Aquilino SA, Caplan DJ. Relationship between crown placement and the survival of endodontically treated teeth. J Prosthet Dent. 2002; 87:256-263 https://doi.org/10.1067/mpr.2002.122014
Poyato-Ferrera M, Segura-Egea JJ, Bullón-Fernández P. Comparison of modified Bass technique with normal toothbrushing practices for efficacy in supragingival plaque removal. Int J Dent Hyg. 2003; 1:110-114 https://doi.org/10.1034/j.1601-5037.2003.00018.x
Stephan R, Miller B. A quantitative method for evaluating physical and chemical agents which modify production of acids in bacterial plaques on human teeth. J Dent Res. 1943; 22:45-51
Jonasson G, Skoglund I, Rythén M. The rise and fall of the alveolar process: dependency of teeth and metabolic aspects. Arch Oral Biol. 2018; 96:195-200 https://doi.org/10.1016/j.archoralbio.2018.09.016
Coleman F. Types of difficult extraction and their treatment. Proc R Soc Med. 1922; 15:(Odontol Sect)76-82
Van der Weijden F, Dell'Acqua F, Slot DE. Alveolar bone dimensional changes of post-extraction sockets in humans: a systematic review. J Clin Periodontol. 2009; 36:1048-1058 https://doi.org/10.1111/j.1600-051X.2009.01482.x
Machiulskiene V, Nyvad B, Baelum V. A comparison of clinical and radiographic caries diagnoses in posterior teeth of 12-year-old Lithuanian children. Caries Res. 1999; 33:340-348 https://doi.org/10.1159/000016532
Schmidlin K, Schnell N, Steiner S Complication and failure rates in patients treated for chronic periodontitis and restored with single crowns on teeth and/or implants. Clin Oral Implants Res. 2010; 21:550-557 https://doi.org/10.1111/j.1600-0501.2009.01907.x
Treatment planning for a patient requiring multiple restorative treatment modalities by a recently qualified dentist Noor Al-Helou Ammar Ahmed Zaki Dental Update 2025 49:11, 927-932.
Authors
NoorAl-Helou
BDS (Hons), MFDS RCS Ed
Dental Core Trainee, Liverpool University Dental Hospital
This article presents a case demonstrating the treatment of a patient using multiple restorative modalities, including endodontics, indirect restorations and prosthetics. The patient's oral condition resulted from a high cariogenic diet, particularly a destructive carbonated drink habit. This case discusses the treatment options for each diagnosis and the rationale behind the final treatment plan. There was a considerable focus on prevention and restoration of teeth in order to achieve optimal oral health and function, as this was the patient's expressed priority.
CPD/Clinical Relevance: Patients with high cariogenic diets present with varying restorative needs within general practice, and this report demonstrates the treatment of a simple case.
Article
TC was a 31-year-old male who presented as a new patient to the practice after a recent relocation. His complaints included some broken-down teeth that were sharp, as well as gaps between his teeth, which were affecting his self-esteem. He was a regular attender at his previous practice where he had a wide variety of treatment including direct restorations, extractions, root canal treatment and the placement of crowns on multiple teeth. TC was not experiencing any dental pain and had no anxieties relating to dental treatment.
He reported brushing once daily in the morning with a 1450ppm fluoride toothpaste using a manual toothbrush. He did not use any interdental products, but did report using a fluoride mouthwash regularly. He also reported having a high-sugar diet with more than four sugar attacks daily. His main issue was the regular consumption of carbonated drinks.
Social and medical history
TC was a non-smoker and had never smoked and he drank no alcohol. He worked as a civil engineer and enjoyed spending time with his family in his spare time. He was fit and well, had no medical conditions took no regular medication and had no allergies.
Examinations
On extra-oral examination, TC had a skeletal Class I with an average smile line. TC had competent lips and there was no facial asymmetry present. On examination of lymph nodes, TMJ and the muscles of mastication, no abnormalities were noted.
Intra-orally, the floor of mouth, tongue, buccal mucosa and sulcus, palate and labial mucosa were assessed, and no abnormalities were noted.
Dental charts including teeth and periodontal tissues
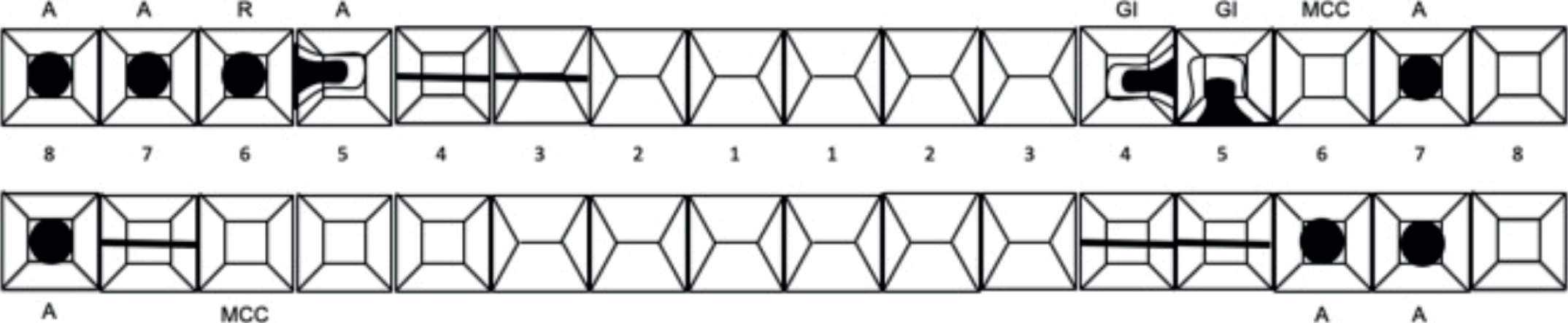
Figure 1 shows the patient's dental chart. On examination, his periodontal tissue was red with generalized inflammation present. His BPE was:
TC's incisal relationship was a Class I with a slight centreline shift to the right. He also had group function on both sides.
Clinical imaging
Patient provided consent to allow their photographs to be held in their records, used for case discussion and also for publication, teaching and use in journals (Figures 2–7).
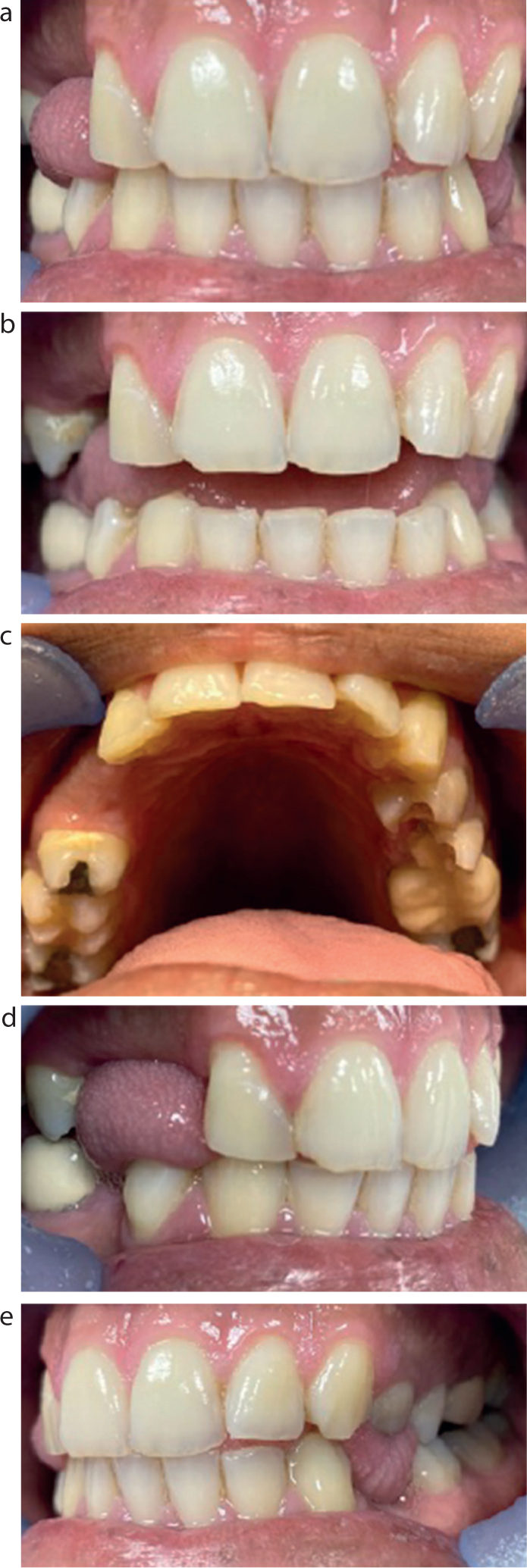
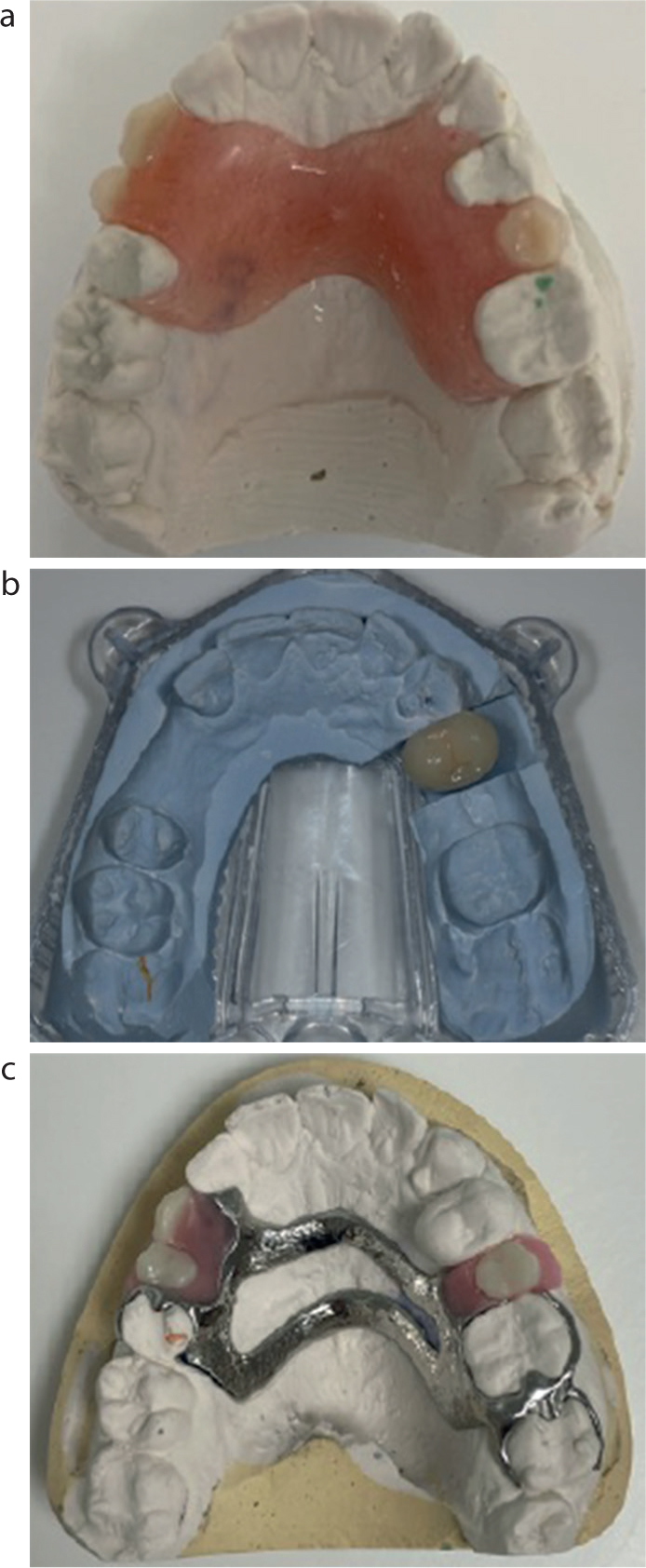
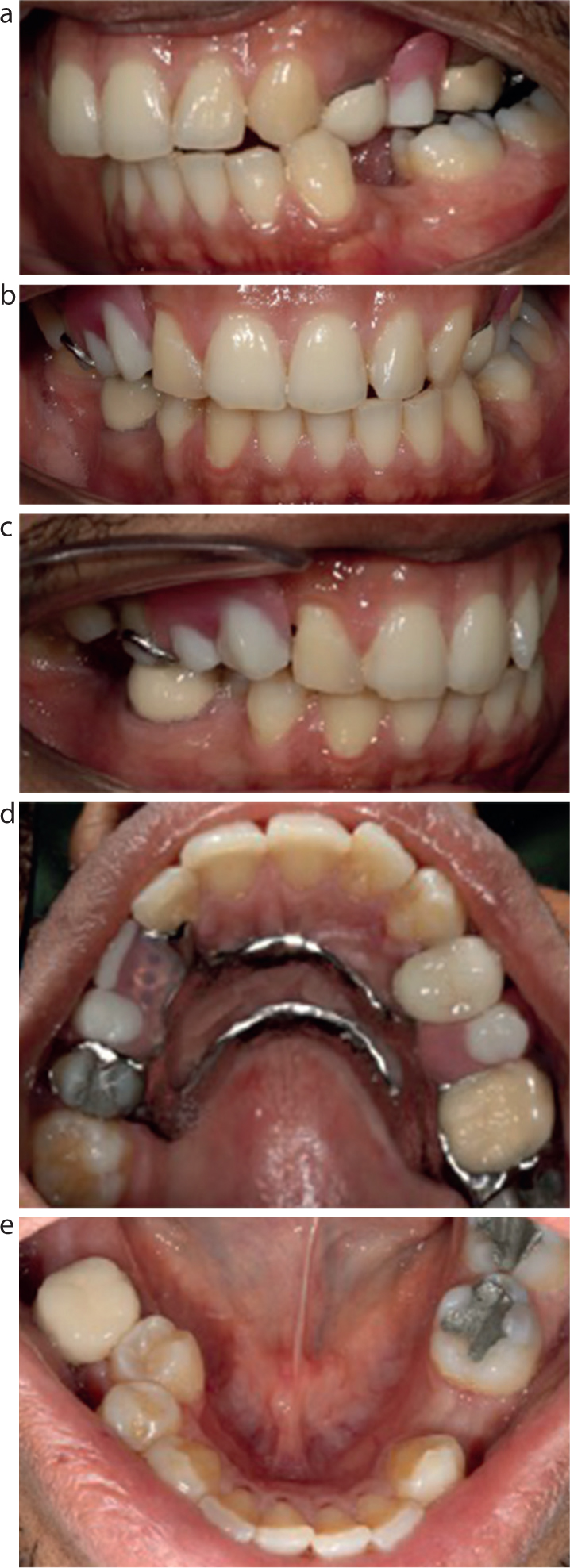
Figure 2. Pre-operative photographs. (a) Front view in occlusion. (b) Front view with 0.5-cm opening. (c) Upper arch, occlusal view. (d) Right view in occlusion. (e) Left view in occlusion.Figure 3. Photographs of laboratory stages. (a) Immediate denture. (b) MCC UL4. (c) CoCr denture.Figure 4. Photographs taken after UL4 crown cementation. (a) Left view in occlusion. (b) Front view in occlusion. (c) Right view in occlusion. (d) Upper arch occlusal view. (e) Lower arch occlusal view.Figure 5. Photographs after fitting the upper partial CoCr denture. (a) Left view in occlusion. (b) Front view in occlusion. (c) Right view in occlusion. (d) Upper arch occlusal view. (e) Lower arch occlusal view.Figure 6.
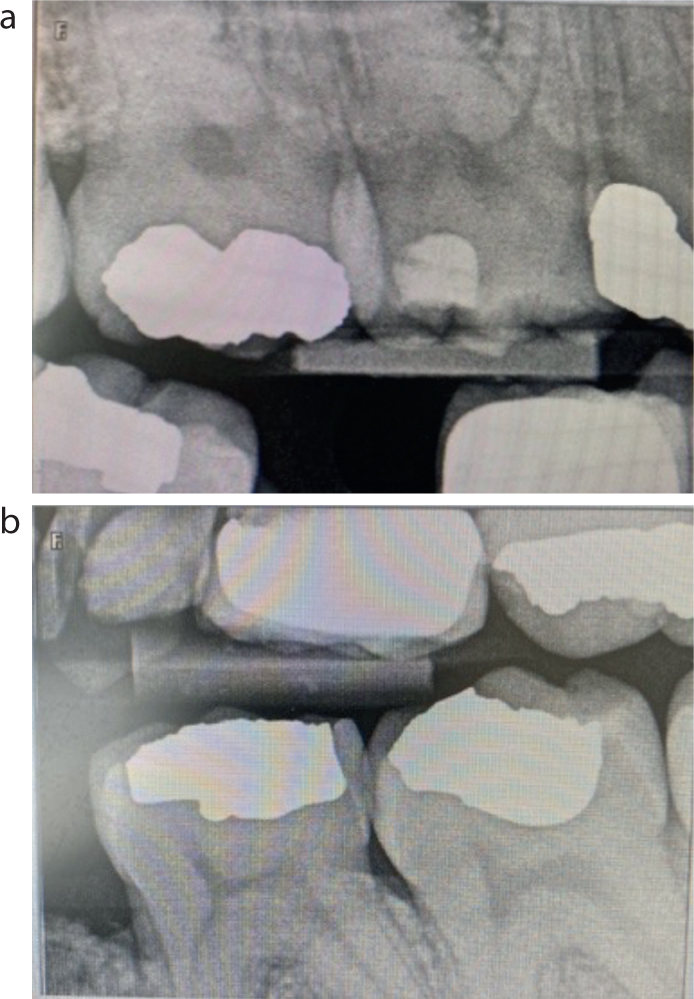
(a) Right and (b) left bitewings. Justification: For the assessment of interproximal caries and bone levels; NRPB: Grade 2; (a) overlapping contacts and film size, (b) film size, therefore 4–7 cannot be seen. Findings: radiolucency consistent with secondary caries UR5. Radiopacity consistent with restorations as charted and all restorations sound. Crestal bone loss only.Figure 7. Peri-apicals of UL4. (a) At the start of treatment; (b) mid-treatment; and (c) at the end of treatment. Justifications: (a) Working length radiograph (inconsistent readings with apex locator); (b) To assess location of master cones (c) Post obturation radiograph for UL4 NRPB: (a) Grade 1; (b,c) Grade 2 (angulation). Findings: (a) Files placed are going all the way to the radiographic apex. Bone level reduction crestal bone only. Radiopacity consistent with restoration; (b) Master cone is between 0 and 2 mm from the radiographic apex. Bone level reduction of crestal bone; (c) No large voids and GP within 2 mm of apex. Bone level reduction of crestal bone only. Radiopacity consistent with restoration.
Diagnoses and risk assessment
Table 1 details the diagnoses, while Table 2 outlines the results of the risk assessment.
Periodontal
Generalized plaque-induced gingivitis
Toothwear
UR21, UL12, LL123 and LR123. BEWE indices used to assess extent of toothwear and patient assigned as BEWE 1
Caries
Secondary caries disto-occlusally on UR5, grossly carious UL5
Peri-apical periodontitis
UL4
Caries risk
High due to evidence of active caries and previous restorations
Periodontal risk
Moderate due presence of calculus and generalized gingival inflammation
Cancer risk
Low due to patient being teetotal and non smoker
Tooth surface loss risk
Moderate due to tooth wear being present on upper and lower anterior teeth
Prognoses
With regards to periodontal health of all existing teeth, the patient had a good prognosis, which would be improved with good oral hygiene instruction, dietary advice and scaling in areas where needed. With regard to the tooth wear in the anterior region, the patient reported that this was from a previous nail-biting habit, which he had stopped. Therefore, with appropriate monitoring, this had a good prognosis.
The UR5 had a questionable prognosis because there was already a large disto-occlusal restoration that now had secondary caries. The patient was advised that good oral hygiene was needed, including the use of interdental brushes in order to improve prognosis. The UL4 had a guarded prognosis because it required both root canal treatment and a crown, for which the risk of failure was higher.1 The UL5 had a hopeless prognosis because, clinically, the caries was subcrestal.
Treatment planning
A range of treatment planning options were considered and are detailed in Table 3. Treatment was decided, and the preferred options are given in Table 4.
UL4
RCT with crown (MCC, ACC, FMC)RCT and direct restorationXLA +/- immediate denture. Long-term options: denture or implantReview and monitor
UR5
Direct restorationCrown (MCC, ACC, FMC)Review and monitor
UL5
XLA +/- immediate denture. Long term options: denture or implantXLA and accept spaceReview and monitor
Toothwear on upper and lower incisors
Direct restoration after OH satisfactoryIndirect restoration after OH satisfactoryReview and monitor
Missing teeth UR34 and UL5 (if patient opted for extraction)*
Acrylic dentureCoCr dentureImplants
*A bridge was not appriopriate owing to the long span and unsuitable abutment teeth.
MCC: metal–ceramic crown; ACC: all-ceramic crown; FMC: full metal crown; OH: oral hygiene; XLA: extraction under local anaesthetic.
Prevention
Oral hygiene instruction including toothbrushing instruction and interdental cleaning adviceDietary adviceAppropriate NSPT in order to address BPEs
Routine conservation
Direct amalgam restoration UR5: amalgam chosen over composite owing to potential issues with moisture control as distal margin was subgingivalExtraction under local anaesthetic of UL5 and provision of upper immediate denture to replace UR34 and UL5
Review of periodontal condition
Advanced conservation
Root canal treatment of the UL4 and provision of a metal ceramic crown
Review
Monitor UR5 clinically and radiographicallyRight and left bitewing radiographs in 6 months as the patient was of high caries risk status
Replacement of immediate upper partial denture with CoCr partial denture
Discussion
TC was a patient who had a variety of restorative treatment needs. These included periodontal support therapy,2,3 direct and indirect restorations and the replacement of multiple missing teeth. This case was particularly challenging because the patient was only 31 years of age and had high expectations for the treatment outcomes. It is important to discuss the likely outcomes prior to commencing treatment to help manage the patient's expectations and ensure they understand all the options available to them.
It was essential to address TC's oral hygiene regimen for the management of his periodontal condition. He admitted to only brushing once daily in the morning, and was therefore advised to brush twice daily for 2 minutes with a 1450ppm sodium fluoride toothpaste.4 TC was also shown the modified Bass technique for brushing.5 This was not demonstrated on a model, but rather in the patient's own mouth because this has been shown to allow for better learning of the technique.5
The patient's dietary habits were addressed at this stage too because he had multiple restorations and active caries present. TC was advised to reduce daily sugar attacks to four, to reduce the number of times the teeth underwent demineralization.6 This would be mainly addressed by TC combating his carbonated drink habit, which he seemed committed to dealing with throughout his visits. Supra- and subgingival debridement was also carried out to remove calculus deposits to allow the patient better ability to carry out their oral hygiene regimen effectively.
The unrestorable UL5 was then addressed, along with the provision of the upper partial immediate denture replacing the UL5 and UR34 (Figure 3a). This was because the patient's primary concern was his tooth spaces, which made him feel self-conscious when he smiled and it was best to ensure this concern was addressed as soon as possible.
The extraction of UL5 was challenging due to the high trabeculation of the bone and the fact that there was little bone loss.7 It was also made difficult due to the fact that the UL5 was heavily carious and broken down.8 Assistance from a colleague was needed to complete the extraction of the UL5, which was an excellent learning opportunity on case selection and when to decide to complete treatment, or when a referral may be more appropriate.
With regards to the provision of an immediate denture, it was explained to the patient that as a result of the extraction of the UL5 prior to fitting the denture, there would be some bone remodelling in that area. This could result in some change in the retention of the denture over a 12-month period.9 The patient had never worn a denture before, and therefore, he was also warned that there would be a period of habituation and was advised that wearing the dentures more often would aid in this. The immediate denture was fitted straight after the extraction of the UL5 and the patient was provided with appropriate denture hygiene advice.
The UR5 had a previous disto-occlusal amalgam restoration that had been placed many years previously. The patient had no symptoms from the area, but on radiographic examination, there was a radiolucency consistent with secondary caries on the distal aspect of the restoration. It was explained to the patient that caries tends to be more extensive clinically than what appears radiographically.10 There were options for the UR5 to be restored either with a direct or an indirect restoration. However, there was a question about whether the tooth was restorable at all. If the tooth was proved to be unrestorable, then TC agreed to having the tooth added onto the existing immediate denture. The distal aspect of the cavity on the UR5 was subgingival; however, a good margin was achieved posteriorly by the placement of a retraction cord and the use of a matrix band. The final restoration was carried out in amalgam. Amalgam was chosen over composite for multiple reasons including the distal subgingival margin making moisture control more difficult, and also that amalgam is able to tolerate high occlusal load. The patient was warned that the UR5 had a questionable long-term prognosis owing to the size of the restoration and the subgingival margin. Oral hygiene instruction was emphasized, particularly with the use of interdental cleaning aids distal to the UR5 to prevent further caries development.
Prior to commencement of any advanced restorative treatments, such as endodontic treatment or the placement of an indirect restoration, the patient's periodontal health was reviewed. This was necessary because it affects the long-term prognosis of any restorative procedure.11 The patient had demonstrated compliance with the oral hygiene regimen recommended. This was demonstrated by reduced calculus and plaque deposits at all subsequent visits. The patient had no increased pocketing around the UR4 that required both root canal treatment and an indirect restoration.
The difficulty of the root canal treatment for the UL4 was assessed using the American Association of Endodontics difficulty assessment guidelines prior to commencement of treatment.12 It was considered to be of minimal difficulty. The UL4 had two canals and both were prepared using rotary instrumentation under rubber dam. The canal system was irrigated with sodium hypochlorite throughout.13 A working length radiograph was taken because there were inconsistent readings with the apex locator to accurately determine the length of the canals. Obturation was completed through the single cone obturation method and the use of a sealer.
Cuspal coverage is important to help prevent fractures in endodontically treated teeth that encounter higher occlusal forces.1 The options were discussed with the patient, and he chose to have a metal–ceramic crown placed. As can be seen from the clinical photography, the shade of the crown is lighter than the natural dentition (Figure 4a). This was due to inaccurate shade taking at a previous visit. This information was given to the patient prior to cementation and the patient was offered a remake of the crown. The patient decided to go ahead with cementation of this crown and accepted the difference in colour.
After a few months, the patient began complaining of denture looseness of his upper immediate partial denture and food stagnation under the palate. On assessment, the denture was unretentive after resorption of the bone in the UL5 region. The patient was offered a replacement acrylic or CoCr denture. After explaining both options to the patient, he opted for a CoCr upper partial denture (Figure 3c). The upper arch was a Kennedy class 3 modification 1.14 As the CoCr was only replacing three missing teeth and both saddles were bounded saddles, this made the denture design simpler. Rest seats were cut on the mesial aspect of the UR5 and the distal aspect of the UR2, as well as the distal aspect on the UL6 and mesial of the UL7. Clasps were used as a retentive feature, and a ring design was used for the connector as the patient disliked the palatal coverage on the immediate denture (Figure 5d). The patient was happy with both the appearance and fit of the CoCr denture, which was both retentive and stable on assessment.
Future treatment considerations for the patient could include rehabilitation of the upper arch with bridgework or implants. An example of this could include the UL5 space being replaced with a bridge or an implant because it is a single space, and both treatment modalities would be reasonable.
Conclusion
Overall, treating this patient has provided multiple learning opportunities in the field of restorative dentistry. Clinical photography skills were developed as a marked improvement can be seen between my pre-operative and post operative photographs. This is an important tool to use when trying to plan restorative cases but also to demonstrate to the patient the difference pre and post treatment. Photography is also an important medico-legal tool.15 I also managed to improve my treatment planning skills as the patient required multiple treatment modalities. This meant I had to plan each treatment phase in consideration of the following stage. If I were to treat a similar patient in the future, I would have also liked to have had some study models. The resulting study and working casts would allow me to monitor the tooth wear as the patient is only 31 and has signs of incisal edge wear. I provided the patient with treatment that was appropriate and addressed their presenting complaints. I also learned a lot from the planning and provision of care.