing the ‘material risks’ for that bulimic patient and giving them neutral, objective, information about what are their BRAN options (meaning Benefits, Risks, Alternatives, Nothing). Assuming that the appropriate diagnosis has been made, and preventive advice has been given, then, if there has been significant breaching of the enamel of the adult upper front teeth, especially in younger people, pragmatic additive direct resin composite bonding should be discussed as being a practical preventive and reparative option, which, in theory at least, is available to them to protect and repair the damage caused by their dentally destructive behaviours.
Why not wait, avoid any restorations and ‘just monitor’?
The primary reason for bonding composite early on to any significantly eroded upper teeth, often at a pragmatically increased anterior vertical dimension, is to protect their reduced, but invaluable ‘dental capital’, meaning their residual sound tooth structure. A secondary benefit, especially when the upper teeth look markedly shortened, thinned, translucent or grey, is that doing so often also provides a psychological benefit for those unfortunate patients who are struggling to overcome their difficult problems, hopefully with effective professional help (Figures 1–7).
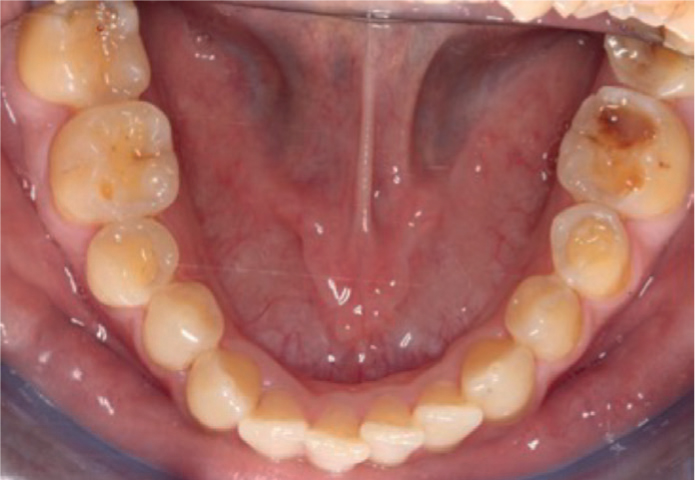
Figure 5. Occlusal view showing erosive tooth surface loss extending into dentine. Because of the protruded tongue positions during vomiting, the hydrochloric acid erodes the palatal surfaces of the upper anterior teeth mainly, and in this case, the occlusal and palatal surfaces of the posterior teeth.Figure 6. (a,b) Severe erosive tooth surface loss affecting all of the upper teeth of this 21-year-old patient with bulimia. Note the ring of intact enamel at the cervical margins (‘the enamel ring of confidence’), which can be used to add direct resin composite predictably to it. That peripheral enamel is nearly always present because the acid is neutralized by the gingival crevicular fluid secreted in those cervical areas. It should be just etched (not bevelled) and the composite should just cover it.Figure 7. The protruded position of the tongue during vomiting usually means it protects the lower anterior teeth, but the acids can spill over on to the back teeth and erode them to variable extents.
Why undertake pragmatic early composite bonding as well as giving preventive advice, rather than ‘measuring’, giving advice and ‘monitoring’?
The additive bonding approach is well proven to deal with a variety of tooth surface loss situations, whatever their causes.3–5 That hands-on approach helps bulimic patients early, before they suffer any further serious tooth surface loss. The main fallacy (meaning the flaw in the reasoning) in advocating the undoubtedly well-intentioned ‘measuring and monitoring’6 approach is that, unlike what happens with caries, the matrix of the enamel and dentine, as well as the calcium and phosphate ions, all disappear in cases of erosive tooth surface loss. That is very unlike what happens with early and moderate caries, where the majority of the tooth's matrix still remains, and consequently there is something left to remineralize. With erosion, any lost matrix is gone, irreversibly and forever, and no amount of wishful thinking, prayer, watching or measuring is going to re-grow it. Ever. In fact, even with early and established caries, effective remineralization will happen predictably only if the patient is compliant consistently with the good advice to reduce drastically their frequency of sugars contacting their teeth and they undertake frequent and effective disruption of their biofilm/plaque. That is ‘a very big ask’ for most sugar addicts. It is due to the uncertainty about any patient's compliance with well-intended advice that many prudent and experienced dentists often fissure seal first permanent molars early on, especially if there has been significant decay in the deciduous dentition.
In the case of tooth surface loss due to chemical erosion (or indeed physical abrasion or attrition, or any combination of those) once that invaluable enamel matrix is lost it is not coming back (Figures 1 and 5) and compliance with prevention certainly cannot be guaranteed in bulimics. Consequently, spending valuable clinical time, repeatedly ‘measuring’ and recording using a questionably reproducible index, or making dubiously accurate sequential plaster study casts, or taking multiple dated photographs, or even employing sophisticated scanning of worn teeth, will not re-grow any more missing tooth structure.
Or, as Irish farmers say, ‘weighing the pig won't fatten it’.
It is possible that the monitoring approach of avoiding any restorations might make some very limited sense, but only if the ‘restorations’ that are advised to be avoided refer to those requiring extensive, further dentally destructive preparations for (presumably) indirect crowns to be used.6,7
Preventive advice and bonding versus advice and ‘measuring and monitoring’
Detailed preventive advice about severely limiting erosive acids in the future is to be encouraged enthusiastically and persistently in any patient with erosive tooth surface loss. However well-intentioned such good advice might be, or how persuasively or consistently it is delivered, bulimic patients are not, sadly, in control of their auto-destructive habits at that time. It is a fallacy that just advising someone with any psychological or addictive behaviour problem ‘just to stop it’, or to do something that would be useful for their health, or their appearance, will result automatically in compliance with that altruistic advice.
The widespread evidence that good information transference does not mean guaranteed compliance with it can be witnessed by ongoing widespread obesity, or addiction to cigarettes, or to various other substances. It was Oscar Wilde who quipped that ‘The only thing to do with good advice is to pass it on – it is no good for oneself’. These rather less witty authors contend that in the case of bulimic patients, that the evidence for long-term outcomes of frequent ‘measuring and monitoring’, to be possibly followed by multiple full crowns are unproven and lacking in compassion, as well as being time-consuming, expensive and inefficient. That is because of the practical problems of the clinical time involved, reliability or reproducibility of indices used for measurements, storage of plaster casts, or availability or reproducibility of photographs or scans.
Those multiple practical problems mean that the approach is of very limited utility for busy dental professionals, or for bulimic patients (or indeed for many others with significant erosive TSL). In truth, the whole measuring approach is, sadly, just another manifestation of ‘McNamara's fallacy’. A ‘McNamara fallacy’ means that it is an error in reasoning ‘to make important something that one can measure, rather than measuring the really important things’.8
In cases of significant bulimia, the really important dental question to answer is ‘what happens to those obviously eroded upper front teeth in the long term if no protective bonding treatment is provided?’ Figure 1 illustrates the devastating dental destruction that stomach hydrochloric acid can do to unprotected teeth. Figures 4–7 illustrate significant damage in a 21-year-old bulimic patient that was treated with a pragmatic ‘satisficing approach’ (meaning one that was ‘sufficient to be satisfactory’) by using gentle bleaching and freehand direct composite bonding, without articulated models or laboratory-made matrices (Figure 8).
Figure 8. The patient had gentle dental bleaching done every third day for 2 hours using 10% carbamide peroxide to avoid excessive sensitivity. Once she was happy with the colour, the additive direct resin composite bonding was done freehand in one session, using a three-bottle bonding system and without using any laboratory wax-up or matrices.
The patient adapted rapidly to the arbitrary change in her anterior occlusion. That was probably because of two important things:
She liked the nicer appearance of her smile that she had been ‘under-promised’ by the trial composite ‘mock-up’ (Figure 10);
She had been warned in advance (and she had already accepted in writing) that her adaptation was an essential requirement if she wanted to keep her remaining ‘dental capital’.
Figure 9. (a) A patient with chronic bulimia with the maxillary anterior teeth severely eroded. (b) She was treated with additive pragmatic composite bonding from her first premolar to first premolar in one session, using a three-bottle system, without mounted diagnostic models or a laboratory wax-up or matrices.Figure 10. A free-hand direct composite mock up placed on dried enamel was completed in a few minutes to improve the proportions and aesthetics of the anterior teeth. This allowed the patient to visualize a possible outcome of treatment and was photographed as part of the consent process. Subtle changes can be made to the final shape and shade following discussion with the patient. The mock-up completed above was part of treatment for the case shown in Figure 6
History of indices for describing tooth surface loss and issues with them
The Basic Erosive Wear Examination (BEWE) is a recognized screening tool that was introduced in 2008.6 The BEWE scoring is based on the amount of tooth structure missing. There are four categories involved, with the structure missing being scored as none (BEWE 0, meaning enamel is intact), a little enamel loss (BEWE 1), or less than 50% of the crown of the tooth missing (BEWE 2) or more than 50% of its structure being missing (BEWE 3) (Table 1). A screening score is awarded to each sextant, based on the most eroded/worn tooth in that sextant scoring as per Table 1. The teeth with highest score in each sextant are then added to give a full mouth score. That total score can then be used to record the extent of erosion/wear in that mouth and to, supposedly, guide the proposed management strategy.
Table 1. BEWE scores.
0
No tooth surface loss
1
Loss of the enamel characteristics
2
Loss of up to 50% of the tooth structure
3
Loss of more than 50% of the structure of the worst affected teeth
The BEWE has some value in highlighting the importance of recognizing and recording the greatly increased problems of TSL for individual patients, for society at large and for the dental profession. However, BEWE is one of many tooth surface loss indices, none of which have found widespread adoption by most general dental practitioners.
In fact, the 2008 BEWE classification6 is just a variation of the 1979 Eccles' Tooth Surface Loss scoring system. Eccles (who was from Northern Ireland and a Professor at Cardiff) suggested a classification for tooth surface loss being recorded as zero (0), a little (1) or less than one-third (2), or more than one-third (3) of the tooth structure being missing. The Eccles 3 category of severity had further subsections termed 3a, 3b, 3c, 3d which were to be recorded depending on increasing severity.9
However, just 5 years later, that Eccles classification was modified slightly for the proposed Smith and Knight Tooth Wear Index (‘TWI’).10 That categorized tooth wear as being none, TWI 0, or TWI 1, meaning minimal enamel loss, or TWI 2, meaning less than one-third of the tooth structure was missing. TWI 3 meant that more than one-third of the tooth structure was missing, while TWI 4 meant that one could see where the pulp was, or used to be.
In summary, the only practical difference from the Eccles classification was that the Smith and Knight TWI 4 proposed replacing the Eccles classification of Eccles 3a–d with a single figure of Smith and Knight TWI 4.
The indices mentioned above are reasonably well known within the UK, but there are many other indices across the globe that aim to measure TSL. Generally speaking, there is little agreement about the reproducibility, or clinical usefulness, of the different tooth surface loss indices.11 The majority of indices cannot measure the rate of tooth wear reproducibly and accurately, and it is arguable how useful they are practically, or whether any index is sensitive enough to monitor subtle changes until it has progressed to its much greater severity.11
Other issues with using tooth wear indices include that they do not take into account the variability or synergy of the possible causative factors, the veracity of the patient's history that they give, the patient's age, their symptoms, the rate of deterioration, or the psychological impact of the changes in their tooth surface shapes might be having on them. While every patient should be treated as an individual with tailored preventive advice being given, there should also be open and frank discussions about the risks and benefits of just monitoring their TSL as opposed to providing early protective, reparative, non-destructive additive bonding because there are serious issues around validity of consent.
Controversies about monitoring and ‘avoiding restorations’ for bulimics
Many experienced pragmatic clinicians, who have been treating many bulimic and other patients with extensive TSL at a young age, question the BEWE dogma of ‘avoiding any restorations’ until the TSL in all sextants is about 50%.
Many clinicians are concerned that the NHS UDA system, in which the majority of dentists within England work, tacitly supports a hands-off, monitoring philosophy that does very little to help the practical dental problems in many bulimic patients, and it also fails to address the wider long-term issues being stored up by the well-reported TSL becoming much worse in younger people – a problem that has been known about for over 25 years in the UK.12
Unfortunately, fear of the GDC regulators and/or no-win no-fee opportunistic lawyers and the multiply flawed NHS UDA system have crushed the compassion out of many dentists and discouraged many NHS GDPs from attempting to help patients, such as bulimics, with extensive tooth surface loss by employing ‘satisficing’ direct freehand composite bonding.13
The pragmatic ‘bondodontists’ argument is that additive (i.e. non-destructive) resin composite bonding, when placed at an appropriate anterior vertical dimension, is now well-proven clinically to give satisfactory medium-term results for many wear and other dental problems.3–5,14,15 The current authors assert that additive bonding of direct resin to eroded teeth in bulimics is just as much a preventive approach as ‘measuring, advising and monitoring’ and that it is more compassionate, more predictable and a more time and cost-effective use of scarce clinical resources. The ‘bondodontist's’ offer to bulimic patients is that they could get ‘self-preservation’ with some modest ‘self-improvement’ while simultaneously avoiding ‘self-destruction’. It ought to be stressed, in advance (preferably in writing) that any direct bonding will not be perfect or permanent, but it should ‘satisfice’ for them, and that it can be polished, repaired, modified or replaced in the future, as required.
In marked contrast, of ‘advise/monitor/and avoid any restorations until BEWE 14 or above’, when applied to bulimic patients, means that any reparative and preventive bonding restorations ought to be avoided. As discussed earlier, the mandibular teeth are usually spared from the worst effects of the vomiting because of the tongue positions and consequently not likely to score even 2 in all three lower sextants. It is usually only the palatal and incisal surfaces of the maxillary anterior teeth that will usually score a high ‘BEWE’ number. As an example of the problem, a score of BEWE 3 is shown in the upper anterior sextant in Figure 1, but only BEWE 1 in the lower arch sextents and upper posterior sextants, with an overall score of about BEWE 8. Consequently, most bulimic cases would fall well below the threshold of BEWE 13 and consequently, the BEWE management strategy would still be to avoid any restorations, presumably including any of the protective, preventive and reparative composite bonding ones such as shown in Figures 8 and 9b.
If interested dental practitioners were to be given enough time and resources, many might wish, and be well able to stop serious problems developing in any patients with significant TSL by using preventive and reparative bonded restorations, such as for bulimics. Such a ‘satisficing’ approach would maintain their already compromised dental capital, as well as helping with their body image and confidence issues while, hopefully, they are getting effective help to overcome their unfortunate psychological issues.
How does pragmatic additive composite bonding actually work in bulimics?
This clinically proven approach involves taking advantage of the patient's ability to adapt to the desired occlusal and other changes.3–6,14,15 That adaptation is programmed by the sophisticated periodontal ligament mechanoreceptors around their teeth and other feedback mechanisms around the face. The ability of most patients to adapt to major changes in their occlusion has been virtually unchallenged in certain fields of dentistry. However, in operative dentistry, the ability to adapt to intended occlusal changes involving a planned increased vertical dimension was described, in England, by Declan Anderson as long ago as 1962.16 That was 13 years before the Norwegian Bjorn Dahl published his work on 20 patients with a device to create anterior space to limit the further dental damage that he did subsequently with his modified pin ledges to repair those worn teeth.17
Validity of consent issues
If the upper anterior teeth are shorter than their widths (e.g. Figures 1 and 2), and if the appearance is unacceptable to that bulimic patient, then sculpting composite on to their dried (NOT etched) visible upper incisor teeth to make them longer than their widths and while making the incisal tips parallel to their interpupillary line, often helps a bulimic patient to visualize, assess and comment on some possible changes in their dental appearance (Figure 10). Once sculpted and cured into position, it is essential to watch the patient's eyes to see their immediate reaction to that reversible direct composite mock-up when they first look in the mirror, and to be wary of any patient who appears ‘underwhelmed’. Because one is dealing with their subjective views about their appearance, it is much more sensible to under-promise and over-deliver, than risk doing things the other way around (Figure 10). However, if those proposed changes, possibly with some minor modifications, appear to the patient to be sufficient and satisfactory for their situation (i.e. to ‘satisfice’), then that unpolished mock-up can be photographed on their phone as an agreed probable aesthetic outcome. The cured composite can then be flicked off without damaging any teeth. Detailed discussions can be undertaken with that patient about any concerns, such as composite longevity, short-term speech issues (mainly when pronouncing the letters S and F and V for a few days), possible discomfort and expected adaptation time. Those aspects need to be balanced against their ‘self-preservation’, meaning that bonding will protect their important load-bearing marginal ridges and the rest of their eroded, but often reasonably sound tooth structure for many years.3–5,14,15
It needs to be emphasized that such a potentially ‘satisficing’ approach is neither ‘permanent’ nor ‘perfect’ (because nothing in life or dentistry ever is) and that the restoration(s) will need to be re-surfaced and/or re-done at some stage, at their expense, depending on their habits. However, their own remaining tooth structure will remain underneath, which is very unlike what happens with full coverage crowns where up to two-thirds is removed for the crown preparations.18
Caution is advised if the patient appears disappointed with a ‘reasonably decent’ mock-up. A gentle comment such as ‘sadly, I don't think that I am the person that you deserve to help you with your particular problem’ allows one to exit gracefully (and, ideally, not charging them for the few minutes involved doing that quick mock-up).
Summary
A ‘satisficing approach’ means doing sufficient treatment for it to be satisfactory for most bulimic patients. It uses pragmatic, additive direct resin composite bonding at an appropriate anterior vertical dimension. That philosophical approach is based on preserving that patient's remaining ‘dental capital’, while simultaneously producing some modest aesthetic improvement during that very difficult phase for them while they are trying to overcome their psychological problems, hopefully with appropriate and effective professional help.
Temporarily sticking direct composite freehand on to their dried maxillary anterior teeth to change their lengths and shapes allows one to assess the patient's reaction to those proposed changes quickly, and in a reversible way (Figure 10). Based on that patient's initial non-verbal reactions and verbal feedback, one can easily modify the composite colour, lengths and shapes in order to ‘satisfice’ for that patient.
Changing anterior vertical dimension is accomplished by using a combination of mutually opposing largely intact teeth, and is not normally a problem, provided that the patient likes the improvement in their appearance and they have accepted, in writing, that their adaptation to the agreed changes is the price that they will have to pay for an improved appearance while keeping their residual dental capital.
That said, the clever mechanoreceptors in the periodontal ligaments usually help most patients to adapt quite quickly to produce a functional new occlusion.
From a psychological perspective, most bulimic patients are grateful for having their most important visible teeth improved and protected by a material that is highly resistant to hydrochloric acid and are reassured by that fact (Figures 8 and 9b).
That ‘satisficing’ approach is smarter in all sorts of ways than unquestioningly adopting the ‘diagnosing, measuring and hoping approach’, which risks allowing ongoing further destruction including, possibly that required for eventual full crowns.18
Most bulimics are content enough with a modest aesthetic improvement provided that they know what to expect in advance and that they like their new smile appearance. The majority seem grateful to be able to get those benefits while maintaining their dental capital with a relatively affordable, largely pain-free non-destructive approach that is neither perfect, nor permanent, but is likely to ‘satisfice’ for them (Figures 6 and 8, and Figures 1, 2 and 9b).