Anusavice K, Shen C, Rawls R. Phillips' Science of Dental Materials, 12th edn. St Louis, Missouri 63043: Elsevier Saunders; 2013
Albers HF. Tooth-Coloured Restoratives: Principles And Techniques, 9th edn. PMPH-USA: BC Decker; 2002
Feilzer AJ, De Gee AJ, Davidson CL. Setting stress in composite resin in relation to configuration of the restoration. J Dent Res. 1987; 66:1636-1639
Park J, Chang J, Ferracane J, Lee IB. How should composite be layered to reduce shrinkage stress: incremental or bulk filling?. Dent Mater. 2008; 24:1501-1505
Cara RR, Fleming GJ, Palin WM, Walmsley AD, Burke FJ. Cuspal deflection and microleakage in premolar teeth restored with resin-based composites with and without an intermediary flowable layer. J Dent. 2007; 35:482-489
Davidson CL, Feilzer AJ. Polymerization shrinkage and polymerization shrinkage stress in polymer-based restoratives. J Dent. 1997; 25:435-440
Burke FJ, Shortall AC. Successful restoration of load-bearing cavities in posterior teeth with direct-replacement resin-based composite. Dent Update. 2001; 28:388-398
Calheiros FC, Kawano Y, Stansbury JW, Braga RR. Influence of radiant exposure on contraction stress, degree of conversion and mechanical properties of resin composites. Dent Mater. 2006; 22:799-803
Ilie N, Jelen E, Hickel R. Is the soft-start polymerisation concept still relevant for modern curing units?. Clin Oral Investig. 2011; 15:21-29
Gao H, Yang BJ, Li N, Feng LM, Shi XY, Zhao WH Bisphenol a and hormone-associated cancers: current progress and perspectives. Medicine (Baltimore). 2015; 94
Chung SY, Kwon H, Choi YH, Karmaus W, Merchant AT, Song KB Dental composite fillings and bisphenol a among children: a survey in South Korea. Int Dent J. 2012; 62:65-69
Analysis of bisphenol a released from resin-based dental sealants. 2017.
Isufi A, Plotino G, Grande NM, Ioppolo P, Testarelli L, Bedini R Fracture resistance of endodontically treated teeth restored with a bulkfill flowable material and a resin composite. Ann Stomatol (Roma). 2016; 7:(1–2)4-10
Garcia D, Yaman P, Dennison J, Neiva G. Polymerization shrinkage and depth of cure of bulk fill flowable composite resins. Oper Dent. 2014; 39:441-448
El-Damanhoury H, Platt J. Polymerization shrinkage stress kinetics and related properties of bulk-fill resin composites. Oper Dent. 2014; 39:374-382
Shortall AC, Palin WM, Burtscher P. Refractive index mismatch and monomer reactivity influence composite curing depth. J Dent Res. 2008; 87:84-88
Sachdeva P, Goswami M, Singh D. Comparative evaluation of shear bond strength and nanoleakage of conventional and self-adhering flowable composites to primary teeth dentin. Contemp Clin Dent. 2016; 7:326-331
Rahimian-Imam S, Ramazani N, Fayazi MR. Marginal microleakage of conventional fissure sealants and self-adhering flowable composite as fissure sealant in permanent teeth. J Dent (Tehran). 2015; 12:430-435
Poitevin A, De Munck J, Van Ende A, Suyama Y, Mine A, Peumans M Bonding effectiveness of self-adhesive composites to dentin and enamel. Dent Mater. 2013; 29:221-230
Makishi P, Pacheco RR, Sadr A, Shimada Y, Sumi Y, Tagami J Assessment of self-adhesive resin composites: nondestructive imaging of resindentin interfacial adaptation and shear bond strength. Microsc Microanal. 2015; 21:1523-1529
Brueckner C, Schneider H, Haak R. Shear bond strength and tooth-composite interaction with self-adhering flowable composites. Oper Dent. 2017; 42:90-100
Weston JF. Predictable nanohybrid composite systems and techniques for anterior and posterior direct restorations. Compend Contin Educ Dent. 2013; 34:(Spec No 5)8-12
Ilie N, Bucuta S, Draenert M. Bulk-fill resin-based composites: an in vitro assessment of their mechanical performance. Oper Dent. 2013; 38:618-625
Freilich MA, Meiers JC, Duncan JP, Goldberg AJ. Fiber-Reinforced Composites in Clinical Dentistry.Chicago: Quintessence Publishing; 2000
Byrappa K, Yoshimura M. Handbook of Hydrothermal Technology: a Technology for Crystal Growth and Materials Processing.Park Ridge, NJ: Noyes Publications; 2001
Krause WR, Park SH, Straup RA. Mechanical properties of Bis-GMA resin short glass fiber composites. J Biomed Mater Res. 1989; 23:1195-1211
Callaghan DJ, Vaziri A, Nayeb-Hashemi H. Effect of fiber volume fraction and length on the wear characteristics of glass fiber-reinforced dental composites. Dent Mater. 2006; 22:84-93
Drummond JL, Lin L, Miescke KJ. Evaluation of fracture toughness of a fiber containing dental composite after flexural fatigue. Dent Mater. 2004; 20:591-599
Shouha PS, Ellakwa AE. Effect of short glass fibers on the polymerization shrinkage stress of dental composite. J Biomed Mater Res B Appl Biomater. 2017; 105:1930-1937
Belli S, Cobankara FK, Eraslan O, Eskitascioglu G, Karbhari V. The effect of fiber insertion on fracture resistance of endodontically treated molars with MOD cavity and reattached fractured lingual cusps. J Biomed Mater Res B Appl Biomater. 2006; 79:35-41
Shouha P, Swain M, Ellakwa A. The effect of fiber aspect ratio and volume loading on the flexural properties of flowable dental composite. Dent Mater. 2014; 30:1234-1244
Randolph LD, Palin WM, Bebelman S, Devaux J, Gallez B, Leloup G Ultra-fast light-curing resin composite with increased conversion and reduced monomer elution. Dent Mater. 2014; 30:594-604
Randolph LD, Palin WM, Watts DC, Genet M, Devaux J, Leloup G The effect of ultrafast photopolymerisation of experimental composites on shrinkage stress, network formation and pulpal temperature rise. Dent Mater. 2014; 30:1280-1289
Resin-based composite materials are widely used in contemporary restorative dentistry. Dental materials are constantly evolving as performance data become available and materials science advances. It is critical that the dental team is aware of changes in the science underpinning the resin-based composite materials that they are using as this may have an impact on how the materials are manipulated clinically and the ultimate success of the restoration. This paper reviews recent developments in resin-based composite materials, concentrating on those used for direct restorative procedures.
CPD/Clinical Relevance: As materials science advances, so the constituent chemicals of resin-based composites may change, affecting the way these materials should be handled clinically by the dental team.
Article
A resin-based composite (RBC) may be defined as a dental material composed of a chemically active resin and an inorganic filler, usually a glass or ceramic.1 The addition of the filler overcomes many of the shortcomings of the resin and enhances the properties of the final material. These effects include:1
Increased mechanical strength, particularly in compression;
Increased wear resistance;
Reduced polymerization shrinkage;
Enhanced optical properties (shade, fluorescence and translucency);
Confers radio-opacity due to the addition of heavy metal salts such as barium;
Reduced polymerization exotherm as the filler acts as a heat sink;
Reduced thermal expansion, closer to that of the tooth.
The resin and filler must be chemically connected using a silane coupling agent as they have no inherent ability to bond together. This permits stresses to be transmitted from the polymer matrix to the filler particles which have a higher modulus of elasticity (ie they are more rigid and stiffer). This results in improved physical and mechanical properties and the inhibition of leaching by preventing water from penetrating along the filler-resin interface.2
A curing system also needs to be incorporated into the material to effect its set. There has been a strong move in recent years towards utilizing some form of light curing system where visible light is used in combination with a photoinitiator contained within the resin to initiate the setting reaction. This so called ‘command set’ is advantageous in that the material may be presented as a paste in optimal condition which may be applied to the site of application and manipulated until the clinician is happy with the position and shape of the restoration, then exposing it to the curing light. RBC materials also contain other chemicals in minute quantities to maintain their stability in ultraviolet light, prevent premature polymerization and modify the optical properties of the product.
Resin-based composites are now widely used in dentistry as they offer excellent aesthetics and bond to dental hard tissues (with the use of an appropriate adhesive system) enabling more conservative (minimally invasive) cavities to be prepared. Such is the popularity and increased applications of resin-based composites that they have almost become ubiquitous materials.1
Most dental materials' development is incremental.1 As problems are identified with existing products the dental material manufacturers identify how to improve on, or eliminate, any shortcoming. However, the scope for potential improvement is restricted to modifying the components of the existing product. In recent years, this has mainly focused on the resin, filler and the photoinitiating system. This paper reviews the recent developments in resin-based composite materials, concentrating on the direct restorative materials.
Polymerization shrinkage and its clinical ramifications
The resins used in RBCs are monomers and, when polymerized into their cured state, a volumetric decrease occurs. This polymerization shrinkage has been cited as one of the most important shortcomings of this family of materials. The effects of these shortcomings are reviewed in Figure 1. Importantly, it is not the polymerization shrinkage which is the problem but the stresses which are generated as a result.
Figure 1. Complications of polymerization shrinkage include: microleakage (leading to pulpitis (pain and compromised pulpal health)); marginal staining; recurrent caries; stress at the interface between the material and tooth leading to partial or total debonding; stress within the surrounding tooth structure leading to pain, cracked cusp syndrome or fracture; stress within the set restoration leading to fracture; inability to manipulate the material to form accurate occlusal relationships and approximal contact areas in Class II restorations.
Conventional clinical placement techniques to minimize polymerization stress
Attempts in recent years, both in clinical techniques and material composition, have aimed to decrease the effects of polymerization stress, which is mainly determined by three factors:1
Polymerization shrinkage;
Internal flowability of the material; and
Polymerization kinetics (speed of cure).
The clinical techniques of reducing stress involve incremental placement of the material.3 Careful placement of the material may have an impact on the magnitude of stress and is associated with the Configuration or C factor.4 This is the ratio of bonded to unbonded surfaces. In posterior cavities with a high C factor (ie more bonded to unbonded surfaces), the so called herring bone or oblique incremental placement technique of RBC placement was postulated where only one or two surfaces are concurrently contacted by the increment of material4 (Figure 2). This reduces the C factor of each increment so permitting stress relief, which occurs more readily in unbonded surfaces. However, in situations where there is a lower, more favourable C factor, such as the restoration of a cusp tip, horizontal placement of each increment may be appropriate (Figure 3). Incremental placement of layers of material no more than 2 mm in depth5 also facilitates light penetration, so ensuring that the product may be fully cured.
Figure 2. The herring bone/oblique incremental placement of RBC in posterior cavities recommended to decrease polymerization stresses.Figure 3. A schematic representation of a Class I cavity which has a high C factor (left figure). There are four surfaces which are bonded compared to one unbonded surface where stress relief during curing may occur. This shape of cavity would require incremental placement of resin composite in an oblique fashion in an attempt to decrease polymerization stresses. Compare this to the restoration of a cusp tip where only the base is bonded where stress relief cannot occur (low C Factor) (figure on right). As a result horizontal layering of the increments would not pose a problem.
Other techniques to reduce polymerization stress involve the use of a flowable RBC as an intermediate layer. This has been shown to reduce the cuspal deflection which can occur during curing of the RBC as a result of polymerization shrinkage.6 Cuspal deflection can lead to cracked cusp syndrome or fracture of the tooth tissue, particularly in teeth with poor compliance.7
It is recommended that a sectional matrix system is used when restoring a Class II cavity8 (Figure 4). If a matrix band designed for dental amalgam is used (eg Siqveland or Tofflemire) deflection of the cusps occurs as the matrix band is tightened, leading to the cusps being bonded in a stressed position. The subsequent polymerization shrinkage would cause further stress and may lead to pain or fracture of the remaining tooth structure. The other advantage of using a sectional matrix is that this system deflects the tooth slightly, which compensates for matrix band thickness to permit the creation of tight, anatomically correct approximal contact areas. However, in cases where cavities have insufficient tooth tissue to support the matrix, or when cusps need to be replaced, the use of a sectional matrix would be difficult. In such situations, SuperMat® (Kerr Dental, Bioggio, Switzerland) may be used (Figure 5).
Figure 4. An example of a sectional matrix system used during the restoration of a Class II cavity in LL5 (Triodent® V3 Sectional Matrix System, Triodent Ltd, Katikati, New Zealand).Figure 5. Kerr Dental's SuperMat® matrix system may be easier to use where insufficient approximal tooth tissue exists to support a sectional matrix system.
Polymerization stresses may also be caused by the internal flowability of the material in its pre-gelation phase, which is exacerbated by polymerization kinetics, namely the speed of cure.1 If the material is cured too quickly, stress relief cannot occur as readily and shorter polymer chains result, which have a detrimental effect on the mechanical properties of the set material.9 For these reasons, it was postulated that different curing modes, such as soft start or ramp cure should be used to reduce the amount of energy applied to the material in the early phase of cure.10 However, these are little used today.
Modifications to the resin
Dental material manufacturers have attempted to reduce polymerization stress by making changes to the composition of the resin component. Combinations of resins, such as bisphenol A polyethylene glycol diether dimethacrylate (bis-EMA) containing resins and urethane dimethacrylate (UDMA), shrink as little as 2.2% when polymerized and so are being used more commonly. bis- EMA also has the advantage of reducing and controlling viscosity, so facilitating clinical manipulation.11
There has been a move away from using the bis-GMA monomer which uses bisphenol A (BPA) in its synthesis to maximize the stress relief during polymerization. Furthermore, bisphenol A has been reported to be a xenoestrogen (mimics the effects of oestrogen) and anti-androgenic.2 This has been implicated in breast,12 ovarian,12 prostatic12 and testicular carcinomas, decreased sperm count, hypospadias, and is detrimental in organogenesis, as demonstrated in molecular modelling and oestrogen receptor-BPA binding in vitro studies, although the effects in humans are not clear.2 There has been concern that, if this chemical is eluded from the material during clinical use, then the patient may be exposed as BPA has been measured in urine.13 That said, a piece of work presented at the IADR meeting in 2017 by the American Dental Association concluded that BPA exposure from 12 dental sealants sold in the USA is well below the daily exposure limit of 50,000 ng per kg body weight per day as set by the US Environmental Protection Agency (EPA) and so can be considered safe.14
More recently, a new family of resin-based composite materials, called the bulk fills, has been developed in an attempt to simplify and quicken their clinical placement, as they may be placed into the cavity in increments of up to 5 mm. In order to achieve this, polymerization stresses had to be decreased. The first commercial product to market was SureFil® SDR® Flow Posterior Bulk Fill Flowable Base (Dentsply, York, PA, USA), which was introduced in 2009 and contains a polymerization modulator (a chemical with a lower modulus of elasticity) which interacts with the photoinitiator camphorquinone (CQ), resulting in a slower elastic modulus development. There are other ways in which these materials may attempt to reduce polymerization stresses. Other products use a polymerization modulator to increase the flexibility of the resin, allowing it to stretch and stress relieve during function.15 Another method is to use two monomers in the resin which work in combination.16 One monomer is a high molecular weight aromatic urethane dimethacrylate (AUDMA) which has fewer reactive groups and so the volumetric shrinkage is reduced. Another class of compounds called addition fragmentation monomers (AFM) work in combination with AUDMA. These methacrylate molecules react into the developing polymer by forming crosslinks between adjacent polymer chains. When stressed during polymerization above a certain point, these molecules break or fragment, so providing a means for relaxation of the developing polymer network to stress relieve. These fragments then react with each other or other nearby reactive sites in a less stressed environment as the polymer chain develops until completion. It is interesting to note that similar volumetric shrinkage occurs between conventional and bulk fill RBCs,17 but less shrinkage stress occurs in the latter products.18
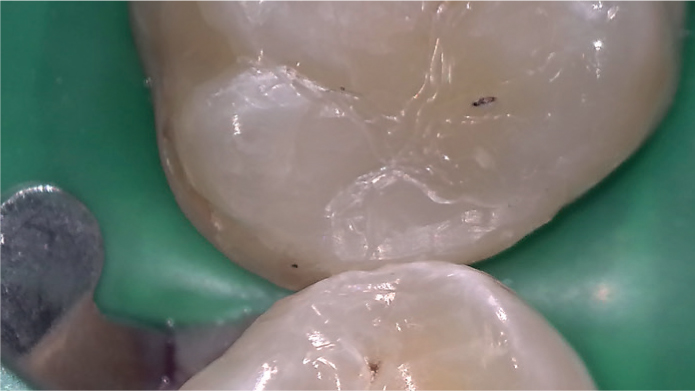
In addition, the penetration of the light through these materials had to be facilitated to permit increased increment thickness. It was shown some time ago that increased curing depth was facilitated by optimizing the mismatch between the refractive index of the filler and resin.19 The refractive index of the resin in bulk fills was therefore modified which resulted in a more translucent material (Figure 6). In the latest products to market, further modifications of the refractive index of the resins have been made in an attempt to overcome this translucency. In the pre-polymerized state, one product (Filtek™ One Bulk Fill Restorative, 3M™, St Paul, MN, USA) is sufficiently translucent to facilitate light penetration to a depth of up to 5 mm, but then during curing the refractive index changes with the final shade being more opaque.20
Figure 6. A restored DO cavity in UR6 using a second generation bulk fill material Filtek™ Bulk Fill Posterior (3M ESPE). Note the slight translucency of the cured restorative material.
Self-adhesive composites
Resin-based composite has no inherent ability to bond to dental hard tissues, instead a compatible bonding agent must be used.1 Another potential simplification aimed at reducing clinical placement time may be the introduction of self-adhesive composites which may be bonded to enamel and dentine without etching and bonding. The most studied products are the low viscosity RBCs, such as fissure sealants, flowable RBCs and self-adhesive luting resins. The evidence is mixed, with nanoleakage scores of both conventional and self-adhering flowable RBCs being comparable in primary teeth21 and microleakage less with self-adhering flowable RBCs compared to conventional fissure sealant. Self-adhering flowable composite can therefore be used as a fissure sealant in permanent teeth.22 However, shear bond strength has been shown to be lower compared with conventional RBCs in both permanent23,24 and primary teeth,21 suggesting that self-etched flowable RBCs clinical application should be carefully considered.23,25
Modifications to the filler
Traditionally, resin-based composites have been referred to and categorized by the average size of the filler particle. Many contemporary materials are composed of particles of different sizes which usually increase the filler loading and are termed hybrids. This has the effect of increasing the mechanical properties and wear resistance of the material whilst providing a means of creating and retaining a polish. For example, a microhybrid is a resin-based composite material whose average particle size is in the micro range (approximately 40 nm).2 The effect of filler loading can be seen by comparing the viscosity of flowable and universal RBC presentations (Figure 7).
Figure 7. Examples of flowable and conventional resin composite materials, namely Filtek™ Supreme XTE Flowable Restorative and Filtek™ Supreme XTE Restorative (both products of 3M ESPE). Note the difference in their viscosities.
Nanofilled composites (also known as nanocomposites) were introduced in an attempt to improve polishability without any detrimental effect on strength. These are composites whose particles are nanometer-sized (1−100 nm) and have been surface treated with silane before they have agglomerated (derived from Latin ‘to form into a ball’) forming loosely bound spheroidal aggregates called clusters (like a bunch of grapes) of primary nanoparticles which may exceed 100 nm.11 When the material is polished, some individual nanoparticles shear at a rate similar to the surrounding resin matrix, so yielding a good polish,11 unlike the old macrofilled particles, which were lost from the softer matrix when it was polished and thus a satisfactory polish was never achievable. Most RBC products which boast improved polishability are composed of particle sizes in the nano range.26Table 1 lists some well-known brands categorized with respect to their filler load.
Product Name
Manufacturer
Type of RBC
ceram.x universal
Dentsply
nanohybrid
Clearfil
AP-X Kuraray
microhybrid
Clearfil Majesty ES-2 Premium
Kuraray
nanohybrid
Filtek™ Supreme XTE Universal Restorative
3M ESPE
nanofilled
Filtek™ Z500 Universal Composite
3M ESPE
nanofilled
Gradia
GC
microhybrid
Herculite XRV™
Kerr
microhybrid
Ice
SDI
nanohybrid
Miris 2
Coltène Whaledent
nanofilled
N'Durance®
Septodont
nanofilled
Polofil Supra
Voco
microhybrid
Premise™
Kerr
nanofilled
Spectrum TPH 3
Dentsply
microhybrid
Synergy D6
Coltène Whaledent
nanohybrid
Venus
Kulzer
nanohybrid
Venus Pearl
Kulzer
nanohybrid
The fillers used in the bulk fill materials mentioned earlier either facilitate penetration of the light energy to effect curing (in which case the particle size has been increased27) or have a lower elastic modulus with the aim of reducing shrinkage stress. The bulk fill RBCs are now available in two viscosities (Figure 8).
Figure 8. Tetric EvoFlow® Bulk Fill (Ivoclar Vivadent, Schaan, Liechtenstein) and Tetric EvoCeram® Bulk Fill (Ivoclar Vivadent) demonstrating the difference in viscosities between the first and second generation bulk fill materials. Compare the viscosity of these products with those in Figure 7.
The low viscosity of the first generation bulk fills (which are now referred to as bulk fill base materials) is due to a reduced filler loading so they may adapt more readily to the floor and walls of the cavity to reduce the potential for voids and increasing depth of cure.27 The second generation (bulk fill restorative) materials have a higher filler loading (76−77% by weight (53−54% by volume)) and so exhibit a higher viscosity, so allowing the whole cavity to be restored using the same product as their compressive strength and wear resistance are higher (Figure 6).
’Ceramic’ composites
Frequently in marketing literature the term ‘ceramic composites’ is often seen. This may be considered misleading as it infers a difference in RBC chemistry. In fact, it refers to the filler being a ceramic and should not be confused with a ceramic material.
Filler particle size and shape
Traditionally, spherical or spheroidal particles or clusters of them have been used in resin-based restorative composite materials. Work has been done on investigating whether RBC reinforced with hydroxyapatite rods and whiskers exhibited increased flexural strength.28 Fibres or whiskers display high tensile strength and they have potential to reinforce RBCs, so improving the mechanical properties and reliability of the material.29,30 The size of the whiskers is significant as improved handling and better mechanical properties are seen with short fibres31 and large fibres were found to separate from the matrix due to residual polymerization shrinkage stress.32,33 A study carried out by Zhang and Darvell concluded that hydroxyapatite whiskers could provide better mechanical properties in bis-GMA-based composites compared with a nano-scale powder.28
The use of glass fibres as fillers in RBCs has also been studied,34 with the use of polyethylene fibres in combination with a regular RBC used to splint teeth. This technique has been shown to strengthen and toughen both RBCs and teeth.35 Shouha's group hypothesized that the addition of a small amount of randomly orientated fibres may improve flexural strength and elastic modulus whilst retaining flowability.36 They examined the aspect ratio (relationship of length to diameter) of glass fibres and volume loading on the flexural strength of flowable RBCs and found that short and very short glass fibres can significantly reinforce flowable dental composite, with the aspect ratio more important than the volume loading for flexural strength. Furthermore, the refractive index of glass fibres is closer to that of the resin and therefore permits light penetration. This is opposed to crystalline whiskers, carbon fibres and carbon nanofibres, which are opaque, yellow and black, respectively, which have also been investigated.
It will be interesting to watch the continuing development of RBCs with respect to filler particle size and shape and whether the use of non-spheroid particles with their potential benefits will become more commonplace in future.
Utilization of different photoinitiators
The traditionally used photoinitiator is camphorquinone which, when exposed to sufficient energy at a wavelength of approximately 470 nm, reacts with an amine accelerator in the RBC to initiate the curing process via a free radical reaction. Although still widely used, there has been a move away from CQ in recent years. Firstly, CQ is yellow in colour and its presence influences the shade of the final product, which may be especially problematic with bleached white shades. Secondly, CQ requires more energy to commence the setting reaction, so the dentist must decrease the thickness of each increment of the RBC to ensure complete set. To overcome these shortcomings, CQ has been used in combination with other photoinitiators37,38 and, indeed, replaced by alternatives. Chemicals such as Lucirin TPO (2,4,6-trimethylbenzoyldiphenylphosphine oxide), PPD (phenylpropanedione) and Ivocerin (bis-(4-methoxybenzoyl) diethylgermane) have a higher quantum efficiency, in other words they are more efficient at absorbing and converting photon energy39 and so they require less light energy to effect the setting reaction.40
Ivocerin was developed by Ivoclar Vivadent and is included in products such as Tetric EvoCeram® Bulk Fill (Figure 8). Lucirin TPO has been shown to provide significantly improved depth of cure compared to CQ.39 This means that the cavity can be filled in one increment of material (up to 5 mm in the purely light cured products) and cured. As a result, the clinical procedure of placement of the restoration is much quicker and simpler, as seen in the bulk fill RBCs. Furthermore, Lucirin TPO has been shown to improve the mechanical properties of the RBC with no increased stress and a low exotherm measured during polymerization, when compared to CQ-containing products.40 Another advantage for the use of Ivocerin is that the tertiary amine accelerator is not required41 and so the material is more colour stable as amine-containing products have a tendency to yellow and darken with time.1
In order for the RBC to cure, it must be exposed to visible light of sufficient intensity and the correct wavelength. It is important to note that the more recently introduced photoinitiators have a peak absorption at a lower wavelength than CQ. For example, Lucirin TPO and PPD are most effective at between 380 and 430 nm,1 whilst the peak absorption of Ivocerin is 408 nm.41 The light source of most light curing units is now derived from LEDs which have a much narrower spectral band. Unless the spectral band of the curing light matches the peak absorption of the photoinitiator, inadequate curing will result, leading to inferior mechanical properties, compromising clinical performance and longevity of the restoration (Figure 9).
Figure 9. A schematic representation of the wavelength range, spectral peaks and light output of a polywave LED curing light, relative to the photoinitiators camphorquinone and Lucirin TPO. Note that the photoinitiator's peak absorption and the spectral bands of the curing light coincide.
With the increasing use of the newer photoinitiators, clinicians are advised to ensure that their curing lights are compatible with each light cured product being used in surgery. Furthermore, they may wish in future to consider purchasing a polywave LED curing light which has a number of LEDs which produce output at all of the necessary peak absorptions to ensure compatibility with all products.
Conclusion
The main recent innovations to resin-based composite materials are to the resin, fillers and photoinitiator. It is imperative that the dental team understand these developments in order to use all materials according to the manufacturer's instructions to optimize their clinical performance.